 Calcium Homeostasis and Disorders: An Integrated Clinical and Laboratory Approach
Calcium Homeostasis and Disorders: An Integrated Clinical and Laboratory Approach
Introduction
Calcium is a vital element in the body, playing a critical role in numerous biochemical processes. Calcium is essential for proper cardiac function, maintenance of bone structural integrity, muscular contraction, and enzymatic signaling in biochemical pathways.[1] Serum calcium is tightly regulated by parathyroid hormone (PTH), calcitonin, and calcitriol. Dietary intake serves as the primary source of calcium, while gastrointestinal absorption is regulated mainly by calcitriol (1,25-dihydroxyvitamin D3), with PTH acting indirectly to modulate this process.[2]
Serum calcium may be measured using a venous sample, with physiologic concentrations ranging from 8.8 mg/dL to 10.4 mg/dL for total calcium and 4.7 mg/dL to 5.2 mg/dL for ionized calcium.[3] Total calcium values should be corrected for the current albumin concentration, as albumin serves as a carrier protein and may influence reported results. Urinary calcium assessment may include measurement of urinary calcium concentration (UCa), calculation of the urinary calcium-to-creatinine ratio (UCa:UCr), or determination of fractional excretion of calcium (FeCa). Calcium imbalances may result from various diseases or therapeutic interventions that alter hormone secretion, receptor responsiveness, intestinal absorption, or renal calcium handling.[4] Laboratory error may lead to inaccurately reported calcium levels, necessitating preventive measures during specimen collection and analysis.
Etiology and Epidemiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology and Epidemiology
Calcium is the 5th most abundant element in the human body and a major structural mineral in bone. An average 70-kg human body contains approximately 1 kg, or about 25 mol, of calcium. The skeleton stores approximately 99% of total body calcium, predominantly as extracellular crystals of unknown structure and a composition approaching hydroxyapatite. Soft tissues and extracellular fluid contain the remaining 1% of total body calcium. Virtually all calcium in the blood is present in plasma.[5]
Approximately 50% of circulating calcium exists in the free, or ionized, form. About 40% of serum calcium is protein-bound, primarily to albumin (80%) and, to a lesser extent, globulins (20%), while approximately 10% exists in complexes with small diffusible inorganic and organic anions (eg, bicarbonate, lactate, citrate). The free calcium fraction is biologically active.[6] Calcium binding to negatively charged protein sites is pH-dependent. Alkalosis increases the negative charge of proteins, thereby increasing calcium binding and reducing free calcium concentrations. Conversely, acidosis decreases the negative charge, reducing calcium binding and increasing free calcium concentrations.[7] In vitro, a 0.1-unit increase in pH is associated with an approximate 0.2 mg/dL (0.05 mmol/L) decrease in ionized calcium, and vice versa.[8] Redistribution of calcium among the 3 plasma pools may occur acutely or chronically due to alterations in protein and small anion concentrations, changes in pH, or shifts in free and total plasma calcium concentrations.[9]
Calcium is physiologically classified as intracellular or extracellular. Intracellular calcium plays a key role in numerous physiologic functions, including muscle contraction, hormone secretion, glycogen metabolism, and cell division. The intracellular calcium concentration within the cytosol of unstimulated cells is approximately 0.1 μmol/L, representing less than 1/20,000 of the concentration in extracellular fluid.[10] Extracellular calcium supplies the calcium ions necessary for maintaining intracellular calcium homeostasis, bone mineralization, blood coagulation, and plasma membrane potential.[11] Calcium stabilizes plasma membranes and influences membrane permeability and excitability. A reduction in plasma-free calcium concentration increases neuromuscular excitability and may result in tetany, whereas an elevated concentration reduces neuromuscular excitability.[12]
Pathophysiology
Calcium is tightly regulated and rarely deviates from physiologic concentrations within the body. Maintenance of calcium homeostasis is essential because calcium participates in numerous critical cellular functions.
PTH, calcitonin, and calcitriol actively regulate calcium levels. The hormone serves as an essential regulator of calcium homeostasis and acts on the renal, skeletal, and gastrointestinal systems to increase serum calcium concentrations. First, PTH promotes intestinal calcium absorption by stimulating renal production of calcitriol, which increases intestinal calcium absorption.[13] Second, the hormone stimulates bone resorption by increasing osteoclast number and activity. Lastly, PTH enhances renal calcium reabsorption by activating adenylyl cyclase in the distal nephron.[14]
PTH is regulated by serum calcium via negative feedback, preventing excessive hormone secretion when calcium is at physiologic levels (≈ 10 mg/dL). Calcium-sensing receptors (CaSRs) in the parathyroid glands continuously monitor serum calcium concentrations and regulate PTH secretion. Genetic mutations affecting CaSRs, such as those observed in familial hypocalciuric hypercalcemia, alter receptor sensitivity to serum calcium levels, resulting in hypocalcemia or hypercalcemia. Calcitonin is secreted by the parafollicular C-cells of the thyroid gland in response to elevated serum calcium levels and inhibits osteoclast activity while decreasing calcium absorption in the intestines and kidneys.[15] The overall effect is a reduction in serum calcium levels.
Calcium and the Renal System
PTH acts on the renal system by activating adenylyl cyclase and 1α-hydroxylase to increase calcium reabsorption and phosphate excretion. Adenylyl cyclase enhances calcium reabsorption in the distal convoluted tubules. 1α-hydroxylase increases the conversion of vitamin D to its active form, calcitriol, resulting in increased intestinal calcium absorption.[16] PTH activity may become attenuated in chronic kidney disease (CKD), leading to hypocalcemia, hyperphosphatemia, and secondary hyperparathyroidism.
Calcium and the Gastrointestinal System
Humans do not endogenously produce calcium. Therefore, this mineral must be ingested and absorbed through the gastrointestinal tract. Calcium levels and calcitriol regulate intestinal calcium absorption. Additional factors, including age, gender, race, and comorbidities, may influence calcium absorption efficiency. Calcitriol increases in response to low serum calcium and stimulates active calcium transport in the duodenum. Elevated serum calcium suppresses this active transport mechanism, and calcium absorption then occurs passively in the jejunum and ileum, resulting in reduced overall absorption efficiency. Calcium is absorbed in ionic form. Therefore, dietary constituents that bind calcium, primarily oxalate, phosphate, sulfate, citrate, fiber, and fats, reduce the amount available for absorption.
