Introduction
Allergic bronchopulmonary aspergillosis (ABPA) is an immune-mediated hypersensitivity reaction to Aspergillus species colonizing the airways, most commonly affecting patients with asthma or cystic fibrosis. Emerging evidence indicates that ABPA also occurs in individuals with COPD, post-tuberculosis lung disease, and non–cystic fibrosis bronchiectasis; however, asthma and cystic fibrosis remain the primary risk populations.[1] The Infectious Diseases Society of America (IDSA) classifies ABPA as an allergic syndrome rather than an invasive fungal infection.[2] In susceptible individuals, airway colonization by Aspergillus fumigatus triggers an exaggerated immune response characterized by elevated total immunoglobulin E (IgE), Aspergillus-specific IgE and IgG antibodies, and eosinophilia. The resulting inflammatory reaction produces the clinical manifestations of ABPA.
ABPA commonly presents as poorly controlled asthma, mucoid impaction (sometimes mistaken for pneumonia), persistent eosinophilia, bronchiectasis, and immunologic evidence of allergy to Aspergillus antigens.[3][4][5] In patients with cystic fibrosis, it typically manifests as difficult-to-control exacerbations that respond to corticosteroids. If untreated, ABPA may progress to bronchiectasis, pulmonary fibrosis, and irreversible lung damage. Rarely, fungi other than Aspergillus can produce a similar syndrome, allergic bronchopulmonary mycosis (ABPM), and some patients with severe asthma exhibit fungal sensitization without meeting full diagnostic criteria, a condition termed severe asthma with fungal sensitization.[6] Treatment strategies target both suppression of the immune response and reduction of fungal burden to decrease antigenic stimulation.[2]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Aspergillus species are ubiquitous environmental molds commonly found in soil and decaying organic matter. More than 100 species are known worldwide. However, most human infections are caused by A fumigatus, with A flavus, A niger, and A terreus accounting for a smaller proportion of infections.[7] Clinical manifestations vary widely and depend largely on host immune status, ranging from hypersensitivity reactions to invasive angioinvasive disease.
A fumigatus is the species most frequently implicated in ABPA.[8][9] This species' small conidia (2–3 μm) can bypass upper airway defenses and reach the distal airways, where they colonize the bronchial tree.[10] ABPA primarily affects patients with asthma or cystic fibrosis who develop hypersensitivity to inhaled fungal antigens. Impaired mucociliary clearance promotes persistent colonization, triggering an exaggerated immune response that may lead to mucus plugging, airway inflammation, and central bronchiectasis if untreated. Genetic susceptibility also appears to contribute to disease risk. The human leukocyte antigen (HLA)-DR alleles DR2 and DR5, and possibly DR4 or DR7, have been associated with increased susceptibility, whereas HLA-DQ2 may confer relative protection, suggesting that host immune factors influence disease expression.[11][12]
Epidemiology
ABPA occurs across all age groups, but diagnosis occurs more frequently in adults. Growing awareness and improved screening have led to increased recognition in pediatric populations.[5][13] Sensitization to Aspergillus, demonstrated by a positive skin prick test or elevated Aspergillus-specific IgE, is present in approximately 25% of patients with asthma and up to 50% of those with cystic fibrosis; however, only a subset of sensitized individuals develop ABPA.
Researchers estimate that allergic bronchopulmonary aspergillosis affects more than 4.8 million people worldwide.[14] Reported prevalence among adults with asthma is approximately 11%, with similar estimates near 10% in pediatric populations. However, many of these data originate from tertiary care centers and likely overestimate prevalence in the general community.[5]
Population-based data from the United States suggest a substantially lower overall prevalence, estimated at approximately 1 to 3 cases per 10,000 patients with asthma. The prevalence increases markedly with asthma severity, reaching approximately 3% to 7% among patients with severe asthma. Researchers typically estimate the overall prevalence of ABPA in individuals with cystic fibrosis at approximately 9%, although it varies widely across populations and geographic regions.[15]
Pathophysiology
ABPA reflects immune dysregulation rather than immune deficiency. The pathogenesis is not fully understood; current evidence suggests that the disorder results from a complex interplay between host immune susceptibility and airway colonization by A fumigatus.[11][16] Not all patients with asthma develop ABPA despite similar environmental exposures, supporting the concept that genetic predisposition plays a central role.
In susceptible individuals, inhaled conidia germinate into hyphae within the airways, leading to persistent colonization rather than invasive infection. Fungal antigens elicit both innate and adaptive immune responses, resulting in a predominantly T helper type 2 (Th2)-mediated hypersensitivity reaction. ABPA is classically associated with type I (IgE-mediated) and Type III (immune complex–mediated) hypersensitivity responses. Activation of Th2 lymphocytes promotes the release of cytokines such as interleukin (IL)-4, IL-5, and IL-13, resulting in elevated IgE levels, eosinophilia, mast cell activation, and mucus hypersecretion. Recurrent inflammation contributes to airway remodeling and the development of bronchiectasis.[17][18]
Normally, mucociliary function and innate immune defenses clear inhaled conidia. However, impaired airway clearance in patients with asthma and cystic fibrosis allows persistent fungal colonization that triggers an exaggerated allergic response. Additional risk factors beyond asthma and cystic fibrosis are structural lung disease and chronic glucocorticoid use. Fungal proteases further disrupt epithelial barrier function, facilitating antigen penetration and amplifying the inflammatory cascade. Unlike invasive aspergillosis, which primarily affects immunocompromised hosts, ABPA typically develops in immunocompetent but atopic individuals with abnormal immune reactivity.[19] Isolation of Aspergillus from respiratory secretions may represent colonization; however, in predisposed patients, colonization can provoke chronic allergic inflammation that produces the characteristic clinical manifestations of ABPA.
