Introduction
Lipoid pneumonia is a rare, underrecognized pulmonary disorder characterized by parenchymal inflammation caused by lipid accumulation in the distal airways and alveoli, impairing gas exchange. The term “lipoid pneumonia” was first introduced by Laughlin in 1925.[1]
The condition is broadly classified into 2 types. Exogenous lipoid pneumonia (ELP) results from aspiration or inhalation of lipid-containing substances, such as mineral oils and vaping products. Endogenous lipoid pneumonia (EnLP), also known as cholesterol pneumonia, arises from internal lipid accumulation due to airway obstruction, cellular necrosis, or metabolic dysfunction. Both forms exhibit nonspecific clinical and radiologic features that overlap with infectious pneumonia, malignancy, and diffuse parenchymal lung diseases, complicating diagnosis.[2] A thorough clinical history, combined with characteristic radiographic and histopathologic findings, often provides essential diagnostic clues.
Heightened clinical awareness is increasingly important given the rising incidence of ELP associated with electronic cigarette (e-cigarette) and tetrahydrocannabinol (THC) oil use among adolescents and young adults, as well as aspiration-related ELP in vulnerable populations, including infants, older adults, and individuals with neuromuscular or esophageal disorders.[3] Despite growing relevance, lipoid pneumonia remains poorly understood, with limited research resulting from frequent underreporting and misdiagnosis. This activity focuses on the etiology, clinical manifestations, evaluation, and treatment of this condition.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
ELP results from the inhalation or aspiration of various lipid-containing substances. Silent aspiration may occur with mineral oil–based laxatives and nasopharyngeal sprays due to their low viscosity and cough-suppressing properties.[4] Petroleum-based ointments applied around tracheostomy cannulas or endotracheal tubes can aerosolize during airway care, leading to pulmonary deposition.[5] Occupational exposures have been reported in fire-breathing entertainers, automobile mechanics using lubricants, furniture polishers, and metalworkers exposed to cutting oils.[6]
E-cigarettes and vaping products (e-liquids) have recently emerged as significant sources of lipid inhalation. These products often contain lipid-rich components, including vitamin E acetate, medium-chain triglycerides, and flavored propylene glycol or vegetable glycerin mixtures. Certain traditional practices, such as nasal instillation of ghee or sesame oil (an Ayurvedic practice known as nasya), oil pulling, and application of camphorated topical oils, are additional recognized risk factors.[7][8]
EnLP arises as a secondary inflammatory response triggered by the release and accumulation of lipids, typically following tissue injury. Endobronchial obstruction from malignant tumors, benign lesions, or strictures is a common cause. Chronic infections that result in airway scarring, such as posttuberculous stenosis, are also implicated. Autoimmune disorders characterized by granulomatous inflammation, including sarcoidosis and granulomatosis with polyangiitis, may contribute to lipid accumulation.[9] Inherited lipid storage disorders, including Niemann-Pick and Wolman diseases, are other etiologies.[10]
Epidemiology
The true incidence of lipoid pneumonia is unknown. Historical autopsy series have estimated the frequency of this condition at 1% to 2.5%. More than 2,800 confirmed or probable cases were identified during the 2019 US outbreak of e-cigarette or vaping product–associated lung injury (EVALI). Bronchoalveolar lavage (BAL) frequently demonstrated lipid-laden macrophages. Vitamin E acetate was detected in 94% of BAL samples, indicating a likely etiologic role for this substance in vaping-associated cases.[11]
A bimodal distribution is now recognized. The 1st peak occurs in adolescents and young adults exposed to THC and nicotine oils. The 2nd peak occurs in older adults aspirating mineral oil or food-borne lipids due to dysphagia or neurological disease. Geographical variation in incidence appears to reflect the popularity of mineral-oil remedies, traditional cultural practices, and differing national regulations concerning vaping products.[12]
Pathophysiology
The pathophysiology of lipoid pneumonia, whether exogenous or endogenous, involves lipid deposition in the alveoli. Accumulation triggers a persistent inflammatory response.