Calcium and the Musculoskeletal System
Bone tissue stores calcium as hydroxyapatite, which is deposited when serum calcium levels are elevated and released when levels are reduced. This process is regulated through endocrine signaling involving the thyroid and parathyroid glands. Elevated serum calcium stimulates calcitonin release from the thyroid gland, which inhibits bone resorption by suppressing osteoclast activity. The effects of PTH on bone tissue depend on exposure pattern, particularly continuous versus intermittent exposure.[17] Continuous PTH exposure promotes osteoclast activation through upregulation of RANKL (receptor activator of nuclear factor κB Ligand), increasing bone resorption and calcium mobilization, thereby contributing to an osteoporotic state. Intermittent PTH exposure favors osteoblast activation and promotes bone formation. Chronically reduced PTH levels result in decreased bone remodeling and, subsequently, weak and brittle bone architecture.[18]
Calcium is essential for muscle contraction. Actin and myosin subunits interact to generate contraction, while troponin and tropomyosin function as regulatory inhibitory proteins. Tropomyosin blocks the actin-myosin binding site, preventing contraction by inhibiting actin–myosin interaction.[19] Muscle contraction occurs when calcium released from the sarcoplasmic reticulum binds to troponin, displacing tropomyosin from the binding site and permitting actin–myosin interaction.[20]
Calcium and the Cardiovascular System
Calcium stabilizes the membrane potential in cardiac myocytes. Calcium influx through L-type calcium channels during the plateau phase of the cardiac action potential promotes myocardial contraction, while the sinoatrial node pacemaker potential is primarily regulated by the funny current and calcium channel activity. Dysregulation of calcium or potassium homeostasis can disrupt this balance. Electrocardiographic evaluation is indicated in severe hyperkalemia to assess for characteristic abnormalities. Calcium gluconate administration helps stabilize the myocardium and reduce susceptibility to cardiac dysrhythmias in this setting.[21]
Prospective cohort studies have demonstrated no association between dietary calcium intake and the risk of heart disease, mortality, or myocardial infarction.[22] Study findings are inconclusive regarding potential differences in cardiovascular risk between dietary calcium and calcium supplementation. Further investigation is required to clarify the role of calcium supplementation in cardiovascular disease prevention.[23]
Calcium serves as a key cofactor in the coagulation cascade and is required for normal hemostasis. During primary hemostasis, von Willebrand factor is released from injured tissue and acts as a bridge between the endothelium and platelet glycoprotein Ib receptors, facilitating platelet adhesion. Calcium is released to support downstream coagulation factor activity within the clotting cascade following platelet adhesion to the endothelium.[24] Tissue factor released from subendothelial tissue binds calcium and factor VII, promoting thrombin formation. Calcium also contributes to the assembly of the prothrombinase complex, which converts prothrombin to thrombin and facilitates the formation of insoluble fibrin.[25] A study of intracerebral hemorrhage involving 2,103 patients demonstrated that hypocalcemia was associated with subtle coagulopathy and correlated with increased bleeding in patients with intracerebral hemorrhage.[26]
Specimen Requirements and Procedure
Fasting is not required for the evaluation of serum calcium levels. Calcium is included in the comprehensive metabolic panel, allowing routine assessment. Fist clenching or forearm exercise may falsely elevate ionized (free) calcium levels. The sample should be collected with the patient seated, as standing increases total calcium concentration.[27] Hemolysis and delayed plasma or serum separation result in decreased calcium concentrations. Samples collected in tubes containing citrate, oxalate, or ethylenediaminetetraacetic acid (EDTA) are unsuitable for calcium analysis.[28]
A venous blood sample is required for serum calcium assessment. In pediatric patients, capillary blood may be obtained from the finger using a lancet and collected into a pipette, slide, or test strip. Whole blood specimens should be analyzed within 15 to 30 minutes of collection. When immediate analysis is not possible, specimens should be kept on ice. Stability on ice is maintained for at least 2 hours. However, concurrent potassium testing from the same specimen may be affected, as low temperature may cause a spurious increase in potassium within 1 hour of collection. Serum is the preferred specimen type when analysis cannot be performed within 1 hour. Specimens should be centrifuged, and serum or plasma should be separated from cellular components within 2 hours of collection.[29]
Samples may be stored at room temperature for up to 8 hours or refrigerated at 2 °C to 8 °C for up to 48 hours. Freezing at −15 °C to −20 °C is recommended when assays are not completed within 48 hours or when separated samples require storage beyond 48 hours. Frozen samples should be thawed only once. Repeated freeze–thaw cycles may result in analyte degradation.[30]
Urinary calcium may be kept in solution by adding 10 mL of 6 mol hydrochloric acid to the collection container prior to a 24-hour urine collection. Urine should be well mixed throughout the collection period. A 24-hour urine collection, timed specimen, or random urine sample may assist in the evaluation of metabolic abnormalities and stone-forming propensity.[31] Urinary calcium may be evaluated by measuring UCa, calculating UCa:UCr, or determining FeCa. A UCa:UCr below approximately 0.20 mg/mg is generally considered within the normal adult range, whereas values above 0.20 mg/mg suggest hypercalciuria. Population- and age-specific reference intervals, particularly in pediatric populations, should be considered.[32]
FeCa also aids in the assessment of abnormal calcium metabolism, and is calculated as follows:
FeCa = (UCa x Serum creatinine) / (Serum calcium × Urinary creatinine)
However, simultaneous urine and serum measurements are required for calculation.[33] This requirement limits FeCa utility in routine practice, particularly when urine and serum sampling cannot be precisely synchronized.
Testing Procedures
Total calcium is commonly measured using spectrophotometric methods, including the o-cresolphthalein complexone and Arsenazo III methods, atomic absorption spectrometry, and, less commonly, isotope dilution mass spectrometry.[34] In contrast, ionized calcium is measured in whole blood using the ion-selective electrode (ISE) potentiometric method.[35]
The free calcium analyzer consists of a microprocessor-controlled pump system that transports calibration solutions, samples, and wash solutions through a measuring cell containing calcium ion–selective, reference, and pH electrodes. Voltage differences between calcium or pH electrodes and the reference electrode are measured using sensitive potentiometric systems for calibration solutions and patient samples. A microprocessor performs calibration and calculates calcium concentration and pH. Most instruments simultaneously measure ionized calcium and pH at 37 °C.[36]
Calcium ISEs contain a calcium-selective membrane enclosing an inner reference solution of calcium chloride, often containing saturated silver chloride and physiologic concentrations of sodium chloride and potassium chloride, along with an internal reference electrode. The reference electrode, typically silver–silver chloride, is immersed in the inner reference solution. Modern calcium ISEs utilize liquid membranes containing an ion-selective calcium sensor dissolved in an organic liquid embedded within a polymeric matrix.[37] Results are influenced by the ionic strength of the specimen since ISEs measure ion activity. Free calcium analyzers, along with their calibrators, are optimized for serum, plasma, or whole blood specimens. Since the ionic strength of these fluids is primarily determined by sodium and chloride concentrations, calibrators are typically prepared in buffer and sodium chloride to achieve a final ionic strength of approximately 160 mmol/kg.[38]
Although the range of sodium and chloride concentrations typically present in serum or plasma does not produce clinically significant inaccuracy in free calcium measurement, substantial errors may occur in other specimen types unless matrix composition and calibrator ionic strength are closely matched. Modern electrodes demonstrate high selectivity for calcium over sodium, potassium, magnesium, hydrogen, and lithium ions.[39]
Interfering Factors
Reported calcium levels may be influenced by multiple factors, including patient age, comorbidities, lifestyle, sex, medical therapies, and conditions during specimen collection. Poor specimen quality, such as lipemic or hemolyzed samples, may produce inaccurate calcium measurements.[40] Exercise immediately prior to blood draw has also been shown to increase calcium levels.[41]
The use of certain medications may cause erroneous calcium measurements. Perchlorate has been reported to produce discrepancies in ionized calcium measurements, resulting in false diagnoses of hypocalcemia or hypercalcemia.[42] Medications associated with increased serum calcium levels include thiazide diuretics, lithium, antacids, and vitamin D supplements.[43]
Urinary calcium excretion is closely related to sodium excretion, with dietary sodium intake influencing reported calcium levels. High-sodium diets increase urinary calcium excretion, whereas low-sodium diets reduce urinary calcium excretion.[44] Clinical interpretation should account for age-related differences, as children exhibit higher UCa:UCr and may be incorrectly classified as hypercalciuric if adult reference thresholds are applied.[45]
Albumin serves as a carrier protein for calcium and may lead to inaccurately reported total serum calcium levels. Evaluation of albumin concentration is important for correcting total calcium and distinguishing true from artifactual calcium abnormalities.[46] The correction equation is as follows:
Adjusted total calcium (mg/dL) = Total calcium (mg/dL) + 0.8 × [4.0 – serum albumin (g/dL)]
Hypoalbuminemia is the most likely cause of artifactual hypocalcemia if albumin-corrected total serum calcium falls within the normal range (8.8 to 10.4 mg/dL) despite a low reported value.[47]
Results, Reporting, and Critical Findings
Hypercalcemia
Hypercalcemia is defined by serum calcium levels above 10.4 mg/dL or ionized calcium levels above 5.2 mg/dL. Patients with hypercalcemia may present with a range of symptoms, including nephrolithiasis, bone fragility and fractures, abdominal pain, constipation, polydipsia, polyuria, and, in severe cases, altered mental status. Clinical findings may include tongue fasciculations, bradycardia, or hyperreflexia.[48]
Initial evaluation of hypercalcemia requires confirmation with albumin-corrected calcium. Serum PTH levels should be measured following confirmation. Elevated PTH indicates PTH-dependent hypercalcemia, which may result from primary hyperparathyroidism, familial hypocalciuric hypercalcemia, or medication-related effects. Suppressed PTH indicates PTH-independent hypercalcemia, which has a broader differential diagnosis. Evaluation should include PTH-related peptide, 25-hydroxyvitamin D3 (calcidiol), and calcitriol levels. Causes of PTH-independent hypercalcemia include immobilization, malignancy, thyrotoxicosis, and vitamin D toxicity.[49]
Patients who are asymptomatic with albumin-corrected calcium levels below 12 mg/dL should be advised to avoid precipitating conditions, such as dehydration, inactivity, dietary calcium intake exceeding 1000 mg/day, and certain medications, including lithium carbonate and thiazides.[50] Patients with albumin-corrected calcium levels above 12 mg/dL may present with mild, moderate, or severe symptoms.[51] Patients with chronic mild hypercalcemia may not require immediate treatment. However, albumin-corrected calcium levels greater than 14 mg/dL require urgent evaluation and management.
