Introduction
Cranial foramina are openings in the skull that allow the passage of neurovascular and lymphatic structures between the cranial cavity and the rest of the body. The skull is a critical osseous structure that protects the brain while accommodating these essential communication pathways. The morphology of the cranial foramina provides protected channels through which nerves, blood vessels, and lymphatic vessels traverse the skull.[1] See Image. Foramen Ovale. This topic reviews the major cranial foramina and the important neurovascular structures that pass through them. See Image. Skull Foramen.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The cranial foramina are best categorized by their anatomical positions on the floor of the cranial cavity. There are 3 distinct sections of the cranial fossae: anterior, middle, and posterior. Each of these regions contains a network of structures that are essential for day-to-day functioning.
Anterior fossa
The anterior fossa is composed of 3 specific bones: the frontal, ethmoid, and lesser wings of the sphenoid. Together, these bones comprise the shallowest recess of the cranium. Specifically, the cribriform plate of the ethmoid bone is porous in its structure and allows for the passage of olfactory axons of cranial nerve (CN) I through its many foramina into the nasal mucosa. These axons are responsible for the sense of smell. As scents are detected, information gets relayed from the olfactory axons into the olfactory bulb, where the sensory input is transferred along the olfactory tract to the entorhinal and piriform cortex of the brain.[2] Also, another foramen worth mentioning is the foramen cecum. It encompasses emissary veins that drain the nasal cavity of blood and reroute it to the superior sagittal vein. It is largely responsible for cerebral cooling due to its valveless architecture.[3]
Before focusing on the middle fossa, a transition area between the anterior and middle fossae known as the superior orbital fissure merits examination. While not defined as a strict foramen, its function is similar, and it is included when discussing the cranial foramina. Its shape differs in that it is more oblong and furrowed. A pair of superior orbital fissures are situated bilaterally between the lesser wing of the sphenoid bone superiorly and the greater wing of the sphenoid bone inferiorly, the fissure allows motor innervation to the ocular muscles, sensory innervation to lacrimal glands and portions of the face. Anatomically, the following structures are in order from superior to inferior:
- Lacrimal nerve
- Frontal nerve
- Superior ophthalmic vein
- Trochlear nerve (CN IV)
- Superior division of the oculomotor nerve (CN III)
- Nasociliary nerve
- Inferior division of the oculomotor nerve (CN III)
- Abducens nerve (CN VI)
- Branch of the inferior ophthalmic vein
Middle Fossa
Similar to the anterior fossa, the middle cranial fossa is also composed of 3 specific bones: the sphenoid and the paired temporal bones. It is home to neurovascular structures that supply sensory innervation to the face and vision, and blood to the cranium. The sphenoid bone houses the following structures through the various foramina:
- Optic canal: optic nerve (CN II) and ophthalmic artery
- Foramen rotundum: maxillary division of the trigeminal nerve (CN V)
- Foramen ovale: mandibular division of the trigeminal nerve (CN V) and lesser petrosal nerve
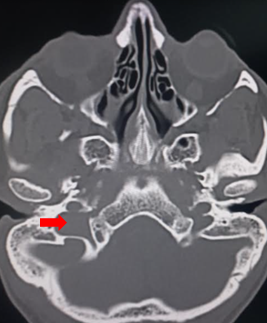
- Foramen lacerum: cartilage-containing space that allows passage for the greater petrosal nerve
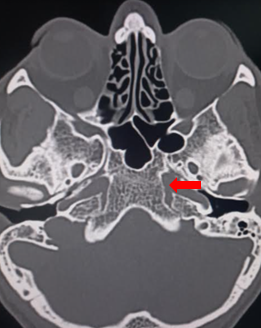
- Foramen spinosum: middle meningeal artery and vein, and the meningeal branch of CN V (see Image. Foramen Spinosum)
The temporal bone transmits the bilateral internal carotid arteries through their respective carotid canals before they form the middle cerebral arteries (MCAs). The MCAs then connect to form the circle of Willis, which supplies the brain with blood.
Posterior fossa
Like the anterior and middle fossae, the posterior cranial fossa also comprises 3 specific bones: the paired temporal bones and the occipital bone. It is the deepest of the fossae and is responsible for several passages that contain neurovascular bundles in each region of the fossa. The temporal portion of the posterior fossa contains the internal acoustic meatus-facial nerve (CN VII), vestibulocochlear nerve (CN VIII), vestibular ganglion, and labyrinthine artery.
