Introduction
Medical imaging plays a key role in the diagnosis and management of appendiceal diseases. In general, appendiceal diseases fall into 2 broad categories: infectious or inflammatory disorders and neoplastic conditions.
Acute appendicitis is a common cause of abdominal pain, with an estimated lifetime risk of 7% to 9%.[1] Classic clinical manifestations include periumbilical pain that localizes to the right lower quadrant (RLQ), along with nausea, vomiting, anorexia, and fever. RLQ pain is typically centered at the McBurney point, located halfway between the umbilicus and the anterior superior iliac spine.[2] Acute appendicitis may result from obstruction, often caused by an appendicolith (see Image. Early Acute Appendicitis with Appendicolith). The condition may be complicated by perforation, with an estimated risk of 2% at 36 hours after symptom onset, increasing by approximately 5% for every additional 12 hours thereafter.[3] Progressive inflammation may lead to increasing tenderness on palpation and guarding. Timely diagnosis of acute appendicitis is crucial due to its potential complications, including perforation and abscess formation (see Image. Acute Appendicitis with Developing Abscess on Computed Tomography).[4][5][6]
The latter category of appendiceal diseases, neoplastic processes, includes epithelial tumors, neuroendocrine tumors (NETs), lymphoma, mesenchymal tumors, sarcomas, and metastases.[7] Most appendiceal neoplasms are epithelial tumors or NETs, with epithelial tumors occurring most commonly in middle-aged and older adults and NETs occurring more frequently in younger patients.[8] Although appendiceal neoplasms are typically asymptomatic, progressive growth can cause luminal obstruction and subsequent acute appendicitis.[9] Neoplastic processes may also present with vague RLQ pain or a palpable mass in the area. Pseudomyxoma peritonei is a severe complication of mucinous appendiceal neoplasms and is characterized by mucin accumulation within the peritoneum and along the serosal surfaces of abdominal and pelvic organs.[10]
Anatomy
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy
The vermiform appendix is a vestigial organ located at the terminal end of the cecum. Grossly, a reliable landmark for identifying the appendiceal base is the convergence of the taeniae coli. The appendix is a true diverticulum because the appendiceal wall contains the same layers as the colon: mucosa, submucosa, longitudinal and circular muscularis propria, and serosa. The appendix also contains scattered B- and T-cell lymphoid aggregates within the mucosa and submucosa—a feature that distinguishes appendiceal tissue from the adjacent colonic tissue from which the organ develops.[11]
Although the location of the appendiceal base is relatively constant, the position of the appendiceal tip is highly variable. Retrocecal positioning is most common, although subcecal, preileal, postileal, and pelvic locations also occur. Appendiceal position may vary with respiration, overlying bowel gas, and patient positioning.[12] Variability in appendiceal location contributes to the diverse clinical presentations of acute appendicitis. The average appendiceal length ranges from 8 to 10 cm, and the average appendiceal diameter is approximately 7 mm, with a typical wall thickness of 2 mm.[13] The appendiceal diameter and wall thickness are important imaging markers of inflammation. In most clinical settings, an appendiceal diameter greater than 7 mm (or greater than 6 mm according to some criteria) and a wall thickness greater than 2 to 3 mm support the diagnosis of acute appendicitis.
Plain Films
Radiography has limited clinical utility in appendiceal imaging. Abdominal radiographs may incidentally demonstrate an appendicolith, which appears as a small calcified RLQ lesion. However, this finding lacks specificity for acute appendicitis.[14] Another radiographic finding associated with complicated appendicitis is pneumoperitoneum. Visible pneumoperitoneum is uncommon, even in the setting of perforation, because most perforations remain locally contained.[15] Overall, abdominal radiographs obtained for acute abdominal pain demonstrate poor sensitivity and specificity for the diagnosis of acute appendicitis. However, identification of bowel obstruction or free intraperitoneal air may aid the diagnosis of other urgent or emergent conditions.[16]
Computed Tomography
Computed tomography (CT) is one of the primary imaging modalities used to evaluate appendiceal disorders. CT has a sensitivity of 87% and a specificity of 76% for detecting acute appendicitis (see Image. Early Acute Appendicitis on Computed Tomography).[17] Oral and rectal contrast administration generally provides little additional diagnostic benefit. Therefore, intravenous contrast-enhanced CT is the preferred imaging technique for diagnosis. Acute appendicitis is classically diagnosed by identifying an enlarged appendix greater than 6 mm in diameter, wall thickening greater than 3 mm, mural hyperenhancement, and surrounding inflammatory changes manifested by periappendiceal fat stranding or free fluid.[18] An obstructing appendicolith may also be identified, although the absence of an appendicolith does not exclude the diagnosis.
