 Catheter Management of Atrial Septal Defect
Catheter Management of Atrial Septal Defect
Introduction
Atrial septal defect (ASD) is one of the most common congenital heart defects, with an estimated incidence of 6 to 10 per 10,000 live births.[1] ASDs are classified as primum, secundum, sinus venosus, and coronary sinus defects. The onset of symptoms varies among different patients, and many remain asymptomatic. Larger defects tend to cause symptoms early in life, while smaller defects often cause symptoms later in life. Symptoms include failure to thrive, shortness of breath, palpitations, enlargement of right heart chambers, peripheral edema, cyanosis, orthodeoxia-platypnea, and paradoxical embolism. Transcatheter closure of the ASD is currently available for secundum ASDs (see Image. Atrial Septal Defect Closure). Currently, 3 United States (US) Food and Drug Administration (FDA)-approved devices for ASD closure: the Amplatzer Septal Occluder, Amplatzer Cribriform, and Gore Cardioform Septal Occluder.
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The heart consists of 4 chambers—2 atria and 2 ventricles. The interatrial septum divides the right and left atria and begins forming during the fifth week of gestation. An ASD arises from the incomplete formation of this septum, leading to abnormal communication between the atria. Embryologically, the septum develops from 2 overlapping components: the septum primum and septum secundum. The septum primum originates from the atrial roof and grows toward the endocardial cushions to close the ostium primum. Resorption of the upper portion of the septum primum creates the ostium secundum, which is later overlapped by the septum secundum growing caudally on the right atrial side to complete septation.[2][3]
ASDs are classified anatomically into 4 types: primum, secundum, sinus venosus, and coronary sinus. The secundum ASD, located at the fossa ovalis, is the most common. Primum ASDs involve the endocardial cushions and often coexist with atrioventricular valve abnormalities. Sinus venosus defects occur near the junction of the superior or inferior vena cava with the right atrium, termed superior or inferior types; superior defects often coexist with anomalous pulmonary venous connections. Coronary sinus defects arise from the partial or complete absence of the coronary sinus roof, permitting communication between the left atrium and the coronary sinus.[4] A patent foramen ovale (PFO) represents a subtype of ostium secundum defect, resulting from incomplete fusion of the septum primum and secundum after birth.
Understanding adjacent cardiac structures is crucial for catheter-based ASD closure. The interatrial septum is a thin, pliable region bordered by the aortic root anteriorly, the superior vena cava (SVC) superiorly, and the inferior vena cava (IVC) inferiorly. The fossa ovalis serves as the principal target site for transcatheter closure devices. The pulmonary veins enter the left atrium posteriorly, and their proximity must be considered to avoid device impingement. The Eustachian valve, the Thebesian valve, and the coronary sinus ostium can influence catheter navigation. Transesophageal echocardiography (TEE) or intracardiac echocardiography helps visualize septal anatomy, defect size, and surrounding tissue rims necessary for stable device anchoring. An adequate septal rim (>5 mm) from vital structures, such as the aortic root, SVC, and pulmonary veins, is essential to ensure proper device positioning and prevent erosion or embolization.
Based on size, ASDs are classified as trivial (<3 mm), small (3–<6 mm), moderate (6–8 mm), or large (>8 mm).[5] The physiologic consequence of an untreated ASD is left-to-right shunting, which increases right atrial and right ventricular volumes, elevates pulmonary blood flow, and can lead to pulmonary hypertension and right-sided heart failure if not corrected. Understanding this pathophysiologic mechanism is fundamental for timing intervention and optimizing patient outcomes in both surgical and catheter-based ASD management.