In ELP, inhaled or aspirated lipid-containing substances bypass normal airway defenses. Silent aspiration or deep inhalation of low-viscosity agents that do not elicit the cough reflex often contributes to alveolar deposition. Once in the alveolar space, long-chain hydrocarbons resist enzymatic degradation and are engulfed by alveolar macrophages, which are unable to metabolize them. This process leads to the formation of vacuolated “foamy” macrophages. Residual lipids are released as these macrophages undergo apoptosis, perpetuating a chronic foreign-body granulomatous reaction characterized by the appearance of multinucleated giant cells, persistent inflammation, surfactant dysfunction, and eventual interstitial fibrosis.
In individuals with chronic aspiration, retained lipids may become encased in granulation tissue, forming a paraffinoma. This well-organized lipogranuloma may radiographically mimic malignancy.
In EnLP, lipid accumulation results from alveolar damage or airway obstruction caused by malignancy, infection, or inflammation. Breakdown of cellular membranes releases cholesterol esters and triglycerides into the alveolar space. Local hypoxia and carbon dioxide retention accelerate lipid deposition and impair clearance. Both forms are characterized by the accumulation of foamy macrophages, ongoing inflammation, and the risk of progression to fibrosis if not identified and managed promptly.[13]
Histopathology
Cytology obtained from BAL or lung biopsy typically demonstrates characteristic findings in lipoid pneumonia. Findings include foamy macrophages with cytoplasmic vacuoles that stain with Oil-Red-O or Sudan black on fresh or frozen sections. Extracellular cholesterol clefts surrounded by foreign-body giant cells are also observed. Although the histopathology of EnLP closely resembles that of ELP, EnLP often exhibits a higher prevalence of intracellular cholesterol clefts. Longstanding disease may show chronic interstitial inflammation and organizing pneumonia.
Routine paraffin embedding dissolves lipid content, rendering it unsuitable for identifying these features. Therefore, frozen-section staining or specialized processing techniques are required for definitive histopathological confirmation.[14]
History and Physical
Nearly half of patients with ELP are asymptomatic.[15] Symptomatic cases are frequently recurrent. Symptom onset in lipoid pneumonia can range from abrupt to insidious, with 2 primary clinical phenotypes recognized. Acute postaspiration inflammation, more common in infants and children, presents with the sudden onset of cough, fever, and dyspnea within hours to days following aspiration. These symptoms are often indistinguishable from those of infectious pneumonia. Chronic, silent microaspirations, typically seen in older adults with dysphagia or neurologic disorders, are characterized by minimal or nonspecific symptoms until incidental imaging reveals abnormalities, or a gradually worsening cough and exertional dyspnea prompt further evaluation.[16] Less common manifestations include fever, night sweats, chest pain, and weight loss.
Physical examination often reveals fine crackles. Wheezing or hemoptysis may occur if bronchial obstruction develops. A thorough and detailed exposure history is essential for accurate diagnosis.
Evaluation
The diagnosis of lipoid pneumonia requires a high index of suspicion. Confirmation necessitates laboratory and radiological evidence. Laboratory evaluation may reveal elevated inflammatory markers, such as C-reactive protein. Arterial blood gas analysis can help assess disease severity. Laboratory findings are generally nonspecific for the condition.
Imaging plays a central role in diagnosis. Chest radiographs often demonstrate bilateral lower-zone or gravity-dependent consolidation. Unilateral, mass-like opacities may also occur, potentially mimicking malignancy or infectious pneumonia.
High-resolution computed tomography provides more definitive diagnostic information. Low-attenuation consolidation or ground-glass opacities with negative Hounsfield units (–30 to –150), indicative of intrapulmonary fat, are observed in approximately 50% to 65% of cases involving mineral oil aspiration. A “crazy-paving” pattern, defined by ground-glass opacity with interlobular and intralobular septal thickening, occurs in approximately 20% of cases. Additional computed tomography findings may include fat-density nodules in a centrilobular distribution (see Image. Lipoid Pneumonia on Chest Computed Tomography).[17] Chronic EnLP may evolve with calcification or cavitation.