The optimal CT diameter threshold for the diagnosis of acute appendicitis is a subject of debate. Some recent studies suggest that a diameter threshold greater than 6 mm is overly sensitive and may contribute to negative appendectomies. Although a 6-mm threshold may be appropriate in pediatric populations, many adults have a normal appendiceal diameter of 6 to 7 mm. Therefore, several studies advocate a diameter threshold greater than 7 mm to improve the diagnostic performance of CT.[19]
CT has a sensitivity of 95% for detecting appendiceal neoplasms in symptomatic patients.[20] Intravenous contrast, as well as oral contrast, may improve tumor detection and staging. Imaging features include appendiceal enlargement, often greater than 15 mm in diameter, cystic dilatation, or a soft-tissue mass. Mucoceles may also be present and can vary in size according to the underlying etiology. Mucoceles measuring less than 2 cm are more likely to result from luminal obstruction, whereas neoplasms typically produce larger mucoceles.[21] CT typically demonstrates a dilated appendix containing homogeneous low-attenuation material, with or without irregular or nodular wall thickening. Additional findings may include a soft-tissue mass, periappendiceal fat stranding, invasion of adjacent structures, or lymphadenopathy.
Imaging of suspected NET on CT typically reveals a small submucosal mass in the distal appendix, usually less than 1 to 2 cm, with avid enhancement, calcifications, or both.[22] Small NETs may remain below the resolution limits of imaging studies.
Magnetic Resonance
Magnetic resonance imaging (MRI) has increasingly been used in pregnant and pediatric populations due to the absence of ionizing radiation (see Image. Acute Appendicitis and Intrauterine Pregnancy on Magnetic Resonance Imaging). MRI demonstrates a sensitivity of 96% and a specificity of 96% for identifying appendicitis, although appendix visualization has been reported as slightly more successful in adults than in children.[23] Imaging criteria for acute appendicitis include visualization of an enlarged appendix greater than 7 mm in diameter, wall thickening greater than 2 mm, periappendiceal fat stranding, a fluid-filled appendix, or free fluid. These imaging findings are consistent across multiple modalities.
MRI for appendiceal evaluation is typically performed without contrast, although imaging protocols vary across institutions (see Image. Acute Appendicitis and Appendicolith on Magnetic Resonance Imaging). Given the relatively long acquisition time of MRI compared with other modalities such as CT, multiple studies have investigated methods to shorten acquisition time. A recent open-access MRI protocol with a 12-minute acquisition time achieved 98% diagnostic accuracy for acute appendicitis and demonstrated high accuracy in pregnant patients and adolescents—populations most commonly evaluated with MRI for appendicitis.[24] Deep learning techniques have also contributed to reduced scan times and improved MRI diagnostic quality.[25]
MRI also plays a primary role in staging appendiceal neoplasms and demonstrates higher accuracy than CT in this setting. Diagnostic performance improves with the addition of diffusion-weighted imaging, which aids in the detection of highly cellular tumor implants. Solid tumors exhibit restricted diffusion, allowing differentiation from adjacent structures. MRI achieves a sensitivity of 95% and a specificity of 70% when combined with delayed gadolinium-enhanced imaging and oral and rectal contrast administration.[26]
Ultrasonography
Ultrasound is a commonly used imaging modality for evaluating appendicitis (see Image. Acute Appendicitis on Ultrasound). As with MRI, ultrasound does not utilize ionizing radiation or contrast agents and is, therefore, beneficial in pediatric and pregnant patient populations. Ultrasound is more readily available and cost-effective than MRI and is often performed as the initial imaging study in suspected appendicitis. A key limitation of this technique is the visualization of the appendix, as patient body habitus, increased visceral or subcutaneous fat, or a large stool burden may impede visualization. Ultrasound performance is also highly operator-dependent, varying with sonographer experience and institutional volume. Some facilities perform ultrasound for appendicitis evaluation daily, whereas others encounter the condition less frequently.
Ultrasound has been shown to be highly effective in the pediatric population, with a diagnostic accuracy of 96% and a visualization rate of 91%.[27] Ultrasound demonstrates lower sensitivity and detection rates in adult populations, although specificity remains high for the diagnosis of appendicitis.[28]
The examination uses graded compression and evaluates for key sonographic features, including an appendiceal diameter greater than 6 mm, periappendiceal fat stranding or inflammation, free fluid, reactive lymph nodes, and mural hyperplasia.[29] Periappendiceal inflammation is one of the most reliable sonographic signs of appendicitis, and the absence of this finding strongly supports exclusion of the diagnosis.