Indications
Transcatheter closure of the ASD can be performed only for the secundum type of ASDs. The other ASD types are repaired surgically because of their location and associated abnormalities of atrioventricular valve defects (primum type) and anomalous pulmonary vein connections (sinus venosus type). Current indications for ASD closure by a transcatheter approach include:
- Symptomatic ASD causing functional impairment (class I)
- Symptomatic (class I) or asymptomatic right atrial and or right ventricular enlargement (class II)
- Symptomatic (class I) or asymptomatic hemodynamically significant defect without symptoms, with a ratio of pulmonary to systemic flow greater than 1.5 (class II)
- Paradoxical embolism [6][7][8]
Contraindications
Contraindications for ASD closure by a transcatheter approach include:
- ASDs other than those of the secundum type, including primum type, sinus venosus type, and coronary sinus defects
- Severe pulmonary hypertension (pulmonary systolic pressure or pulmonary vascular resistance greater than two-thirds of systemic pressure or systemic vascular resistance) [9]
- Eisenmenger syndrome or net right-to-left shunt
- Defects larger than 38 mm in diameter [3]
- Absent or insufficient rim of tissue around the defect [6][8]
Equipment
Catheter-based ASD closure should be performed in a dedicated cardiac catheterization laboratory or hybrid operating room equipped with high-quality biplane fluoroscopy and real-time echocardiographic imaging capabilities, including TEE or ICE.[10] Essential equipment includes hemodynamic monitoring systems, catheterization trays, sheaths and guidewires, occlusion devices such as the Amplatzer Septal Occluder, and retrieval tools in case of device malposition or complications. Resuscitation and surgical backup equipment, including cardiopulmonary bypass capability, must be available on-site to manage rare but potentially life-threatening complications. Access to sterile interventional supplies, ultrasound-guided vascular access systems, and postprocedure recovery units further enhances safety and efficiency. Comprehensive facility preparedness and a trained multidisciplinary team ensure the highest standard of care for patients undergoing transcatheter ASD closure.
Types of ASD closure devices include:
- Amplatzer Septal Occluder
- This device, approved by the FDA in 2001, is the most commonly used for transcatheter closure. This double-disc occluder is constructed from a self-expanding nitinol mesh lined with polyester fabric, which promotes occlusion and tissue ingrowth. The device's central waist anchors within the defect, centering the device and ensuring complete closure of the interatrial communication. The design enables controlled deployment, retrievability before release, and long-term stability following endothelialization.
- Amplatzer Cribriform Occluder
- Developed by Abbott Laboratories, it is designed to close multifenestrated ASDs and is indicated for cribriform ASDs in patients with signs of right ventricular overload. This device features large, equal-sized right and left discs connected by a narrow central waist.
- Gore Helex and Gore Cardioform Septal Occluder
- These devices are used to close ASDs and PFOs up to 17 mm. The occluder comprises 5 platinum-filled nickel-titanium (nitinol) wire frames covered with expanded polytetrafluoroethylene (ePTFE). This device consists of 2 discs, each with 5 petals.
- Several devices have received Conformité Européene marking in Europe but have not been approved by the FDA for use in the US. These include:
- BioSTAR (BioSTAR, Inc., Maple Grove, MN)
- CardioSEAL (NMT Medical, Boston, MA)
- Solysafe Septal Occluder (Solitaire, Inc, Minneapolis, MN)
- Modified Rashkind PDA umbrella
- ATRIASEPT I-ASD (ATRIASEPT, Inc, Houston, TX)
- ATRIASEPT II-ASD (ATRIASEPT, Inc, Houston, TX)
- ULTRASEPT (Ultrasept Medical, Inc, Los Angeles, CA)
- Sideris’ wireless devices (Sideris Medical, Inc, Miami, FL)
- PFM ASD-R device (PFM Medical, Inc, Cologne, Germany)
Personnel
Successful transcatheter closure of an ASD requires a skilled, multidisciplinary team to ensure procedural precision, patient safety, and optimal outcomes. The interventional cardiologist is the primary operator, performing catheter navigation, defect measurement, and device deployment under fluoroscopic and echocardiographic guidance. A second interventionalist or structural heart specialist often assists with guidewire manipulation, sheath management, and device delivery, particularly in complex or large defects.
An echocardiographer, typically a cardiologist or anesthesiologist with expertise in TEE/ICE, is crucial in defining septal anatomy, measuring defect size, confirming adequate septal rims, and guiding device placement in real time. The cardiac anesthesiologist ensures hemodynamic stability, manages sedation or general anesthesia, and coordinates with the procedural team during critical moments such as device deployment or retrieval. Cardiac catheterization laboratory nurses and technologists are crucial for patient preparation, maintaining a sterile field, monitoring vital signs, operating imaging equipment, and documenting procedural parameters.
