 Cheiralgia Paresthetica (Wartenberg Syndrome)
Cheiralgia Paresthetica (Wartenberg Syndrome)
Introduction
The radial nerve is susceptible to compression at multiple locations throughout its course. Cheiralgia paresthetica refers specifically to compression or irritation of the superficial branch of the radial nerve in the forearm. Wartenberg first described this condition in 1932, introduced the term cheiralgia paresthetica, and reported 5 clinical cases. The condition is also commonly referred to as Wartenberg syndrome or superficial radial nerve palsy.
The superficial branch of the radial nerve is purely sensory and has no motor component.[1] Therefore, cheiralgia paresthetica presents with pain, burning, numbness, or paresthesia over the dorsoradial aspect of the hand, often involving the first and second digits. Symptoms are frequently aggravated by pronation, pinching, gripping, or repetitive wrist motion, reflecting the dynamic nature of irritation at the point where the nerve becomes superficial.[1]
The radial nerve originates from the posterior cord of the brachial plexus and contains fibers from C5 through C8 and occasionally T1. The nerve descends between the long head of the triceps and the axillary artery, enters the posterior compartment of the arm via the triangular interval, courses along the spiral groove of the humerus, and penetrates the lateral intermuscular septum to enter the anterior compartment of the arm before continuing distally toward the elbow and forearm.[2] Approximately 3 to 5 cm proximal to the supinator, the radial nerve bifurcates into the posterior interosseous nerve and the superficial branch of the radial nerve. The posterior interosseous nerve passes deep into the supinator, while the superficial branch continues distally along the anterolateral forearm, deep to the brachioradialis and near the radial artery.[2]
At approximately 9 cm proximal to the radial styloid, the superficial branch of the radial nerve pierces the deep fascia between the middle and distal thirds of the forearm to become subcutaneous. The nerve subsequently divides into dorsomedial and dorsolateral branches, approximately 4.9 to 5.5 cm proximal to the styloid process. The branches course alongside the cephalic vein and traverse the first dorsal compartment of the wrist near the abductor pollicis longus and extensor pollicis brevis tendons. Sensory innervation includes the dorsolateral and dorsomedial aspects of the first digit proximal to the interphalangeal joint, the dorsoradial hand, and the dorsal aspects of the second and third digits and the radial half of the fourth digit proximal to the distal interphalangeal joints.[3][4] Recent literature emphasizes the value of high-resolution dynamic ultrasonography in evaluating the superficial branch of the radial nerve, particularly during its subcutaneous course near the radial styloid. Ultrasonography can demonstrate focal nerve enlargement, dynamic compression, or positional irritation and may guide targeted interventions in patients with persistent symptoms or inconclusive electrodiagnostic testing.[5]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Cheiralgia paresthetica results from compression, traction, or irritation of the superficial sensory branch of the radial nerve, most commonly at the distal forearm, where the nerve becomes subcutaneous near the radial styloid (see Image. Cheiralgia Paresthetica). The nerve is particularly vulnerable to external mechanical forces and repetitive motion because of its superficial course.[2] External compression is a common cause and may result from tight wristbands, watches, handcuffs, casts, splints, or prolonged pressure during occupational or recreational activities. Repetitive wrist pronation and supination and forceful gripping can exacerbate symptoms by increasing friction or tension on the nerve at its exit point through the deep fascia.[6]
Traumatic and iatrogenic causes are also well recognized. Direct blunt trauma to the radial forearm, distal radius fractures, and surgical procedures involving the wrist or forearm may result in scar formation or localized nerve entrapment. Injection-related injury and postoperative fibrosis have also been described as contributing factors.[7] Additionally, anatomic variations may predispose individuals to nerve irritation. The relationship of the superficial branch of the radial nerve to the brachioradialis, extensor carpi radialis longus, and first dorsal compartment tendons can create dynamic compression during wrist motion, particularly in patients with tendon hypertrophy or inflammatory conditions.[4] Results from recent studies have highlighted the role of dynamic ultrasonographic assessment in identifying focal nerve enlargement, positional compression, or perineural adhesions, thereby supporting a mechanical cause in patients without clear static structural abnormalities.[5]
Epidemiology