Histopathology
Histopathologic findings in ABPA include chronic airway inflammation with prominent eosinophilic infiltration, mucus impaction, and airway remodeling that may progress to structural damage and central bronchiectasis. Bronchi often contain thick plugs of allergic mucin composed of degenerating eosinophils, fungal hyphae, fibrin, inflammatory cells, Charcot-Leyden crystals, and Curschmann spirals. The hyphae are typically septate and demonstrate acute-angle branching at approximately 45°, a characteristic feature of Aspergillus species (see Image. Aspergillus Hyphae). Bronchocentric granulomatosis may be observed in some cases, reflecting airway-centered granulomatous inflammation associated with hypersensitivity to fungal antigens. Although fibrosis may develop in advanced disease, ABPA remains primarily an airway-centered inflammatory process rather than a parenchymal invasive infection.[16][17]
History and Physical
Clinical Presentation
ABPA often presents with worsening respiratory symptoms in patients with asthma or cystic fibrosis despite appropriate therapy. Patients frequently report recurrent episodes of wheezing, cough, and dyspnea, along with radiographic findings of transient or “fleeting” pulmonary infiltrates and central bronchiectasis. Expectoration of thick, brownish mucus plugs is a classic feature and should raise strong clinical suspicion.[16][20]
Although wheezing is common, it may be absent during periods of disease quiescence. Some patients have incidentally discovered pulmonary infiltrates on imaging obtained for worsening asthma control. Additional symptoms may include pleuritic chest pain, hemoptysis, fatigue, and low-grade fever. Constitutional symptoms such as anorexia or weight loss are less typical but may occur in advanced disease.
ABPA is strongly associated with poorly controlled asthma characterized by increased exacerbation frequency despite optimized therapy. In patients with cystic fibrosis, the disorder often manifests as recurrent pulmonary exacerbations that respond more favorably to corticosteroids than to antibiotics. ABPA may also coexist with allergic fungal sinusitis, presenting with chronic sinus congestion and purulent discharge.
Physical Examination
Physical examination findings are often nonspecific. Patients with asthma commonly demonstrate wheezing or rhonchi, whereas those with cystic fibrosis may exhibit crackles related to bronchiectasis and mucus plugging. Tachypnea may occur during acute exacerbations or when secondary infection is present.
Evaluation
No single test confirms the diagnosis of ABPA. Clinicians establish the diagnosis by integrating clinical presentation, immunologic testing, and characteristic radiographic findings.[16] The International Society for Human and Animal Mycology (ISHAM)-ABAP working group recommends screening for ABPA annually in patients with asthma and cystic fibrosis, particularly if they are symptomatic with frequent exacerbations despite appropriate therapy. Evaluation for ABPA typically begins by confirming sensitization to A fumigatus through serum Aspergillus-specific IgE testing or skin testing. Intradermal skin tests are more sensitive than skin prick tests for detecting sensitization; however, many centers favor serum IgE assays because they offer greater standardization and reproducibility.[16] Skin testing demonstrates an immediate type I hypersensitivity reaction, indicating IgE-mediated sensitization to A fumigatus. A negative skin-prick test, followed by the absence of intradermal reactivity, makes ABPA unlikely.
If sensitization is confirmed, clinicians should measure total serum IgE and obtain a peripheral eosinophil count, as most patients demonstrate elevated levels of both markers. Although no single threshold definitively establishes the diagnosis, many experts use an IgE threshold of 500 IU/mL. Eosinophil counts are typically greater than 500/mm3, often exceeding 1000/mm3; however, systemic corticosteroids may lower IgE and eosinophil levels. Marked eosinophilia, greater than 2000/mm3, should prompt consideration of alternative diagnoses, such as eosinophilic granulomatosis with polyangiitis.[16][21]
Measurement of Aspergillus-specific IgG and serum precipitins provides supporting diagnostic evidence. Serum precipitins are IgG antibodies to Aspergillus antigens detected by gel diffusion. Serum precipitins and Aspergillus-specific IgG detected by immunoassay serve as markers of type III hypersensitivity and chronic Aspergillus exposure, helping to confirm sustained exposure to Aspergillus antigens.
Imaging
Chest radiography has limited sensitivity and may be normal in early disease. When abnormal, findings may include transient pulmonary infiltrates, mucus plugging, or features suggestive of bronchiectasis; however, chest x-ray lacks the sensitivity required for definitive evaluation. Classic radiographic signs of mucoid impaction include:
- “Finger-in-glove” opacities, representing impacted mucus within dilated bronchi
- Tram-track opacities, reflecting thickened bronchial walls
- Toothpaste shadows, caused by dense mucus filling the bronchi
- Ring shadows, representing cross-sectional views of dilated airways (see Images. Chronic Obstructive Pulmonary Disease and Allergic Bronchopulmonary Aspergillosis) [22]
High-resolution computed tomography is the imaging modality of choice for suspected ABPA because it more accurately detects bronchiectasis and airway abnormalities not visible on plain radiographs. Characteristic findings include central bronchiectasis, mucoid impaction, centrilobular nodules, and tree-in-bud opacities (see Images. Central Bronchiectasis and Mucoid Impaction and Central Bronchiectasis).
Pulmonary Function Tests
Pulmonary function tests help quantify functional impairment, monitor disease progression, and assess treatment response in patients with ABPA. Most patients exhibit an obstructive ventilatory defect reflecting underlying airway inflammation. As the disease advances, a mixed obstructive–restrictive pattern may develop due to bronchiectasis and fibrosis. Diffusing capacity is often preserved early in the disease course but may decline in advanced disease. Fixed airflow limitation can occur in patients with longstanding airway damage.
Bronchoscopy
Bronchoscopy is not routinely used to establish the diagnosis of ABPA. When performed, mucoid impaction is a characteristic feature of ABPA, and bronchial brushings may reveal mucus plugs containing aggregates of eosinophils, fungal hyphae, and eosinophil-derived Charcot–Leyden crystals. The presence of hyphae within mucus strongly supports the diagnosis. Bronchoalveolar lavage fluid typically demonstrates eosinophilia, particularly in steroid-naive patients, along with elevated Aspergillus-specific IgE and IgA produced in the airways.[18]
Clinicians should consider bronchoscopy if the diagnosis is uncertain, when sputum culture results are nondiagnostic, when they are unable to obtain a sputum sample, when the patient has unexplained hemoptysis, or when the patient has possible chronic infection, such as tuberculosis, before initiating systemic glucocorticoids.[16] Fungal sputum cultures are recommended by the ISHAM working group to help identify the causative organism and guide management. However, a positive culture alone does not establish the diagnosis.
Diagnostic Criteria
Although the Rosenberg-Patterson criteria historically defined ABPA, modern diagnostic approaches favor the revised ISHAM criteria, which incorporate advances in immunologic testing and imaging.
The International Society for Human and Animal Mycology proposed revised diagnostic criteria
Predisposing conditions
Clinicians should suspect ABPA in patients with underlying airway disease, most commonly bronchial asthma or cystic fibrosis. ABPA may also occur in individuals with bronchiectasis, COPD, or radiologic features consistent with these conditions, such as mucus plugging, finger-in-glove opacities, or transient pulmonary infiltrates.