The initial management of hypercalcemia includes administration of normal saline, which provides the most effective early therapeutic intervention. The addition of calcitonin produces a reduction in serum calcium within approximately 48 hours. Bisphosphonate therapy provides a more sustained effect, with serum calcium reduction typically occurring within 2 to 4 days.[52] Patients who have renal failure or do not respond to bisphosphonate therapy may be managed with denosumab. This agent suppresses bone remodeling and may induce hypocalcemia, requiring monitoring of serum calcium and calcidiol levels.[53] Hemodialysis is a last-line intervention for severe hypercalcemia, particularly in malignancy-associated cases with concurrent renal insufficiency.[54] Careful monitoring is required to prevent fluid overload, especially in patients with reduced cardiac reserve and renal insufficiency.[55]
Hypocalcemia
Hypocalcemia is characterized by total serum calcium levels below 8.8 mg/dL or ionized calcium levels below 4.7 mg/dL.[56] Due to multiple etiologic factors, patients with hypocalcemia require careful evaluation incorporating laboratory values, clinical presentation, symptoms, medications, and comorbidities. Initial assessment of this electrolyte deficiency requires confirmation using albumin-corrected calcium. Early manifestations of hypocalcemia include neuromuscular irritability, presenting as perioral and fingertip tingling and numbness, distal extremity paresthesia, and painful muscle cramps.[57]
Physical examination findings may include contraction of ipsilateral facial muscles elicited by tapping over the facial nerve, known as the Chvostek sign. Another is carpal spasm induced by inflation of a blood pressure cuff to 20 mm Hg above systolic pressure, producing wrist flexion and interphalangeal joint extension, known as the Trousseau sign (see Image. Chvostek And Trousseau Signs).[58] Acute and chronic hypocalcemia present with distinct clinical features. Acute hypocalcemia is more commonly associated with cardiac manifestations, including QT prolongation and T-wave abnormalities. Chronic hypocalcemia may present with dermatologic findings, including dry skin, coarse hair, and brittle nails, as well as neurologic complications such as intracranial calcification.[59]
Hypocalcemia may result from diseases, treatments, medications, and electrolyte abnormalities. Metabolic alkalosis reduces serum ionized calcium due to increased binding of calcium to albumin in alkalotic states. Chronic conditions associated with hypocalcemia include hypoparathyroidism, CKD, liver disease, and vitamin D deficiency.[60] Acute conditions such as sepsis, pancreatitis (due to fat saponification), and acute kidney injury may also result in hypocalcemia. Severe hypomagnesemia may cause secondary hypocalcemia, as observed in some cases associated with proton pump inhibitor therapy. Proton pump inhibitors also reduce gastric acidity, thereby decreasing intestinal calcium absorption. A 2017 case report described 2 pediatric patients on dialysis for CKD who developed acute hypocalcemia and alkalotic episodes a week after initiation of sodium polystyrene sulfonate for hyperkalemia management.[61]
Other medications associated with hypocalcemia include corticosteroids and antiepileptics, typically with long-term use, as well as aminoglycosides, cisplatin, and bisphosphonates. Acute hypocalcemia is common in patients receiving large-volume blood transfusions, such as during the management of traumatic hemorrhage, due to citrate-mediated calcium chelation. Given the essential role of calcium in coagulation, patients with trauma receiving transfusions require close monitoring to prevent severe hypocalcemic events.[62]
Treatment of hypocalcemia depends on symptom severity. Patients with mild symptoms may be treated with calcitriol 0.5 mcg orally twice daily and elemental calcium, typically as calcium carbonate 500 mg orally 4 times daily to optimize absorption. Multiple formulations and routes of calcium administration are available. Calcium carbonate may be administered orally as tablets or as a crushed preparation mixed with liquid. Absorption of calcium carbonate depends on gastric acidity. Absorption may improve with food administration or substitution with calcium citrate, which is less dependent on gastric acidity.[63] Persistent hypocalcemia should prompt evaluation for hypomagnesemia, which must be corrected to restore normal serum calcium levels.
Calcium gluconate is available in liquid form. Maintenance of serum calcium above 8 mg/dL (2 mmol/L) is essential in severely symptomatic patients with hypocalcemia. Calcium gluconate may be administered as a continuous intravenous infusion over 10 to 20 minutes to reduce the risk of cardiac complications, including arrhythmias.[64] Serum calcium should be evaluated every 3 to 6 months, with 24-hour UCa assessment performed annually. Phosphate binders should be administered in patients with comorbid hyperphosphatemia to prevent calcium phosphate precipitation and soft-tissue calcification.
Hypocalciuria
Hypocalciuria may result from medications, diseases, and genetic disorders. Common medications associated with reduced urinary calcium excretion include thiazides and estrogen. Genetic conditions, such as FHH, an autosomal dominant disorder characterized by decreased sensitivity of CaSRs in the parathyroid gland, maintain an elevated serum calcium baseline with associated hypocalciuria.[65] Another genetic cause includes Gitelman syndrome, a salt-wasting tubulopathy presenting with muscle spasms, weakness, and salt craving, along with multiple electrolyte abnormalities, including hypocalciuria.[66] The differential diagnosis also includes hypoparathyroidism, pseudohypoparathyroidism, intestinal malabsorption, rickets, and hypothyroidism.[67]
Hypercalciuria
Hypercalciuria may result from the use of certain medications, as well as the effects of diseases and genetic disorders. Common medications associated with increased urinary calcium excretion include spironolactone, corticosteroids, and acetazolamide.[68] Calcium-containing supplements should also be considered as a contributing factor. The differential diagnosis includes hyperparathyroidism, malignancy, multiple myeloma, sarcoidosis, Paget disease, increased intestinal absorption, and osteoporosis.[69]
Clinical Significance
Calcium dysregulation may reflect underlying disease and may also contribute to a range of adverse effects. The following section highlights multiple organ systems in which calcium is associated with pathologic processes.
Osteoporosis
Osteoporosis is a disorder affecting bone composition, with resultant reductions in bone density and mineralization. Clinical consequences include progressive bone loss leading to fragility and, ultimately, fractures. Approximately 1.5 million fractures occur annually due to osteoporosis, a condition affecting more than 10 million adults in the US, the majority of whom are women.[70] Osteoporosis is frequently underdiagnosed and undertreated in men, resulting in higher mortality following hip fractures. Adequate dietary calcium and vitamin D intake from childhood through early adulthood contributes to the attainment of peak bone mass and delays age-related bone loss. For osteoporosis prevention, the American College of Obstetricians and Gynecologists recommends calcium and vitamin D supplementation beginning as early as 9 years of age, with dosing adjusted according to age.[71] Calcium supplementation also reduces fracture and fall risk in adults aged 65 and older.[72]
The US Food and Drug Administration (FDA) has approved a health claim suggesting that adequate calcium and vitamin D intake, in conjunction with regular physical activity, may reduce the risk of osteoporosis later in life.[73] In contrast, the 2018 US Preventive Services Task Force (USPSTF) concluded that insufficient evidence exists to determine whether supplementation with calcium and vitamin D provides greater benefit than potential harm. Accordingly, the 2018 USPSTF guidelines recommend against routine supplementation with vitamin D and calcium for fracture prevention in community-dwelling, asymptomatic adults. This recommendation does not apply to individuals with symptomatic osteoporosis or established vitamin D deficiency.
Gastrointestinal Malignancy
Calcium binds to bile acids and fatty acids, forming insoluble complexes that protect the gastrointestinal mucosa from acid exposure and related metabolites. Calcium also participates in intracellular signaling pathways that may reduce cellular proliferation by promoting differentiation and apoptosis.[74] Although study findings are inconsistent, available evidence suggests a potential role for calcium in colorectal cancer prevention. An inverse association between daily calcium intake and colorectal cancer risk has been observed, most prominently among older women and individuals with distal colon cancers.[75] However, additional clinical trials are required to clarify these associations. No FDA indication has been established for calcium supplementation in colorectal cancer prevention, as further investigation is ongoing.
Hypoparathyroidism
Low PTH levels may result from autoimmune or surgical destruction of parathyroid tissue, congenital parathyroid abnormalities, impaired PTH regulation, or end-organ resistance to PTH. The systemic consequence is hypocalcemia, which may range from mild to severe manifestations.
Surgical destruction most commonly occurs during thyroid, parathyroid, or neck surgery. Postthyroidectomy hypocalcemia is the most frequent complication of thyroid surgery, with acute manifestations including seizures, laryngospasm, prolonged QT interval, and tetany.[76] Postoperative hypocalcemia may be transient, resulting from glandular stress or partial parathyroid injury, or permanent, arising from inadvertent parathyroid excision.[77][78] Calcium and vitamin D supplementation is typically initiated after thyroid surgery and gradually tapered over 3 to 6 weeks to prevent hypocalcemic symptoms.