Cheiralgia paresthetica (superficial radial nerve neuropathy) is regarded as an uncommon and frequently underrecognized focal neuropathy, in part because symptoms can overlap with de Quervain tenosynovitis and other causes of radial-sided wrist pain. Results from a recent retrospective series of patients with superficial radial nerve neuropathy characterized the condition as rare and commonly related to trauma or external compression.[8] Compared with more common entrapment neuropathies, carpal tunnel syndrome is substantially more prevalent, with a classic population-based Rochester study estimating an age-adjusted incidence of carpal tunnel syndrome of 105 per 100,000 person-years, with higher rates in women than men.[9] Population-level estimates indicate that radial tunnel syndrome is uncommon. Results from a large US insurance-database study showed an annual incidence of 0.0091% and indicated that the diagnosis is rarely assigned.[10] Results from studies evaluating sex and age distributions among patients with superficial radial nerve neuropathy suggested a predominance among women in some series rather than a universally validated fixed ratio such as 4:1, with presentations occurring across adult age ranges.[8]
Pathophysiology
Cheiralgia paresthetica results from focal compression, traction, or repetitive irritation of the superficial sensory branch of the radial nerve, most often at the distal forearm where the nerve pierces the deep fascia and becomes subcutaneous near the radial styloid.[2][3] Mechanical stress at this superficial transition zone can produce localized neurapraxia, segmental demyelination, and ischemia, leading to abnormal afferent signaling and neuropathic symptoms, including burning pain, dysesthesia, and paresthesia, in the dorsoradial distribution of the hand.[1] Furthermore, dynamic factors, such as pronation and supination, tight external compression, or repetitive wrist motion, may worsen symptoms by increasing frictional irritation or traction on the nerve where it courses between the brachioradialis and adjacent tendinous structures.[8] In refractory cases, perineural adhesions or focal entrapment may perpetuate symptoms even in the absence of an obvious mass lesion. Dynamic ultrasonography may demonstrate focal nerve enlargement or irritation and can support targeted, image-guided interventions.[8]
Histopathology
Histopathologic evaluation is not routinely performed in cheiralgia paresthetica because the diagnosis is typically clinical and supported by targeted imaging or electrodiagnostic assessment when needed. When tissue is examined, most often during surgical exploration for refractory symptoms or evaluation of an alternative diagnosis, findings generally reflect chronic compressive neuropathy rather than a disease-specific microscopic pattern.[1] Reported histopathologic changes in compressive sensory neuropathies may include segmental demyelination, endoneurial edema, perineurial thickening, and variable axonal loss depending on chronicity. In longstanding cases, fibrosis and chronic inflammatory changes may be seen in perineural soft tissues, consistent with repeated mechanical irritation or scarring.[8] Additionally, if a space-occupying lesion (eg, ganglion, lipoma, or nerve sheath tumor) is identified as the underlying cause of superficial radial nerve compression, histopathology reflects the primary lesion rather than cheiralgia paresthetica itself. In such cases, microscopic examination is directed toward confirming the etiology (eg, benign cystic lesion or peripheral nerve sheath tumor) and, when clinically indicated, excluding a malignant neoplasm.[7]
History and Physical
Inspection
Inspection should assess for masses, scars, or signs of external compression, such as tight wristbands or casts. The clinician should also evaluate for skin changes over the dorsoradial aspect of the wrist or forearm.
Sensory Examination
Sensation in the first dorsal web space is particularly specific to the superficial branch of the radial nerve. Light touch sensation may be abnormal and has been reported in up to 100% of patients. Two-point discrimination may also be abnormal, typically measuring 4 to 5 mm greater than the contralateral side or greater than 15 mm. Abnormal 2-point discrimination findings have been reported in up to 80% of patients. Vibration sense at 256 Hz may be abnormal and has been reported in up to 100% of patients.
Motor Examination
True motor weakness or muscle atrophy should not be present because the nerve is purely sensory. Grip and pinch strength may appear reduced in up to 80% of patients, usually because of pain rather than denervation.
Provocative and Special Tests
The Tinel test is the most common and important test. Percussion should be performed along the course of the superficial branch of the radial nerve and the lateral antebrachial cutaneous nerve to identify the segment with maximal nerve irritation. Additionally, the Hoffmann test may be performed to evaluate for upper motor neuron pathology when indicated.