A perfusionist or cardiothoracic surgical team should be immediately available as a safety measure in case of complications requiring emergent surgical intervention, such as device embolization, perforation, or erosion. Postprocedure, nurses, pharmacists, and advanced practitioners coordinate recovery care, monitor for arrhythmias, bleeding, or thromboembolic events, and ensure appropriate antiplatelet therapy and follow-up imaging. Effective communication and coordination among all members of this interprofessional team are vital for optimizing patient-centered outcomes and ensuring procedural safety in ASD device closure.
Preparation
Preprocedure Evaluation
A comprehensive preprocedure evaluation is essential to ensure patient safety and procedural success in transcatheter ASD closure. The assessment begins with a detailed clinical history and physical examination, emphasizing any history of metal hypersensitivity—particularly to nickel, as many occluder devices (eg, Amplatzer) contain nitinol. A review of anticoagulation status, prior cardiac interventions, arrhythmia history, and comorbid conditions such as pulmonary hypertension or right heart failure is also critical.
TEE remains the gold standard for defining ASD anatomy. This imaging study enables the evaluation of defect type (ostium secundum vs other variants), size, and margins (rims) to determine the suitability for device closure. Adequate rim tissue—especially around the aortic and superior vena cava borders—is essential for device stability. Three-dimensional (3D) TEE provides enhanced visualization and facilitates accurate device sizing. ICE may be an alternative imaging modality, particularly in adult patients or when TEE is contraindicated.
Right heart catheterization is performed to assess pulmonary artery pressures, pulmonary vascular resistance, and the shunt ratio (Qp/Qs). This helps determine the hemodynamic significance and confirms the absence of irreversible pulmonary hypertension. A Qp/Qs ratio greater than 1.5:1 with evidence of right heart enlargement typically supports closure. In cases where TEE findings are inconclusive or complex anatomy is suspected, cardiac magnetic resonance imaging (MRI) or computed tomography angiography (CTA) can provide a detailed 3D assessment of the interatrial septum and exclude partial anomalous pulmonary venous return (PAPVR) or other structural anomalies that may alter management.
Before the procedure, the patient should receive comprehensive counseling regarding the risks, benefits, alternatives, and long-term outcomes of device closure. Informed consent must be obtained, and any questions or concerns addressed. On the day of the procedure, the patient should be evaluated for active infections, uncontrolled arrhythmias, or decompensated heart failure, which may warrant postponement. Preanesthetic evaluation should include airway assessment and optimization of comorbid conditions. Baseline laboratory studies (complete blood count, coagulation profile, metabolic panel/renal function) and a 12-lead electrocardiogram should be reviewed to ensure procedural readiness.
Antibiotic Prophylaxis
Antibiotic prophylaxis prevents infective endocarditis and other procedure-related infections during and after catheter-based ASD closure.[11] Although the overall risk of endocarditis following transcatheter closure is low, a prosthetic device temporarily increases susceptibility to bacterial colonization until complete endothelialization occurs. Current recommendations from the American Heart Association (AHA) and the European Society of Cardiology (ESC) support the administration of a single preprocedural antibiotic dose, typically a first-generation cephalosporin such as cefazolin (1–2 g intravenously [IV]) within 30 to 60 minutes before vascular access is established. Alternatives for patients with a β-lactam allergy include vancomycin (15 mg/kg IV) or clindamycin (600 mg IV). This prophylaxis primarily targets skin flora, including Staphylococcus aureus and Staphylococcus epidermidis, the most common pathogens implicated in device-related infections.
Routine postoperative antibiotic therapy is not indicated once the device has been placed successfully and no signs of infection are present. However, patients are advised to maintain infective endocarditis prophylaxis (typically with amoxicillin 2 g orally 30 to 60 minutes before procedures) for at least 6 months after closure or until imaging confirms complete endothelialization of the device. This is particularly important for patients undergoing dental procedures, upper respiratory tract interventions, or invasive genitourinary or gastrointestinal procedures during the early post-implantation period.
