Introduction
In vitro fertilization (IVF) is a groundbreaking assisted reproductive technology (ART) that has revolutionized fertility treatment since its inception in the late 20th century. First successfully performed by Dr. Robert Edwards and Dr. Patrick Steptoe in 1978 with the birth of Louise Brown in the United Kingdom, the world's first "test-tube baby," IVF offered new hope to individuals and couples facing infertility.[1] IVF involves retrieving oocytes from the ovaries following ovarian stimulation and fertilization with sperm outside the body in a laboratory setting. The resulting embryos are cultured for several days and then transferred into the uterus, typically under ultrasound guidance, to achieve pregnancy.
Over the decades, IVF has evolved from an experimental procedure into a widely accepted and increasingly successful treatment, thanks to advancements in medical technology, laboratory techniques, and genetic screening. The International Committee for Monitoring Assisted Reproductive Technology (ICMART) has maintained the World IVF registry data since 1989. It estimates that around 10 million infants have been born from ART since its conception.[2] Today, IVF accounts for 2.6% of births in the United States and steadily grows each year.[CDC. ART Surveillance. 2024] IVF is indicated for a wide range of infertility etiologies, including tubal factors, severe male-factor infertility, endometriosis, ovulatory dysfunction, and unexplained infertility.[3] Its use has expanded beyond treating infertility to include preimplantation genetic testing for hereditary or chromosomal conditions, fertility preservation, and family building through donor gametes or gestational carriers. As the field continues to progress, IVF remains a cornerstone of reproductive medicine, continually expanding the possibilities of conception and parenthood.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy
Recognition of female pelvic anatomy (see Image. The Female Genital Organs) is paramount in properly understanding and completing IVF.[4] Mullerian anomalies and other structural defects within and outside of the uterus may impact initial implantation and ongoing pregnancy success.[5] Essential anatomical structures include:
- Ovaries: The site of oocyte (egg) production. Follicles are fluid-filled sacs within which oocytes develop. During each menstrual cycle, 1 follicle matures and releases a mature oocyte during ovulation. After the dominant follicle releases a mature oocyte, the ruptured follicle becomes the corpus luteum, which plays an essential role in implantation and early pregnancy. If fertilization does not occur, the corpus luteum degenerates, causing progesterone levels to drop and trigger menstruation. The ovaries are also the site of estrogen and progesterone production and secretion.
- Fallopian tubes: Natural site of fertilization in unassisted conception, bypassed in IVF.
- Uterus: Composed of 3 layers: the serosa, the myometrium, and the endometrium. The endometrium thickens to support embryo implantation.
- Cervix: The lower part of the uterus that serves as a canal between the uterus and the vagina. Embryo transfer catheters pass from the vagina through the cervix into the endometrial cavity during IVF.
- Vagina: The opening of the reproductive tract. Oocyte retrieval is performed through the vagina.
Physiology
Regulation of reproductive hormones is complex and multifaceted. The hypothalamic-pituitary-gonadal (HPG) axis is central in regulating reproductive hormones, which naturally fluctuate throughout the menstrual cycle.[6] In IVF, the HPG axis is manipulated through medication to allow precise control over follicular development, ovulation, and endometrial preparation for embryo transfer. Understanding the roles these following hormones play is critical in understanding the medications used in IVF:
- Follicle-stimulating hormone (FSH): Promotes follicle development in the ovaries
- Luteinizing hormone (LH): Mid-cycle LH surge triggers ovulation and leads to the release of a mature oocyte from the dominant follicle.
- Gonadotropin-releasing hormone (GnRH): Secreted by the hypothalamus in a pulsatile manner to stimulate the anterior pituitary to release FSH and LH.
- Human chorionic gonadotropin (hCG): Produced by the embryo after fertilization. Maintains the corpus luteum and progesterone production until the placenta takes over at approximately 8-10 weeks of gestation.
- Estradiol: Produced by developing follicles. Stimulates endometrial growth and triggers the LH surge.
- Progesterone: Prepares and supports the endometrium for implantation. Critical in maintaining early pregnancy.
Please see StatPearls' companion resources, "Physiology, Female Reproduction" and "Physiology, Menstrual Cycle" for more in-depth information.[7][8]
Indications
Infertility remains a persistent global reproductive health issue with significant impacts. From 1990 to 2021, its prevalence among individuals aged 15 to 49 has steadily increased worldwide, with projections indicating continued growth over the next several decades.[9] The American Society for Reproductive Medicine (ASRM) defines infertility as a disease, condition, or status characterized by the following:
- "In patients having regular, unprotected intercourse and without any known etiology for either partner suggestive of impaired reproductive ability, evaluation should be initiated at 12 months when the female partner is younger than 35 years of age and at 6 months when the female partner is 35 years of age or older.
- "The inability to achieve a successful pregnancy based on a patient’s medical, sexual, and reproductive history, age, physical findings, diagnostic testing, or any combination of those factors."