A common sonographic mimic of appendicitis is lymphoid hyperplasia, a benign condition characterized by enlargement of the appendiceal wall, particularly within the lamina propria.[30] The lamina propria appears as a hypoechoic innermost layer of the appendix. Thickening greater than 0.8 mm is diagnostic of lymphoid hyperplasia, even in the presence of an overall enlarged appendix.[31] This condition is managed nonoperatively and is typically associated with inflammatory conditions, such as viral enteritis.
Mucoceles may also be detected on ultrasound when evaluating for appendiceal neoplasms. Mucoceles appear as ovoid cystic masses with variable echogenicity. Sonographic features include concentric echogenic layers (onion skin appearance), acoustic shadowing from mural calcifications, and a pear-shaped appendix. Regional lymphadenopathy, periappendiceal fat stranding, and free fluid may also be evident.[32]
Nuclear Medicine
Nuclear medicine studies are primarily utilized for staging proven appendiceal cancers using positron emission tomography (PET). Radiotracer selection depends on tumor histology. Common options include fluorodeoxyglucose for appendiceal carcinomas and 68Ga-DOTATATE (gallium-68 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid–tyrosine 3-octreotate) for neuroendocrine neoplasms. Evaluation of mucinous appendiceal neoplasms is limited on PET/CT, particularly fluorodeoxyglucose PET, due to the hypocellular composition of these tumors.[33] Continued progress is observed in the development of PET radiotracers. PET/CT imaging with 18F-fibroblast activation protein inhibitor has demonstrated clinical utility as a supplemental PET agent in the evaluation of appendiceal neoplasms.[34]
Clinical Significance
Acute appendicitis may be established clinically after a thorough history and physical examination. However, imaging is frequently used for confirmation. Multiple imaging modalities are available to aid clinical assessment, including ultrasound, CT, and MRI. The choice of imaging modality depends on availability and patient demographics.
CT is the most commonly used imaging modality due to its speed, sensitivity, and specificity. Ultrasound is often the first-line imaging modality in pediatric populations and demonstrates high diagnostic accuracy. Differences in technologist experience with appendiceal imaging across patient populations make operator dependence a major confounding factor in ultrasound evaluation. MRI is not always readily available but is increasingly utilized in the evaluation of appendicitis, particularly in pediatric and pregnant populations. Continued improvements in MRI speed and diagnostic performance are expected to further expand its clinical utility.
Although less commonly performed, imaging for appendiceal neoplasms demonstrates high sensitivity and specificity. The diagnostic yield increases in symptomatic patients, as appendiceal neoplasms may present with symptoms mimicking acute appendicitis, as well as generalized abdominal pain, a palpable mass, or bowel obstruction. Imaging studies, including PET/CT, are primarily utilized for staging. These studies more frequently identify epithelial tumors, whereas NETs are less commonly detected due to their small size and nonaggressive behavior. Definitive diagnosis of appendiceal neoplasms requires pathologic examination following appendectomy.
Negative appendectomy rates are below 12% in men but may reach up to 33% in women. Improved imaging accuracy may reduce unnecessary surgical intervention.[35] Selection of the most appropriate imaging study is essential to optimize diagnostic yield in specific clinical scenarios. Imaging findings for acute appendicitis may occasionally be equivocal. Clinical correlation with physical examination and relevant laboratory values is necessary in such scenarios. The Pediatric Appendicitis Score (PAS) is a commonly used clinical scoring tool and has demonstrated utility as an adjunct in the diagnosis of appendicitis.[36]
Media
(Click Image to Enlarge)

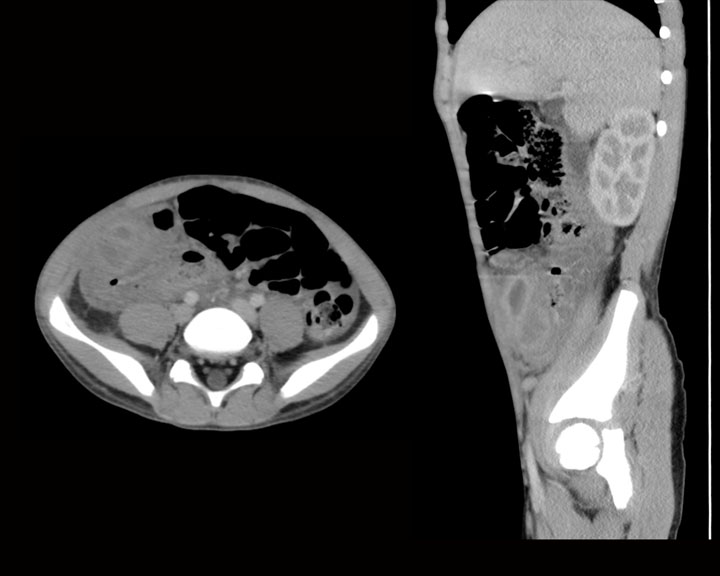
Early Acute Appendicitis With Appendicolith. This computed tomography scan shows early acute appendicitis with a dilated, fluid-filled appendix. The appendix contains an appendicolith and is positioned directly resting on the urinary bladder.