The Finkelstein test may be falsely positive in up to 96% of patients. Superficial radial nerve neuropathy may coexist with de Quervain tenosynovitis, complicating interpretation. The Dellon test is performed with active, forceful hyperpronation of the forearm with ulnar deviation and wrist flexion while the elbow is extended at the side. During the Wartenberg neuritis compression test, direct pressure at the brachioradialis insertion reproduces symptoms. Similarly, during the superficial radial nerve compression test, direct pressure at the junction of the brachioradialis and extensor carpi radialis longus elicits symptoms.
Optional Diagnostic Nerve Block
A local anesthetic block of the superficial branch of the radial nerve may be performed to support the diagnosis. The injection is performed subcutaneously near the area of maximal Tinel test response. Ultrasonographic guidance is preferred to reduce the risk of nerve injury. Following a successful block, the Finkelstein test findings should become negative, and grip and pinch strength typically improve.
Evaluation
The evaluation of cheiralgia paresthetica is primarily clinical, supported by targeted imaging or electrodiagnostic testing when the diagnosis is uncertain or symptoms persist. No disease-specific national or international guidelines address cheiralgia paresthetica. However, evaluation principles align with broader recommendations for peripheral nerve entrapment syndromes. Laboratory studies are not routinely indicated because cheiralgia paresthetica is a focal mechanical neuropathy. Laboratory testing may be considered only when alternative diagnoses are suspected, such as systemic inflammatory, metabolic, or infectious neuropathies.
Electrodiagnostic studies, including nerve conduction studies and electromyography, may be performed to exclude proximal radial neuropathy, cervical radiculopathy, or generalized peripheral neuropathy. However, electrodiagnostic findings are often normal in cheiralgia paresthetica because the superficial radial nerve is small and purely sensory, limiting test sensitivity.[8] However, ultrasonography is a valuable adjunct to the evaluation. High-resolution and dynamic ultrasonography can identify focal nerve enlargement, compression, positional irritation, or perineural adhesions at the point where the superficial radial nerve becomes subcutaneous. Ultrasonography also allows assessment for external compression or space-occupying lesions and can guide diagnostic or therapeutic injections.
Magnetic resonance imaging is not routinely required but may be useful when a mass lesion, postsurgical scarring, or alternative pathology is suspected. MRI can delineate soft tissue structures and exclude other causes of dorsoradial wrist pain. Moreover, a diagnostic superficial radial nerve block using local anesthetic may be used when clinical findings are equivocal. Resolution of symptoms after the block supports the diagnosis and may help distinguish cheiralgia paresthetica from coexisting conditions, such as de Quervain tenosynovitis. Overall, accurate evaluation relies on careful clinical localization, judicious use of imaging, and selective application of adjunctive diagnostic tools to confirm superficial radial nerve involvement and exclude mimicking conditions.
Treatment / Management
Management of cheiralgia paresthetica is primarily nonoperative. The initial focus should be on identifying and removing sources of external compression, such as watches, bands, splints, and casts, and reducing repetitive mechanical irritation.[11] Patients should be encouraged to rest, avoid provocative maneuvers, and modify occupational and recreational activities that exacerbate symptoms. Nonsteroidal anti-inflammatory drugs and neuropathic pain medications may be used as adjuncts when clinically appropriate.[11](B3)
In refractory cases, temporary thumb spica splinting and image-guided perineural interventions are reasonable additions. Results from reports described ultrasonography-guided release and perineural corticosteroid injection around the superficial radial nerve as minimally invasive options in selected patients, such as those with perineural adhesions or neuroma-related irritation.[12] More recently, reports described ultrasonography-guided hydrodissection, including the use of 5% dextrose, as a targeted approach when dynamic ultrasonography findings show focal enlargement or irritation and symptoms persist despite conservative measures.[5][13] Underlying medical or regional pain contributors that may compound neuropathic symptoms should also be assessed and addressed. Results from a classic series of 52 patients showed that conservative treatment achieved excellent or good outcomes in 71% of patients.[11](B3)
Surgical intervention is reserved for persistent symptoms despite nonoperative treatment, and a sufficient trial, often approximately 6 months, is typically recommended before proceeding. Clinicians should use caution when operating on patients with painless paresthesias because surgical complications can create painful neuropathic symptoms.[11] Multiple surgical techniques have been described. Approaches focusing on the nerve include open decompression and neurolysis and endoscopically assisted decompression for broader entrapments.[14] Adjunctive strategies to reduce recurrent perineural scarring include neurolysis with nerve wrapping using adhesion barriers, such as amnion-based allografts, in selected patients. Results from reports described this approach as a preliminary option.[15] Other techniques focus on eliminating the underlying compressive source, such as fascial bands, masses, or anatomic variants. For example, a report described a split brachioradialis tendon that entrapped the superficial radial nerve, which required excision of the accessory slip during surgical release.[7](B3)