The occipital portion of the posterior fossa contains the following neurovascular structures:
- Jugular foramen: divided into 3 portions (see Image. Jugular Foamen)
- Anterior-inferior petrosal sinus
- Middle-glossopharyngeal nerve (CN IX), vagus nerve (CN X), and the descending portion of the accessory nerve (CN XI)
- Posterior-sigmoid sinus at the junction of the internal jugular vein
- Hypoglossal canal: hypoglossal nerve (CN XII)
- Foramen magnum: the largest of the cranial foramina and contains the following structures:
- Medulla
- Paired vertebral arteries
- Paired anterior spinal arteries
- Paired posterior spinal arteries
- Ascending portion of CN XI
- Dural veins
Embryology
The cranium derives from both mesenchymal and neural crest cells.[4][5] In addition to its dual origin, ossification of the skull also occurs in a dualistic manner, with endochondral ossification and intramembranous ossification. Endochondral ossification is the bone-forming process that utilizes a cartilage template as its initial framework before ossification is complete.[6] The other ossification process, known as intramembranous ossification, occurs when dormant mesenchymal cells differentiate into osteoblasts.[7] Therefore, the classification of foramina can be based on the origin of the development or on the ossification process.[8]
Surgical Considerations
Instead of examining specific cases requiring neurosurgical intervention, this topic emphasizes the important concepts in surgical patient care. A neurosurgical consult, along with proper medical imaging, is the first crucial step in determining the specific pathology and whether surgical intervention is required. Furthermore, the physician must account for the risks and benefits of the procedure(s) and for patient autonomy. If surgical intervention is necessary and agreed upon, the exact procedure(s) may vary on a case-by-case basis depending on the severity of the pathology and the risks and benefits of the approach.
Clinical Significance
This section covers the most commonly encountered clinical issues that involve the cranial foramina.
Anterior cranial fossa
Trauma to the anterior cranial fossa, most specifically a fracture of the cribriform plate, can result in rhinorrhea, or a runny nose. This rhinorrhea is very important compared to the run-of-the-mill runny nose because after sustaining a fracture of the cribriform plate, the osseous fracture allows cerebrospinal fluid to extravasate into the nasal passages. The appearance of cerebrospinal fluid is normally clear; however, trauma can shear the vasculature, causing mixing. Filter paper may be used to detect the presence of cerebrospinal fluid. Blood moves less, and cerebrospinal fluid moves more, producing 2 concentric rings resembling a halo or target sign.[9] This finding is urgent and may also lead to more serious complications such as meningitis, cranial abscess, or anosmia due to the shearing of the olfactory axons within the bony framework of the cribriform plate.
Middle cranial fossa
Continuing with traumatic injury to the cranium, specifically damage to the middle meningeal artery, can result in epidural bleeds. The middle meningeal artery branches from the maxillary artery in the middle cranial fossa, with the assistance of the foramen spinosum, guiding its passage until it splits into its respective anterior and posterior divisions.[10] Non-contrast computed tomography is necessary to evaluate for epidural bleeds in the case of head trauma. A unique and distinctive condition known as crocodile tears syndrome affects the greater petrosal nerve within the foramen lacerum (see Image. Foramen Lacerum). Iatrogenic injury from surgery or conditions like Bell palsy can allow the nerve to incorrectly innervate the lacrimal gland instead of the submandibular gland during recovery. When exposed to gustatory or olfactory stimuli, unilateral tearing occurs on the side of injury instead of increased salivation.[11]
Posterior cranial fossa
The most commonly encountered anatomic irregularities of the posterior cranial fossa involve the brainstem and the inferior portion of the cerebellum. The German pathologist, Hans Chiari, described these brainstem and cerebellar malformations. He documented and named 2 specific anatomic variants: Chiari malformation types I and II. Chiari malformation type I results from an abnormally small or misshapen cranium during fetal development. As a result, the brain parenchyma, most notably the cerebellar tonsils, herniates through the foramen magnum. Chiari malformation type II also includes the herniation of the cerebellum as well as the medulla and fourth ventricle, and this is characteristically due to a smaller-than-average posterior fossa. In addition, type II is almost always associated with myelomeningocele.[12] The second clinical correlation of noteworthy importance is Vernet syndrome. Also known as jugular foramen syndrome, this disorder involves cranial nerve palsies of cranial nerves IX-XI. Occasionally, CN XII may be affected as well. These cranial nerve palsies are usually caused by direct compression from masses of the jugular foramen, such as acoustic neuromas, meningiomas, or glomus tumors.[13][14][15] Patients often complain of the following symptoms:
- Hoarseness
- Difficulty swallowing
- Partial or complete paralysis of neck muscles
- Decreased salivary output
- Sagging of the soft palate
- Partial or complete paralysis of the tongue muscles
Media
(Click Image to Enlarge)
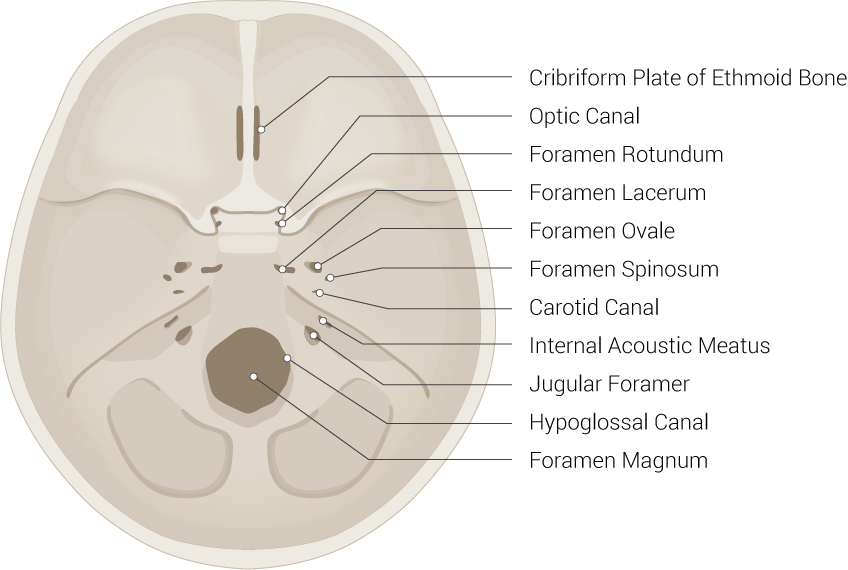
Skull Foramina. This illustration includes the cribriform plate of the ethmoid bone, optic canal, foramen rotundum, foramen lacerum, foramen ovale, foramen spinosum, carotid canal, internal acoustic meatus, jugular foramen, hypoglossal canal, and foramen magnum.