Contributed by K Carter, DO
(Click Image to Enlarge)
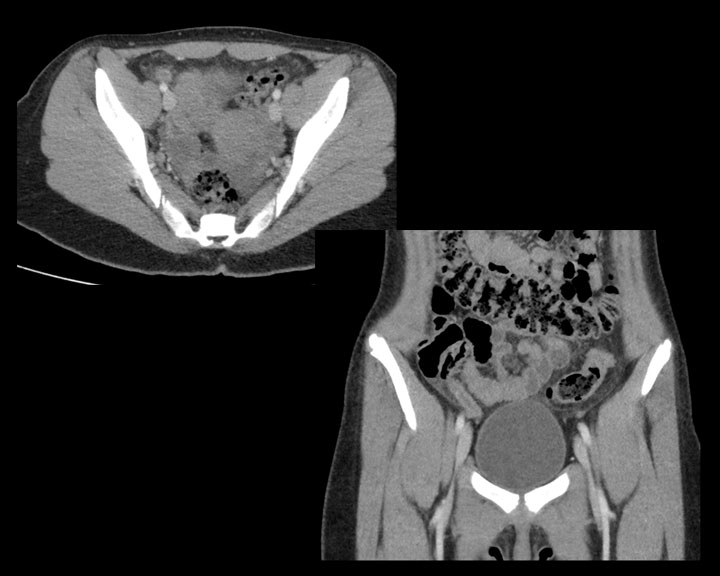
Acute Appendicitis With Developing Abscess on Computed Tomography. Axial and sagittal images demonstrate acute appendicitis in the right lower quadrant. A dilated, fluid-filled tubular structure is visible alongside a surrounding fluid collection and stranding, consistent with a developing abscess.
Contributed by K Carter, DO
(Click Image to Enlarge)
Early Acute Appendicitis on Computed Tomography. A mildly dilated appendix filled with fluid is visible, along with adjacent fat stranding, in the right lower quadrant.
Contributed by K Carter, DO
(Click Image to Enlarge)
