Introduction
The X chromosome plays a vital role in numerous biological functions and is crucial for the development of various tissues, including those of the nervous system, blood, liver, bones, kidneys, retina, ears, heart, skin, and teeth. Mutations or alterations in its genes are associated with over 530 known disorders.[1] An X-linked trait or disorder occurs from a pathogenic variant in a gene on the X chromosome.
In 1961, Mary Lyon proposed that in the cells of mammalian females, one of the two X chromosomes undergoes random inactivation during early embryonic development. As a result, both males and females effectively have a single active X chromosome. Lyon's hypothesis significantly advanced the understanding of the basic mechanisms underlying X-linked diseases.[2][3][4][5]
Classically, X-linked inheritance is described as either X-linked recessive or X-linked dominant (see Image. Pattern of X-Linked Inheritance).
X-Linked Recessive Inheritance
Males who carry a pathogenic variant are affected, whereas females—who have a second nonpathogenic copy of the gene—are typically unaffected (or only mildly affected). A male with an affected allele on his single X chromosome is hemizygous and cannot transmit the disorder to his male offspring, but all his daughters are obligate carriers. Healthy heterozygous carrier females can pass the disorder to affected sons. Thus, from affected males, it can be transmitted to male grandchildren through a carrier daughter (diagonal or Knight's move transmission).
The X chromosome from a male is transmitted to daughters, and the Y chromosome is transferred to sons. If an affected male has children with a healthy female, none of his male offspring are affected, but all of his female offspring are carriers. If a carrier female has children with a healthy male, each male offspring has a 50% chance of being affected, and each female offspring has a 50% chance of being a carrier.
Variable expression: Heterozygous females carry one pathogenic allele on one X chromosome and one normal allele on the other. These females may exhibit variable expression of X-linked recessive disorders due to the random process of X inactivation. This variability results in mosaicism, where some cells inactivate the X chromosome with the mutant allele, whereas others inactivate the X chromosome with the normal allele.[1]
X-Linked Disorders in Females
Although X-linked recessive disorders typically affect males, females may occasionally be affected. This observation can be explained by one of the following possibilities:
- Heterozygosity: Inactivation is a random process that may involve either the X chromosome carrying the mutant allele or the one carrying the normal allele in a heterozygous female. This inactivation does not lead to complete silencing of one X chromosome, as approximately one-third of X-linked genes are expressed from both chromosomes to varying degrees across cells. The clinical significance of this incomplete inactivation is not yet fully understood.[PubMed PMID: 29022598] In cases where the X chromosome with the mutant allele remains active in the majority of cells (skewed X inactivation), disease expression can occur. This phenomenon has been observed in disorders such as Duchenne muscular dystrophy and hemophilia A.[6][7]
- Homozygosity: When both X chromosomes in a female carry a mutant allele, disease expression occurs. This phenomenon has been reported in conditions like hemophilia A and ichthyosis.[8][9]
- Translocations: If a female carries a translocation involving an autosome and one of the X chromosomes, and this translocation disrupts a gene on the X chromosome, the disorder may manifest. This phenomenon has been observed in cases of Duchenne muscular dystrophy.[10][11][10]
- In females with Turner syndrome (who have only one X chromosome), if the single X chromosome carries a mutant allele, the disorder may be expressed. Hemophilia has been reported in females with Turner syndrome.[12]
X-Linked Dominant Inheritance
Both males and females can be affected, but females are affected more frequently and usually less severely. Affected males can transmit the mutant allele to all their daughters but not to their sons. Affected females have a 50% chance of transmitting the mutant allele to each of their sons and daughters. Examples include vitamin D–resistant (hypophosphatemic) rickets and Charcot-Marie-Tooth disease.[13][14]
