Introduction
Ultrasound is well-suited for clinical practice given its affordability, portability, and lack of radiation exposure during image acquisition. These features allow clinicians from almost any specialty the ability to perform image-guided evaluations and interventions.[1][2][3][4][5] Radiologists are uniquely suited to perform these evaluations and procedures, given their extensive training, knowledge of human anatomy, and understanding of the varied anatomical appearances across multiple imaging modalities.[6]
Part of a radiologist’s training involves understanding medical physics, including how medical images are obtained. In ultrasound, the sonographer or physician utilizes a transducer to interrogate the area of interest. Within the transducer are piezoelectric crystals that vibrate when exposed to an alternating current. These vibrations generate sound waves transmitted into the patient’s soft tissues via a layer of ultrasound gel. The sound waves then interact with the tissue and are ultimately reflected to the transducer. Once the sound waves return to the transducer, they are converted back into an electric current. The computer then calculates the time interval between when the sound wave was initially generated and when the transducer received it to determine the location (depth) of the tissue that reflected the sound wave.
When planning a procedure, one must consider the type of transducer that yields the highest quality images. There are a variety of transducers that can be used with varied frequencies and shapes. In general, higher-frequency transducers are used for imaging more superficial structures, as they offer better resolution. However, the higher-frequency sound wave is more easily attenuated and has a decreased ability to penetrate tissue, limiting its use in the evaluation of deeper structures. For deeper structures or larger patients, one might choose a lower frequency or curved transducer. When imaging small body parts, such as a finger, a small transducer (hockey stick) may help.
Image guidance for procedures includes ultrasound, fluoroscopy, computed tomography, and, in some cases, magnetic resonance imaging (MRI). In general, ultrasound is particularly helpful in guiding soft tissue procedures such as therapeutic tendon sheath injection, soft tissue biopsy, and cyst or abscess aspiration/drainage.[1][7] Ultrasound, computed tomography, and fluoroscopy guidance can be used for both joint aspiration and therapeutic injection. The chosen modality may depend on availability, user expertise, the body part to be treated, and the patient's body habitus. Advantages of ultrasound include the absence of ionizing radiation and direct, real-time visualization of the needle and surrounding soft tissues during the procedure. During fluoroscopic guidance, the needle is intermittently imaged, and its position is assessed only relative to the associated osseous structures. The involved soft-tissue structures must be inferred from anatomical knowledge. Also, fluoroscopy often requires a contrast agent to verify needle placement, whereas ultrasound allows direct visualization of the needle position. Computed tomography is useful for biopsy of osseous structures or therapeutic injection of deep anatomic structures, which can be difficult to visualize with ultrasound or palpate on physical examination.[7][8][9][10]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The long head biceps muscle has a proximal insertion at the shoulder, where the tendon is intra-articular, originating on the supraglenoid tubercle and superior glenoid labrum. It exits the glenohumeral joint at the level of the humeral head near the rotator cuff attachments on the humerus, entering the bicipital groove. It is held within the proximal bicipital groove by the coracohumeral and transverse humeral ligaments as well as fibers of the subscapularis tendon.
In most patients, there are distinct attachments of the long and short heads of the biceps tendon on the radial tuberosity. The distal biceps tendons traverse the elbow joint and attach to the radial tuberosity. The long head normally constitutes the more proximal insertion on the radial tuberosity and the short head the more distal. Therefore, it is possible to have an isolated tear of either the long or short head.
At the distal biceps myotendinous junction, there is a broad aponeurosis known as the lacertus fibrosus (also called the bicipital aponeurosis), which circumferentially covers the flexor muscle attachments as well as the median nerve and brachial artery. This aponeurosis originates at the distal biceps tendon and inserts onto the radial tuberosity and proximal ulna. It is held in place by multiple strong fascial connections and serves as a protective covering for the neurovascular structures that course beneath. In most cases, the lacertus fibrosus prevents a torn biceps tendon from retracting more than a few centimeters proximal to the elbow joint; however, if the lacertus fibrosus is also injured, the tendon retraction may be more severe, making surgical repair more difficult.