Serologic studies, including antinuclear antibodies, rheumatoid factor, and scleroderma antibodies, can help exclude connective tissue diseases. Pulmonary function tests in lipoid pneumonia often demonstrate a reduced diffusing capacity. A restrictive ventilatory pattern may also be observed. These findings are nonspecific and occur in various other pulmonary conditions.
Bronchoscopy is a critical diagnostic tool, supporting the diagnosis of lipoid pneumonia and helping exclude other potential etiologies, such as infectious pneumonia. Identification of lipid-laden macrophages in BAL fluid, stained with Oil-Red-O, supports the diagnosis. This finding is neither highly sensitive nor specific.[18] A lipid-laden macrophage index (LLMI) greater than 50% can distinguish lipoid pneumonia from infectious and other inflammatory lung diseases with high accuracy. Additional tissue sampling via transbronchial or surgical lung biopsy may be required to establish a definitive diagnosis when BAL results are inconclusive or a localized lesion raises concern for malignancy.
Treatment / Management
Management of lipoid pneumonia begins with elimination of the inciting exposure, which remains the cornerstone of therapy. Immediate cessation of e-cigarette or vaping products, substitution of water-soluble lubricants in tracheostomy care, and swallowing evaluation for patients with dysphagia are recommended. Occupational counseling and appropriate respiratory protection are essential for individuals exposed to aerosolized oils in the workplace.
Supportive care includes maintaining oxygen saturation above 92% with supplemental oxygen as needed. Corticosteroids are widely used based on observational data. A commonly employed regimen consists of prednisone at 0.5 to 1 mg/kg/day for 1 to 2 weeks, followed by a taper over 6 to 8 weeks. Therapy should continue only if demonstrable clinical or radiologic improvement occurs. Empirical antimicrobials should be discontinued once infection is excluded through negative microbiologic testing.[19](B3)
Patients who do not respond to corticosteroids and exposure elimination may be considered for whole-lung or segmental lavage to remove lipid material and inflammatory debris. Lavage should be performed only in centers experienced with procedures similar to those used for pulmonary alveolar proteinosis.[20](B3)
Adjunctive therapies, including intravenous immunoglobulin for immune modulation in immunocompromised pediatric patients and macrolide antibiotics for anti-inflammatory effects in select patients, have been explored. Current evidence is limited to fewer than 10 published cases with inconsistent outcomes.
Differential Diagnosis
The following differential diagnoses should be carefully considered when evaluating a patient for lipoid pneumonia:
- Bacterial, viral, or fungal pneumonia
- Aspiration pneumonia
- Acute respiratory distress syndrome
- Pulmonary alveolar proteinosis
- Acute eosinophilic pneumonia
- Cryptogenic or secondary organizing pneumonia
- Connective tissue disease–associated interstitial lung disease
- Idiopathic interstitial pneumonias
- Lung neoplasm
- Pulmonary hamartoma
Pulmonary hamartoma should be specifically excluded when EnLP presents as a fat-containing pulmonary nodule. Across these conditions, clinical, radiologic, and histopathologic features may overlap with those of lipoid pneumonia. A comprehensive evaluation is therefore essential to establish an accurate diagnosis.
Prognosis
Prognosis in lipoid pneumonia depends on the underlying etiology, timeliness of diagnosis, patient age, and presence of comorbid conditions. Acute vaping-associated ELP often resolves within weeks following exposure cessation and corticosteroid therapy. Chronic aspiration-related disease may progress to fibrosis if not identified and managed promptly.
Complications
Potential complications of lipoid pneumonia include the following:
- Acute or chronic respiratory failure
- Acute respiratory distress syndrome
- Diffuse alveolar hemorrhage
- Secondary infection within lipid-rich consolidations
- Pulmonary hypertension with resultant right heart failure
- Postinfectious bronchiectasis
- Progressive pulmonary fibrosis
Effective prevention requires addressing modifiable risk factors, including cessation of vaping or aspiration-prone practices. Continuous assessment and tailored management reduce the likelihood of long-term outcomes, such as pulmonary fibrosis.