Autoimmune destruction is another acquired cause and typically presents during childhood or adolescence. Permanent hypoparathyroidism in this setting occurs as part of autoimmune polyglandular syndrome type 1, resulting from mutations in the AIRE (autoimmune regulator) gene.[79] Activating CaSR antibodies may also develop, producing inappropriate negative feedback and reduced PTH secretion.[80]
Abnormal parathyroid development in utero may cause hypoparathyroidism in infants and children. DiGeorge syndrome is a prototypical example, resulting from a 22q11 deletion that leads to defective development of the pharyngeal pouches and their derivatives. Clinical manifestations include cardiac anomalies, hypocalcemia, thymic hypoplasia, and immunodeficiency.[81]
Peripartum Effects
Professional organizations, such as the American College of Obstetricians and Gynecologists, recommend 1,500 mg to 2,000 mg of calcium daily to reduce the risk of preeclampsia in pregnant women with baseline calcium intake of 600 mg or less. Similarly, the World Health Organization recommends the same dosage range of 1,500 mg to 2,000 mg for pregnant women with low dietary calcium intake and increased risk of gestational hypertension.[82] A 2020 mouse model study demonstrated improved placental efficiency in animals receiving adequate vitamin D, while vitamin D deficiency was associated with altered placental morphogenesis and microstructure.[83] Calcitonin levels increase during pregnancy and lactation and are thought to provide a protective effect by reducing maternal bone loss.
Hypocalcemia may occur within the first days of life, termed "neonatal hypocalcemia," with prematurity as the most common risk factor. Other contributors include maternal diabetes, maternal hyperparathyroidism, and small-for-gestational-age status.[84] Early-onset neonatal hypocalcemia is often asymptomatic and typically occurs within the first 72 hours of life. Neonates at high risk should be monitored during this period for the development of this electrolyte derangement. Late-onset neonatal hypocalcemia, occurring after 72 hours of life, is generally symptomatic and may present with tachycardia, tachypnea, apnea episodes, and seizures.[85]
Chronic Kidney Disease
PTH effectiveness may be reduced in patients with CKD due to impaired renal responsiveness. Consequently, hypocalcemia, hyperphosphatemia, and secondary hyperparathyroidism may occur. Elevated serum phosphate levels stimulate increased PTH secretion, while the diseased kidney is unresponsive. Calcium-containing phosphate binders may be used to reduce serum phosphate levels. Calciphylaxis is a rare complication resulting from calcium–phosphate deposition with rapid calcification of subcutaneous tissues, leading to necrotic skin ulcers, most commonly in advanced renal failure.[86] Calcium citrate should be avoided in these patients due to increased intestinal aluminum absorption, which may result in neurotoxicity and osteomalacia.[87]
Clinicians should consider the potential consequences of oral calcium intake in patients with CKD. Increased intake is associated with an elevated risk of vascular calcification, particularly in patients on dialysis receiving calcium-containing phosphate binders compared with non–calcium-containing phosphate binders. Research analyses indicate that treatment with calcium phosphate binders is associated with progression of coronary and aortic calcification in patients with CKD undergoing hemodialysis.[88]
Conversely, the Dallas Heart Study evaluated the association between coronary artery calcification and end-stage kidney disease in adults with diabetes. The study concluded that adults with both diabetes and CKD have a higher risk of coronary artery calcification compared with patients with CKD alone.[89]
Calcium Nephrolithiasis
Increased calcium excretion contributes to the development of renal stones, composed of either calcium oxalate or calcium phosphate. Historically, patients were advised to reduce calcium intake to prevent hypercalciuria. However, study findings indicate that dietary calcium intake reduces the risk of kidney stone formation, largely through effects on intestinal oxalate absorption. Dietary calcium promotes the formation of calcium–oxalate complexes within the intestinal tract, reducing the absorption of both ions. Calcium restriction increases intestinal oxalate absorption, resulting in greater renal oxalate excretion. Increased urinary oxalate enhances calcium oxalate complex formation within the renal system, promoting stone formation.
A 2012 study of 5,400 women demonstrated that individuals with a history of kidney stones had higher calcium absorption, while increased calcium intake was associated with reduced absorption. Thiazide diuretics increase renal calcium reabsorption, reduce urinary calcium excretion, and may be used for calcium stone prevention in the absence of primary hyperparathyroidism.[90]
Quality Control and Lab Safety
Laboratory errors during sample collection and analysis may produce inaccurate information for the clinical team. Spuriously low calcium values have been reported when anticoagulant-containing collection tubes are underfilled, due to excess chelating agents binding calcium.[91] Calcium measurement is also influenced by specimen quality. Hemolysis and lipemia may interfere with colorimetric or spectrophotometric methods through hemoglobin interference or light-scattering effects. Elevated lipids are a common source of preanalytical error in laboratory tests, including calcium assays, and should be addressed prior to analysis. A 2018 study evaluating methods for processing lipemic samples demonstrated that ultracentrifugation best preserves specimen integrity without exceeding clinically significant interference thresholds.[92] Venous stasis during blood collection may cause a mild, localized increase in calcium levels due to hemodynamic changes. Repeat sampling and reanalysis should be performed when laboratory error is suspected.
The Clinical Laboratory Improvement Amendments of 1988 (CLIA) require laboratories to implement quality control procedures to monitor the accuracy and precision of the entire testing process. For nonwaived tests, CLIA regulations require analysis of at least 2 levels of quality control materials every 24 hours.[93] Quality control samples may be assayed more frequently when necessary to ensure accurate results. Quality control materials should be assayed after instrument calibration or maintenance to verify analytical performance.[94]
Acceptable ranges and interpretive guidelines for quality control outcomes are essential to ensure accuracy and reliability in laboratory testing. Determination of acceptable ranges and interpretive rules is based on balancing detection of clinically significant analytical errors with an acceptable false alert rate. Performance characteristics should be defined for each analyte prior to the selection of appropriate quality control rules.[95] Westgard multirules are typically used to evaluate quality control runs. These rules detect systematic errors, random errors, and shifts in the mean or standard deviation of quality control data. When a run is identified as out of control, the system should be thoroughly investigated to identify the underlying cause. Testing should not proceed until the issue has been resolved.[96]
The laboratory must participate in an external quality control or proficiency testing program. Participation enables assessment of laboratory accuracy and reliability relative to other laboratories performing the same or comparable assays. The proficiency testing plan should be integrated into the laboratory quality assurance plan and the overall quality management system.[97]
Maintaining safety in clinical laboratories is a fundamental aspect of healthcare practice, ensuring the safety of both healthcare personnel and patients. Laboratory safety requires established procedures and precautions for handling potentially hazardous chemical and biological materials. Safety measures include the appropriate use of personal protective equipment, including gloves, laboratory coats, and protective eyewear. Additional protocols encompass careful specimen handling to prevent contamination and to maintain diagnostic accuracy. Proper decontamination procedures and appropriate waste disposal are essential to prevent the transmission of infectious agents. Regular training and continuing education programs equip laboratory personnel with the skills necessary to respond effectively to emergencies and adverse events.[98] Adherence to these measures enables clinical laboratories to provide accurate, reliable, and safe diagnostic services, thereby contributing to high-quality patient care.
Enhancing Healthcare Team Outcomes
Effective management of calcium disorders is essential to optimize patient outcomes and reduce morbidity. Calcium plays a critical role in numerous biochemical pathways. Therefore, understanding the effects of various diseases and therapeutic interventions on calcium homeostasis is fundamental for accurate diagnosis and management. Given the multifactorial nature of calcium imbalance, an interprofessional approach is strongly recommended to individualize patient care and ensure appropriate treatment strategies. Clinical findings should be integrated with laboratory data, with consideration of medication effects and comorbid conditions on calcium levels.
A coordinated, team-based strategy is particularly important in patients receiving therapies known to affect calcium metabolism. Patients treated with bisphosphonates require ongoing monitoring for long-term complications, including osteonecrosis of the jaw, which occurs more frequently in individuals with multiple myeloma or metastatic bone disease.[99] Various medical therapies and interventions may disrupt calcium balance, necessitating close collaboration among healthcare professionals to develop safe and effective management plans.[100]
Interprofessional collaboration among physicians, advanced practitioners, nurses, pharmacists, and dietitians is essential for comprehensive care delivery. Each team member contributes specialized expertise: clinicians guide diagnosis and treatment decisions, pharmacists evaluate medication-related effects and interactions, nurses monitor patient status and support adherence, and dietitians provide nutritional guidance to support calcium balance. Effective communication and care coordination facilitate timely identification and correction of abnormalities, reduce errors, and enhance patient safety. A structured, collaborative approach emphasizing shared responsibility, ethical practice, and continuous communication enables patient-centered care and improved clinical outcomes in patients with calcium disorders.