Essential criteria
Both of the following are required:
- Evidence of A fumigatus sensitization, demonstrated by either elevated A fumigatus–specific IgE (≥0.35 kUA/L) or a positive immediate hypersensitivity skin test.
- Elevated total serum IgE, typically 500 IU/mL or higher, though lower values may be acceptable when other diagnostic features strongly support ABPA.
Additional criteria
At least 2 of the following should be present:
- Elevated A fumigatus–specific IgG antibodies (≥27 mgA/L) or positive serum precipitins
- Chest imaging consistent with ABPA, including central bronchiectasis, mucus plugging, high-attenuation mucus, or transient pulmonary opacities
- Peripheral blood eosinophilia (generally ≥500 cells/µL in patients who are steroid naive)
Rosenberg-Patterson Criteria
The Rosenberg-Patterson criteria consist of 8 major and 3 minor features. Although historically important, clinicians no longer recommend them for routine diagnosis.
Major criteria
- Asthma
- Transient pulmonary infiltrates
- Immediate cutaneous reactivity to A fumigatus
- Elevated total serum IgE
- Serum precipitating antibodies to A fumigatus
- Peripheral eosinophilia
- Elevated A fumigatus–specific IgE and IgG
- Central bronchiectasis
Minor criteria
- Expectoration of brown mucus plugs
- Positive sputum culture for Aspergillus species
- Late (Arthus-type) skin reactivity
Diagnostic Considerations in Cystic Fibrosis
Diagnosing ABPA in patients with cystic fibrosis can be challenging because many clinical and radiographic features overlap with baseline cystic fibrosis lung disease. The Cystic Fibrosis Foundation recommends maintaining a high index of suspicion in patients who develop otherwise unexplained clinical deterioration, including worsening cough, wheezing, increased sputum production, or declining pulmonary function.
Evaluation typically includes the following:
- Total serum IgE of 500 IU/mL or higher or a significant rise from the patient’s baseline level
- Evidence of Aspergillus sensitization, demonstrated by elevated Aspergillus-specific IgE, IgG antibodies, or positive serum precipitins
- New or changing radiographic abnormalities, such as pulmonary infiltrates, mucus plugging, or bronchiectasis
Because cystic fibrosis shares many pulmonary manifestations with ABPA, diagnosis relies heavily on immunologic findings and changes in the patient’s clinical status relative to baseline rather than isolated symptoms.
Treatment / Management
The primary aim of treatment in ABPA is to control acute inflammation, prevent recurrent exacerbations, and limit progressive lung injury, thereby preserving lung function. The ISHAM does not endorse treating patients with ABPA who are asymptomatic.
Corticosteroids
Systemic corticosteroids, most commonly prednisone or prednisolone, represent the first-line treatment for acute ABPA. Corticosteroids reduce airway inflammation, improve airflow obstruction, decrease serum total IgE levels, and lower peripheral eosinophil counts. Effective treatment promotes the resolution of pulmonary infiltrates and helps prevent progressive, irreversible lung damage.
Prednisolone is frequently used at an initial dose of 0.5 mg/kg daily for 2 weeks, followed by 0.5 mg/kg every other day for approximately 8 weeks. Clinicians then gradually taper the dose, typically by 5 mg every 2 weeks, with a total treatment duration of 3 to 5 months, depending on disease severity and response. Some patients require a daily maintenance dose of 5 to 7.5 mg to prevent relapse.
Clinicians typically reassess total serum IgE levels 6 to 8 weeks after initiating therapy and periodically during follow-up. A reduction of at least 35% from baseline indicates an adequate therapeutic response. Conversely, a 50% or greater increase from the post-treatment nadir, particularly when accompanied by clinical or radiographic worsening, indicates relapse and may require intensification of therapy. Inhaled corticosteroids may help control underlying asthma symptoms and reduce bronchospasm, but they do not replace systemic corticosteroids for the treatment of ABPA.[16](A1)
Oral Antifungal Agents
Antifungal therapy reduces the airway fungal burden and antigenic stimulus in ABPA, thereby decreasing exacerbations and serving as a steroid-sparing strategy. Itraconazole is commonly used in patients with recurrent exacerbations or glucocorticoid dependence, and clinicians should consider drug interactions, hepatotoxicity monitoring, and therapeutic drug monitoring when available. The dosing is as follows:
- Adults: 200 mg 3 times/d for 3 days, then twice daily with a meal for approximately 16 weeks
- Children: 5 mg/kg/d once a day or split twice daily if the dose exceeds 200 mg/d
Patients take the liquid itraconazole on an empty stomach, and those on the capsule form should avoid acid-blocking medications. Current guidelines recommend oral prednisolone or itraconazole monotherapy for acute ABPA, reserving combination therapy for patients with recurrent exacerbations. When itraconazole is ineffective or not tolerated, clinicians may use triazoles such as voriconazole (400 mg every 12 hours for 2 doses followed by a maintenance dose of 200 mg twice daily for 16 weeks) or posaconazole in selected patients; nebulized lipid amphotericin B (25 to 50 mg once or twice weekly) is an emerging option with limited evidence.
Routine monitoring of serum IgE levels is integral, as up to 35% of flares are asymptomatic.[23] A 100% rise in serum IgE indicates an exacerbation of ABPA. When present, a chest radiograph is necessary.[24] First-line treatment for a flare is a tapering dose of systemic glucocorticoids.
Clinicians consider a patient with ABPA in remission when serum IgE levels return to normal or are only mildly elevated, radiographic abnormalities resolve, and the patient has been off systemic glucocorticoids for 6 months. Patients continue inhaled corticosteroids for asthma treatment in accordance with the Global Initiative for Asthma guidelines. Clinicians monitor disease activity by measuring total serum IgE every 3 to 6 months. Rising levels may signal relapse and can coincide with new pulmonary opacities or peripheral eosinophilia. Experts recommend annual spirometry and repeated testing whenever symptoms change to assess lung function. Antifungal therapy is generally not used for routine prevention of exacerbations due to limited evidence of benefit and the potential for adverse effects.