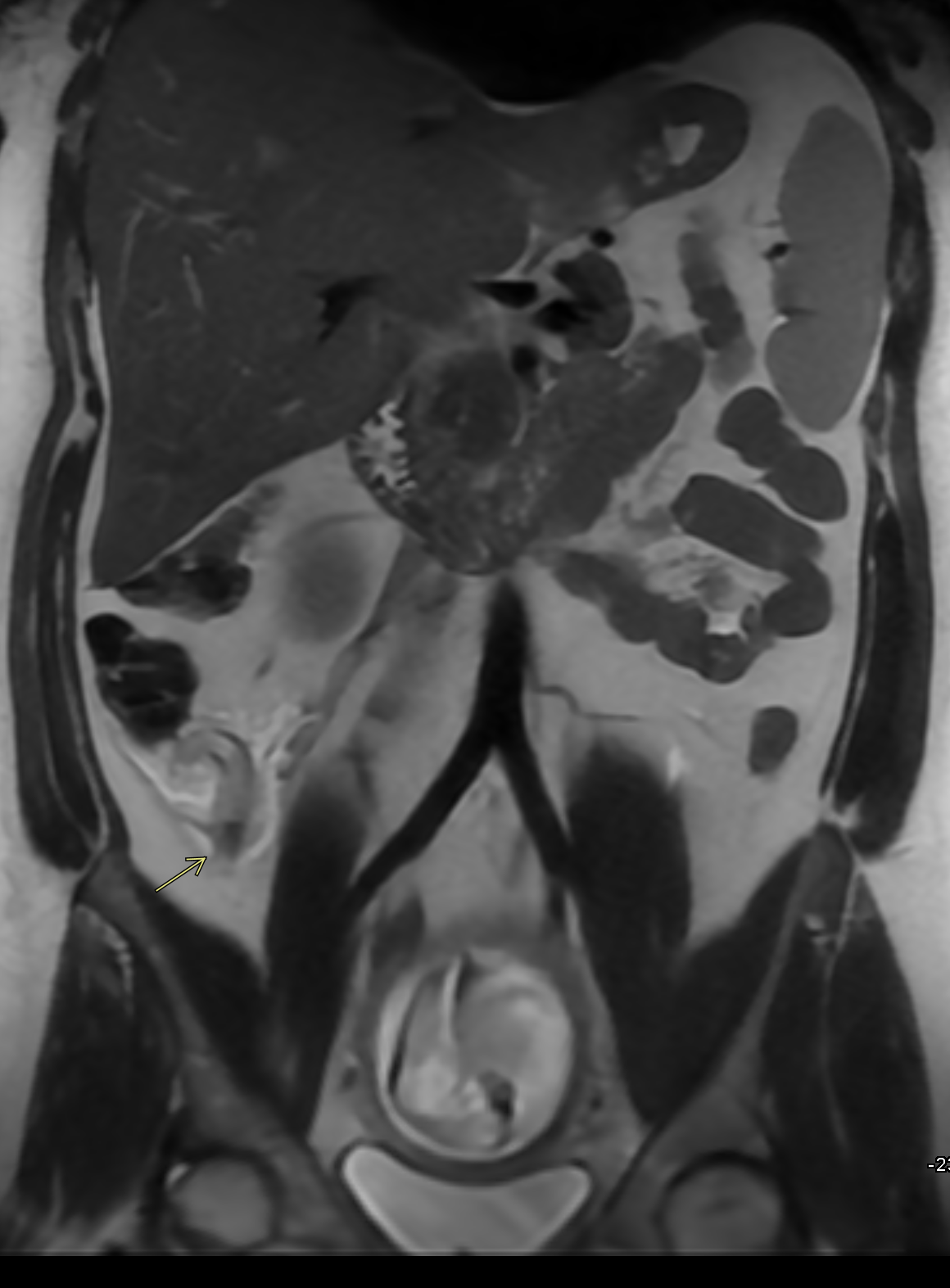
Acute Appendicitis and Intrauterine Pregnancy on Magnetic Resonance Imaging. A coronal single-shot fast spin echo abdominal scan shows a dilated appendix measuring up to 10 mm with surrounding inflammatory changes. An intrauterine pregnancy is noted as a partial finding in the lower field.
Contributed by G Durupt, DO
(Click Image to Enlarge)
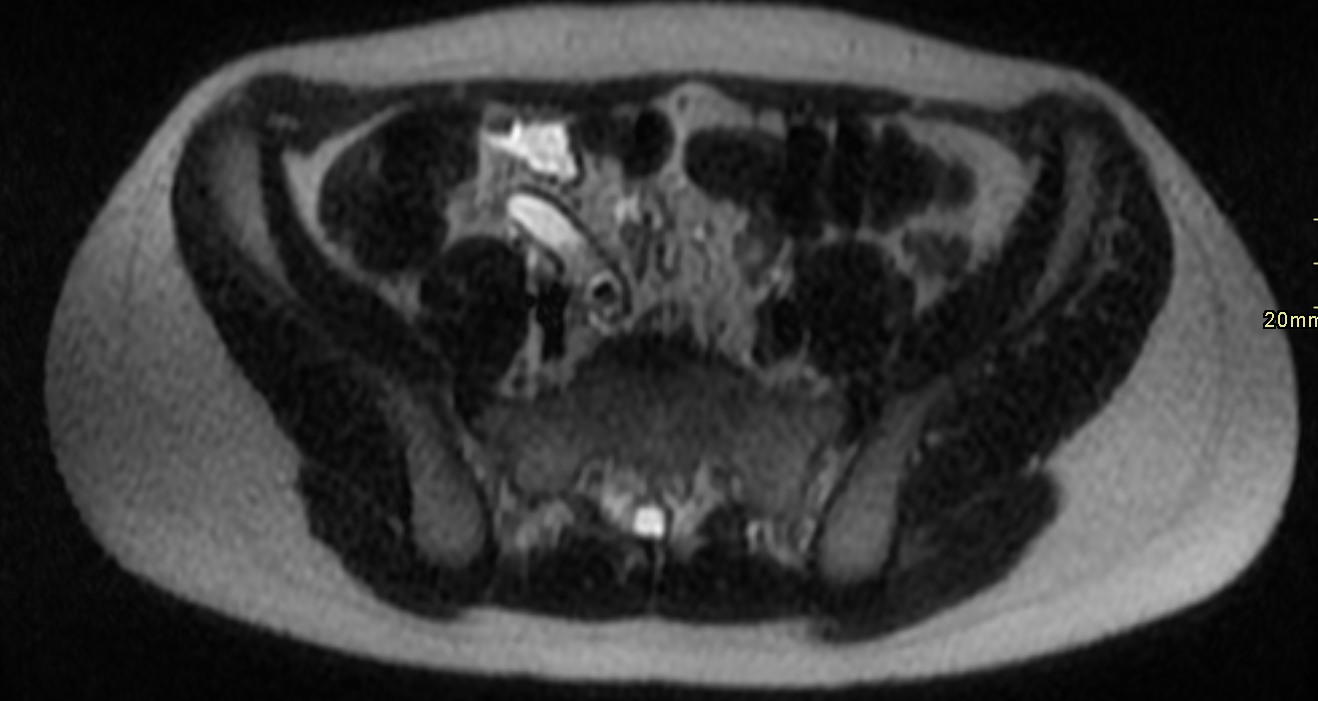
Acute Appendicitis and Appendicolith on Magnetic Resonance Imaging. This axial T2-weighted scan reveals a dilated appendix measuring 11 mm. The tip of the appendix shows a small amount of periappendiceal fluid and an ovoid filling defect consistent with an appendicolith.