- "The need for medical intervention, including, but not limited to, the use of donor gametes or donor embryos to achieve a successful pregnancy either as an individual or with a partner."[10]
Around 12.7% of reproductive-age women seek infertility treatment annually in the United States, and around 85% of couples with infertility have an identifiable cause.[11] IVF is indicated for a wide range of infertility etiologies, including tubal factors, severe male-factor infertility, endometriosis, ovulatory dysfunction, and unexplained infertility.[3] IVF's use has expanded beyond treating infertility to include preimplantation genetic testing for hereditary or chromosomal conditions, fertility preservation, and family building through donor gametes or gestational carriers. ASRM recommends IVF as first-line therapy in women aged 38 years or older, in cases of severe male factor or bilateral tubal disease, and when preimplantation genetic testing is required.
Tubal Factor
Tubal infertility, accounting for 11% to 67% of infertility cases, is typically caused by blocked fallopian tubes or the inability of the fallopian tubes to obtain an oocyte from the ovary as a result of pelvic adhesive disease.[11] Pelvic inflammatory disease (PID) is the most common cause of tubal damage, usually as a result of Chlamydia trachomatis infections.[12][13] Bacterial infections can result in tubal occlusion or peritubular adhesions that render in vivo fertilization unlikely. Hysterosalpingograms, a technique in which radiopaque dye is injected into the uterine cavity and tracked through the fallopian tubes under fluoroscopy, are used to assess tubal patency. IVF bypasses the tubal damage by transferring embryos directly into the uterus.
Endometriosis
Endometriosis, a chronic inflammatory disease defined by the presence of endometrial tissue outside of the uterine cavity, is significantly more prevalent in women with infertility compared to those without.[14] The mechanisms of how endometriosis causes infertility are not yet fully understood, but research has shown that pelvic adhesions, chronic intraperitoneal inflammation, disturbed folliculogenesis, and decreased embryo implantation have all been described in women with endometriosis. Laparoscopic surgery has been found to increase the rate of pregnancy from 4.7% to 30.7%, indicating the importance of restoring normal pelvic anatomy for a spontaneous pregnancy. Unfortunately, women with endometriosis have a significantly lower success rate with IVF compared to other causes of infertility, with more advanced disease correlated to inferior outcomes.[15]
Male factor
Male factor infertility plays a role in 35% of cases of infertility.[11] Poor semen quality, including decreased sperm count, motility, or morphology (shape of the sperm), can be successfully treated medically or surgically in approximately 50% of men. Intrauterine insemination can also increase pregnancy rates in couples where the male partner has a low number of motile sperm. If such treatments fail, IVF with or without intracytoplasmic sperm injection (ICSI) can be utilized. In cases of azoospermia, obstructive or nonobstructive, or testicular hypofunction, treatment involves surgical sperm extraction from the testes or epididymis for immediate fertilization via ICSI or cryopreservation for use at a later time.[11]
Diminished Ovarian Reserve
With increasing age, we see a decline in fertility due to progressive loss of follicles and oocytes, as well as a decrease in oocyte quality.[11] IVF cannot overcome the impact of age on oocyte quantity and quality. However, women who are unable to get pregnant using their own oocytes due to diminished ovarian reserve are presented with the option to utilize donor oocytes or donor embryos. Premature ovarian insufficiency (POI) is defined as the loss of normal ovarian function before the age of 40, resulting in infertility.[16] IVF utilizing donor oocyte is the most effective treatment.
Ovulatory Dysfunction
Disorders of ovulation account for approximately 25% of cases of infertility according to the World Health Organization.[11] The most common source of anovulation is polycystic ovary syndrome (PCOS), accounting for 70% of cases of anovulation. Other causes include obesity, thyroid disease, pituitary disease, functional hypothalamic amenorrhea, adrenal hyperplasia/tumors, and idiopathic chronic anovulation.[11]
Fertility Preservation
IVF is also utilized in women who desire to preserve their fertility. Women with cancer or other illnesses may need to undergo gonadotoxic treatments that pose a threat to ovarian function. These women can cryopreserve either oocytes or embryos before chemotherapy or radiation, which can then be transferred at a future time. Oocyte cryopreservation is also a viable option for individuals who wish to delay childbearing. That women’s fertility dramatically decreases in the fourth decade of life has been established. This drop in fecundability results from decreased oocyte quantity and quality. Women who are not interested in pregnancy in the near future can cryopreserve oocytes or embryos for future use.[17]
Preimplantation Genetic Testing
For couples at risk of transmitting a known genetic disorder or women of advanced maternal age at higher risk for chromosomal abnormalities, IVF offers the opportunity for preimplantation genetic testing before embryo transfer to significantly reduce the risk of transferring embryos with specific genetic or chromosomal abnormalities.[18] Notably, genetic testing does not eliminate all risk.
Unexplained Infertility
For unexplained infertility, IVF is generally reserved for those who do not conceive after several cycles of ovulation induction with intrauterine insemination, or when expedited treatment is desired due to age or prognosis.[19]
Contraindications
Absolute contraindications to IVF are uncommon. However, IVF should not be performed in women who have a significant risk of morbidity and mortality of pregnancy if IVF were successful. The American Heart Association states that women with modified World Health Organization (WHO) class IV cardiovascular disease, including severe pulmonary hypertension, Eisenmenger syndrome, severe systemic ventricular dysfunction, or severe cyanotic heart disease, should not attempt pregnancy. Thus, IVF with embryo transfer is contraindicated in these cases.[20]
Other absolute contraindications include the presence of untreated gynecologic malignancy, active pelvic infection, or uncorrected uterine or pelvic anomalies that preclude embryo implantation or gestation. Relative contraindications include uncontrolled systemic disease, such as severe liver or renal dysfunction, poorly controlled diabetes, or hypertension, until adequately managed, as these conditions are associated with adverse pregnancy outcomes."[21] For women with these significant medical issues who desire a biological child, oocyte retrieval may still be considered for use with a gestational carrier if pregnancy is contraindicated, but gamete retrieval is not.