Biologics
Omalizumab is a recombinant humanized monoclonal anti-IgE antibody that inhibits IgE binding to FcεRI receptors on mast cells and basophils, thereby reducing allergic inflammation.[25][26] Omalizumab is FDA-approved as an add-on therapy for moderate-to-severe allergic asthma that remains uncontrolled despite optimized inhaled corticosteroid–long-acting bronchodilator therapy. Although not specifically approved for ABPA, growing evidence supports its use as a steroid-sparing agent in patients with treatment-dependent or refractory disease, including those with asthma or cystic fibrosis.(A1)
Study results demonstrate improvements in symptoms, reductions in exacerbations, decreased need for oral corticosteroids, and improved pulmonary function. Clinicians determine omalizumab dosing based on baseline serum IgE levels and body weight, typically 75 to 375 mg administered subcutaneously every 2 to 4 weeks. Because many patients with ABPA have IgE levels exceeding the approved dosing range, clinicians often use the maximum recommended dose. Cost and insurance coverage may limit accessibility.
Emerging evidence supports the use of anti-IL-5 (mepolizumab and benralizumab) and anti-IL-4Rα (dupilumab) agents in refractory ABPA, particularly in steroid-dependent disease with marked eosinophilia or coexisting severe asthma.[27] These medications can improve lung function, reduce exacerbations, and aid in steroid-sparing in refractory ABPA. Additionally, inhaled agents, such as investigational antifungals (eg, opelconazole), may offer long-term treatment strategies with potentially lower systemic toxicity.(A1)
Antibiotics
Clinicians prescribe appropriate antibiotics to treat concurrent bacterial infections that may complicate ABPA, particularly in patients with underlying bronchiectasis or cystic fibrosis.
Supportive Measures
Clinicians often recommend airway clearance therapies for patients with ABPA complicated by bronchiectasis to improve mucus mobilization and reduce airway obstruction. Strategies may include nebulized hypertonic saline (typically preceded by a bronchodilator to minimize bronchospasm) and mechanical clearance techniques such as oscillatory positive expiratory pressure devices or high-frequency chest wall oscillation vests. Patients should minimize exposure to environments with high mold burden, including areas containing decomposing organic material, water-damaged buildings, or visible indoor mold. Although definitive evidence is limited, reducing fungal exposure may help decrease antigenic stimulation.
Differential Diagnosis
Clinicians must consider a variety of alternative diagnoses in the presence of peripheral eosinophilia and radiological abnormalities. The following list contains some of the potential differential diagnoses:
- Acute eosinophilic pneumonia
- Asthma with fungal sensitization
- Bronchiectasis unrelated to ABPA
- Bronchocentric granulomatosis
- Chronic eosinophilic pneumonia
- Chronic pulmonary aspergillosis
- Drug- or toxin-induced eosinophilic pneumonia
- Eosinophilic granulomatosis with polyangiitis
- Hypereosinophilic syndromes
- Löffler syndrome
- Mucoid impaction of the bronchi
- Parasitic infections, including tropical pulmonary eosinophilia, a clinical manifestation of lymphatic filariasis
- Pulmonary tuberculosis and nontuberculous mycobacterial infections [16]
Staging
The revised ISHAM-ABPA working group recommendations for clinical classification and treatment response criteria for ABPA and ABPM are as follows:
- Acute ABPA: Newly diagnosed ABPA or an exacerbation of ABPA marked by 14 days or more of clinical or radiologic worsening plus a 50% or greater increase in serum IgE. Clinicians should distinguish this from an asthma exacerbation, bronchiectasis, or infection. Experts define an asthma exacerbation as at least 48 hours of worsening symptoms without radiologic or immunologic evidence of worsening. Whereas patients with an infective or bronchiectasis exacerbation also present with 48 hours of worsening symptoms in addition to an increase in cough, breathlessness, sputum volume or consistency, sputum purulence, fatigue, malaise, fever, or hemoptysis, without immunological or radiological deterioration of ABPA/M.
- Response: The ISHAM defines a response as a 50% reduction in active symptoms and radiologic opacities, or a decline in serum total IgE of at least 20%, following 8 weeks of treatment.
- Remission: Patients exhibit 6 months or longer of both clinical and radiological improvement, are off glucocorticoids, and do not have a 50% or greater increase in serum IgE from the most recent measurement during clinical stability. The recommendations consider patients on long-term antifungal treatment who meet these criteria also in remission.
- Treatment-Dependent ABPA: Patients with 2 or more ABPA or ABPM exacerbations within 3 months of stopping glucocorticoids or worsening respiratory symptoms in combination with worse imaging or a rise in serum total IgE by 50% within 4 weeks of tapering oral steroids on 2 separate occasions.
- Advanced ABPA: Patients exhibit 10 or more segments of bronchiectasis due to ABPA on chest imaging and cor pulmonale or chronic type 2 respiratory failure.[16]
The ISHAM classifies ABPA based on high-resolution computed tomography findings as follows:
- Serological ABPA (ABPA-S): Fulfils the diagnostic criteria of ABPA with an absence of radiological findings of ABPA on HRCT
- ABPA with bronchiectasis (ABPA-B): Satisfies the diagnostic requirements of ABPA along with the presence of bronchiectasis
- ABPA with high attenuation mucus (ABPA-HAM): ABPA, along with the presence of high attenuation mucus on HRCT
- ABPA with mucus plugging (ABPA-MP): ABPA with mucus plugging but without high-attenuation mucus
- ABPA with chronic pleuropulmonary fibrosis (ABPA-CPF): Fulfils the diagnostic criteria of ABPA with at least 2 radiological features suggestive of fibrosis (including fibrocavitary lesions, pulmonary fibrosis, pleural thickening, fungal ball, and fibro-cavitary lesions) [16]
Prognosis
The natural history, progression, remission patterns, and recurrence rates of ABPA remain incompletely defined.[28] Patients without central bronchiectasis at diagnosis (serologic ABPA) generally preserve lung function over time, even with intermittent exacerbations. With appropriate treatment and monitoring, long-term disease control is achievable, and prolonged remissions are common.[16]
Treatment of acute ABPA with systemic corticosteroids typically results in reduced sputum production, improved control of bronchospasm, radiographic resolution of pulmonary infiltrates, and a 25% to 35% or greater decline in total serum IgE within 6 to 8 weeks. Serum IgE levels rarely normalize completely but usually fall to approximately 50% of the peak value observed during the acute episode.[19] Precipitating IgG antibodies may persist and are not reliable markers of treatment response.