Strict adherence to aseptic technique during vascular access, device handling, and sheath manipulation is equally crucial in preventing catheter-related infections. Postprocedure monitoring for fever, bacteremia, or local infection at the access site should be routinely performed. Combining evidence-based antibiotic prophylaxis and meticulous sterile technique minimizes infectious complications following transcatheter ASD closure.
Technique or Treatment
Intraoperative Management and Device Deployment
Transcatheter ASD closure is typically performed in a cardiac catheterization laboratory or hybrid suite under moderate sedation or general anesthesia, depending on the complexity of the defect and the need for continuous TEE guidance. Most ASDs can be safely closed under moderate sedation; however, general anesthesia is often preferred in pediatric cases or when precise TEE imaging is required.[12] Before vascular access, a single preoperative dose of intravenous antibiotics is administered to minimize the risk of infection associated with the procedure.[13]
The patient is prepped and draped in sterile fashion, and femoral venous access is obtained under ultrasound guidance. Access is typically through the right femoral vein, though bilateral femoral venous access may be used, mainly when intracardiac echocardiography (ICE) is employed. A single venous access is usually sufficient when TEE is used for imaging. ICE requires an 8 to 10 French sheath (25–35 cm in length) for catheter stability, while the second access begins with a 6 French sheath, which is then upgraded to 6 to 12 French depending on the device size. Larger sheaths are needed for larger occluders. Some operators also obtain femoral arterial access for continuous pressure monitoring and angiographic reference.[12]
Once access is secured, systemic anticoagulation with unfractionated heparin is initiated to maintain an activated clotting time (ACT) of greater than 250 seconds throughout the procedure. Bivalirudin may be an alternative in patients with heparin-induced thrombocytopenia or allergy. Under fluoroscopic and echocardiographic guidance, the ICE catheter is advanced into the right atrium to visualize the interatrial septum and assess the adequacy of the rim. The ASD size is measured in multiple planes, and color Doppler imaging is used to characterize shunt direction and magnitude.[13]
Under combined fluoroscopic and ICE visualization, an angled-tip catheter over a J-tip guidewire is advanced from the right atrium across the defect into the left atrium. The wire is subsequently directed into the left superior pulmonary vein for support and exchanged for a super-stiff guidewire. The delivery sheath is advanced over this wire into the left atrium. To determine the true ASD diameter, an ASD sizing balloon is inflated with contrast under fluoroscopy until left-to-right shunting ceases, as confirmed by color Doppler on ICE. The “stop-flow” technique, in which the balloon is inflated and deflated incrementally until flow ceases, is preferred because it minimizes overestimating defect size. The balloon is then deflated and withdrawn while maintaining the wire position.[13]
The Amplatzer Septal Occluder—a self-expanding, double-disc device made of nitinol mesh with a polyester fabric patch—is the most commonly used closure device and has been FDA-approved since 2001. The device's central waist centers the occluder within the defect, providing stable apposition of both discs across the septum. The device is carefully prepared by immersing it in saline, attaching it to the delivery cable, and flushing the loader sheath to prevent air embolism. The occluder is advanced through the delivery sheath to the left atrium. The left atrial disc is first deployed under ICE and fluoroscopic visualization, ensuring proper expansion and alignment against the septum. Controlled tension is maintained to create mild “tenting” of the septum without prolapse. Once the left disc is well seated, the right atrial disc is unsheathed, completing the device deployment.[12]
Device stability is evaluated with both ICE and fluoroscopy. Color Doppler is used to assess for residual shunting—central color flow through the waist may be acceptable, but flow around the disc edges suggests undersizing or additional defects. In such cases, the device should be retrieved, and a defect reassessment performed. For multiple adjacent ASDs, a larger or cribriform occluder may be used if defects are less than 7 mm apart; otherwise, separate devices are placed for distant defects. Once satisfactory positioning and complete closure are confirmed, the “Minnesota Wiggle” (push-pull maneuver) tests stability. The device is released and rechecked for residual flow and position if stable.[13]
The ICE catheter is used to assess for pericardial effusion or device malposition upon completion. The delivery and venous sheaths are then withdrawn, and hemostasis is achieved with manual compression or a figure-of-8 suture. To reverse anticoagulation, protamine may be administered at the operator’s discretion.