Personnel
IVF is a highly interprofessional medical procedure that requires the coordinated efforts of professionals across multiple specialties. Its success relies on a collaborative team working together to ensure each stage of the process is performed with precision and care. The ASRM recommends the following:
- A physician who has completed an American College of Graduate Medical Education-approved 3-year fellowship in reproductive endocrinology and infertility and is board-certified by the American Board of Obstetrics and Gynecology
- A nurse with training in reproductive medicine and clinical assisted reproductive technologies
- Physician or nurse trained in gynecological ultrasonography
- Embryology laboratory director (PhD or MD) with a high complexity laboratory director or embryology laboratory director certification
- Embryology laboratory personnel trained in gamete and embryo cryopreservation and micromanipulation techniques [22]
Preparation
Individuals planning for IVF undergo preconception evaluation and counseling before the start of the treatment cycle to optimize both IVF and pregnancy outcomes.[3] Comprehensive preconception evaluation supports appropriate patient selection and maximizes fertility success, while effective counseling promotes shared decision-making and helps set realistic expectations for treatment.[3] Recommended routine testing includes:
- Ovarian-reserve testing: Ovarian-reserve testing helps guide medication dosing for ovarian stimulation and set patient expectations for oocyte yield. This evaluation is especially important for individuals at risk of being "poor responders" and those at risk for cycle cancellation or ovarian hyperstimulation syndrome.[21] Ovarian reserve is evaluated using cycle day 3 FSH and estradiol (E2), anti-Mullerian hormone (AMH), or antral follicle count.[23]
- Ovulatory evaluation: In women with irregular cycles, amenorrhea, or clinical suspicion for ovulatory dysfunction, assessment is indicated. In the absence of regular menses or with abnormal results, targeted laboratory evaluation is warranted to identify underlying etiologies, eg, hyperprolactinemia, PCOS, hypothalamic amenorrhea, congenital adrenal hyperplasia, or POI.[23]
- Anatomy evaluation: Uterine cavity imaging identifies any anatomical issues, including endometrial polyps or fibroids, adhesions, or septa that may interfere with embryo implantation.[23] Fibroids and polyps that distort the uterine cavity are associated with reduced pregnancy and live birth rates. Similarly, Müllerian anomalies may contribute to recurrent IVF failure. Uterine anatomy evaluation may be performed via saline-infused sonogram or hysteroscopy before undergoing IVF in those patients with suspected abnormal anatomy.
- Semen analysis: Semen analysis is utilized to assess sperm morphology, concentration, and motility, and provide insight into whether the male factor is contributing to infertility.[3] Abnormal semen analysis can guide further evaluation and help identify treatable conditions, eg, infection or varicocele.
- Medical comorbidities: Before an IVF cycle, clinicians should conduct a thorough evaluation to ensure patients are in good medical standing.[24] Infectious disease screening for HIV, hepatitis B and C, and syphilis is recommended for both partners. Maternal-fetal medicine (MFM) specialists play a critical role in optimizing the management of chronic conditions and reducing risks in high-risk patients before IVF. They provide individualized counseling, coordinate care, and guide preconception interventions. National guidelines recommend MFM consultation before assisted reproductive technology to help minimize maternal and fetal morbidity and mortality.[25][26]
- Lifestyle Factors: Environmental factors play a significant role in fertility. Exercise, diet, obesity, tobacco use, illicit drug use, and exposure to occupational or environmental hazards have all been shown to play a significant negative role in reproductive outcomes, both assisted and unassisted.[21] Preconception counseling should address modifiable risk factors to improve pregnancy outcomes.
Technique or Treatment
Controlled Ovarian Stimulation
The IVF cycle begins with ovarian stimulation to induce the development of multiple ovarian follicles for retrieval. Multiple protocols have been utilized, ranging from no stimulation via a natural cycle to various levels of controlled ovarian stimulation using pharmacologic methods. Natural cycle IVF is not commonly performed because of the lower clinical pregnancy rate.[27] In IVF cycles, GnRH analogs are utilized to suppress premature ovulation, allowing for controlled egg maturation and retrieval during a treatment cycle. Several protocols are available:
- GnRH agonist protocols: Also termed "long luteal," GnRH agonists prevent the LH surge by downregulating GnRH receptors and suppressing LH and FSH. These protocols are typically longer-duration protocols and are associated with hypoestrogenic adverse effects.[28][29]
- GnRH antagonist protocols: GnRH antagonists provide more immediate inhibition of pituitary GnRH receptors, leading to quicker suppression of LH and FSH. This protocol is shorter, requires less gonadotropin, and is associated with significantly lower risk of ovarian hyperstimulation syndrome (OHSS).[28][29] ASRM recommends antagonist protocols to reduce the risk of OHSS.[30]
Both approaches are effective for LH surge suppression, but the choice is individualized based on patient characteristics and risk profile. Exogenous FSH is also administered to maintain supraphysiologic FSH concentrations throughout the follicular phase, promote the development of multiple follicles rather than a single dominant follicle, and avoid atresia.[31] Knowing that ovarian stimulation does not create new follicles but rather supports the developing follicles recruited for that cycle is important. Follicular growth is monitored by transvaginal ultrasonography, and blood levels of E2 help determine whether changes to the stimulation protocol are indicated. When at least 3 follicles reach 18 mm, the LH surge trigger shot is administered.