Progression to irreversible bronchiectasis or pulmonary fibrosis may occur in patients with recurrent or treatment-dependent disease. Early diagnosis, appropriate therapy, and close follow-up may help limit long-term structural damage. Patients with severe fixed airflow limitation (persistently reduced forced expiratory volume in 1 second) or extensive bronchiectasis have a less favorable prognosis.[16]
Complications
Complications arise primarily from recurrent inflammation, mucus impaction, and progressive structural airway damage, rather than from invasive fungal infection.
Airway and Pulmonary Complications
- Recurrent asthma exacerbations
- Glucocorticoid dependence
- Progressive and irreversible central bronchiectasis
- Mucoid impaction
- Recurrent or chronic lobar atelectasis
- Fixed airflow limitation
- Progressive pulmonary fibrosis
- Chronic respiratory failure
- Pulmonary hypertension and cor pulmonale
- Recurrent pulmonary infections due to bronchiectasis
- Hemoptysis
- Air trapping and hyperinflation
- Bronchial wall thickening and airway remodeling
- Chronic pulmonary aspergillosis
- Aspergilloma
- Fibrocavitary lung disease [16][29]
Treatment-Related Adverse Effects
- Glucocorticoids: Hypertension, diabetes, glaucoma, osteoporosis, adrenal suppression, cataracts, mood changes, and increased infection risk
- Itraconazole and voriconazole: Hepatoxicity, worsening congestive heart failure, peripheral neuropathy, visual disturbances, photosensitivity, and QT prolongation [30]
- Omalizumab: Anaphylaxis and joint pain
Patients should undergo bone density monitoring in addition to monitoring of liver function, blood glucose, and blood pressure.
Postoperative and Rehabilitation Care
Indications for surgical intervention for ABPA are refractory disease, massive hemoptysis, aspergilloma, and chronic cavitary disease.[16][31][32] Surgery does not cure ABPA, as it is an immune-mediated disorder. Postoperative care emphasises respiratory monitoring, airway clearance, infection prevention, and continuation of medical therapy, with pulmonary rehabilitation providing supportive care. Patients should receive an annual influenza vaccine in addition to the pneumococcal vaccine per recommended guidelines.
Deterrence and Patient Education
ABPA is a chronic allergic lung condition caused by an exaggerated immune response to A fumigatus, a common environmental mold that colonizes the airways. This disease primarily affects patients with asthma or cystic fibrosis and can lead to recurrent inflammation, mucus plugging, bronchiectasis, and progressive lung damage if not appropriately managed. Healthcare professionals should educate patients that ABPA is not an infection that spreads from person to person but an allergic reaction due to colonization that requires long-term monitoring and, at times, prolonged therapy. Clear counseling about the purpose of systemic corticosteroids and antifungal agents is essential, particularly regarding adherence, expected benefits, and potential adverse effects. Patients should understand that symptom improvement may precede normalization of laboratory values, and rising total IgE levels may signal relapse before significant clinical deterioration.
Patients should promptly report worsening respiratory symptoms, including increased wheezing, shortness of breath, productive cough, brown mucus plugs, or hemoptysis. Clinicians should reinforce the importance of regular follow-up appointments, pulmonary function testing, and laboratory monitoring to help detect exacerbations early. Environmental counseling should focus on minimizing mold exposure when feasible, including avoiding damp indoor environments, compost, decaying vegetation, and poorly ventilated spaces. Encourage good home ventilation and mold remediation if needed. Optimizing control of underlying asthma or cystic fibrosis, maintaining airway clearance strategies, and promoting smoking cessation are critical preventive strategies that reduce exacerbations, preserve lung function, and improve long-term outcomes.
Enhancing Healthcare Team Outcomes
ABPA is a chronic, immune-mediated pulmonary disorder caused by hypersensitivity to A fumigatus colonizing the airways. This condition most commonly affects patients with asthma or cystic fibrosis and is characterized by recurrent wheezing, mucus plugging, elevated total and Aspergillus-specific IgE, eosinophilia, and central bronchiectasis on imaging. Rather than representing invasive infection, ABPA reflects exaggerated Th2-driven inflammation that can lead to progressive airway damage, fibrosis, and fixed airflow limitation if not recognized and treated early. Prompt diagnosis and appropriate use of systemic corticosteroids and antifungal therapy, along with monitoring of serum IgE, are critical to preventing irreversible lung injury.
Effective management of ABPA requires coordinated interprofessional collaboration. Physicians and advanced practitioners must accurately identify diagnostic criteria, differentiate ABPA from mimicking conditions, and implement evidence-based treatment strategies while monitoring for relapse. Nurses play a vital role in patient education, symptom monitoring, adherence reinforcement, and early identification of exacerbations.
Pharmacists contribute by reviewing medication regimens for drug–drug interactions (particularly azoles), counseling on adverse effects, and supporting steroid-sparing strategies. Respiratory therapists assist with pulmonary function testing and airway clearance techniques. Clear communication among team members ensures timely laboratory monitoring, imaging follow-up, and therapy adjustments. Coordinated care improves symptom control, reduces exacerbations and steroid dependence, enhances patient safety, and supports long-term preservation of lung function through patient-centered, team-based management.
Media
(Click Image to Enlarge)
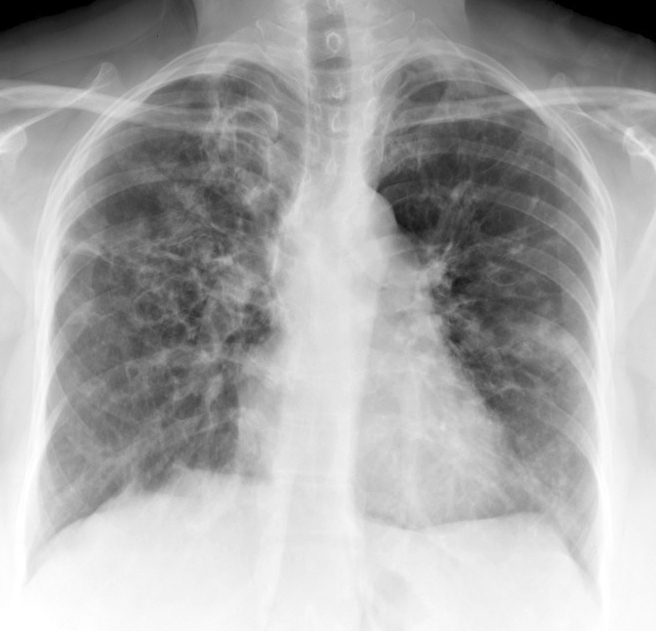
Chronic Obstructive Pulmonary Disease and Allergic Bronchopulmonary Aspergillosis. Posterior-anterior chest radiograph demonstrating bilateral central bronchiectasis with bronchial wall thickening and mucus plugging consistent with allergic bronchopulmonary aspergillosis.