Some X-linked dominant disorders, such as incontinentia pigmenti (Bloch-Sulzberger syndrome), show mosaicism in heterozygous females.[15]
X-linked dominant lethals: X-linked dominant lethal disorders are incompatible with early embryonic survival in males. These disorders are observed only in females because the severe form typically results in the death of male embryos, whereas females, being less severely affected, can survive.[16]
Current View
Many female carriers of X-linked recessive disorders demonstrate mild phenotypes. This observation is attributed to the variable expressivity of X-linked disorders and the involvement of multiple mechanisms, such as skewed X-inactivation, somatic mosaicism, and others. Recently, studies have proposed discontinuing the terms dominant and recessive and classifying all such conditions simply as X-linked disorders.[17][18][19]
Development
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Development
The mechanisms regulating the expression of the active X chromosome during early development remain a subject of debate. Genes on the single active X chromosome in mammals were long believed to be upregulated 2-fold to match the expression of genes on 2 autosomes, thereby compensating for the loss of Y-linked genes.[PubMed PMID: 18729722] Early evidence from microarray studies supported this hypothesis, reporting an X-to-autosome expression ratio (X:AA) of approximately 1.[PubMed PMID: 16341221] However, later studies using more accurate RNA sequencing methods challenged this view, showing X:AA ratios closer to 0.5.[PubMed PMID: 21102464]
More recently, partial upregulation of the X chromosome has been reported, with expression estimated at about 1.6 times that of autosomal genes.[PubMed PMID: 40359939] In parallel, single-cell transcriptome studies of early human embryos revealed that X-linked genes in males are not upregulated 2-fold and that expression in females gradually declines to match male levels.[PubMed PMID: 30642250] These findings result in a dosage imbalance between the X chromosomes and autosomes in both sexes, contradicting the assumption of complete dosage compensation proposed by Ohno. Moreover, X-linked genes exhibit greater expression variability and lower dosage sensitivity, supporting the insensitive X hypothesis. This hypothesis suggests that many X-linked genes can tolerate dosage fluctuations without detrimental effects.[PubMed PMID: 30642250]
Molecular Level
The HUGO Gene Nomenclature Committee has identified 829 sequence-coding genes on the X chromosome, of which 205 are linked to monogenic disorders.[PubMed PMID: 30304474][OMIM®. An Online Catalog of Human Genes and Genetic Disorders (2020)]
The impact of sex on the expression of these disorders varies depending on the specific gene involved. Some genes show a more equal effect on both sexes, affecting hemizygous males and heterozygous females similarly.
- MECP2, CDKL5, and DDX3X typically arise de novo and preferentially affect heterozygous females.[PubMed PMID: 20301670][PubMed PMID: 15492925][PubMed PMID: 15499549][PubMed PMID: 26235985]. Hemizygous males with mutations in these genes are often nonviable unless the variants are milder (hypomorphic) or mosaic in nature.
- Genes such as IQSEC2, NEXMIF, KDM5C, HUWE1, USP9X, and CLCN4 were initially thought to cause disorders primarily in males but are now recognized as affecting females as well.[PubMed PMID: 30206421][PubMed PMID: 33144681][PubMed PMID: 32279304][PubMed PMID: 29180823][PubMed PMID: 33298948][PubMed PMID: 27550844]
- Interestingly, 2 X-linked disorders associated with PCDH19 and EFNB1 display an unusual pattern: they predominantly affect heterozygous females and mosaic males, whereas hemizygous males typically do not manifest the condition.[PubMed PMID: 22267240][PubMed PMID: 18043713]
Testing
Diagnosis of X-linked disorders typically begins with a detailed clinical evaluation and family history, with attention to patterns consistent with X-linked inheritance, such as a higher prevalence in males, transmission through maternal lines, and the absence of male-to-male transmission. Clinical suspicion is further supported by characteristic signs and symptoms associated with specific disorders, such as progressive muscle weakness in Duchenne muscular dystrophy or bleeding tendencies in Hemophilia A.
X-Linked Recessive Inheritance
The following features are necessary to establish the clinical diagnosis.
- The disorder predominantly affects males.