Indications
Ultrasound has uses in a wide range of musculoskeletal procedures, including joint or bursa aspiration to evaluate for infection or crystalline deposition disease; joint or bursa injection, such as an arthrogram or steroid injection; tendon sheath injection; tendinosis therapy, such as dry needling; platelet-rich plasma injection; and percutaneous biopsy. Injections into a joint, bursa, or tendon sheath can be both therapeutic (pain relief) and diagnostic, allowing the referring provider to assess the patient’s pathology based on their pain response post-treatment.[11][12]
Shoulder pain can be complex and multifactorial. Clinicians use a combination of physical examination, history, and imaging to establish a differential diagnosis.[13][14] In some cases, MRI may identify multiple abnormal findings, and injections may help elucidate their clinical significance. For example, the MRI examination may identify a superior labral tear and biceps tendinosis in addition to a rotator cuff tear, but the physical examination is most consistent with rotator cuff pathology. The orthopedist may request a biceps tendon injection to determine if a biceps tenodesis at the time of rotator cuff repair is indicated.[6][15][16]
Contraindications
Absolute contraindications to corticosteroid injections include local infection and bacteremia. If the infusion is intra-articular, absolute contraindications would also include septic arthrosis and intra-articular fracture. In the setting of biceps tendon sheath injection, it should be noted that the biceps tendon sheath communicates with the glenohumeral joint. Therefore, medication injected into the biceps tendon sheath also extends to the joint. If the clinical indication is to assess for septic arthrosis or tenosynovitis, one must carefully evaluate the overlying soft tissues for signs of cellulitis. It is crucial to avoid contamination of the joint or tendon sheath by placing the needle through infected soft tissue before accessing the joint. Relative contraindications include local or juxta-articular osteoporosis, coagulopathy, or recent injection or multiple frequent injections, defined as 3 or more injections over the last year or within the prior 6 weeks.[17]
Equipment
Several varieties of steroids are available on the market today, including methylprednisolone acetate, triamcinolone, betamethasone acetate with betamethasone sodium phosphate, and dexamethasone sodium phosphate, each with its own strengths and weaknesses. The most commonly used steroids in the United States include methylprednisolone, triamcinolone hexacetonide, triamcinolone acetonide, and betamethasone.[18]
Of note, the equivalent potency of betamethasone and dexamethasone sodium phosphate is approximately 5 times that of the others. Solubility also varies between the steroid formulations. For example, the acetate portion of betamethasone is insoluble, while the sodium phosphate portion of betamethasone and dexamethasone sodium phosphate is freely water-soluble. Particle size varies from 0.5 micrometers for dexamethasone to over 500 micrometers for methylprednisolone acetate, and triamcinolone exhibits extensive particle aggregation, requiring meticulous mixing of the solution before injection.
Dosage varies based on the chosen steroid and the location treated, with small joints (metacarpophalangeal, facet, acromioclavicular) receiving higher amounts, and medium-sized joints (elbow, wrist) and larger joints (knee, shoulder, hip, ankle) receiving higher amounts. For example, while a large joint might require 40 to 80mg of methylprednisolone acetate, that same joint would only require 8 to 15 mg of dexamethasone sodium phosphate. Similarly, a small joint might require 4 to 10 mg of methylprednisolone acetate, while that same joint would only require 0.8 to 2 mg of dexamethasone sodium phosphate. Some examples of steroid mixtures used for biceps tendon sheath injection at our institution include 3.75 mg dexamethasone mixed with 2 ml 1% lidocaine or 1ml betamethasone (6 mg/ml) mixed with 2 ml 1% lidocaine.[19]
Before injecting the steroid, a local anesthetic is provided to the skin and superficial soft tissues using 1% lidocaine. Although around 5 to 7 mL is the typical amount for local anesthesia, it bears mentioning that the maximum safe dosage for lidocaine in the United States is 300 mg, which equates to 30 mL of 1% lidocaine.[18] Bupivacaine is an alternative medication that can be useful for anesthesia. Its long duration of action is advantageous, but it has shown the highest toxicity to chondrocytes of the local anesthetics. It should never be used for intraarticular injections.[11][12][18][20][21]
Preparation
As with every image-guided procedure, planning begins with reviewing the patient’s history, clinical indication, and relevant prior imaging, including plain film, ultrasound, CT, and MRI. After reviewing the history and available imaging, a decision should be made on whether the requested procedure is medically indicated and the best available to address the clinical concern. All medications should be reviewed, with specific attention to anticoagulation therapy, blood thinners (including fish oil and vitamin E), and aspirin. Risks and benefits of continuing or discontinuing anticoagulation should be considered on a case-by-case basis and may involve discussion with the prescribing provider.[5][22] Additionally, one needs to review the patient’s allergies to ensure there are no prior reactions to any planned medications, including skin-cleansing agents and adhesives.