Contributed by H Shulman, MD
(Click Image to Enlarge)

Central Bronchiectasis. CT scan of the chest reveals central bronchiectasis in a patient with COPD and allergic bronchopulmonary aspergillosis.
Contributed by H Shulman, MD
(Click Image to Enlarge)
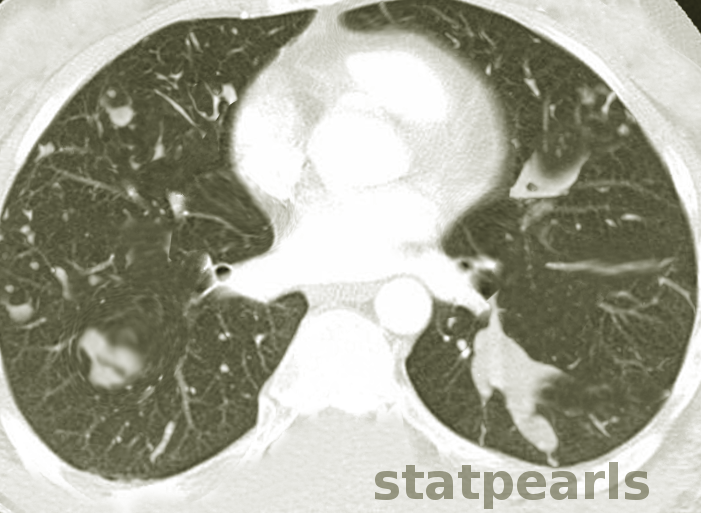
Central Bronchiectasis and Mucoid Impaction. Computed tomography of the chest reveals central bronchiectasis and mucoid impaction in a patient with allergic bronchopulmonary aspergillosis.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
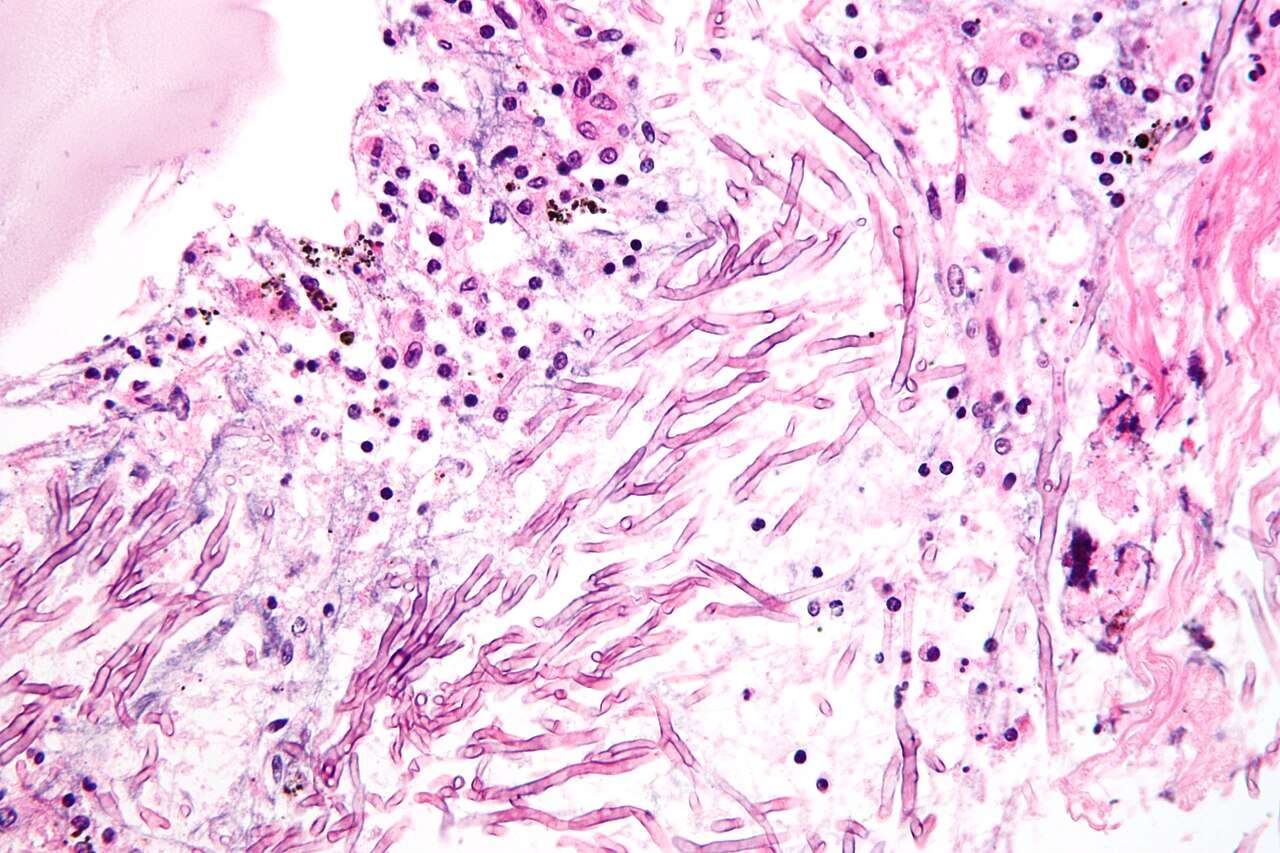
Aspergillus Hyphae. Hematoxylin and eosin stain showing uniform septate hyphae with acute-angle branching.