Antithrombotic Therapy
Following transcatheter closure of an atrial septal defect (ASD), appropriate antithrombotic therapy is essential to prevent device-related thrombus formation and subsequent thromboembolic complications during the period before endothelialization. The metallic mesh structure of occluder devices, such as the Amplatzer Septal Occluder, can transiently promote platelet adhesion and thrombus formation until the device becomes fully endothelialized, typically within 3 to 6 months. Following transcatheter ASD closure, dual antiplatelet therapy (DAPT) is initiated immediately to reduce the risk of device-related thrombus formation until complete endothelialization occurs.
Standard practice, as recommended by the American College of Cardiology (ACC) and the European Society of Cardiology (ESC), includes administering a loading dose of clopidogrel (300–600 mg) and aspirin (300 mg) immediately after the procedure. This is followed by maintenance DAPT with aspirin (75–100 mg daily) and clopidogrel (75 mg daily) for 1 to 6 months, depending on patient risk factors and device size. In uncomplicated cases with low thromboembolic risk, particularly in pediatric patients, some centers may use aspirin monotherapy for 6 months. After the DAPT period, aspirin monotherapy is continued for at least 5 years to provide long-term protection against thromboembolic events.[12][13] In patients with additional thrombotic risk factors—such as atrial fibrillation, hypercoagulable states, or large device size—systemic anticoagulation (eg, warfarin with an international normalized ratio [INR] of 2.0–3.0) may be considered for the first 3 months, either in place of or in addition to antiplatelet therapy. However, this approach should be individualized based on bleeding risk and consultation with a cardiologist.
Postprocedure Follow-Up and Long-Term Management
Careful postprocedural monitoring and structured follow-up are essential to ensure the long-term success of transcatheter ASD closure. Immediately following device deployment, patients are observed in a monitored setting for 12 to 24 hours to assess for arrhythmias, bleeding, vascular access complications, or pericardial effusion. Continuous cardiac monitoring is recommended for at least the first 24 hours, as transient atrial arrhythmias—such as atrial fibrillation or supraventricular tachycardia—are not uncommon due to septal irritation.
Echocardiographic evaluation plays a central role in follow-up. TTE is typically performed before discharge, at 1 month, 3 to 6 months, and 12 months postprocedure to confirm complete device seating, absence of residual shunt, and progressive endothelialization. TEE may be indicated in adults, where visualization is suboptimal, or if there are concerns about thrombus formation or erosion. Once closure and device stability are confirmed, long-term follow-up may transition to annual or biennial intervals. Patients should be counseled to avoid strenuous physical activity and heavy lifting for at least 1 to 2 weeks following the procedure to prevent vascular complications at the femoral access site. Competitive sports or vigorous aerobic exercise may be resumed after 3 months, provided follow-up imaging confirms stable closure and no evidence of right heart strain.
Endocarditis prophylaxis remains important during the early postimplantation phase. According to AHA and ESC guidelines, antibiotic prophylaxis is advised 6 months after device implantation or until complete endothelialization is documented.[14][15] For patients with residual shunts adjacent to the device, ongoing prophylaxis is warranted for procedures with a bacteremia risk. Long-term outcomes following transcatheter ASD closure are excellent, with most patients achieving full functional recovery and normalizing right heart chamber size and pulmonary pressures. Interprofessional care coordination among cardiologists, nurses, and pharmacists ensures adherence to antithrombotic therapy, surveillance imaging, and secondary prevention strategies, maximizing patient safety and procedural durability.
Complications
Major complications related to the transcatheter ASD closure include:
Clinical Significance
Catheter-based management of ASDs represents a significant advancement in the treatment of congenital heart disease, offering a minimally invasive alternative to open-heart surgery with reduced morbidity, shorter hospital stays, and faster recovery times. The clinical significance lies in its ability to effectively eliminate left-to-right shunting between the atria, thereby preventing long-term complications such as right heart dilation, pulmonary hypertension, atrial arrhythmias, and paradoxical embolism. Successful transcatheter closure leads to improved cardiac efficiency, symptomatic relief, and enhanced exercise tolerance.