- X-linked recessive disorders are transmitted through healthy carrier females to their sons.
- Male-to-male transmission is absent.
X-Linked Dominant Inheritance
The following features are necessary to establish the clinical diagnosis.
- Both males and females are affected, with females more commonly affected.
- Females are less severely affected.
- Affected males transmit the disorder only to their daughters, whereas affected females can transmit the disorder to both sons and daughters.
Once clinical suspicion is raised, genetic testing is used to confirm the diagnosis. Many of these disorders can now be detected prenatally through chorionic villus sampling or amniocentesis, followed by molecular analysis during early pregnancy. In families with a known pathogenic variant, carrier testing can be offered to at-risk female relatives for reproductive planning. However, spontaneous mutations may occur, and in such cases, the disorder may arise in individuals with no previous family history.
Add: Pedigree examples to demonstrate this section
Clinical Significance
As most of the genes are related to brain function (reference PMID), most disorders involve neurological deterioration. This neurological role of the X chromosome helps explain why 6% of developmental disorders are attributed to X-related disorders.[PubMed PMID: 33504798][PubMed PMID: 36323681] Despite the general bias that X-linked disorders are more commonly diagnosed in males, a large cohort study showed that males and females are equally affected.[PubMed PMID: 33504798]
Moreover, X-chromosome genes were significantly more often linked to intellectual disability, seizures, and difficulties in language development. In contrast, they showed no significant association with motor delays, spasticity, or ataxia.[PubMed PMID: 36323681]
Family Counseling
Understanding inheritance patterns is crucial in counseling families about potential risks for offspring. Tables 1 and 2 summarize the possible outcomes for X-linked recessive and dominant disorders based on parental genotypes.
Table 1. Inheritance Pattern of X-linked Recessive Disorders
| Parental Genotype | Child Gender | Inheritance Chance | Outcome |
| Carrier mother + healthy father | Son | 25% |
Affected (inherits mutant X from mother) |
| Son | 25% |
Unaffected (inherits normal X from mother) |
|
| Daughter | 25% |
Unaffected (inherits normal X from both parents) |
|
| Daughter | 25% |
Carrier (inherits mutant X from mother) |
|
| Healthy mother + affected father | Son | 50% |
Unaffected (inherits normal X from mother) |
| Daughter | 50% |
Carrier (mutant X from father, normal X from mother) |
|
| Carrier mother + affected father | Son | 25% |
Affected (mutant X from mother) |
| Son | 25% |
Unaffected (normal X from mother) |
|
| Daughter | 25% |
Carrier (mutant X from father, normal X from mother) |
|
| Daughter | 25% |
Affected (mutant X from both parents) |
|
| Any child | 100% |
Affected (inherits mutant X from both parents) |
Table 2. Inheritance Patterns of X-Linked Dominant Disorders
| Parental Genotype | Child Gender | Inheritance Chance | Outcome |
| Affected mother + healthy father | Son or daughter | 50% |
Affected (inherits mutant X from mother) |
| Son or daughter | 50% |
Unaffected (inherits normal X from mother) |
|
|
Healthy mother + affected father |
Son | 0% |
Unaffected (inherits Y from father) |
| Daughter | 100% |
Affected (inherits mutant X from father) |
|
|
Affected mother + affected father |
Son | 50% |
Affected (inherits mutant X from mother) |
| Son | 50% |
Unaffected (inherits normal X from mother) |
|
| Daughter | 50% |
Affected (mutant X from father, normal X from mother) |
|
| Daughter | 50% |
Severely affected or possibly lethal (mutant X from both parents) |
Common X-Linked Disorders
- Red-green color blindness is a common disorder affecting at least 10% of males and about 1% of females. The condition may be partial or complete, with the complete form being less common.