Nephron, Public Domain, via Wikimedia Commons
References
Ren J, Luo Y, Sun L, Chang C, Sun Y. Allergic bronchopulmonary aspergillosis in patients with chronic obstructive pulmonary disease: a case series and literature review. BMC pulmonary medicine. 2025 Dec 5:25(1):554. doi: 10.1186/s12890-025-04027-8. Epub 2025 Dec 5 [PubMed PMID: 41350669]
Level 2 (mid-level) evidencePatterson TF, Thompson GR 3rd, Denning DW, Fishman JA, Hadley S, Herbrecht R, Kontoyiannis DP, Marr KA, Morrison VA, Nguyen MH, Segal BH, Steinbach WJ, Stevens DA, Walsh TJ, Wingard JR, Young JA, Bennett JE. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2016 Aug 15:63(4):e1-e60. doi: 10.1093/cid/ciw326. Epub 2016 Jun 29 [PubMed PMID: 27365388]
Level 1 (high-level) evidenceAgarwal R, Chotirmall SH, Chalmers JD. Allergic bronchopulmonary aspergillosis and Aspergillus-related airway diseases in bronchiectasis: a narrative review. Journal of thoracic disease. 2025 Dec 31:17(12):11501-11519. doi: 10.21037/jtd-2025-1548. Epub 2025 Dec 26 [PubMed PMID: 41522133]
Level 3 (low-level) evidenceOguma T, Taniguchi M, Shimoda T, Kamei K, Matsuse H, Hebisawa A, Takayanagi N, Konno S, Fukunaga K, Harada K, Tanaka J, Tomomatsu K, Asano K. Allergic bronchopulmonary aspergillosis in Japan: A nationwide survey. Allergology international : official journal of the Japanese Society of Allergology. 2018 Jan:67(1):79-84. doi: 10.1016/j.alit.2017.04.011. Epub 2017 May 23 [PubMed PMID: 28546015]
Level 3 (low-level) evidenceAgarwal R, Muthu V, Sehgal IS, Dhooria S, Prasad KT, Soundappan K, Rudramurthy SM, Aggarwal AN, Chakrabarti A. Prevalence of Aspergillus Sensitization and Allergic Bronchopulmonary Aspergillosis in Adults With Bronchial Asthma: A Systematic Review of Global Data. The journal of allergy and clinical immunology. In practice. 2023 Jun:11(6):1734-1751.e3. doi: 10.1016/j.jaip.2023.04.009. Epub 2023 Apr 23 [PubMed PMID: 37088374]
Level 1 (high-level) evidenceChowdhary A, Agarwal K, Kathuria S, Gaur SN, Randhawa HS, Meis JF. Allergic bronchopulmonary mycosis due to fungi other than Aspergillus: a global overview. Critical reviews in microbiology. 2014 Feb:40(1):30-48. doi: 10.3109/1040841X.2012.754401. Epub 2013 Feb 5 [PubMed PMID: 23383677]
Level 3 (low-level) evidenceThompson GR 3rd, Young JH. Aspergillus Infections. The New England journal of medicine. 2021 Oct 14:385(16):1496-1509. doi: 10.1056/NEJMra2027424. Epub [PubMed PMID: 34644473]
Vitte J, Ranque S, Carsin A, Gomez C, Romain T, Cassagne C, Gouitaa M, Baravalle-Einaudi M, Bel NS, Reynaud-Gaubert M, Dubus JC, Mège JL, Gaudart J. Multivariate Analysis As a Support for Diagnostic Flowcharts in Allergic Bronchopulmonary Aspergillosis: A Proof-of-Concept Study. Frontiers in immunology. 2017:8():1019. doi: 10.3389/fimmu.2017.01019. Epub 2017 Aug 22 [PubMed PMID: 28878778]
Chatterjee P, Moss CT, Omar S, Dhillon E, Hernandez Borges CD, Tang AC, Stevens DA, Hsu JL. Allergic Bronchopulmonary Aspergillosis (ABPA) in the Era of Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) Modulators. Journal of fungi (Basel, Switzerland). 2024 Sep 18:10(9):. doi: 10.3390/jof10090656. Epub 2024 Sep 18 [PubMed PMID: 39330416]
Rafique A, Sharmin S, Raj A, Mohiuddin AL, Mahmud MIA, Bin Md Omer H. Comparative overview of Aspergillus fumigatus, A. flavus, and A. niger: Pathogenicity, resistance, and public health significance. Journal of infection and public health. 2026 Feb:19(2):103070. doi: 10.1016/j.jiph.2025.103070. Epub 2025 Dec 3 [PubMed PMID: 41353833]
Level 2 (mid-level) evidenceWang Y, Zhang L, Sun Y, Zhang Y. The Triad of Pathogenesis in Allergic Bronchopulmonary Aspergillosis: Interactions among {italic}Aspergillus fumigatus{/italic}, Epithelium, and Immunity. International archives of allergy and immunology. 2026:187(4):406-419. doi: 10.1159/000547550. Epub 2025 Jul 30 [PubMed PMID: 40738023]
Chauhan B, Santiago L, Kirschmann DA, Hauptfeld V, Knutsen AP, Hutcheson PS, Woulfe SL, Slavin RG, Schwartz HJ, Bellone CJ. The association of HLA-DR alleles and T cell activation with allergic bronchopulmonary aspergillosis. Journal of immunology (Baltimore, Md. : 1950). 1997 Oct 15:159(8):4072-6 [PubMed PMID: 9378997]
Agarwal R, Sehgal IS, Dhooria S, Muthu V, Prasad KT, Bal A, Aggarwal AN, Chakrabarti A. Allergic bronchopulmonary aspergillosis. The Indian journal of medical research. 2020 Jun:151(6):529-549. doi: 10.4103/ijmr.IJMR_1187_19. Epub [PubMed PMID: 32719226]
Denning DW, Pleuvry A, Cole DC. Global burden of allergic bronchopulmonary aspergillosis with asthma and its complication chronic pulmonary aspergillosis in adults. Medical mycology. 2013 May:51(4):361-70. doi: 10.3109/13693786.2012.738312. Epub 2012 Dec 4 [PubMed PMID: 23210682]
Maleki M, Mortezaee V, Hassanzad M, Mahdaviani SA, Poorabdollah M, Mehrian P, Behnampour N, Mirenayat MS, Abastabar M, Tavakoli M, Hedayati MT. Prevalence of allergic bronchopulmonary aspergillosis in cystic fibrosis patients using two different diagnostic criteria. European annals of allergy and clinical immunology. 2020 May:52(3):104-111. doi: 10.23822/EurAnnACI.1764-1489.121. Epub 2020 May 5 [PubMed PMID: 31702121]