Beyond patient outcomes, this approach has reshaped the standard of care for ASD management by enhancing procedural safety and expanding treatment eligibility to a broader range of patients, including those previously considered high-risk for surgery. The technique’s precision, guided by advanced echocardiographic and fluoroscopic imaging, enables tailored device selection and optimal placement, thereby minimizing complications such as residual shunts or device embolization. As a result, catheter-based ASD closure has become the preferred therapeutic strategy in most cases, demonstrating high procedural success rates and long-term efficacy.
Enhancing Healthcare Team Outcomes
Effective catheter-based management of ASDs relies on a coordinated, multidisciplinary team approach. Interventional cardiologists lead the procedure, performing device deployment, sizing, and hemodynamic monitoring to ensure optimal outcomes. At the same time, echocardiographers provide real-time imaging guidance through transesophageal or intracardiac echocardiography to ensure accurate device placement and defect closure. Cardiac anesthesiologists or sedation specialists maintain hemodynamic stability and optimize patient comfort during the procedure. Catheterization laboratory nurses and technologists manage equipment, monitor vital signs, maintain sterile technique, and assist with device preparation and sheath insertion and removal.
Postprocedure, advanced clinicians, pharmacists, and nurses coordinate anticoagulation and antiplatelet therapy, monitor for complications such as thrombus, arrhythmia, or vascular access issues, and educate patients on activity restrictions, endocarditis prophylaxis, and follow-up imaging. Effective communication between team members is critical for anticipating procedural challenges, responding to complications, and delivering patient-centered care. Collaboration across all roles enhances patient safety, improves clinical outcomes, and strengthens team performance while managing catheter-based ASD.
Media
(Click Image to Enlarge)
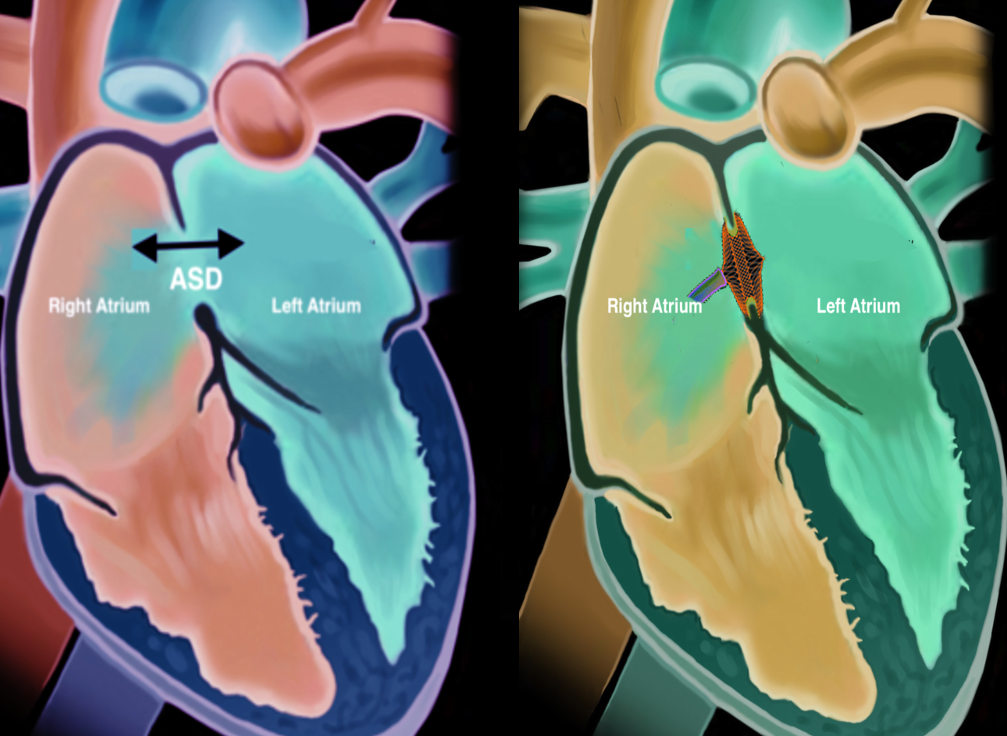
Atrial Septal Defect Closure. This image illustrates a before-and-after image of the heart with an atrial septal defect closure.