- Hemophilia A results from a mutation in the factor VIII gene. This condition may be inherited or caused by a spontaneous mutation. An acquired form can develop if a patient produces antibodies to factor VIII. The major complications involve bleeding, which can range from mild to life-threatening. Though rare today, transmission of HIV or hepatitis C occurred historically through contaminated blood products, especially in the 1980s and 1990s.
- Duchenne muscular dystrophy is caused by a mutation in the dystrophin gene. This condition leads to progressive muscle weakness, often resulting in respiratory failure and premature death.
- X-linked agammaglobulinemia leads to a failure in B-cell maturation, resulting in the absence of plasma cells and antibodies. Affected individuals are highly susceptible to recurrent and sometimes fatal infections.
- Alport syndrome is a genetically heterogeneous X-linked disorder affecting the basement membrane, particularly in the kidneys, eyes, and inner ears. This condition is associated with mutations in the type IV collagen gene.
- Charcot-Marie-Tooth disease is the most common inherited neurological disorder. This condition is characterized by peripheral neuropathy in the absence of metabolic or biochemical dysfunction. The condition shows variable penetrance, and spontaneous mutations have also been reported. Charcot-Marie-Tooth disease typically presents within the first two decades of life.
- Fabry disease is an X-linked lysosomal storage disorder marked by the accumulation of glycosphingolipids in vascular endothelium, smooth muscle, and epithelial cells. This buildup can cause multi-organ dysfunction. In young individuals presenting with skin lesions, renal failure, stroke, or cardiac events, Fabry disease should be considered.
- Other less common X-linked disorders include:
- Adrenoleukodystrophy is caused by mutations in the ABCD1 gene, leading to the accumulation of very long-chain fatty acids. This disorder primarily affects the brain and adrenal glands, causing progressive neurological decline and adrenal insufficiency, usually starting in childhood.
- Kabuki syndrome results from mutations in the KDM6A gene. This condition is characterized by distinctive facial features, developmental delay, heart defects, and immune abnormalities.
- Lesch-Nyhan syndrome is caused by mutations in the HPRT1 gene, leading to a deficiency of the HGPRT enzyme. This condition presents in infancy with excess uric acid (causing gout and kidney stones), along with severe neurological symptoms such as self-mutilation and movement disorders.