Contributed by G Durupt, DO
(Click Image to Enlarge)

Acute Appendicitis on Ultrasound. A blind-ending tubular structure is identified in the right lower quadrant, measuring up to 7 mm in diameter.
Contributed by K Carter, DO
References
Humes D, Speake WJ, Simpson J. Appendicitis. BMJ clinical evidence. 2007 Jul 1:2007():. pii: 0408. Epub 2007 Jul 1 [PubMed PMID: 19454096]
Level 1 (high-level) evidenceGrover CA, Sternbach G. Charles McBurney: McBurney's point. The Journal of emergency medicine. 2012 May:42(5):578-81. doi: 10.1016/j.jemermed.2011.06.039. Epub 2011 Oct 5 [PubMed PMID: 21982626]
Bickell NA, Aufses AH Jr, Rojas M, Bodian C. How time affects the risk of rupture in appendicitis. Journal of the American College of Surgeons. 2006 Mar:202(3):401-6 [PubMed PMID: 16500243]
Level 2 (mid-level) evidenceLeonards LM, Pahwa A, Patel MK, Petersen J, Nguyen MJ, Jude CM. Neoplasms of the Appendix: Pictorial Review with Clinical and Pathologic Correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 2017 Jul-Aug:37(4):1059-1083. doi: 10.1148/rg.2017160150. Epub 2017 Jun 9 [PubMed PMID: 28598731]
Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet (London, England). 2015 Sep 26:386(10000):1278-1287. doi: 10.1016/S0140-6736(15)00275-5. Epub [PubMed PMID: 26460662]
Level 3 (low-level) evidenceLotfollahzadeh S, Lopez RA, Deppen JG. Appendicitis. StatPearls. 2026 Jan:(): [PubMed PMID: 29630245]
Tang LH. Epithelial neoplasms of the appendix. Archives of pathology & laboratory medicine. 2010 Nov:134(11):1612-20 [PubMed PMID: 21043814]
Wu H, Chintagumpala M, Hicks J, Nuchtern JG, Okcu MF, Venkatramani R. Neuroendocrine Tumor of the Appendix in Children. Journal of pediatric hematology/oncology. 2017 Mar:39(2):97-102. doi: 10.1097/MPH.0000000000000598. Epub [PubMed PMID: 27306228]
Komo T, Kohashi T, Hihara J, Oishi K, Yoshimitsu M, Kanou M, Nakashima A, Aoki Y, Miguchi M, Kaneko M, Mukaida H, Hirabayashi N. Intestinal obstruction caused by low-grade appendiceal mucinous neoplasm: A case report and review of the literature. International journal of surgery case reports. 2018:51():37-40. doi: 10.1016/j.ijscr.2018.08.001. Epub 2018 Aug 9 [PubMed PMID: 30138868]
Level 3 (low-level) evidenceRizvi SA, Syed W, Shergill R. Approach to pseudomyxoma peritonei. World journal of gastrointestinal surgery. 2018 Aug 27:10(5):49-56. doi: 10.4240/wjgs.v10.i5.49. Epub [PubMed PMID: 30190782]
Mizumoto T. B and T cells in lymphoid tissues of human appendix. International archives of allergy and applied immunology. 1976:51(1):80-93 [PubMed PMID: 132409]
Hodge BD, Kashyap S, Khorasani-Zadeh A. Anatomy, Abdomen and Pelvis: Appendix. StatPearls. 2026 Jan:(): [PubMed PMID: 29083761]
Willekens I, Peeters E, De Maeseneer M, de Mey J. The normal appendix on CT: does size matter? PloS one. 2014:9(5):e96476. doi: 10.1371/journal.pone.0096476. Epub 2014 May 6 [PubMed PMID: 24802879]
Level 2 (mid-level) evidenceUlukaya Durakbaşa C, Taşbaşi I, Tosyali AN, Mutus M, Sehiralti V, Zemheri E. An evaluation of individual plain abdominal radiography findings in pediatric appendicitis: results from a series of 424 children. Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES. 2006 Jan:12(1):51-8 [PubMed PMID: 16456751]