Media
(Click Image to Enlarge)
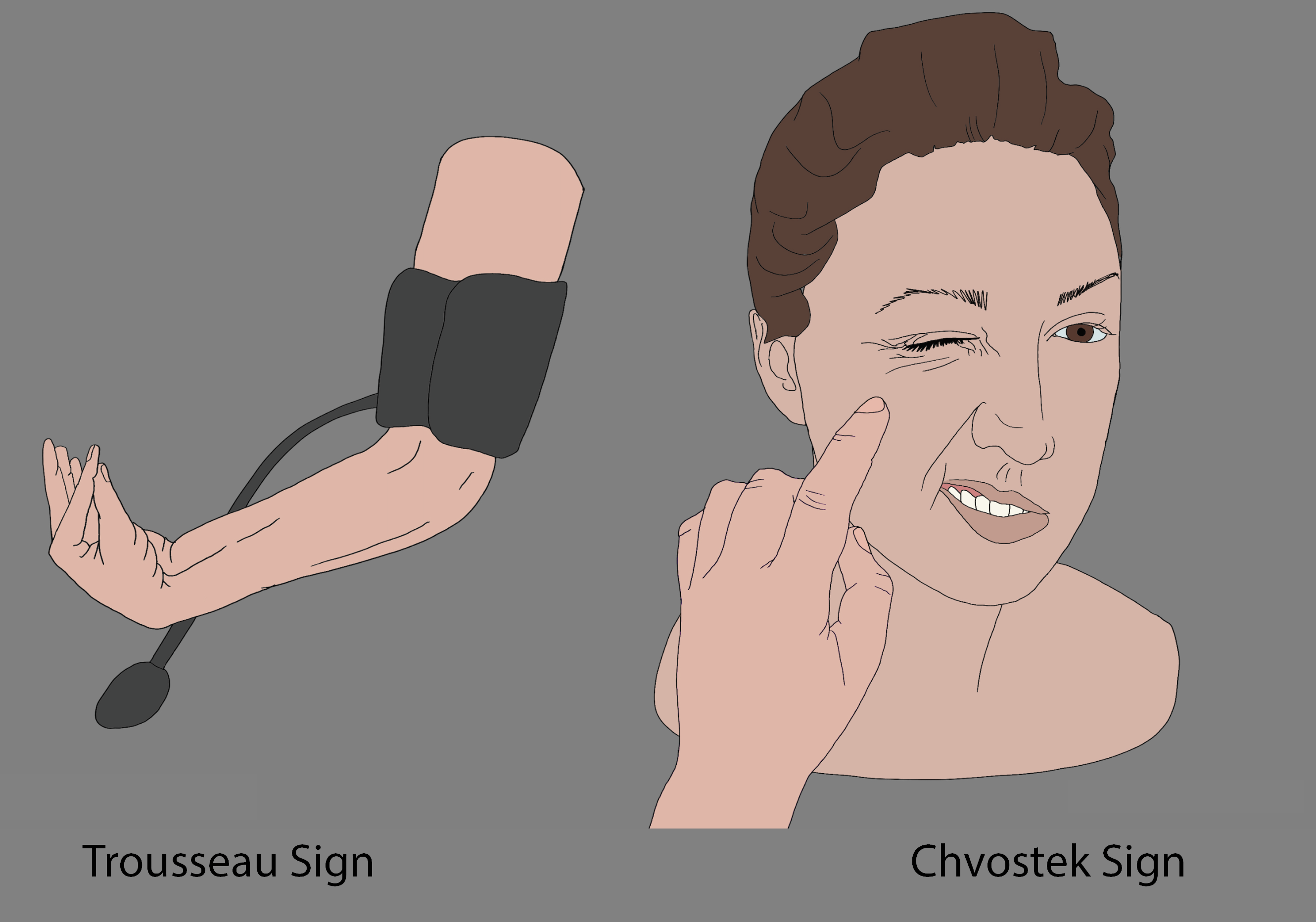
Chvostek And Trousseau Signs. This illustration shows facial tapping that elicits the Chvostek sign (right) and blood pressure cuff inflation that produces the Trousseau sign (left). Both physical findings are associated with clinically significant hypocalcemia.
Contributed by Chelsea Rowe.
References
Cormick G, Belizán JM. Calcium Intake and Health. Nutrients. 2019 Jul 15:11(7):. doi: 10.3390/nu11071606. Epub 2019 Jul 15 [PubMed PMID: 31311164]
Gennari C. Calcium and vitamin D nutrition and bone disease of the elderly. Public health nutrition. 2001 Apr:4(2B):547-59 [PubMed PMID: 11683549]
Baird GS. Ionized calcium. Clinica chimica acta; international journal of clinical chemistry. 2011 Apr 11:412(9-10):696-701. doi: 10.1016/j.cca.2011.01.004. Epub 2011 Jan 14 [PubMed PMID: 21238441]
Level 3 (low-level) evidenceReid IR, Bolland MJ. Controversies in medicine: the role of calcium and vitamin D supplements in adults. The Medical journal of Australia. 2019 Nov:211(10):468-473. doi: 10.5694/mja2.50393. Epub 2019 Nov 3 [PubMed PMID: 31680267]
Schöfl C. [Update - Calcium Metabolism]. Deutsche medizinische Wochenschrift (1946). 2019 Aug:144(16):1125-1132. doi: 10.1055/a-0833-9674. Epub 2019 Aug 15 [PubMed PMID: 31416104]
Nordin BE. Calcium and osteoporosis. Nutrition (Burbank, Los Angeles County, Calif.). 1997 Jul-Aug:13(7-8):664-86 [PubMed PMID: 9263260]
Wilson RF, Binkley LE, Sabo FM Jr, Wilson JA, Munkarah MM, Dulchavsky SA, Diebel LN. Electrolyte and acid-base changes with massive blood transfusions. The American surgeon. 1992 Sep:58(9):535-44; discussion 544-5 [PubMed PMID: 1524320]
Maier JD, Levine SN. Hypercalcemia in the Intensive Care Unit: A Review of Pathophysiology, Diagnosis, and Modern Therapy. Journal of intensive care medicine. 2015 Jul:30(5):235-52. doi: 10.1177/0885066613507530. Epub 2013 Oct 15 [PubMed PMID: 24130250]
Zheng J, Zeng X, Wang S. Calcium ion as cellular messenger. Science China. Life sciences. 2015 Jan:58(1):1-5. doi: 10.1007/s11427-014-4795-y. Epub 2015 Jan 10 [PubMed PMID: 25576449]
Canario A, Flik G. Endocrinology of calcium homeostasis. General and comparative endocrinology. 2007 Jun-Jul:152(2-3):242 [PubMed PMID: 17586159]
Level 3 (low-level) evidenceHoenderop JG, Nilius B, Bindels RJ. Calcium absorption across epithelia. Physiological reviews. 2005 Jan:85(1):373-422 [PubMed PMID: 15618484]
Level 3 (low-level) evidenceParekh AB, Putney JW Jr. Store-operated calcium channels. Physiological reviews. 2005 Apr:85(2):757-810 [PubMed PMID: 15788710]
Level 3 (low-level) evidenceSorensen MD. Calcium intake and urinary stone disease. Translational andrology and urology. 2014 Sep:3(3):235-40. doi: 10.3978/j.issn.2223-4683.2014.06.05. Epub [PubMed PMID: 26816771]
Greger R, Lang F, Oberleithner H. Distal site of calcium reabsorption in the rat nephron. Pflugers Archiv : European journal of physiology. 1978 May 18:374(2):153-7 [PubMed PMID: 566424]
Level 3 (low-level) evidenceFelsenfeld AJ, Levine BS. Calcitonin, the forgotten hormone: does it deserve to be forgotten? Clinical kidney journal. 2015 Apr:8(2):180-7. doi: 10.1093/ckj/sfv011. Epub 2015 Mar 20 [PubMed PMID: 25815174]
Duque EJ, Elias RM, Moysés RMA. Parathyroid Hormone: A Uremic Toxin. Toxins. 2020 Mar 17:12(3):. doi: 10.3390/toxins12030189. Epub 2020 Mar 17 [PubMed PMID: 32192220]
Talmage RV, Mobley HT. Calcium homeostasis: reassessment of the actions of parathyroid hormone. General and comparative endocrinology. 2008 Mar 1:156(1):1-8 [PubMed PMID: 18160068]
Level 3 (low-level) evidenceFong J, Khan A. Hypocalcemia: updates in diagnosis and management for primary care. Canadian family physician Medecin de famille canadien. 2012 Feb:58(2):158-62 [PubMed PMID: 22439169]
Szent-Györgyi AG. Calcium regulation of muscle contraction. Biophysical journal. 1975 Jul:15(7):707-23 [PubMed PMID: 806311]
Level 3 (low-level) evidenceJiang H, Stephens NL. Calcium and smooth muscle contraction. Molecular and cellular biochemistry. 1994 Jun 15:135(1):1-9 [PubMed PMID: 7816050]
Level 3 (low-level) evidenceMasilamani K, van der Voort J. The management of acute hyperkalaemia in neonates and children. Archives of disease in childhood. 2012 Apr:97(4):376-80. doi: 10.1136/archdischild-2011-300623. Epub 2011 Sep 13 [PubMed PMID: 21920871]
Level 3 (low-level) evidenceXiao Q, Murphy RA, Houston DK, Harris TB, Chow WH, Park Y. Dietary and supplemental calcium intake and cardiovascular disease mortality: the National Institutes of Health-AARP diet and health study. JAMA internal medicine. 2013 Apr 22:173(8):639-46. doi: 10.1001/jamainternmed.2013.3283. Epub [PubMed PMID: 23381719]
Wang L, Manson JE, Song Y, Sesso HD. Systematic review: Vitamin D and calcium supplementation in prevention of cardiovascular events. Annals of internal medicine. 2010 Mar 2:152(5):315-23. doi: 10.7326/0003-4819-152-5-201003020-00010. Epub [PubMed PMID: 20194238]
Level 1 (high-level) evidencePalta S, Saroa R, Palta A. Overview of the coagulation system. Indian journal of anaesthesia. 2014 Sep:58(5):515-23. doi: 10.4103/0019-5049.144643. Epub [PubMed PMID: 25535411]
Level 3 (low-level) evidenceYu J, Su H, Wei S, Chen F, Liu C. Calcium content mediated hemostasis of calcium-modified oxidized microporous starch. Journal of biomaterials science. Polymer edition. 2018 Oct:29(14):1716-1728. doi: 10.1080/09205063.2018.1481585. Epub 2018 Jun 14 [PubMed PMID: 29813002]
Morotti A, Charidimou A, Phuah CL, Jessel MJ, Schwab K, Ayres AM, Romero JM, Viswanathan A, Gurol ME, Greenberg SM, Anderson CD, Rosand J, Goldstein JN. Association Between Serum Calcium Level and Extent of Bleeding in Patients With Intracerebral Hemorrhage. JAMA neurology. 2016 Nov 1:73(11):1285-1290. doi: 10.1001/jamaneurol.2016.2252. Epub [PubMed PMID: 27598746]
Krahn J, Lou H. Ionized calcium: whole blood, plasma or serum? Clinical laboratory. 2008:54(5-6):185-9 [PubMed PMID: 18780665]