Media
(Click Image to Enlarge)
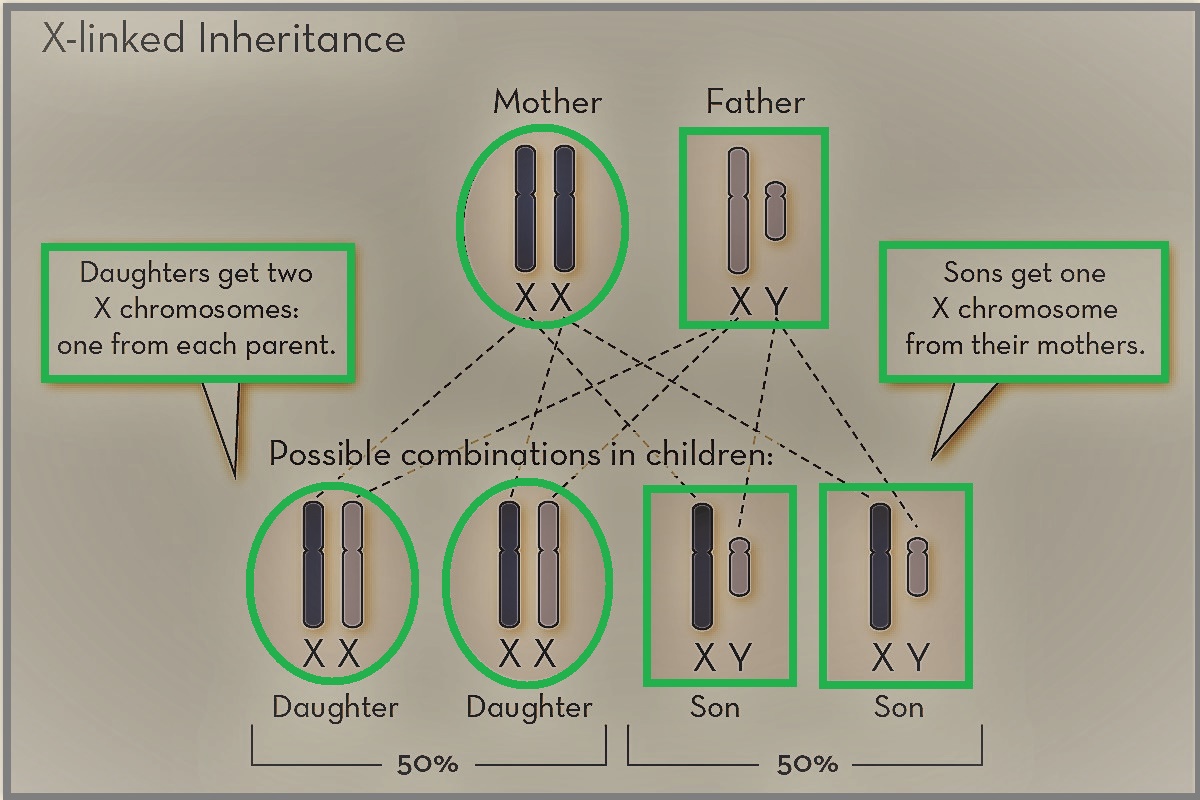
Pattern of X-Linked Inheritance. Daughters inherit one X chromosome from each parent, whereas sons inherit the X chromosome from the mother and the Y chromosome from the father, resulting in characteristic transmission patterns of X-linked traits.
Contributed by DK Yadav, MBBS
References
Migeon BR. X-linked diseases: susceptible females. Genetics in medicine : official journal of the American College of Medical Genetics. 2020 Jul:22(7):1156-1174. doi: 10.1038/s41436-020-0779-4. Epub 2020 Apr 14 [PubMed PMID: 32284538]
LYON MF. Gene action in the X-chromosome of the mouse (Mus musculus L.). Nature. 1961 Apr 22:190():372-3 [PubMed PMID: 13764598]
Level 3 (low-level) evidenceGendrel AV, Heard E. Fifty years of X-inactivation research. Development (Cambridge, England). 2011 Dec:138(23):5049-55. doi: 10.1242/dev.068320. Epub [PubMed PMID: 22069183]
Level 3 (low-level) evidenceHarper PS. Mary Lyon and the hypothesis of random X chromosome inactivation. Human genetics. 2011 Aug:130(2):169-74. doi: 10.1007/s00439-011-1013-x. Epub [PubMed PMID: 21643983]
Level 3 (low-level) evidenceSagie S, Monovich E. [MARY LYON (1925-2014) AND THE RANDOM INACTIVATION OF CHROMOSOME X]. Harefuah. 2016 Mar:155(3):140-4, 197 [PubMed PMID: 27305745]
Brioschi S, Gualandi F, Scotton C, Armaroli A, Bovolenta M, Falzarano MS, Sabatelli P, Selvatici R, D'Amico A, Pane M, Ricci G, Siciliano G, Tedeschi S, Pini A, Vercelli L, De Grandis D, Mercuri E, Bertini E, Merlini L, Mongini T, Ferlini A. Genetic characterization in symptomatic female DMD carriers: lack of relationship between X-inactivation, transcriptional DMD allele balancing and phenotype. BMC medical genetics. 2012 Aug 16:13():73 [PubMed PMID: 22894145]
Yang C, Yu Z, Zhang W, Cao L, Ouyang W, Hu F, Zhang P, Bai X, Ruan C. A novel missense mutation, p.Phe360Cys, in FIX gene results in haemophilia B in a female patient with skewed X-inactivation. Haemophilia : the official journal of the World Federation of Hemophilia. 2018 Mar:24(2):e68-e70. doi: 10.1111/hae.13423. Epub 2018 Feb 5 [PubMed PMID: 29405493]
Nair PS, Shetty S, Ghosh K. A homozygous female hemophilia A. Indian journal of human genetics. 2012 Jan:18(1):134-6. doi: 10.4103/0971-6866.96685. Epub [PubMed PMID: 22754241]
Level 3 (low-level) evidenceNagtzaam IF, Stegmann AP, Steijlen PM, Herbergs J, Van Lent-Albrechts JA, Van Geel M, Van Steensel MA. Clinically manifest X-linked recessive ichthyosis in a female due to a homozygous interstitial 1·6-Mb deletion of Xp22.31. The British journal of dermatology. 2012 Apr:166(4):905-7. doi: 10.1111/j.1365-2133.2011.10685.x. Epub 2012 Feb 6 [PubMed PMID: 21985695]