Deterrence and Patient Education
Counseling should emphasize the risks of inhaling oil-based substances, particularly flavored e-cigarettes, which are frequently perceived as harmless. Older adults should be advised against using mineral oil–based laxatives, with safer alternatives recommended whenever possible. Patients should be instructed to disclose all over-the-counter medications, herbal remedies, and recreational substances, as these agents may contain hidden lipid components. Education on early recognition of respiratory symptoms and the importance of seeking prompt medical evaluation is essential for timely diagnosis and effective management.
Enhancing Healthcare Team Outcomes
Lipoid pneumonia, once considered a rare autopsy finding, is now increasingly recognized across all age groups due to evolving exposure risks, including widespread use of e-cigarettes and over-the-counter oil-based products. Effective diagnosis and management require a high degree of clinical suspicion and coordinated interprofessional collaboration. Primary care providers play a pivotal role in prevention and early detection. Remaining informed about common yet underrecognized risk factors, such as vaping and using mineral oil laxatives, is essential, particularly in individuals with dysphagia or gastroesophageal reflux disease. Patients may not voluntarily disclose use of e-cigarettes, herbal supplements, or over-the-counter medications. Therefore, proactive inquiry about these exposures during history-taking is recommended.
Diagnosis relies on thorough clinical evaluation, supported by high-resolution imaging and, when necessary, confirmatory cytology or histopathology. Electronic health record prompts and decision support tools may enhance early identification of lipoid pneumonia. Nurses, respiratory therapists, speech-language pathologists, radiologists, and pulmonologists all contribute to optimizing care. Nurses and respiratory therapists monitor for clinical deterioration, while speech-language pathologists assess swallowing function to reduce aspiration risk. Radiologists provide critical imaging interpretation. Pulmonologists oversee advanced interventions, including bronchoscopy and lavage.
The absence of randomized trials and the rising incidence of this condition highlight the need for ongoing education for healthcare professionals and the public. Laws restricting e-cigarette access and targeted public awareness campaigns may reduce the number of new cases. Early recognition, patient education, and a coordinated interprofessional approach are essential to improving outcomes and avoiding unnecessary interventions, such as inappropriate antibiotic use.[21]
Media
(Click Image to Enlarge)
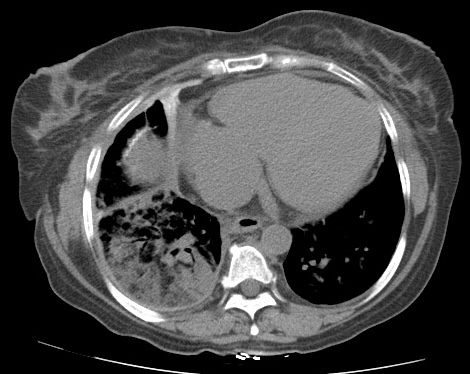
Lipoid Pneumonia on Chest Computed Tomography. This axial computed tomography image demonstrates multifocal consolidations with fat attenuation in the lower lobes bilaterally, consistent with lipoid pneumonia.