Once the requested procedure is determined to be clinically indicated, the patient should be made aware of the risks, benefits, and alternatives. While nearly all musculoskeletal injections are considered low risk, some potential risks of ultrasound-guided procedures include pain, infection, bleeding, damage to nearby structures, allergic reaction, steroid flare, and failure to address the clinical concern (eg, failure to relieve pain). Additionally, if steroids are inadvertently injected into the subcutaneous soft tissues, atrophy of the subcutaneous fat or skin discoloration can occur. Although extremely rare, it has been documented in the literature that steroid injections can weaken tendons; thus, there is a theoretical risk of tendon rupture.[18] Once this discussion is completed and all the patient’s questions are answered to their satisfaction, written consent must be obtained. If the procedure is performed for pain relief, pre- and post-procedural pain levels should also be recorded to document an objective measure of symptomatic relief. Following the procedure and before releasing the patient from the radiology department, the patient is given return precautions, including signs of a post-procedural infection such as worsening pain beyond baseline, redness, swelling, and/or fever. Although exceedingly rare, an intraarticular joint infection would require urgent medical attention. Thus, patients are instructed to seek care at an urgent care center or the emergency department if symptoms occur outside normal business hours.
Technique or Treatment
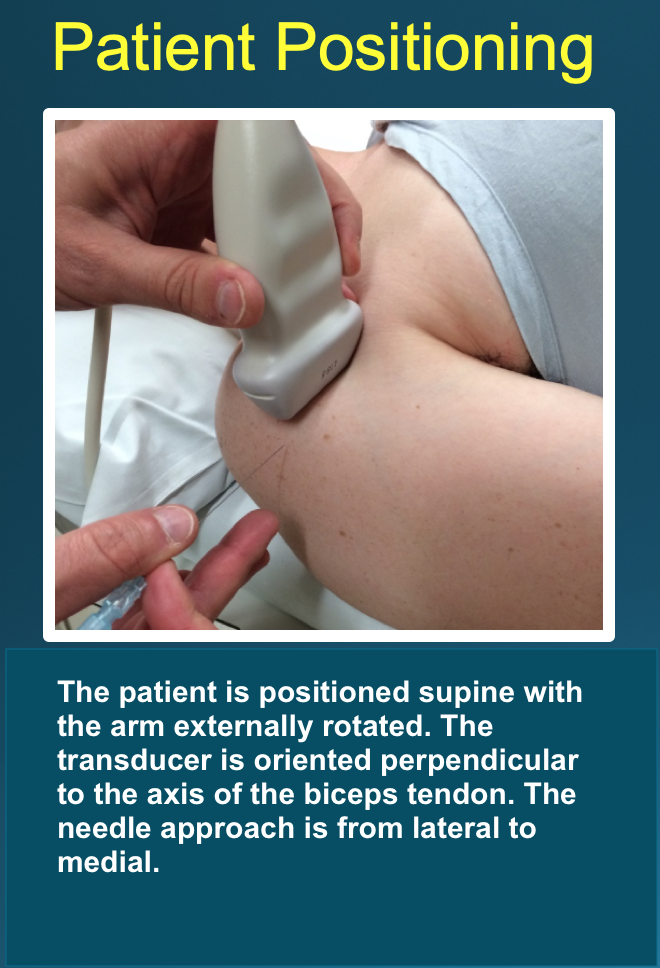
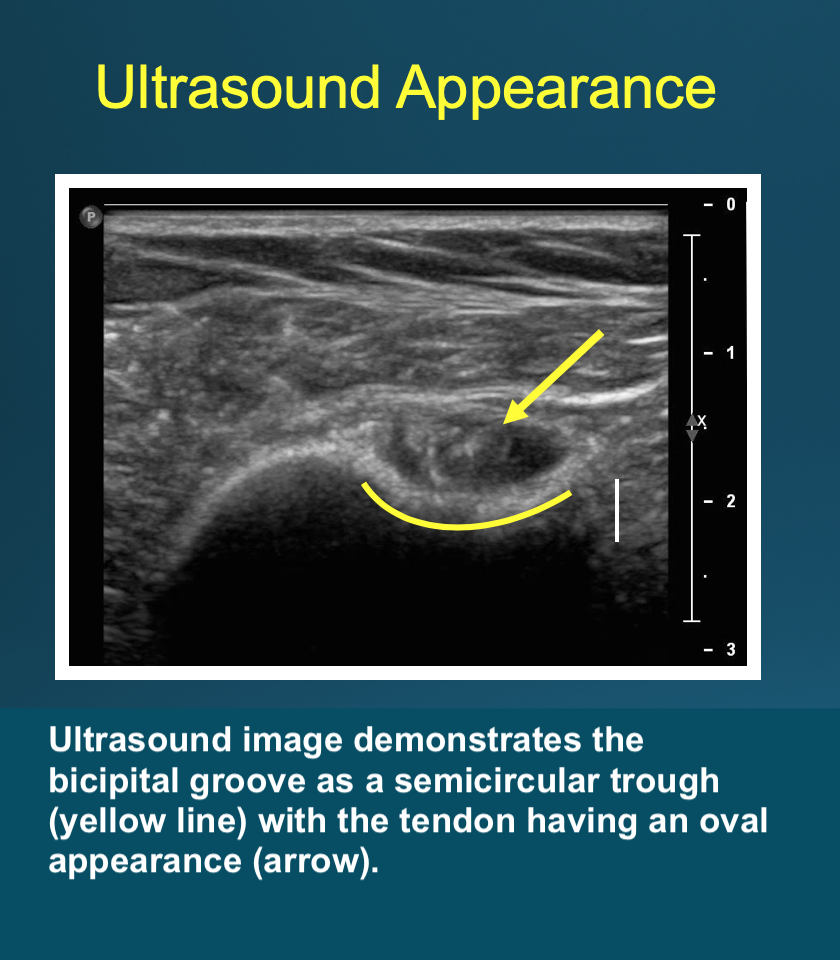
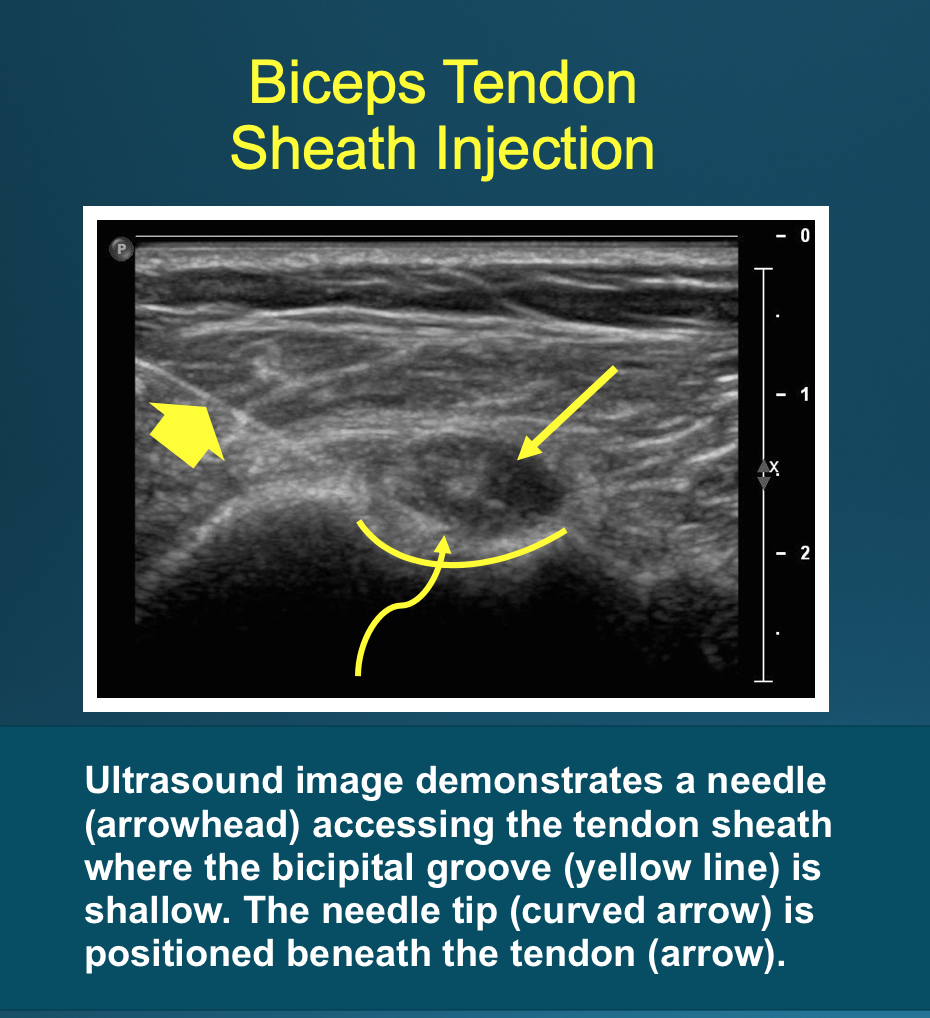