Cao L, Chen M, Phipps RA, Del Guidice RE, Handy BC, Wagar EA, Meng QH. Causes and impact of specimen rejection in a clinical chemistry laboratory. Clinica chimica acta; international journal of clinical chemistry. 2016 Jul 1:458():154-8. doi: 10.1016/j.cca.2016.05.003. Epub 2016 May 7 [PubMed PMID: 27166198]
Jacobsz LA, Zemlin AE, Roos MJ, Erasmus RT. Chemistry and haematology sample rejection and clinical impact in a tertiary laboratory in Cape Town. Clinical chemistry and laboratory medicine. 2011 Oct 14:49(12):2047-50. doi: 10.1515/CCLM.2011.743. Epub 2011 Oct 14 [PubMed PMID: 21995606]
Level 2 (mid-level) evidenceAtay A, Demir L, Cuhadar S, Saglam G, Unal H, Aksun S, Arslan B, Ozkan A, Sutcu R. Clinical biochemistry laboratory rejection rates due to various types of preanalytical errors. Biochemia medica. 2014:24(3):376-82. doi: 10.11613/BM.2014.040. Epub 2014 Oct 15 [PubMed PMID: 25351356]
Level 3 (low-level) evidenceJones AN, Shafer MM, Keuler NS, Crone EM, Hansen KE. Fasting and postprandial spot urine calcium-to-creatinine ratios do not detect hypercalciuria. Osteoporosis international : a journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2012 Feb:23(2):553-62. doi: 10.1007/s00198-011-1580-7. Epub 2011 Feb 24 [PubMed PMID: 21347742]
Rath B, Aggarwal MK, Mishra TK, Talukdar B, Murthy NS, Kabi BC. Urinary calcium creatinine ratio and hypercalciuria. Indian pediatrics. 1994 Mar:31(3):311-6 [PubMed PMID: 7896367]
Level 1 (high-level) evidenceFelsenfeld AJ, Levine BS, Rodriguez M. Pathophysiology of Calcium, Phosphorus, and Magnesium Dysregulation in Chronic Kidney Disease. Seminars in dialysis. 2015 Nov-Dec:28(6):564-77. doi: 10.1111/sdi.12411. Epub 2015 Aug 25 [PubMed PMID: 26303319]
Ohnishi ST. A method of estimating the amount of calcium bound to the metallochromic indicator arsenazo III. Biochimica et biophysica acta. 1979 Aug 22:586(2):217-30 [PubMed PMID: 38853]
Copeland BE, Grisley DW, Casella J, Bailey H. Comparison of serum calcium measurements with respect to five models of atomic absorption spectrometers using NBS-AACC calcium reference method and isotope-dilution mass spectrometry as the definitive method. American journal of clinical pathology. 1976 Oct:66(4):619-33 [PubMed PMID: 788497]
Level 3 (low-level) evidenceHuang WT, Shahid S, Anderson P. Validation of a Real-Time ISE Methodology to Quantify the Influence of Inhibitors of Demineralization Kinetics in vitro Using a Hydroxyapatite Model System. Caries research. 2018:52(6):598-603. doi: 10.1159/000488597. Epub 2018 May 25 [PubMed PMID: 29804111]
Level 1 (high-level) evidenceCarey CM, Vogel GL. Measurement of Calcium Activity in Oral Fluids by Ion Selective Electrode: Method Evaluation and Simplified Calculation of Ion Activity Products. Journal of research of the National Institute of Standards and Technology. 2000 Mar-Apr:105(2):267-73. doi: 10.6028/jres.105.030. Epub 2000 Apr 1 [PubMed PMID: 27551609]
Sena SF, Bowers GN Jr. Measurement of ionized calcium in biological fluids: ion-selective electrode method. Methods in enzymology. 1988:158():320-34 [PubMed PMID: 3374382]
Level 3 (low-level) evidenceKaufman RA, Tietz NW. Ion effects in measurement of ionized calcium with a calcium-selective electrode. Clinical chemistry. 1980 Apr:26(5):640-4 [PubMed PMID: 6266696]
West J, Atherton J, Costelloe SJ, Pourmahram G, Stretton A, Cornes M. Preanalytical errors in medical laboratories: a review of the available methodologies of data collection and analysis. Annals of clinical biochemistry. 2017 Jan:54(1):14-19. doi: 10.1177/0004563216669384. Epub 2016 Oct 5 [PubMed PMID: 27614351]
Lippi G, Banfi G, Church S, Cornes M, De Carli G, Grankvist K, Kristensen GB, Ibarz M, Panteghini M, Plebani M, Nybo M, Smellie S, Zaninotto M, Simundic AM, European Federation for Clinical Chemistry and Laboratory Medicine Working Group for Preanalytical Phase. Preanalytical quality improvement. In pursuit of harmony, on behalf of European Federation for Clinical Chemistry and Laboratory Medicine (EFLM) Working group for Preanalytical Phase (WG-PRE). Clinical chemistry and laboratory medicine. 2015 Feb:53(3):357-70. doi: 10.1515/cclm-2014-1051. Epub [PubMed PMID: 25490032]
Level 2 (mid-level) evidenceRuppe MD. Medications that affect calcium. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2011 Mar-Apr:17 Suppl 1():26-30. doi: 10.4158/EP10281.RA. Epub [PubMed PMID: 21134875]
Gruber M, Nehring C, Creutzenberg M, Graf B, Hopf S. Perchlorate (Irenat®) may falsely lower measured ionised calcium. Clinical chemistry and laboratory medicine. 2011 Jun:49(6):1019-24. doi: 10.1515/CCLM.2011.160. Epub 2011 Mar 24 [PubMed PMID: 21428857]
Level 3 (low-level) evidenceLiu J, Tio MC, Verma A, Schmidt IM, Ilori TO, Knauf F, Mc Causland FR, Waikar SS. Determinants and Outcomes Associated With Urinary Calcium Excretion in Chronic Kidney Disease. The Journal of clinical endocrinology and metabolism. 2022 Jan 1:107(1):e281-e292. doi: 10.1210/clinem/dgab574. Epub [PubMed PMID: 34390334]
Manz F, Kehrt R, Lausen B, Merkel A. Urinary calcium excretion in healthy children and adolescents. Pediatric nephrology (Berlin, Germany). 1999 Nov:13(9):894-9 [PubMed PMID: 10603144]
Jain A, Bhayana S, Vlasschaert M, House A. A formula to predict corrected calcium in haemodialysis patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2008 Sep:23(9):2884-8. doi: 10.1093/ndt/gfn186. Epub 2008 Apr 3 [PubMed PMID: 18388119]
Shrimanker I, Bhattarai S. Electrolytes. StatPearls. 2026 Jan:(): [PubMed PMID: 31082167]
Yu E, Sharma S. Physiology, Calcium. StatPearls. 2026 Jan:(): [PubMed PMID: 29489276]
Cano-Torres EA, González-Cantú A, Hinojosa-Garza G, Castilleja-Leal F. Immobilization induced hypercalcemia. Clinical cases in mineral and bone metabolism : the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases. 2016 Jan-Apr:13(1):46-7. doi: 10.11138/ccmbm/2016.13.1.046. Epub 2016 May 11 [PubMed PMID: 27252745]
Level 3 (low-level) evidenceBilezikian JP. Hypercalcemia. Disease-a-month : DM. 1988 Dec:34(12):737-99 [PubMed PMID: 3061760]