Minimal stimulation protocols utilize clomiphene citrate, a selective estrogen receptor modulator (SERM), or letrozole, an aromatase inhibitor, with or without gonadotropins. When gonadotropin stimulation is decreased or eliminated, the cost to the couple is reduced. The minimal stimulation protocol is gaining more support, as studies have found that, while the live birth rate is slightly lower than with the long GnRHa protocol (49% versus 63%), the rates of ovarian hyperstimulation syndrome and multiple pregnancies are significantly lower.[32][33]
Oocyte Retrieval
Regardless of the stimulation protocol, mature oocytes are retrieved 34 to 36 hours after administration of a trigger shot to stimulate the LH surge (typically either hCG or recombinant LH). Oocyte retrieval is performed using ultrasound-guided transvaginal aspiration and intravenous sedation. The ovaries are visualized using a vaginal ultrasound probe, and an attached needle guide helps the physician direct the needle into each follicle and aspirate the follicular fluid. The fluid is handed off to an embryologist in the lab to analyze it and collect any oocytes present.
Embryo Fertilization
Fertilization is achieved via conventional IVF, where oocytes and prepared sperm are co-incubated in culture media for 12 to 18 hours to allow natural sperm penetration, or by ICSI.[34] The semen sample is prepared by isolating sperm using density centrifugation or swim-up methods and washing it in media with a high protein concentration to promote capacitation, a process necessary for fertilization.[35] Male factor infertility may require ICSI, where 1 immobilized sperm is directly injected into a mature oocyte. This bypasses the need for the sperm to penetrate the zona pellucida, the glycoprotein matrix that surrounds the oocyte. Fertilization is confirmed typically 16 to 18 hours postinsemination by the presence of 2 pronuclei and extrusion of the second polar body.[36] The resulting embryos are further cultured for several days and reassessed for developmental quality. Embryos can undergo preimplantation genetic testing at this stage.
Embryo Transfer
Embryos can be transferred fresh into the uterus or cryopreserved for transfer at a later date. Fertilized embryos are transferred at the cleavage stage (3 days after fertilization) or the blastocyst stage (5 days after fertilization). The blastocyst-stage transfer offers higher live birth rates per cycle and is achieved with fewer embryos, resulting in lower multiple gestation rates.[37] However, the downside of blastocyst-stage transfer is that fewer embryos may be available for transfer due to the loss of embryos that did not survive in culture to day 5.
Embryos are transferred under transabdominal ultrasound guidance into the uterus by a catheter passing through the cervix.[38] The embryos are placed 1 to 2 cm from the uterine fundus. After the transfer, the catheter is checked under the microscope to ensure the embryo is not retained in the catheter and that all embryos were successfully placed in the uterus. The number of embryos transferred will depend on the embryo stage, embryo quality, maternal age, and patient preference. In the absence of a natural corpus luteum, progesterone supplementation is initiated to support implantation and early pregnancy development.
Complications
While IVF is a low-risk procedure, monitoring for complications and risks associated with the procedure, including ovarian hyperstimulation syndrome, ovarian torsion, intra-abdominal bleeding, infection, heterotopic pregnancy, and multiple gestation, is important.
Ovarian Hyperstimulation Syndrome
OHSS is the most serious, potentially life-threatening complication of ovarian stimulation and ovulation induction. It almost always occurs after stimulation with exogenous gonadotropins.[39] OHSS is driven by VEGF (vascular endothelial growth factor) released from hyperstimulated granulosa cells, leading to capillary leak, third spacing, ascites, and hemoconcentration.[40] In mild cases, women experience abdominal distension, nausea, and vomiting. In more severe cases, ascites develops with severe abdominal pain and possible pleural effusion, which may lead to decreased pulmonary function and hypoxia.
Patients may show signs of hypovolemia, oliguria, elevated creatinine, increased liver transaminases, leukocytosis, and electrolyte abnormalities. Hemoconcentration will increase the risk of thromboembolism. In critical cases, acute renal failure and disseminated intravascular coagulation may result in death. The WHO estimates the incidence of severe OHSS to be 0.2% to 1% of all stimulation cycles.[41] Reduced hCG doses and the use of recombinant LH (Lupron) are alternative ovulation triggers that are proposed to reduce the risk of OHSS.[39]
Ovarian Torsion
Ovarian torsion is an uncommon but serious complication of IVF, primarily due to ovarian enlargement from controlled ovarian hyperstimulation and the presence of multiple or large follicles or cysts.[42] Prompt recognition is critical so that surgical intervention can be performed to preserve ovarian function.