Contributed by Steve Lange, MD
References
Laughlen GF. Studies on Pneumonia Following Naso-Pharyngeal Injections of Oil. The American journal of pathology. 1925 Jul:1(4):407-414.1 [PubMed PMID: 19969662]
Hadda V, Khilnani GC. Lipoid pneumonia: an overview. Expert review of respiratory medicine. 2010 Dec:4(6):799-807. doi: 10.1586/ers.10.74. Epub [PubMed PMID: 21128754]
Level 3 (low-level) evidenceDavidson K, Brancato A, Heetderks P, Mansour W, Matheis E, Nario M, Rajagopalan S, Underhill B, Wininger J, Fox D. Outbreak of Electronic-Cigarette-Associated Acute Lipoid Pneumonia - North Carolina, July-August 2019. MMWR. Morbidity and mortality weekly report. 2019 Sep 13:68(36):784-786. doi: 10.15585/mmwr.mm6836e1. Epub 2019 Sep 13 [PubMed PMID: 31513559]
Simmons A, Rouf E, Whittle J. Not your typical pneumonia: a case of exogenous lipoid pneumonia. Journal of general internal medicine. 2007 Nov:22(11):1613-6 [PubMed PMID: 17846847]
Level 3 (low-level) evidenceTancredi A, Graziano P, Scaramuzzi R, Scaramuzzi G, Carosi I, Attino V, Cuttitta A, Taurchini M. Exogenous Lipoid Pneumonia due to Chronic Inhalation of Oily Product Used as a Lubricant of Tracheotomy Cannula. The Eurasian journal of medicine. 2018 Jun:50(2):125-127. doi: 10.5152/eurasianjmed.2018.17325. Epub 2018 Jun 1 [PubMed PMID: 30002581]
Gondouin A, Manzoni P, Ranfaing E, Brun J, Cadranel J, Sadoun D, Cordier JF, Depierre A, Dalphin JC. Exogenous lipid pneumonia: a retrospective multicentre study of 44 cases in France. The European respiratory journal. 1996 Jul:9(7):1463-9 [PubMed PMID: 8836660]
Level 2 (mid-level) evidenceAl-Kindi H, Abdoani R, El-Iraqi M, Praseeda I. Lipoid Pneumonia Following Aspiration of Ghee (animal fat) in an Omani Infant. Oman medical journal. 2008 Apr:23(2):108-11 [PubMed PMID: 22379548]
Level 2 (mid-level) evidenceKuroyama M, Kagawa H, Kitada S, Maekura R, Mori M, Hirano H. Exogenous lipoid pneumonia caused by repeated sesame oil pulling: a report of two cases. BMC pulmonary medicine. 2015 Oct 30:15():135. doi: 10.1186/s12890-015-0134-8. Epub 2015 Oct 30 [PubMed PMID: 26518258]
Level 3 (low-level) evidenceByerley JS, Hernandez ML, Leigh MW, Antoon JW. Clinical approach to endogenous lipoid pneumonia. The clinical respiratory journal. 2016 Mar:10(2):259-63. doi: 10.1111/crj.12203. Epub 2014 Sep 16 [PubMed PMID: 25123703]
Nicholson AG, Wells AU, Hooper J, Hansell DM, Kelleher A, Morgan C. Successful treatment of endogenous lipoid pneumonia due to Niemann-Pick Type B disease with whole-lung lavage. American journal of respiratory and critical care medicine. 2002 Jan 1:165(1):128-31 [PubMed PMID: 11779742]
Blount BC, Karwowski MP, Shields PG, Morel-Espinosa M, Valentin-Blasini L, Gardner M, Braselton M, Brosius CR, Caron KT, Chambers D, Corstvet J, Cowan E, De Jesús VR, Espinosa P, Fernandez C, Holder C, Kuklenyik Z, Kusovschi JD, Newman C, Reis GB, Rees J, Reese C, Silva L, Seyler T, Song MA, Sosnoff C, Spitzer CR, Tevis D, Wang L, Watson C, Wewers MD, Xia B, Heitkemper DT, Ghinai I, Layden J, Briss P, King BA, Delaney LJ, Jones CM, Baldwin GT, Patel A, Meaney-Delman D, Rose D, Krishnasamy V, Barr JR, Thomas J, Pirkle JL, Lung Injury Response Laboratory Working Group. Vitamin E Acetate in Bronchoalveolar-Lavage Fluid Associated with EVALI. The New England journal of medicine. 2020 Feb 20:382(8):697-705. doi: 10.1056/NEJMoa1916433. Epub 2019 Dec 20 [PubMed PMID: 31860793]