Level 3 (low-level) evidenceJacobs PA, Hunt PA, Mayer M, Bart RD. Duchenne muscular dystrophy (DMD) in a female with an X/autosome translocation: further evidence that the DMD locus is at Xp21. American journal of human genetics. 1981 Jul:33(4):513-8 [PubMed PMID: 7258185]
Level 3 (low-level) evidenceUchida T, Ogata H, Shirai Z, Mitsudome A. [Duchenne muscular dystrophy (DMD) in a female with an X-autosome translocation]. No to hattatsu = Brain and development. 1988 Jan:20(1):28-32 [PubMed PMID: 3279979]
Level 3 (low-level) evidenceShahriari M, Bazrafshan A, Moghadam M, Karimi M. Severe hemophilia in a girl infant with mosaic Turner syndrome and persistent hyperplastic primary vitreous. Blood coagulation & fibrinolysis : an international journal in haemostasis and thrombosis. 2016 Apr:27(3):352-3. doi: 10.1097/MBC.0000000000000424. Epub [PubMed PMID: 26484646]
Morena J, Gupta A, Hoyle JC. Charcot-Marie-Tooth: From Molecules to Therapy. International journal of molecular sciences. 2019 Jul 12:20(14):. doi: 10.3390/ijms20143419. Epub 2019 Jul 12 [PubMed PMID: 31336816]
Pavone V, Testa G, Gioitta Iachino S, Evola FR, Avondo S, Sessa G. Hypophosphatemic rickets: etiology, clinical features and treatment. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2015 Feb:25(2):221-6. doi: 10.1007/s00590-014-1496-y. Epub 2014 Jun 24 [PubMed PMID: 24957364]
Cammarata-Scalisi F, Fusco F, Ursini MV. Incontinentia Pigmenti. Actas dermo-sifiliograficas. 2019 May:110(4):273-278. doi: 10.1016/j.ad.2018.10.004. Epub 2019 Jan 17 [PubMed PMID: 30660327]
Franco B, Ballabio A. X-inactivation and human disease: X-linked dominant male-lethal disorders. Current opinion in genetics & development. 2006 Jun:16(3):254-9 [PubMed PMID: 16650755]
Level 3 (low-level) evidenceDobyns WB. The pattern of inheritance of X-linked traits is not dominant or recessive, just X-linked. Acta paediatrica (Oslo, Norway : 1992). Supplement. 2006 Apr:95(451):11-5 [PubMed PMID: 16720459]
Level 3 (low-level) evidenceMehta A, Beck M, Sunder-Plassmann G, Germain DP. General aspects of X-linked diseases. Fabry Disease: Perspectives from 5 Years of FOS. 2006:(): [PubMed PMID: 21290690]
Level 3 (low-level) evidenceDobyns WB, Filauro A, Tomson BN, Chan AS, Ho AW, Ting NT, Oosterwijk JC, Ober C. Inheritance of most X-linked traits is not dominant or recessive, just X-linked. American journal of medical genetics. Part A. 2004 Aug 30:129A(2):136-43 [PubMed PMID: 15316978]