Optimal positioning can be patient-dependent; however, most patients are positioned supine with the arm externally rotated. The transducer is placed on the skin perpendicular to the axis of the biceps tendon (see Image. Patient Positioning). This results in an image in which the bicipital groove appears as a semicircular trough, with the tendon appearing circular or oval (see Image: Ultrasound Appearance). The approach is from lateral to medial with an in-plane technique. The patient’s skin is marked at the planned injection site. The skin is then prepped and draped in a sterile fashion. A sterile ultrasound probe cover is placed on the selected probe. The subcutaneous soft tissues are then infiltrated with 1% lidocaine as the needle is advanced towards the biceps tendon under ultrasound guidance. Optimally, one should enter the tendon sheath in an area where the bicipital groove is shallow, allowing the needle to be positioned somewhat parallel to the transducer. The more parallel the needle is to the transducer, the more clearly it can be visualized on ultrasound. A steeper approach leads to decreased reflection of sound waves returning to the transducer and poorer visualization. If the needle tip is positioned superficial to the tendon, the subdeltoid bursa can fill with fluid mimicking the tendon sheath; thus, the ideal positioning is beneath the tendon to avoid this pitfall (see Image. Biceps Tendon Sheath Injection).
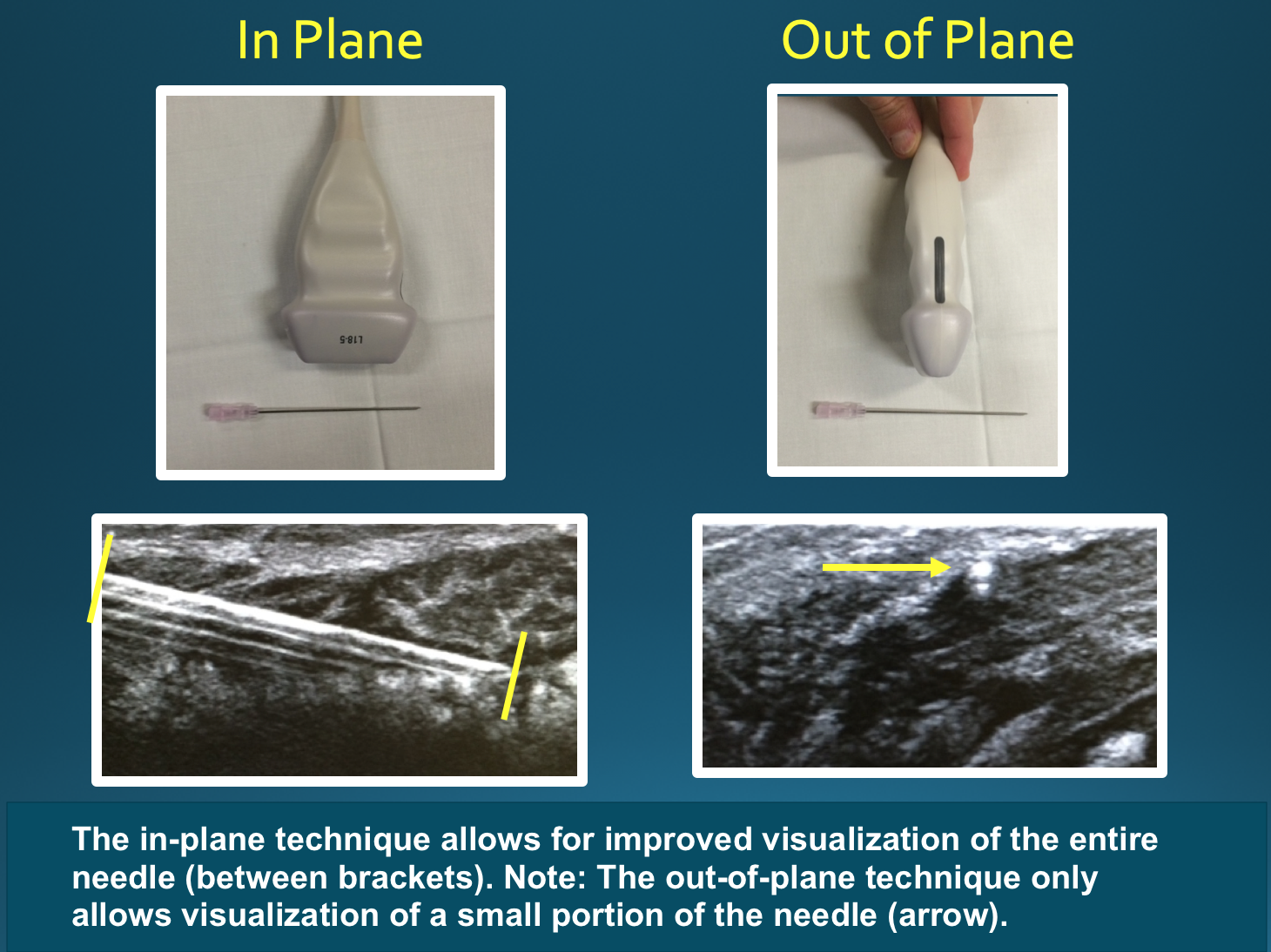