Contributed by S Bhimji, MD
References
Hoffman JI, Kaplan S. The incidence of congenital heart disease. Journal of the American College of Cardiology. 2002 Jun 19:39(12):1890-900 [PubMed PMID: 12084585]
Naqvi N, McCarthy KP, Ho SY. Anatomy of the atrial septum and interatrial communications. Journal of thoracic disease. 2018 Sep:10(Suppl 24):S2837-S2847. doi: 10.21037/jtd.2018.02.18. Epub [PubMed PMID: 30305943]
Munjal R, H Frishman W. Management of Atrial Septal Defect in the Adult Population. Cardiology in review. 2025 Sep 15:():. doi: 10.1097/CRD.0000000000001044. Epub 2025 Sep 15 [PubMed PMID: 40952726]
Webb G, Gatzoulis MA. Atrial septal defects in the adult: recent progress and overview. Circulation. 2006 Oct 10:114(15):1645-53 [PubMed PMID: 17030704]
Level 3 (low-level) evidenceYang MC, Wu JR. Recent review of transcatheter closure of atrial septal defect. The Kaohsiung journal of medical sciences. 2018 Jul:34(7):363-369. doi: 10.1016/j.kjms.2018.05.001. Epub 2018 May 30 [PubMed PMID: 30063008]
Fraisse A, Latchman M, Sharma SR, Bayburt S, Amedro P, di Salvo G, Baruteau AE. Atrial septal defect closure: indications and contra-indications. Journal of thoracic disease. 2018 Sep:10(Suppl 24):S2874-S2881. doi: 10.21037/jtd.2018.08.111. Epub [PubMed PMID: 30305947]
Vasquez AF, Lasala JM. Atrial septal defect closure. Cardiology clinics. 2013 Aug:31(3):385-400. doi: 10.1016/j.ccl.2013.05.003. Epub [PubMed PMID: 23931101]
Stout KK, Daniels CJ, Aboulhosn JA, Bozkurt B, Broberg CS, Colman JM, Crumb SR, Dearani JA, Fuller S, Gurvitz M, Khairy P, Landzberg MJ, Saidi A, Valente AM, Van Hare GF. 2018 AHA/ACC Guideline for the Management of Adults With Congenital Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Journal of the American College of Cardiology. 2019 Apr 2:73(12):1494-1563. doi: 10.1016/j.jacc.2018.08.1028. Epub 2018 Aug 16 [PubMed PMID: 30121240]
Level 1 (high-level) evidenceSandeep B, Li H, Huang X, Xiao Z. An editorial regarding the article 'A meta-analysis of atrial septal defect closure in patients with severe pulmonary hypertension: is there a room for poking holes amidst debate?'. Current problems in cardiology. 2024 Jan:49(1 Pt C):102172. doi: 10.1016/j.cpcardiol.2023.102172. Epub 2023 Oct 29 [PubMed PMID: 37907187]
Level 1 (high-level) evidencePham TH, Singh GD. 3D Intracardiac Echocardiography for Structural Heart Interventions. Interventional cardiology clinics. 2024 Jan:13(1):11-17. doi: 10.1016/j.iccl.2023.08.005. Epub 2023 Oct 3 [PubMed PMID: 37980061]
Xu WZ, Shou XY, Li JH, Yu JG, Zhang ZW, Yu J, Ye JJ. Non-fluoroscopic percutaneous transcatheter closure of atrial septal defects in children under transesophageal echocardiographic guidance. World journal of pediatrics : WJP. 2018 Aug:14(4):378-382. doi: 10.1007/s12519-018-0179-x. Epub 2018 Aug 15 [PubMed PMID: 30141110]
Beneki E, Dimitriadis K, Pyrpyris N, Tzimas G, Skalidis I, Meier D, Antiochos P, Kostakis P, Pavlou E, Perone F, Tsivgoulis G, Aggeli C, de Backer O, Tsioufis K. Navigating the Uncertainties of Antithrombotic Therapy After Transcatheter Patent Foramen Ovale Closure: A Comprehensive Review. Catheterization and cardiovascular interventions : official journal of the Society for Cardiac Angiography & Interventions. 2025 Sep:106(3):2037-2047. doi: 10.1002/ccd.70049. Epub 2025 Jul 23 [PubMed PMID: 40702786]