Campos Canelas AL, Fernandez HM, Crociati Meguins L, Silva Barros S, Crociati Meguins EM, Ishak G, Rodrigues De Moraes LA. Pneumoperitoneum in association with perforated appendicitis in a Brazilian Amazon woman. Case report. Il Giornale di chirurgia. 2010 Mar:31(3):80-2 [PubMed PMID: 20426916]
Level 3 (low-level) evidencevan Randen A, Laméris W, Luitse JS, Gorzeman M, Hesselink EJ, Dolmans DE, Peringa J, van Geloven AA, Bossuyt PM, Stoker J, Boermeester MA, OPTIMA study group. The role of plain radiographs in patients with acute abdominal pain at the ED. The American journal of emergency medicine. 2011 Jul:29(6):582-589.e2. doi: 10.1016/j.ajem.2009.12.020. Epub 2010 Apr 24 [PubMed PMID: 20825832]
Iamwat J, Teerasamit W, Apisarnthanarak P, Noppakunsomboon N, Kaewlai R. Predictive ability of CT findings in the differentiation of complicated and uncomplicated appendicitis: a retrospective investigation of 201 patients undergone appendectomy at initial admission. Insights into imaging. 2021 Oct 21:12(1):143. doi: 10.1186/s13244-021-01086-3. Epub 2021 Oct 21 [PubMed PMID: 34674054]
Level 2 (mid-level) evidencePark G, Lee SC, Choi BJ, Kim SJ. Stratified computed tomography findings improve diagnostic accuracy for appendicitis. World journal of gastroenterology. 2014 Oct 14:20(38):13942-9. doi: 10.3748/wjg.v20.i38.13942. Epub [PubMed PMID: 25320531]
Level 2 (mid-level) evidenceMoskowitz E, Khan AD, Cribari C, Schroeppel TJ. Size matters: Computed tomographic measurements of the appendix in emergency department scans. American journal of surgery. 2019 Aug:218(2):271-274. doi: 10.1016/j.amjsurg.2018.12.010. Epub 2018 Dec 11 [PubMed PMID: 30558802]
Pickhardt PJ, Levy AD, Rohrmann CA Jr, Kende AI. Primary neoplasms of the appendix manifesting as acute appendicitis: CT findings with pathologic comparison. Radiology. 2002 Sep:224(3):775-81 [PubMed PMID: 12202713]
Level 2 (mid-level) evidenceSpyropoulos C, Rentis A, Alexaki E, Triantafillidis JK, Vagianos C. Appendiceal mucocele and pseudomyxoma peritonei; the clinical boundaries of a subtle disease. The American journal of case reports. 2014 Aug 27:15():355-60. doi: 10.12659/AJCR.890837. Epub 2014 Aug 27 [PubMed PMID: 25163976]
Level 3 (low-level) evidenceBayhan Z, Yildiz YA, Akdeniz Y, Gonullu E, Altintoprak F, Mantoglu B, Capoglu R, Kahyaoglu Akkaya Z. Appendix Neuroendocrine Tumor: Retrospective Analysis of 4026 Appendectomy Patients in a Single Center. Emergency medicine international. 2020:2020():4030527. doi: 10.1155/2020/4030527. Epub 2020 Sep 3 [PubMed PMID: 32963833]
Level 2 (mid-level) evidenceDuke E, Kalb B, Arif-Tiwari H, Daye ZJ, Gilbertson-Dahdal D, Keim SM, Martin DR. A Systematic Review and Meta-Analysis of Diagnostic Performance of MRI for Evaluation of Acute Appendicitis. AJR. American journal of roentgenology. 2016 Mar:206(3):508-17. doi: 10.2214/AJR.15.14544. Epub [PubMed PMID: 26901006]
Level 1 (high-level) evidenceJones AO, Nol J. Open-Access 12-Minute MRI Screening for Acute Appendicitis: A Five-Year Retrospective Observational Study of Diagnostic Accuracy. Journal of clinical medicine. 2024 Nov 28:13(23):. doi: 10.3390/jcm13237257. Epub 2024 Nov 28 [PubMed PMID: 39685716]