The in-plane technique, in which the needle is parallel to the transducer, provides improved visualization of the entire needle and reduces the risk of damage to surrounding structures. If using an out-of-plane technique, one would only see a small portion of the needle, making it difficult to appreciate the needle tip's position (see Image: Ultrasound Techniques). Some options to increase needle visibility include beam steering, heel-toe maneuver, using a larger-gauge needle, and entering the skin farther from the target, which allows for a more parallel orientation but a longer needle path.[23][24]
Given the superficial nature of the biceps tendon, the use of a higher frequency ultrasound transducer (10 to 15 MHz) allows for better near-field resolution. The probe should be maintained perpendicular to the tendon to maximize the reflection of sound beams and reduce anisotropy, which can result in poor tendon visualization.
Complications
Potential complications include pain, infection, bleeding, damage to nearby structures, allergic reaction, and non-therapeutic results. Complications specific to steroid use include septic arthritis, post-injection flare, local tissue atrophy, skin discoloration, tendon rupture, cartilage damage, avascular necrosis, flushing, and increased blood glucose level. If inadvertently injected intravascularly, there can be severe CNS and cardiac effects, particularly with insoluble, particulate formulations such as triamcinolone, which can embolize and lead to stroke.[18] As mentioned previously, the maximum safe dose of lidocaine in the ultrasound is 300 mg or 30 ml of 1% lidocaine. Above this threshold, there is a risk of CNS, cardiac, and skeletal muscle toxicity. Local anesthetics are toxic to chondrocytes in both animal studies and in vitro studies using human chondrocytes; bupivacaine is the most chondrotoxic, and ropivacaine the least. Lidocaine is most often used because it is the least expensive and most readily available.[20][21]