Illustrated by B Palmer
(Click Image to Enlarge)
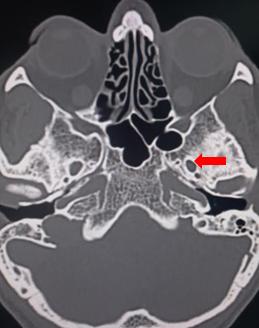
Foramen Ovale.
Contributed by S Munakomi, MD
(Click Image to Enlarge)

Foramen Spinosum.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
Foramen Lacerum.
Contributed by S Munakomi, MD
(Click Image to Enlarge)
Jugular Foramen.
Contributed by S Munakomi, MD
References
McGonnell IM, Akbareian SE. Like a hole in the head: Development, evolutionary implications and diseases of the cranial foramina. Seminars in cell & developmental biology. 2019 Jul:91():23-30. doi: 10.1016/j.semcdb.2018.08.011. Epub 2018 Oct 30 [PubMed PMID: 30385045]
Branigan B, Tadi P. Physiology, Olfactory. StatPearls. 2024 Jan:(): [PubMed PMID: 31194396]
Cabanac M, Brinnel H. Blood flow in the emissary veins of the human head during hyperthermia. European journal of applied physiology and occupational physiology. 1985:54(2):172-6 [PubMed PMID: 4043044]
Couly GF, Coltey PM, Le Douarin NM. The triple origin of skull in higher vertebrates: a study in quail-chick chimeras. Development (Cambridge, England). 1993 Feb:117(2):409-29 [PubMed PMID: 8330517]
Level 3 (low-level) evidenceNoden DM, Trainor PA. Relations and interactions between cranial mesoderm and neural crest populations. Journal of anatomy. 2005 Nov:207(5):575-601 [PubMed PMID: 16313393]
Level 3 (low-level) evidenceMackie EJ, Ahmed YA, Tatarczuch L, Chen KS, Mirams M. Endochondral ossification: how cartilage is converted into bone in the developing skeleton. The international journal of biochemistry & cell biology. 2008:40(1):46-62 [PubMed PMID: 17659995]
Eames BF, Helms JA. Conserved molecular program regulating cranial and appendicular skeletogenesis. Developmental dynamics : an official publication of the American Association of Anatomists. 2004 Sep:231(1):4-13 [PubMed PMID: 15305282]
Level 3 (low-level) evidenceAkbareian SE, Pitsillides AA, Macharia RG, McGonnell IM. Occipital foramina development involves localised regulation of mesenchyme proliferation and is independent of apoptosis. Journal of anatomy. 2015 Jun:226(6):560-74. doi: 10.1111/joa.12304. Epub [PubMed PMID: 25994127]
Sunder R, Tyler K. Basal skull fracture and the halo sign. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2013 Mar 19:185(5):416. doi: 10.1503/cmaj.120055. Epub 2012 Aug 13 [PubMed PMID: 22891200]
Level 3 (low-level) evidenceKhairat A, Waseem M. Epidural Hematoma. StatPearls. 2024 Jan:(): [PubMed PMID: 30085524]
Modi P, Arsiwalla T. Crocodile Tears Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 30247828]
Hidalgo JA, Tork CA, Varacallo M. Arnold Chiari Malformation. StatPearls. 2023 Jan:(): [PubMed PMID: 28613730]
AlShareef S, Newton BW. Accessory Nerve Injury. StatPearls. 2024 Jan:(): [PubMed PMID: 30335278]
Thomas K, Minutello K, Das JM. Neuroanatomy, Cranial Nerve 9 (Glossopharyngeal). StatPearls. 2026 Jan:(): [PubMed PMID: 30969699]
Das JM, Al Khalili Y. Jugular Foramen Syndrome. StatPearls. 2024 Jan:(): [PubMed PMID: 31751061]