Level 2 (mid-level) evidenceLiu JJ, Lin C, Liu W, Zhu L, Ma CX, Wang X, Xu J, Lu YT, Zhang YF, Jiang B, Wang WB, Feng F. Rapid MR examination with deep learning reconstruction improves diagnosis of complicated acute appendicitis. European journal of radiology. 2026 Feb:195():112554. doi: 10.1016/j.ejrad.2025.112554. Epub 2025 Nov 19 [PubMed PMID: 41289720]
Kim DW, Suh CH, Yoon HM, Kim JR, Jung AY, Lee JS, Cho YA. Visibility of Normal Appendix on CT, MRI, and Sonography: A Systematic Review and Meta-Analysis. AJR. American journal of roentgenology. 2018 Sep:211(3):W140-W150. doi: 10.2214/AJR.17.19321. Epub 2018 Jul 24 [PubMed PMID: 30040469]
Level 1 (high-level) evidenceRoberts K, Moore H, Raju M, Gent R, Piotto L, Taranath A, Ee M, Linke R, Goh DW. Diagnostic Ultrasound for Acute Appendicitis: The Gold Standard. Journal of pediatric surgery. 2024 Feb:59(2):235-239. doi: 10.1016/j.jpedsurg.2023.10.028. Epub 2023 Oct 20 [PubMed PMID: 37985334]
Lock A, Necas M. Diagnostic Performance of Ultrasound in Adult Appendicitis. A Retrospective Review of 331 Cases. Journal of medical radiation sciences. 2026 Mar 11:():. doi: 10.1002/jmrs.70079. Epub 2026 Mar 11 [PubMed PMID: 41814672]
Level 2 (mid-level) evidencePacharn P, Ying J, Linam LE, Brody AS, Babcock DS. Sonography in the evaluation of acute appendicitis: are negative sonographic findings good enough? Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2010 Dec:29(12):1749-55 [PubMed PMID: 21098847]
Level 2 (mid-level) evidenceXu Y, Jeffrey RB, DiMaio MA, Olcott EW. Lymphoid Hyperplasia of the Appendix: A Potential Pitfall in the Sonographic Diagnosis of Appendicitis. AJR. American journal of roentgenology. 2016 Jan:206(1):189-94. doi: 10.2214/AJR.15.14846. Epub [PubMed PMID: 26700351]
Kwon LM, Lee K, Min SK, Ahn SM, Ha HI, Kim MJ. Ultrasound features of secondary appendicitis in pediatric patients. Ultrasonography (Seoul, Korea). 2018 Jul:37(3):233-243. doi: 10.14366/usg.17029. Epub 2017 Aug 25 [PubMed PMID: 29141286]
Sanchez TR, Corwin MT, Davoodian A, Stein-Wexler R. Sonography of Abdominal Pain in Children: Appendicitis and Its Common Mimics. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine. 2016 Mar:35(3):627-35. doi: 10.7863/ultra.15.04047. Epub 2016 Feb 18 [PubMed PMID: 26892821]
Berger KL, Nicholson SA, Dehdashti F, Siegel BA. FDG PET evaluation of mucinous neoplasms: correlation of FDG uptake with histopathologic features. AJR. American journal of roentgenology. 2000 Apr:174(4):1005-8 [PubMed PMID: 10749239]
Level 2 (mid-level) evidenceDong Y, Huang S, Wu H, Cao M, Huang Y, Tang G, Zhou W. Superiority of (18)F-FAPI-42 PET/CT in the detection of primary tumor and management of appendiceal neoplasm to (18)F-FDG PET/CT and CE-CT. Cancer imaging : the official publication of the International Cancer Imaging Society. 2024 May 7:24(1):58. doi: 10.1186/s40644-024-00706-7. Epub 2024 May 7 [PubMed PMID: 38715096]
Joshi MK, Joshi R, Alam SE, Agarwal S, Kumar S. Negative Appendectomy: an Audit of Resident-Performed Surgery. How Can Its Incidence Be Minimized? The Indian journal of surgery. 2015 Dec:77(Suppl 3):913-7. doi: 10.1007/s12262-014-1063-0. Epub 2014 Apr 9 [PubMed PMID: 27011482]
Attia MW. The Paediatric Appendicitis Score (PAS) was useful in children with acute abdominal pain. Evidence-based medicine. 2009 Feb:14(1):26. doi: 10.1136/ebm.14.1.26. Epub [PubMed PMID: 19181958]