Minisola S, Pepe J, Piemonte S, Cipriani C. The diagnosis and management of hypercalcaemia. BMJ (Clinical research ed.). 2015 Jun 2:350():h2723. doi: 10.1136/bmj.h2723. Epub 2015 Jun 2 [PubMed PMID: 26037642]
Turner JJO. Hypercalcaemia - presentation and management . Clinical medicine (London, England). 2017 Jun:17(3):270-273. doi: 10.7861/clinmedicine.17-3-270. Epub [PubMed PMID: 28572230]
Farias ML. [Hypercalcemia of malignancy: clinical features, diagnosis and treatment]. Arquivos brasileiros de endocrinologia e metabologia. 2005 Oct:49(5):816-24 [PubMed PMID: 16444366]
Hosking DJ, Cowley A, Bucknall CA. Rehydration in the treatment of severe hypercalcaemia. The Quarterly journal of medicine. 1981 Autumn:50(200):473-81 [PubMed PMID: 7342172]
Koo WS, Jeon DS, Ahn SJ, Kim YS, Yoon YS, Bang BK. Calcium-free hemodialysis for the management of hypercalcemia. Nephron. 1996:72(3):424-8 [PubMed PMID: 8852491]
Pepe J, Colangelo L, Biamonte F, Sonato C, Danese VC, Cecchetti V, Occhiuto M, Piazzolla V, De Martino V, Ferrone F, Minisola S, Cipriani C. Diagnosis and management of hypocalcemia. Endocrine. 2020 Sep:69(3):485-495. doi: 10.1007/s12020-020-02324-2. Epub 2020 May 4 [PubMed PMID: 32367335]
de Brito Galvão JF, Schenck PA, Chew DJ. A Quick Reference on Hypocalcemia. The Veterinary clinics of North America. Small animal practice. 2017 Mar:47(2):249-256. doi: 10.1016/j.cvsm.2016.10.017. Epub 2016 Dec 22 [PubMed PMID: 28012786]
Level 3 (low-level) evidenceGarabédian M. [Hypocalcemia]. La Revue du praticien. 1998 Jun 1:48(11):1201-6 [PubMed PMID: 9781172]
Schenck PA, Chew DJ. Hypocalcemia: a quick reference. The Veterinary clinics of North America. Small animal practice. 2008 May:38(3):455-8, viii. doi: 10.1016/j.cvsm.2008.01.021. Epub [PubMed PMID: 18402868]
Level 3 (low-level) evidenceBove-Fenderson E, Mannstadt M. Hypocalcemic disorders. Best practice & research. Clinical endocrinology & metabolism. 2018 Oct:32(5):639-656. doi: 10.1016/j.beem.2018.05.006. Epub 2018 May 28 [PubMed PMID: 30449546]
Fukumoto S, Namba N, Ozono K, Yamauchi M, Sugimoto T, Michigami T, Tanaka H, Inoue D, Minagawa M, Endo I, Matsumoto T. Causes and differential diagnosis of hypocalcemia--recommendation proposed by expert panel supported by ministry of health, labour and welfare, Japan. Endocrine journal. 2008 Oct:55(5):787-94 [PubMed PMID: 18490837]
Giancarelli A, Birrer KL, Alban RF, Hobbs BP, Liu-DeRyke X. Hypocalcemia in trauma patients receiving massive transfusion. The Journal of surgical research. 2016 May 1:202(1):182-7. doi: 10.1016/j.jss.2015.12.036. Epub 2015 Dec 30 [PubMed PMID: 27083965]
Straub DA. Calcium supplementation in clinical practice: a review of forms, doses, and indications. Nutrition in clinical practice : official publication of the American Society for Parenteral and Enteral Nutrition. 2007 Jun:22(3):286-96 [PubMed PMID: 17507729]
Feingold KR, Adler RA, Ahmed SF, Anawalt B, Blackman MR, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hamilton E, Hofland J, Jan de Beur S, Kalra S, Kaltsas G, Kapoor N, Kim M, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Schafer AL, Shoback DM. Hypocalcemia: Diagnosis and Treatment. Endotext. 2000:(): [PubMed PMID: 25905251]
Boisen IM, Mos I, Lerche-Black EM, Juul A, Bräuner-Osborne H, Blomberg Jensen M. Heterozygous Mutation (Q459R) in the Calcium-Sensing Receptor Gene Causes Familial Hypocalciuric Hypercalcemia 1 (FHH1). The Journal of clinical endocrinology and metabolism. 2020 Apr 1:105(4):. pii: dgz205. doi: 10.1210/clinem/dgz205. Epub [PubMed PMID: 32160303]
Conticini E, Negro A, Magnani L, Ugolini R, Atienza-Mateo B, Frediani B, Salvarani C. Gitelman syndrome associated with chondrocalcinosis and severe neuropathy: a novel heterozygous mutation in SLC12A3 gene. Reumatismo. 2020 Apr 10:72(1):67-70. doi: 10.4081/reumatismo.2020.1255. Epub 2020 Apr 10 [PubMed PMID: 32292023]
Hanseree P, Staples AC, Cryns VL, Hansen KE. Hypocalciuria as a Predictor of Reduced Intestinal Calcium Absorption. Journal of the Endocrine Society. 2017 Sep 1:1(9):1179-1187. doi: 10.1210/js.2017-00234. Epub 2017 Aug 7 [PubMed PMID: 29264573]
Letavernier E, Daudon M. Vitamin D, Hypercalciuria and Kidney Stones. Nutrients. 2018 Mar 17:10(3):. doi: 10.3390/nu10030366. Epub 2018 Mar 17 [PubMed PMID: 29562593]
Wróblewski T, Wystrychowski A. [Hypercalciuria]. Przeglad lekarski. 2011:68(2):107-13 [PubMed PMID: 21751520]
Alejandro P, Constantinescu F. A Review of Osteoporosis in the Older Adult: An Update. Rheumatic diseases clinics of North America. 2018 Aug:44(3):437-451. doi: 10.1016/j.rdc.2018.03.004. Epub 2018 Jun 13 [PubMed PMID: 30001785]
Hauk L, American College of Obstetricians and Gynecologists. ACOG releases practice bulletin on osteoporosis. American family physician. 2013 Aug 15:88(4):269-75 [PubMed PMID: 23944732]
American Geriatrics Society Workgroup on Vitamin D Supplementation for Older Adults. Recommendations abstracted from the American Geriatrics Society Consensus Statement on vitamin D for Prevention of Falls and Their Consequences. Journal of the American Geriatrics Society. 2014 Jan:62(1):147-52. doi: 10.1111/jgs.12631. Epub 2013 Dec 18 [PubMed PMID: 24350602]
Level 3 (low-level) evidenceWallingford JC. Perspective: Structure-Function Claims on Infant Formula. Advances in nutrition (Bethesda, Md.). 2018 May 1:9(3):183-192. doi: 10.1093/advances/nmy006. Epub [PubMed PMID: 29767697]
Level 3 (low-level) evidenceMilner JA, McDonald SS, Anderson DE, Greenwald P. Molecular targets for nutrients involved with cancer prevention. Nutrition and cancer. 2001:41(1-2):1-16 [PubMed PMID: 12094610]
Terry P, Baron JA, Bergkvist L, Holmberg L, Wolk A. Dietary calcium and vitamin D intake and risk of colorectal cancer: a prospective cohort study in women. Nutrition and cancer. 2002:43(1):39-46 [PubMed PMID: 12467133]
Level 2 (mid-level) evidenceMacefield G, Burke D. Paraesthesiae and tetany induced by voluntary hyperventilation. Increased excitability of human cutaneous and motor axons. Brain : a journal of neurology. 1991 Feb:114 ( Pt 1B)():527-40 [PubMed PMID: 2004255]