Enhancing Healthcare Team Outcomes
As mentioned above, shoulder pain is often multifactorial in etiology. Often, the radiologist and orthopedist work together to determine the underlying cause of a patient’s pain. A patient typically presents initially to their primary care provider, and if clinically indicated, they may be referred to an orthopedic specialist for further evaluation. Considering the patient’s history and physical exam findings, further evaluation with diagnostic imaging is sometimes indicated to evaluate for underlying pathology. It is not uncommon for imaging evaluation, such as MRI, to demonstrate multiple abnormalities, any of which could be causing the patient’s pain. In these cases, it can help perform a diagnostic and sometimes therapeutic injection to help clarify the clinical significance of the imaging findings. If a patient experiences pain relief after a targeted injection, it can be inferred that the treated area was a pain generator. Alternatively, if the patient does not have pain relief, one can infer that this area was not a pain generator. The patient’s response is clinically important as it can guide what surgical procedures, if any, may be offered for symptomatic relief. It can also help a patient avoid unnecessary surgical procedures. Orthopedic nurses set up the procedure, assist during the procedure, and provide patient instruction. Physical therapy may be needed to assist with post-procedure recovery exercises and to strengthen the muscles around the shoulder joint. These disciplines need to function as an interprofessional team to achieve optimal patient outcomes from this procedure.