Srivastava A, Patel DA, Dia A, Nathan S, Blair JE, Paul J, Sharma P, Smazil J, Roark L, Friant J, McDowell M, Kalathiya R, Shah AP. Shortened dual anti-platelet therapy duration after percutaneous patent foramen ovale and atrial septal defect closure. The Journal of invasive cardiology. 2025 Aug 11:():. doi: 10.25270/jic/25.00118. Epub 2025 Aug 11 [PubMed PMID: 40815602]
Saric M, Perk G, Purgess JR, Kronzon I. Imaging atrial septal defects by real-time three-dimensional transesophageal echocardiography: step-by-step approach. Journal of the American Society of Echocardiography : official publication of the American Society of Echocardiography. 2010 Nov:23(11):1128-35. doi: 10.1016/j.echo.2010.08.008. Epub 2010 Sep 15 [PubMed PMID: 20833505]
Level 2 (mid-level) evidenceJung SY, Choi JY. Transcatheter closure of atrial septal defect: principles and available devices. Journal of thoracic disease. 2018 Sep:10(Suppl 24):S2909-S2922. doi: 10.21037/jtd.2018.02.19. Epub [PubMed PMID: 30305951]
Munteanu IR, Novaconi RC, Merce AP, Falnita LS, Dima CN, Feier HB. From Catheter Complication to Surgical Success: Urgent Retrieval of an Embolized Amplatzer Device and Valve Repair. Reports (MDPI). 2025 Sep 19:8(3):. doi: 10.3390/reports8030185. Epub 2025 Sep 19 [PubMed PMID: 40981143]
Patil N, Anne U, Narsimhan C, Reddy P, Kapadiya A, Menon R, Gurram P. Massive Systemic and Pulmonary Air Embolism During Atrial Septal Defect Device Closure Managed Successfully by Catheter Aspiration. JACC. Case reports. 2025 Sep 24:30(29):105149. doi: 10.1016/j.jaccas.2025.105149. Epub [PubMed PMID: 41005836]
Level 3 (low-level) evidenceMatsubara Y, Yamano M, Yamano T, Nakamura T, Nakanishi N, Zen K, Shiraishi H, Matoba S. Effects of Transcatheter Atrial Septal Defect Closure in Elderly Patients with Long-Standing Persistent Atrial Fibrillation. International heart journal. 2025:66(5):805-812. doi: 10.1536/ihj.25-244. Epub [PubMed PMID: 41034026]
Lahiri S, Baman M, Huibonhoa RM, Ferns S. High-Density Mapping for AVNRT Ablation with Distorted Conduction System Anatomy Post-ASD Device Closure-Case Report. Indian pacing and electrophysiology journal. 2025 Sep 23:():. pii: S0972-6292(25)00151-2. doi: 10.1016/j.ipej.2025.09.002. Epub 2025 Sep 23 [PubMed PMID: 40998288]
Level 3 (low-level) evidenceWerner RS, Prêtre R, Maisano F, Wilhelm MJ. Fracture of a Transcatheter Atrial Septal Defect Occluder Device Causing Mitral Valve Perforation. The Annals of thoracic surgery. 2019 Jul:108(1):e29-e30. doi: 10.1016/j.athoracsur.2018.11.015. Epub 2018 Dec 12 [PubMed PMID: 30550803]
O'Byrne ML, Levi DS. State-of-the-Art Atrial Septal Defect Closure Devices for Congenital Heart. Interventional cardiology clinics. 2019 Jan:8(1):11-21. doi: 10.1016/j.iccl.2018.08.008. Epub [PubMed PMID: 30449418]
Faccini A, Butera G. Atrial septal defect (ASD) device trans-catheter closure: limitations. Journal of thoracic disease. 2018 Sep:10(Suppl 24):S2923-S2930. doi: 10.21037/jtd.2018.07.128. Epub [PubMed PMID: 30305952]