Heterotopic Pregnancy
Heterotopic pregnancy occurs when there is simultaneously an intra-uterine pregnancy and an extra-uterine pregnancy. These abnormal pregnancies are typically associated with multiple embryo transfer, tubal infertility, pelvic adhesions, and a history of ectopic pregnancy.[43]
Multiple Gestation
Multiple gestation has historically been a major consequence of ART; however, rates have declined significantly with the adoption of single embryo transfer to promote singleton gestation.[44] Current guidelines published by ASRM and the Society for Assisted Reproductive Technology (SART) recommend single embryo transfer for patients with a favorable prognosis (ie, younger than 35, more than 1 high-quality embryo available, first or second IVF cycle, previous successful IVF, or recipient of donor oocytes). As a result of these recommendations, twin gestations decreased from 23% in 2014 to 12.4% in 2017.[44] Multiple gestations can lead to an increased risk to both mother and fetus, including preterm birth and hypertensive disorders of pregnancy.
Interestingly, however, the rate of hypertensive disorders in IVF twin pregnancies compared to twins conceived naturally does not differ.[45][44][46] However, a significant difference in the rate of preterm birth between IVF twin versus naturally conceived twin pregnancies does not seem to be present, likely due to the higher risk of both hypertension and preterm birth in twin pregnancies in general.[47] One systematic review and meta-analysis found that clear differences emerge when comparing singleton pregnancies.
Additional Complications
Pandey et al found that singleton IVF pregnancies are associated with increased risk of hypertensive disorders of pregnancy, preterm delivery, as well as gestational diabetes, antepartum hemorrhage, congenital abnormalities, cesarean sections, low birth weight, small for gestational age, and perinatal mortality. However, Hayashi et al found that adverse obstetric outcomes in infertile patients were independent of treatment type, suggesting maternal factors, rather than ART methods, eg, IVF and ICSI, may underlie these risks.[48]
Clinical Significance
Infertility remains a growing public health concern, now estimated to affect 10% to 15% of couples in many developed nations and poses significant challenges for individuals of reproductive age worldwide.[21] Fortunately, advances in ARTs have expanded treatment possibilities, with IVF emerging as the most commonly used and effective option, offering the highest success rates for clinical pregnancy and live birth.[21] Since the first IVF birth in 1978, more than 5 million children have been conceived using this technology, underscoring its transformative impact.[37] As access to ART continues to grow, it offers meaningful hope to individuals and couples striving to overcome infertility and build their families.
Enhancing Healthcare Team Outcomes
IVF is a cornerstone of assisted reproductive technology used to manage infertility from tubal disease, male factor infertility, endometriosis, ovulatory dysfunction, and diminished ovarian reserve. The process involves controlled ovarian stimulation by manipulating the hypothalamic-pituitary-gonadal axis, oocyte retrieval, in vitro fertilization, and embryo transfer into a hormonally prepared uterus. Advances in embryo culture and preimplantation genetic testing have expanded its applications and improved outcomes. Careful evaluation of reproductive anatomy, hormonal function, and patient-specific risk factors is essential to guide therapy and minimize complications such as ovarian hyperstimulation syndrome, multiple gestation, and ectopic or heterotopic pregnancy.
Interprofessional collaboration is fundamental to optimizing IVF outcomes and patient-centered care. Physicians lead diagnosis and treatment planning, while primary care clinicians and advanced practitioners facilitate early recognition, initial evaluation, and timely referral. Nurses coordinate care, provide education, and monitor treatment response, while embryologists oversee fertilization and embryo development. Pharmacists ensure safe and effective medication management. All team members share responsibility for clear communication, emotional support, and shared decision-making to address the psychological stress associated with IVF, thereby improving adherence, reducing attrition, and enhancing overall safety, quality, and reproductive success.
Media
(Click Image to Enlarge)
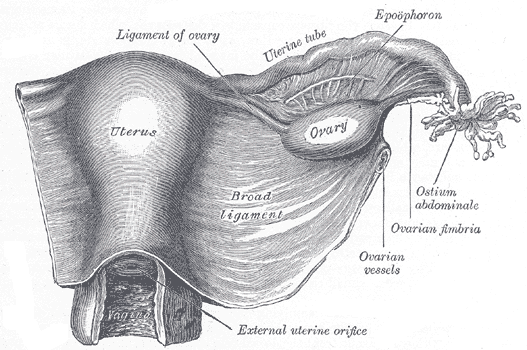