Hundahl SA, Cady B, Cunningham MP, Mazzaferri E, McKee RF, Rosai J, Shah JP, Fremgen AM, Stewart AK, Hölzer S. Initial results from a prospective cohort study of 5583 cases of thyroid carcinoma treated in the united states during 1996. U.S. and German Thyroid Cancer Study Group. An American College of Surgeons Commission on Cancer Patient Care Evaluation study. Cancer. 2000 Jul 1:89(1):202-17 [PubMed PMID: 10897019]
Level 2 (mid-level) evidenceGlover GH. Multipoint Dixon technique for water and fat proton and susceptibility imaging. Journal of magnetic resonance imaging : JMRI. 1991 Sep-Oct:1(5):521-30 [PubMed PMID: 1790376]
Guo CJ, Leung PSC, Zhang W, Ma X, Gershwin ME. The immunobiology and clinical features of type 1 autoimmune polyglandular syndrome (APS-1). Autoimmunity reviews. 2018 Jan:17(1):78-85. doi: 10.1016/j.autrev.2017.11.012. Epub 2017 Nov 4 [PubMed PMID: 29108822]
Chamberlin M, Kemp EH, Weetman AP, Khadka B, Brown EM. Immunosuppressive therapy of autoimmune hypoparathyroidism in a patient with activating autoantibodies against the calcium-sensing receptor. Clinical endocrinology. 2019 Jan:90(1):214-221. doi: 10.1111/cen.13886. Epub 2018 Nov 14 [PubMed PMID: 30358904]
Rayannavar A, Levitt Katz LE, Crowley TB, Lessig M, Grand K, Goldmuntz E, Zackai EH, McDonald-McGinn DM. Association of hypocalcemia with congenital heart disease in 22q11.2 deletion syndrome. American journal of medical genetics. Part A. 2018 Oct:176(10):2099-2103. doi: 10.1002/ajmg.a.40495. Epub 2018 Oct 1 [PubMed PMID: 30277015]
. WHO recommendation: Calcium supplementation during pregnancy for the prevention of pre-eclampsia and its complications. 2018:(): [PubMed PMID: 30629391]
Wilson RL, Phillips JA, Bianco-Miotto T, McAninch D, Goh Z, Anderson PH, Roberts CT. Reduced Dietary Calcium and Vitamin D Results in Preterm Birth and Altered Placental Morphogenesis in Mice During Pregnancy. Reproductive sciences (Thousand Oaks, Calif.). 2020 Jun:27(6):1330-1339. doi: 10.1007/s43032-019-00116-2. Epub 2020 Jan 1 [PubMed PMID: 32046423]
Vuralli D. Clinical Approach to Hypocalcemia in Newborn Period and Infancy: Who Should Be Treated? International journal of pediatrics. 2019:2019():4318075. doi: 10.1155/2019/4318075. Epub 2019 Jun 19 [PubMed PMID: 31320908]
Venkataraman PS, Blick KE, Fry HD, Rao RK. Postnatal changes in calcium-regulating hormones in very-low-birth-weight infants. Effect of early neonatal hypocalcemia and intravenous calcium infusion on serum parathyroid hormone and calcitonin homeostasis. American journal of diseases of children (1960). 1985 Sep:139(9):913-6 [PubMed PMID: 4036926]
Marques SA, Kakuda AC, Mendaçolli TJ, Abbade LP, Marques ME. Calciphylaxis: a rare but potentially fatal event of chronic kidney disease. Case report. Anais brasileiros de dermatologia. 2013 Nov-Dec:88(6 Suppl 1):44-7. doi: 10.1590/abd1806-4841.20132280. Epub [PubMed PMID: 24346877]
Level 3 (low-level) evidenceKirschbaum BB, Schoolwerth AC. Acute aluminum toxicity associated with oral citrate and aluminum-containing antacids. The American journal of the medical sciences. 1989 Jan:297(1):9-11 [PubMed PMID: 2913801]
Level 3 (low-level) evidenceChertow GM, Burke SK, Raggi P, Treat to Goal Working Group. Sevelamer attenuates the progression of coronary and aortic calcification in hemodialysis patients. Kidney international. 2002 Jul:62(1):245-52 [PubMed PMID: 12081584]
Level 1 (high-level) evidenceKramer H, Toto R, Peshock R, Cooper R, Victor R. Association between chronic kidney disease and coronary artery calcification: the Dallas Heart Study. Journal of the American Society of Nephrology : JASN. 2005 Feb:16(2):507-13 [PubMed PMID: 15601745]
Level 2 (mid-level) evidenceCourbebaisse M, Prot-Bertoye C, Daudon M. [Nephrolithiasis: From mechanisms to preventive medical treatment]. Nephrologie & therapeutique. 2020 Feb:16(1):65-75. doi: 10.1016/j.nephro.2020.01.001. Epub 2020 Feb 29 [PubMed PMID: 32122798]
Sachs C, Rabouine P, Chaneac M, Kindermans C, Dechaux M, Falch-Christiansen T. Preanalytical errors in ionized calcium measurements induced by the use of liquid heparin. Annals of clinical biochemistry. 1991 Mar:28 ( Pt 2)():167-73 [PubMed PMID: 1859155]
Castro-Castro MJ, Candás-Estébanez B, Esteban-Salán M, Calmarza P, Arrobas-Velilla T, Romero-Román C, Pocoví-Mieras M, Aguilar-Doreste JÁ, Commission on Lipoprotein and Vascular Diseases, Sociedad Española de Química Clínica. Removing Lipemia in Serum/Plasma Samples: A Multicenter Study. Annals of laboratory medicine. 2018 Nov:38(6):518-523. doi: 10.3343/alm.2018.38.6.518. Epub [PubMed PMID: 30027694]
Level 2 (mid-level) evidenceFulton II MR, Zubair M, Taghavi S. Laboratory Evaluation of Sepsis. StatPearls. 2026 Jan:(): [PubMed PMID: 37603649]
Lowe D, Sanvictores T, Zubair M, John S. Serum Alkaline Phosphatase: Clinical and Laboratory Perspectives. StatPearls. 2026 Jan:(): [PubMed PMID: 29083622]
Sonagra AD, Zubair M. Laboratory Evaluation of Hereditary Hemochromatosis. StatPearls. 2026 Jan:(): [PubMed PMID: 37603641]
Bayat H. Selecting multi-rule quality control procedures based on patient risk. Clinical chemistry and laboratory medicine. 2017 Oct 26:55(11):1702-1708. doi: 10.1515/cclm-2016-1077. Epub [PubMed PMID: 28236626]
Level 2 (mid-level) evidenceGandhi T, Zubair M, Bhatt H. Cancer Antigen 125. StatPearls. 2026 Jan:(): [PubMed PMID: 32965916]
Novack ML, Zubair M. Natriuretic Peptide B Type Test. StatPearls. 2026 Jan:(): [PubMed PMID: 32310596]
Major P, Lortholary A, Hon J, Abdi E, Mills G, Menssen HD, Yunus F, Bell R, Body J, Quebe-Fehling E, Seaman J. Zoledronic acid is superior to pamidronate in the treatment of hypercalcemia of malignancy: a pooled analysis of two randomized, controlled clinical trials. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2001 Jan 15:19(2):558-67 [PubMed PMID: 11208851]
Level 1 (high-level) evidenceWeaver CM, Peacock M. Calcium. Advances in nutrition (Bethesda, Md.). 2011 May:2(3):290-2. doi: 10.3945/an.111.000463. Epub 2011 Apr 30 [PubMed PMID: 22332061]
Level 3 (low-level) evidence