Media
(Click Image to Enlarge)
Patient Positioning.
Contributed by D Byerly, MD
(Click Image to Enlarge)
Ultrasound Appearance.
Contributed by D Byerly, MD
(Click Image to Enlarge)
Biceps Tendon Sheath Injection.
Contributed by D Byerly, MD
(Click Image to Enlarge)
Ultrasound Techniques.
Contributed by D Byerly, MD
References
Yiannakopoulos CK, Megaloikonomos PD, Foufa K, Gliatis J. Ultrasound-guided versus palpation-guided corticosteroid injections for tendinosis of the long head of the biceps: A randomized comparative study. Skeletal radiology. 2020 Apr:49(4):585-591. doi: 10.1007/s00256-019-03315-9. Epub 2019 Nov 12 [PubMed PMID: 31712838]
Level 2 (mid-level) evidenceMonseau AJ, Nizran PS. Common injections in musculoskeletal medicine. Primary care. 2013 Dec:40(4):987-1000, ix-x. doi: 10.1016/j.pop.2013.08.012. Epub 2013 Sep 24 [PubMed PMID: 24209729]
Sánchez Barrancos IM, Manso García S, Lozano Gago P, Hernández Rodríguez T, Conangla Ferrín L, Ruiz Serrano AL, González Santisteban R. [Usefulness and reliabitlity of musculoskeletal point of care ultrasound in family practice (2): Muscle injuries, osteoarthritis, rheumatological diseases and eco-guided procedures]. Atencion primaria. 2019 Feb:51(2):105-117. doi: 10.1016/j.aprim.2018.07.011. Epub 2018 Dec 24 [PubMed PMID: 30591207]
Chen KC, Lin AC, Chong CF, Wang TL. An overview of point-of-care ultrasound for soft tissue and musculoskeletal applications in the emergency department. Journal of intensive care. 2016:4():55. doi: 10.1186/s40560-016-0173-0. Epub 2016 Aug 15 [PubMed PMID: 27529031]
Level 3 (low-level) evidenceSorensen B, Hunskaar S. Point-of-care ultrasound in primary care: a systematic review of generalist performed point-of-care ultrasound in unselected populations. The ultrasound journal. 2019 Nov 19:11(1):31. doi: 10.1186/s13089-019-0145-4. Epub 2019 Nov 19 [PubMed PMID: 31749019]
Level 1 (high-level) evidenceWittich CM, Ficalora RD, Mason TG, Beckman TJ. Musculoskeletal injection. Mayo Clinic proceedings. 2009 Sep:84(9):831-6; quiz 837. doi: 10.4065/84.9.831. Epub [PubMed PMID: 19720781]
Daniels EW, Cole D, Jacobs B, Phillips SF. Existing Evidence on Ultrasound-Guided Injections in Sports Medicine. Orthopaedic journal of sports medicine. 2018 Feb:6(2):2325967118756576. doi: 10.1177/2325967118756576. Epub 2018 Feb 22 [PubMed PMID: 29511701]
Adler RS, Sofka CM. Percutaneous ultrasound-guided injections in the musculoskeletal system. Ultrasound quarterly. 2003 Mar:19(1):3-12 [PubMed PMID: 12970612]
Soh E, Li W, Ong KO, Chen W, Bautista D. Image-guided versus blind corticosteroid injections in adults with shoulder pain: a systematic review. BMC musculoskeletal disorders. 2011 Jun 25:12():137. doi: 10.1186/1471-2474-12-137. Epub 2011 Jun 25 [PubMed PMID: 21702969]
Level 1 (high-level) evidenceKumar Sahu A, Rath P, Aggarwal B. Ultrasound-guided injections in musculo-skeletal system - An overview. Journal of clinical orthopaedics and trauma. 2019 Jul-Aug:10(4):669-673. doi: 10.1016/j.jcot.2019.05.013. Epub 2019 May 22 [PubMed PMID: 31316237]