The Female Genital Organs. The uterus and right broad ligament are seen from behind, along with the uterine tube, ovary, epoophoron, and ovarian fimbria.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Zhao Y, Brezina P, Hsu CC, Garcia J, Brinsden PR, Wallach E. In vitro fertilization: four decades of reflections and promises. Biochimica et biophysica acta. 2011 Sep:1810(9):843-52. doi: 10.1016/j.bbagen.2011.05.001. Epub 2011 May 13 [PubMed PMID: 21605628]
Level 3 (low-level) evidenceAdamson GD, Creighton P, de Mouzon J, Zegers-Hochschild F, Dyer S, Chambers GM. How many infants have been born with the help of assisted reproductive technology? Fertility and sterility. 2025 Jul:124(1):40-50. doi: 10.1016/j.fertnstert.2025.02.009. Epub 2025 Feb 11 [PubMed PMID: 39947276]
Santoro N, Polotsky AJ. Infertility Evaluation and Treatment. The New England journal of medicine. 2025 Mar 13:392(11):1111-1119. doi: 10.1056/NEJMcp2311150. Epub [PubMed PMID: 40073310]
Harris-Glocker M, McLaren JF. Role of female pelvic anatomy in infertility. Clinical anatomy (New York, N.Y.). 2013 Jan:26(1):89-96. doi: 10.1002/ca.22188. Epub 2012 Nov 30 [PubMed PMID: 23197390]
de Ziegler D, Pirtea P, Galliano D, Cicinelli E, Meldrum D. Optimal uterine anatomy and physiology necessary for normal implantation and placentation. Fertility and sterility. 2016 Apr:105(4):844-54. doi: 10.1016/j.fertnstert.2016.02.023. Epub 2016 Feb 27 [PubMed PMID: 26926252]
Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Animal reproduction science. 2011 Apr:124(3-4):229-36. doi: 10.1016/j.anireprosci.2010.08.030. Epub 2010 Sep 3 [PubMed PMID: 20869180]
Level 3 (low-level) evidenceRosner J, Samardzic T, Sarao MS. Physiology, Female Reproduction. StatPearls. 2026 Jan:(): [PubMed PMID: 30725817]
Thiyagarajan DK, Basit H, Jeanmonod R. Physiology, Menstrual Cycle. StatPearls. 2026 Jan:(): [PubMed PMID: 29763196]
Liang Y, Huang J, Zhao Q, Mo H, Su Z, Feng S, Li S, Ruan X. Global, regional, and national prevalence and trends of infertility among individuals of reproductive age (15-49 years) from 1990 to 2021, with projections to 2040. Human reproduction (Oxford, England). 2025 Mar 1:40(3):529-544. doi: 10.1093/humrep/deae292. Epub [PubMed PMID: 39752330]
Practice Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org. Definitions of infertility and recurrent pregnancy loss: a committee opinion. Fertility and sterility. 2020 Mar:113(3):533-535. doi: 10.1016/j.fertnstert.2019.11.025. Epub 2020 Feb 27 [PubMed PMID: 32115183]
Level 3 (low-level) evidenceCarson SA, Kallen AN. Diagnosis and Management of Infertility: A Review. JAMA. 2021 Jul 6:326(1):65-76. doi: 10.1001/jama.2021.4788. Epub [PubMed PMID: 34228062]
Ahmad G, Watson A, Vandekerckhove P, Lilford R. Techniques for pelvic surgery in subfertility. The Cochrane database of systematic reviews. 2006 Apr 19:(2):CD000221 [PubMed PMID: 16625531]
Level 1 (high-level) evidenceAbrao MS, Muzii L, Marana R. Anatomical causes of female infertility and their management. International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 2013 Dec:123 Suppl 2():S18-24. doi: 10.1016/j.ijgo.2013.09.008. Epub 2013 Sep 11 [PubMed PMID: 24119894]
Meuleman C, Vandenabeele B, Fieuws S, Spiessens C, Timmerman D, D'Hooghe T. High prevalence of endometriosis in infertile women with normal ovulation and normospermic partners. Fertility and sterility. 2009 Jul:92(1):68-74. doi: 10.1016/j.fertnstert.2008.04.056. Epub 2008 Aug 5 [PubMed PMID: 18684448]
Level 2 (mid-level) evidenceMarcoux S, Maheux R, Bérubé S. Laparoscopic surgery in infertile women with minimal or mild endometriosis. Canadian Collaborative Group on Endometriosis. The New England journal of medicine. 1997 Jul 24:337(4):217-22 [PubMed PMID: 9227926]
Level 1 (high-level) evidenceStuenkel CA, Gompel A. Primary Ovarian Insufficiency. The New England journal of medicine. 2023 Jan 12:388(2):154-163. doi: 10.1056/NEJMcp2116488. Epub [PubMed PMID: 36630623]
O'Connor KA, Holman DJ, Wood JW. Declining fecundity and ovarian ageing in natural fertility populations. Maturitas. 1998 Oct 12:30(2):127-36 [PubMed PMID: 9871907]
. Preimplantation Genetic Testing: ACOG Committee Opinion, Number 799. Obstetrics and gynecology. 2020 Mar:135(3):e133-e137. doi: 10.1097/AOG.0000000000003714. Epub [PubMed PMID: 32080053]
Level 3 (low-level) evidencePractice Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org, Practice Committee of the American Society for Reproductive Medicine. Evidence-based treatments for couples with unexplained infertility: a guideline. Fertility and sterility. 2020 Feb:113(2):305-322. doi: 10.1016/j.fertnstert.2019.10.014. Epub [PubMed PMID: 32106976]