Agarwal R, Sehgal IS, Muthu V, Denning DW, Chakrabarti A, Soundappan K, Garg M, Rudramurthy SM, Dhooria S, Armstrong-James D, Asano K, Gangneux JP, Chotirmall SH, Salzer HJF, Chalmers JD, Godet C, Joest M, Page I, Nair P, Arjun P, Dhar R, Jat KR, Joe G, Krishnaswamy UM, Mathew JL, Maturu VN, Mohan A, Nath A, Patel D, Savio J, Saxena P, Soman R, Thangakunam B, Baxter CG, Bongomin F, Calhoun WJ, Cornely OA, Douglass JA, Kosmidis C, Meis JF, Moss R, Pasqualotto AC, Seidel D, Sprute R, Prasad KT, Aggarwal AN. Revised ISHAM-ABPA working group clinical practice guidelines for diagnosing, classifying and treating allergic bronchopulmonary aspergillosis/mycoses. The European respiratory journal. 2024 Apr:63(4):. doi: 10.1183/13993003.00061-2024. Epub 2024 Apr 4 [PubMed PMID: 38423624]
Level 1 (high-level) evidenceGago S, Denning DW, Bowyer P. Pathophysiological aspects of Aspergillus colonization in disease. Medical mycology. 2019 Apr 1:57(Supplement_2):S219-S227. doi: 10.1093/mmy/myy076. Epub [PubMed PMID: 30239804]
Shah A, Panjabi C. Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity. Allergy, asthma & immunology research. 2016 Jul:8(4):282-97. doi: 10.4168/aair.2016.8.4.282. Epub [PubMed PMID: 27126721]
Stevens DA, Moss RB, Kurup VP, Knutsen AP, Greenberger P, Judson MA, Denning DW, Crameri R, Brody AS, Light M, Skov M, Maish W, Mastella G, Participants in the Cystic Fibrosis Foundation Consensus Conference. Allergic bronchopulmonary aspergillosis in cystic fibrosis--state of the art: Cystic Fibrosis Foundation Consensus Conference. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2003 Oct 1:37 Suppl 3():S225-64 [PubMed PMID: 12975753]
Level 3 (low-level) evidenceRoboubi A, Audousset C, Fréalle É, Brun AL, Laurent F, Vitte J, Mortuaire G, Lefevre G, Cadranel J, Chenivesse C. Allergic bronchopulmonary aspergillosis: A multidisciplinary review. Journal de mycologie medicale. 2023 Aug:33(3):101392. doi: 10.1016/j.mycmed.2023.101392. Epub 2023 May 4 [PubMed PMID: 37172543]
Baxter CG, Denning DW, Jones AM, Todd A, Moore CB, Richardson MD. Performance of two Aspergillus IgG EIA assays compared with the precipitin test in chronic and allergic aspergillosis. Clinical microbiology and infection : the official publication of the European Society of Clinical Microbiology and Infectious Diseases. 2013 Apr:19(4):E197-204. doi: 10.1111/1469-0691.12133. Epub 2013 Jan 18 [PubMed PMID: 23331929]
Milliron B, Henry TS, Veeraraghavan S, Little BP. Bronchiectasis: Mechanisms and Imaging Clues of Associated Common and Uncommon Diseases. Radiographics : a review publication of the Radiological Society of North America, Inc. 2015 Jul-Aug:35(4):1011-30. doi: 10.1148/rg.2015140214. Epub 2015 May 29 [PubMed PMID: 26024063]
Patterson R, Greenberger PA, Halwig JM, Liotta JL, Roberts M. Allergic bronchopulmonary aspergillosis. Natural history and classification of early disease by serologic and roentgenographic studies. Archives of internal medicine. 1986 May:146(5):916-8 [PubMed PMID: 3516103]
Greenberger PA. Allergic bronchopulmonary aspergillosis. The Journal of allergy and clinical immunology. 2002 Nov:110(5):685-92 [PubMed PMID: 12417875]
Nové-Josserand R, Grard S, Auzou L, Reix P, Murris-Espin M, Brémont F, Mammar B, Mely L, Hubert D, Durieu I, Burgel PR. Case series of omalizumab for allergic bronchopulmonary aspergillosis in cystic fibrosis patients. Pediatric pulmonology. 2017 Feb:52(2):190-197. doi: 10.1002/ppul.23612. Epub 2016 Oct 7 [PubMed PMID: 27717223]
Level 2 (mid-level) evidenceVoskamp AL, Gillman A, Symons K, Sandrini A, Rolland JM, O'Hehir RE, Douglass JA. Clinical efficacy and immunologic effects of omalizumab in allergic bronchopulmonary aspergillosis. The journal of allergy and clinical immunology. In practice. 2015 Mar-Apr:3(2):192-9. doi: 10.1016/j.jaip.2014.12.008. Epub 2015 Jan 29 [PubMed PMID: 25640470]
Level 1 (high-level) evidenceChen X, Zhi H, Wang X, Zhou Z, Luo H, Li J, Sehmi R, O'Byrne PM, Chen R. Efficacy of Biologics in Patients with Allergic Bronchopulmonary Aspergillosis: A Systematic Review and Meta-Analysis. Lung. 2024 Aug:202(4):367-383. doi: 10.1007/s00408-024-00717-y. Epub 2024 Jun 19 [PubMed PMID: 38898129]
Level 1 (high-level) evidenceVlahakis NE, Aksamit TR. Diagnosis and treatment of allergic bronchopulmonary aspergillosis. Mayo Clinic proceedings. 2001 Sep:76(9):930-8 [PubMed PMID: 11560305]
Agarwal R. Allergic bronchopulmonary aspergillosis. Chest. 2009 Mar:135(3):805-826. doi: 10.1378/chest.08-2586. Epub [PubMed PMID: 19265090]
Jaruratanasirikul S, Sriwiriyajan S. Effect of omeprazole on the pharmacokinetics of itraconazole. European journal of clinical pharmacology. 1998 Apr:54(2):159-61 [PubMed PMID: 9626921]
Denning DW, Cadranel J, Beigelman-Aubry C, Ader F, Chakrabarti A, Blot S, Ullmann AJ, Dimopoulos G, Lange C, European Society for Clinical Microbiology and Infectious Diseases and European Respiratory Society. Chronic pulmonary aspergillosis: rationale and clinical guidelines for diagnosis and management. The European respiratory journal. 2016 Jan:47(1):45-68. doi: 10.1183/13993003.00583-2015. Epub [PubMed PMID: 26699723]
Patel DC, Bhandari P, Epstein DJ, Liou DZ, Backhus LM, Berry MF, Shrager JB, Lui NS. Surgical resection for patients with pulmonary aspergillosis in the national inpatient sample. Journal of thoracic disease. 2021 Aug:13(8):4977-4987. doi: 10.21037/jtd-21-151. Epub [PubMed PMID: 34527336]