Layden JE, Ghinai I, Pray I, Kimball A, Layer M, Tenforde MW, Navon L, Hoots B, Salvatore PP, Elderbrook M, Haupt T, Kanne J, Patel MT, Saathoff-Huber L, King BA, Schier JG, Mikosz CA, Meiman J. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin - Final Report. The New England journal of medicine. 2020 Mar 5:382(10):903-916. doi: 10.1056/NEJMoa1911614. Epub 2019 Sep 6 [PubMed PMID: 31491072]
Lin J, Huang LL, Zhang JW, Ye MH, Feng JX. Endogenous lipoid pneumonia presenting as solitary pulmonary nodule: a case report. International journal of clinical and experimental pathology. 2015:8(8):9727-30 [PubMed PMID: 26464746]
Level 3 (low-level) evidenceButt YM, Smith ML, Tazelaar HD, Vaszar LT, Swanson KL, Cecchini MJ, Boland JM, Bois MC, Boyum JH, Froemming AT, Khoor A, Mira-Avendano I, Patel A, Larsen BT. Pathology of Vaping-Associated Lung Injury. The New England journal of medicine. 2019 Oct 31:381(18):1780-1781. doi: 10.1056/NEJMc1913069. Epub 2019 Oct 2 [PubMed PMID: 31577870]
Samhouri BF, Tandon YK, Hartman TE, Harada Y, Sekiguchi H, Yi ES, Ryu JH. Presenting Clinicoradiologic Features, Causes, and Clinical Course of Exogenous Lipoid Pneumonia in Adults. Chest. 2021 Aug:160(2):624-632. doi: 10.1016/j.chest.2021.02.037. Epub 2021 Feb 26 [PubMed PMID: 33647249]
Betancourt SL, Martinez-Jimenez S, Rossi SE, Truong MT, Carrillo J, Erasmus JJ. Lipoid pneumonia: spectrum of clinical and radiologic manifestations. AJR. American journal of roentgenology. 2010 Jan:194(1):103-9. doi: 10.2214/AJR.09.3040. Epub [PubMed PMID: 20028911]
Franquet T, Giménez A, Bordes R, Rodríguez-Arias JM, Castella J. The crazy-paving pattern in exogenous lipoid pneumonia: CT-pathologic correlation. AJR. American journal of roentgenology. 1998 Feb:170(2):315-7 [PubMed PMID: 9456935]
Sung S, Tazelaar HD, Crapanzano JP, Nassar A, Saqi A. Adult exogenous lipoid pneumonia: A rare and underrecognized entity in cytology - A case series. CytoJournal. 2018:15():17. doi: 10.4103/cytojournal.cytojournal_29_17. Epub 2018 Jul 13 [PubMed PMID: 30112015]
Level 2 (mid-level) evidenceYasui H, Yokomura K, Suda T. A severe case of acute exogenous lipoid pneumonia treated with systemic corticosteroid. Respiratory medicine case reports. 2016:17():64-7. doi: 10.1016/j.rmcr.2016.01.009. Epub 2016 Jan 25 [PubMed PMID: 27222789]
Level 3 (low-level) evidenceKim HJ, Lee WH, Jeong N, Lee JH, Park JH, Jang HJ, Kim HK. Lipoid pneumonitis in a patient with an accidental ingestion of kerosene successfully treated with bronchoscopic segmental lavage and systemic steroid: Case report. Medicine. 2018 Oct:97(41):e12786. doi: 10.1097/MD.0000000000012786. Epub [PubMed PMID: 30313102]
Level 3 (low-level) evidenceRebuli ME, Rose JJ, Noël A, Croft DP, Benowitz NL, Cohen AH, Goniewicz ML, Larsen BT, Leigh N, McGraw MD, Melzer AC, Penn AL, Rahman I, Upson D, Crotty Alexander LE, Ewart G, Jaspers I, Jordt SE, Kligerman S, Loughlin CE, McConnell R, Neptune ER, Nguyen TB, Pinkerton KE, Witek TJ Jr. The E-cigarette or Vaping Product Use-Associated Lung Injury Epidemic: Pathogenesis, Management, and Future Directions: An Official American Thoracic Society Workshop Report. Annals of the American Thoracic Society. 2023 Jan:20(1):1-17. doi: 10.1513/AnnalsATS.202209-796ST. Epub [PubMed PMID: 36584985]
Level 3 (low-level) evidence