Mauricio R, Sharma G, Lewey J, Tompkins R, Plowden T, Rexrode K, Canobbio M, Skowronski J, Hameed A, Silversides C, Reynolds H, Vaught A, American Heart Association Cardiovascular Disease and Stroke in Women and Underrepresented Populations Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Council on Lifelong Congenital Heart Disease and Heart Health in the Young. Assessing and Addressing Cardiovascular and Obstetric Risks in Patients Undergoing Assisted Reproductive Technology: A Scientific Statement From the American Heart Association. Circulation. 2025 Feb 25:151(8):e661-e676. doi: 10.1161/CIR.0000000000001292. Epub 2025 Jan 15 [PubMed PMID: 39811953]
Howell EP, Harris BS, Kuller JA, Acharya KS. Preconception Evaluation Before In Vitro Fertilization. Obstetrical & gynecological survey. 2020 Jun:75(6):359-368. doi: 10.1097/OGX.0000000000000788. Epub [PubMed PMID: 32603474]
Level 2 (mid-level) evidencePractice Committee of the American Society for Reproductive Medicine, Practice Committee of the Society for Assisted Reproductive Technology, Practice Committee of the Society of Reproductive Biologists and Technologists. Electronic address: asrm@asrm.org. Minimum standards for practices offering assisted reproductive technologies: a committee opinion. Fertility and sterility. 2020 Mar:113(3):536-541. doi: 10.1016/j.fertnstert.2019.11.024. Epub 2020 Feb 25 [PubMed PMID: 32111480]
Level 3 (low-level) evidence. Infertility Workup for the Women's Health Specialist: ACOG Committee Opinion, Number 781. Obstetrics and gynecology. 2019 Jun:133(6):e377-e384. doi: 10.1097/AOG.0000000000003271. Epub [PubMed PMID: 31135764]
Level 3 (low-level) evidenceAmerican College of Obstetricians and Gynecologists’ Committee on Obstetric Practice, Committee on Genetics, U.S. Food and Drug Administration. Committee Opinion No 671: Perinatal Risks Associated With Assisted Reproductive Technology. Obstetrics and gynecology. 2016 Sep:128(3):e61-8. doi: 10.1097/AOG.0000000000001643. Epub [PubMed PMID: 27548556]
Level 3 (low-level) evidenceSociety for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org, Lappen JR, Pettker CM, Louis JM. Society for Maternal-Fetal Medicine Consult Series #54: Assessing the risk of maternal morbidity and mortality. American journal of obstetrics and gynecology. 2021 Apr:224(4):B2-B15. doi: 10.1016/j.ajog.2020.12.006. Epub 2020 Dec 9 [PubMed PMID: 33309560]
Society for Maternal-Fetal Medicine (SMFM). Electronic address: pubs@smfm.org, Kaimal A, Norton ME. Society for Maternal-Fetal Medicine Consult Series #55: Counseling women at increased risk of maternal morbidity and mortality. American journal of obstetrics and gynecology. 2021 Apr:224(4):B16-B23. doi: 10.1016/j.ajog.2020.12.007. Epub 2020 Dec 9 [PubMed PMID: 33309561]
Pelinck MJ, Vogel NE, Arts EG, Simons AH, Heineman MJ, Hoek A. Cumulative pregnancy rates after a maximum of nine cycles of modified natural cycle IVF and analysis of patient drop-out: a cohort study. Human reproduction (Oxford, England). 2007 Sep:22(9):2463-70 [PubMed PMID: 17586833]
Level 2 (mid-level) evidence. Gonadotrophin-releasing hormone antagonists for assisted reproductive technology. Obstetrics and gynecology. 2011 Sep:118(3):706-707. doi: 10.1097/AOG.0b013e31822bbbb2. Epub [PubMed PMID: 21860304]
Depalo R, Jayakrishan K, Garruti G, Totaro I, Panzarino M, Giorgino F, Selvaggi LE. GnRH agonist versus GnRH antagonist in in vitro fertilization and embryo transfer (IVF/ET). Reproductive biology and endocrinology : RB&E. 2012 Apr 13:10():26. doi: 10.1186/1477-7827-10-26. Epub 2012 Apr 13 [PubMed PMID: 22500852]
Practice Committee of the American Society for Reproductive Medicine. Electronic address: asrm@asrm.org. Prevention of moderate and severe ovarian hyperstimulation syndrome: a guideline. Fertility and sterility. 2024 Feb:121(2):230-245. doi: 10.1016/j.fertnstert.2023.11.013. Epub 2023 Dec 13 [PubMed PMID: 38099867]
Smacklon N, Fauser BC. Regulation of follicle development and novel approaches to ovarian stimulation for IVF. Human reproduction update. 2000 Jul-Aug:6(4):307-12 [PubMed PMID: 10972517]
Zhang JJ, Merhi Z, Yang M, Bodri D, Chavez-Badiola A, Repping S, van Wely M. Minimal stimulation IVF vs conventional IVF: a randomized controlled trial. American journal of obstetrics and gynecology. 2016 Jan:214(1):96.e1-8. doi: 10.1016/j.ajog.2015.08.009. Epub 2015 Aug 8 [PubMed PMID: 26259908]
Level 1 (high-level) evidenceShrestha D, La X, Feng HL. Comparison of different stimulation protocols used in in vitro fertilization: a review. Annals of translational medicine. 2015 Jun:3(10):137. doi: 10.3978/j.issn.2305-5839.2015.04.09. Epub [PubMed PMID: 26207230]