Level 3 (low-level) evidenceLenz R, Kieb M, Diehl P, Grim C, Vogt S, Tischer T. [Muscle, tendon and joint injections : What is the evidence?]. Der Orthopade. 2016 May:45(5):459-68. doi: 10.1007/s00132-016-3262-9. Epub [PubMed PMID: 27147429]
Barile A, La Marra A, Arrigoni F, Mariani S, Zugaro L, Splendiani A, Di Cesare E, Reginelli A, Zappia M, Brunese L, Duka E, Carrafiello G, Masciocchi C. Anaesthetics, steroids and platelet-rich plasma (PRP) in ultrasound-guided musculoskeletal procedures. The British journal of radiology. 2016 Sep:89(1065):20150355. doi: 10.1259/bjr.20150355. Epub 2016 Jul 7 [PubMed PMID: 27302491]
Larson HM, O'Connor FG, Nirschl RP. Shoulder pain: the role of diagnostic injections. American family physician. 1996 Apr:53(5):1637-47 [PubMed PMID: 8623691]
Nelson KH, Briner W Jr, Cummins J. Corticosteroid injection therapy for overuse injuries. American family physician. 1995 Nov 1:52(6):1811-6 [PubMed PMID: 7484691]
Zuckerman JD, Meislin RJ, Rothberg M. Injections for joint and soft tissue disorders: when and how to use them. Geriatrics. 1990 Apr:45(4):45-52, 55 [PubMed PMID: 2180787]
Leversee JH. Aspiration of joints and soft tissue injections. Primary care. 1986 Sep:13(3):579-99 [PubMed PMID: 3538090]
Conway R, O'Shea FD, Cunnane G, Doran MF. Safety of joint and soft tissue injections in patients on warfarin anticoagulation. Clinical rheumatology. 2013 Dec:32(12):1811-4. doi: 10.1007/s10067-013-2350-z. Epub 2013 Aug 8 [PubMed PMID: 23925554]
Level 2 (mid-level) evidenceMacMahon PJ, Eustace SJ, Kavanagh EC. Injectable corticosteroid and local anesthetic preparations: a review for radiologists. Radiology. 2009 Sep:252(3):647-61. doi: 10.1148/radiol.2523081929. Epub [PubMed PMID: 19717750]
Skedros JG, Hunt KJ, Pitts TC. Variations in corticosteroid/anesthetic injections for painful shoulder conditions: comparisons among orthopaedic surgeons, rheumatologists, and physical medicine and primary-care physicians. BMC musculoskeletal disorders. 2007 Jul 6:8():63 [PubMed PMID: 17617900]
Freire V, Bureau NJ. Injectable Corticosteroids: Take Precautions and Use Caution. Seminars in musculoskeletal radiology. 2016 Nov:20(5):401-408. doi: 10.1055/s-0036-1594286. Epub 2016 Dec 21 [PubMed PMID: 28002861]
McColl GJ, Dolezal H, Eizenberg N. Common corticosteroid injections. An anatomical and evidence based review. Australian family physician. 2000 Oct:29(10):922-6 [PubMed PMID: 11059079]
Jaffe TA, Raiff D, Ho LM, Kim CY. Management of Anticoagulant and Antiplatelet Medications in Adults Undergoing Percutaneous Interventions. AJR. American journal of roentgenology. 2015 Aug:205(2):421-8. doi: 10.2214/AJR.14.13342. Epub [PubMed PMID: 26204296]
Geannette C, Williams D, Berkowitz J, Miller TT. Ultrasound-Guided Biceps Tendon Sheath Injection: Spectrum of Preprocedure Appearances. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2019 Dec:38(12):3267-3271. doi: 10.1002/jum.15062. Epub 2019 Jun 11 [PubMed PMID: 31187487]
Gofeld M, Hurdle MF, Agur A. Biceps Tendon Sheath Injection: An Anatomical Conundrum. Pain medicine (Malden, Mass.). 2019 Jan 1:20(1):138-142. doi: 10.1093/pm/pny051. Epub [PubMed PMID: 29635324]