Bing Y, Ouellette RJ. Fertilization in vitro. Methods in molecular biology (Clifton, N.J.). 2009:550():251-66. doi: 10.1007/978-1-60327-009-0_16. Epub [PubMed PMID: 19495709]
Rao M, Tang L, Wang L, Chen M, Yan G, Zhao S. Cumulative live birth rates after IVF/ICSI cycles with sperm prepared by density gradient centrifugation vs. swim-up: a retrospective study using a propensity score-matching analysis. Reproductive biology and endocrinology : RB&E. 2022 Mar 31:20(1):60. doi: 10.1186/s12958-022-00933-2. Epub 2022 Mar 31 [PubMed PMID: 35361225]
Level 2 (mid-level) evidenceAnifandis G, Messini C, Dafopoulos K, Sotiriou S, Messinis I. Molecular and cellular mechanisms of sperm-oocyte interactions opinions relative to in vitro fertilization (IVF). International journal of molecular sciences. 2014 Jul 22:15(7):12972-97. doi: 10.3390/ijms150712972. Epub 2014 Jul 22 [PubMed PMID: 25054321]
Level 3 (low-level) evidenceGlujovsky D, Farquhar C, Quinteiro Retamar AM, Alvarez Sedo CR, Blake D. Cleavage stage versus blastocyst stage embryo transfer in assisted reproductive technology. The Cochrane database of systematic reviews. 2016 Jun 30:(6):CD002118. doi: 10.1002/14651858.CD002118.pub5. Epub 2016 Jun 30 [PubMed PMID: 27357126]
Level 1 (high-level) evidencePractice Committee of the American Society for Reproductive Medicine. Electronic address: ASRM@asrm.org, Practice Committee of the American Society for Reproductive Medicine. Performing the embryo transfer: a guideline. Fertility and sterility. 2017 Apr:107(4):882-896. doi: 10.1016/j.fertnstert.2017.01.025. Epub [PubMed PMID: 28366416]
Namavar Jahromi B MD, Parsanezhad ME MD, Shomali Z MD, Bakhshai P MD, Alborzi M MD, Moin Vaziri N MD PhD, Anvar Z PhD. Ovarian Hyperstimulation Syndrome: A Narrative Review of Its Pathophysiology, Risk Factors, Prevention, Classification, and Management. Iranian journal of medical sciences. 2018 May:43(3):248-260 [PubMed PMID: 29892142]
Level 3 (low-level) evidenceKumar P, Sait SF, Sharma A, Kumar M. Ovarian hyperstimulation syndrome. Journal of human reproductive sciences. 2011 May:4(2):70-5. doi: 10.4103/0974-1208.86080. Epub [PubMed PMID: 22065820]
Binder H, Dittrich R, Einhaus F, Krieg J, Müller A, Strauss R, Beckmann MW, Cupisti S. Update on ovarian hyperstimulation syndrome: Part 1--Incidence and pathogenesis. International journal of fertility and women's medicine. 2007 Jan-Feb:52(1):11-26 [PubMed PMID: 17987884]
Gorkemli H, Camus M, Clasen K. Adnexal torsion after gonadotrophin ovulation induction for IVF or ICSI and its conservative treatment. Archives of gynecology and obstetrics. 2002 Nov:267(1):4-6 [PubMed PMID: 12410364]
Liu M, Zhang X, Geng L, Xia M, Zhai J, Zhang W, Zhang Y, Sun Y, Zhang J, Zhu D, Zhao H, Chen ZJ. Risk Factors and Early Predictors for Heterotopic Pregnancy after In Vitro Fertilization. PloS one. 2015:10(10):e0139146. doi: 10.1371/journal.pone.0139146. Epub 2015 Oct 28 [PubMed PMID: 26510008]
Practice Committee of the American Society for Reproductive Medicine and the Practice Committee for the Society for Assisted Reproductive Technologies. Electronic address: ASRM@asrm.org. Guidance on the limits to the number of embryos to transfer: a committee opinion. Fertility and sterility. 2021 Sep:116(3):651-654. doi: 10.1016/j.fertnstert.2021.06.050. Epub 2021 Jul 28 [PubMed PMID: 34330423]
Level 3 (low-level) evidenceZhu L, Zhang Y, Liu Y, Zhang R, Wu Y, Huang Y, Liu F, Li M, Sun S, Xing L, Zhu Y, Chen Y, Xu L, Zhou L, Huang H, Zhang D. Maternal and Live-birth Outcomes of Pregnancies following Assisted Reproductive Technology: A Retrospective Cohort Study. Scientific reports. 2016 Oct 20:6():35141. doi: 10.1038/srep35141. Epub 2016 Oct 20 [PubMed PMID: 27762324]
Level 2 (mid-level) evidenceKawwass JF, Badell ML. Maternal and Fetal Risk Associated With Assisted Reproductive Technology. Obstetrics and gynecology. 2018 Sep:132(3):763-772. doi: 10.1097/AOG.0000000000002786. Epub [PubMed PMID: 30095760]
Marino JL, Moore VM, Willson KJ, Rumbold A, Whitrow MJ, Giles LC, Davies MJ. Perinatal outcomes by mode of assisted conception and sub-fertility in an Australian data linkage cohort. PloS one. 2014:9(1):e80398. doi: 10.1371/journal.pone.0080398. Epub 2014 Jan 8 [PubMed PMID: 24416127]
Hayashi M, Nakai A, Satoh S, Matsuda Y. Adverse obstetric and perinatal outcomes of singleton pregnancies may be related to maternal factors associated with infertility rather than the type of assisted reproductive technology procedure used. Fertility and sterility. 2012 Oct:98(4):922-8. doi: 10.1016/j.fertnstert.2012.05.049. Epub 2012 Jul 2 [PubMed PMID: 22763098]