Surgical Decompression
To approach the superficial branch of the radial nerve, the incision is typically centered over the site of maximal Tinel test response at the distal forearm. The nerve is identified between the brachioradialis and extensor carpi radialis longus and released from constricting fascia and adhesions. Decompression is then performed along the symptomatic segment.[14]
Postoperative Care
Postoperative care commonly emphasizes early motion with protective activity modification for a short interval, followed by progressive rehabilitation. Therapy may include range of motion exercises and desensitization strategies. Return to higher-demand activities should be individualized based on symptoms and healing.[14]
Differential Diagnosis
Cheiralgia paresthetica must be differentiated from other conditions that produce radial-sided wrist or hand pain and sensory disturbance because treatment strategies vary substantially depending on the underlying diagnosis. De Quervain tenosynovitis is the most common clinical mimic. Both conditions may present with radial wrist pain, and the Finkelstein Test can be falsely positive in cheiralgia paresthetica because of the close anatomic relationship between the superficial radial nerve and the first dorsal compartment. Unlike cheiralgia paresthetica, de Quervain tenosynovitis lacks neuropathic sensory symptoms and focal sensory changes in the superficial radial nerve distribution.[1]
First-digit carpometacarpal joint arthritis is a common cause of radial-sided first-digit and wrist pain, particularly in older adults. Pain is typically mechanical and exacerbated by pinching and gripping, with associated joint tenderness, crepitus, or reduced range of motion. Sensory examination findings are usually normal, helping to distinguish first-digit carpometacarpal joint arthritis from superficial radial nerve entrapment.[16] Additionally, intersection syndrome is an overuse tenosynovitis occurring at the intersection of the first dorsal compartment tendons, including the abductor pollicis longus and extensor pollicis brevis, with the second dorsal compartment tendons, including the extensor carpi radialis longus and extensor carpi radialis brevis. Patients typically report dorsoradial distal forearm pain with swelling and crepitus during wrist motion, without sensory disturbance in the superficial radial nerve distribution.[17]
Cervical radiculopathy, particularly involving the C6 or C7 nerve roots, may cause sensory symptoms in the radial forearm and hand but is often associated with neck pain, radiating arm symptoms, and neurologic findings beyond the superficial radial nerve territory.[8] Radial tunnel syndrome and posterior interosseous nerve syndrome involve proximal compression of the radial nerve. Radial tunnel syndrome typically presents with forearm pain, whereas posterior interosseous nerve syndrome may cause motor weakness. Neither condition typically produces isolated sensory symptoms over the dorsoradial aspect of the hand.[10] Moreover, carpal tunnel syndrome may occasionally be confused with cheiralgia paresthetica because both conditions can cause hand paresthesias. However, symptoms of carpal tunnel syndrome predominantly involve the palmar aspect of the first, second, and third digits and may include thenar motor weakness, which is absent in superficial radial nerve entrapment.[9]Finally, lateral antebrachial cutaneous nerve neuropathy can cause sensory changes over the lateral forearm but does not typically extend into the dorsoradial hand or first dorsal web space.[8] Peripheral polyneuropathy and complex regional pain syndrome should be considered when symptoms are bilateral, diffuse, or accompanied by autonomic, trophic, or vasomotor changes rather than focal sensory findings localized to the superficial radial nerve.[6]
Prognosis
The prognosis of cheiralgia paresthetica is generally favorable, particularly when the inciting source of compression or irritation is identified early and addressed. Because the superficial branch of the radial nerve is purely sensory, the condition does not result in motor deficit or muscle atrophy, and many patients experience improvement with conservative treatment alone.[11] Nonoperative treatment, including activity modification, avoidance of external compression, splinting, and pharmacologic therapy, has been associated with good-to-excellent outcomes in the majority of patients. Results from one classic series showed that approximately 71% of patients treated conservatively achieved good or excellent results, supporting an initial trial of nonoperative therapy.[11]
When symptoms persist despite adequate conservative treatment, surgical decompression may provide durable relief. Results from published case series of patients undergoing superficial radial nerve release showed high rates of symptom improvement, particularly when a focal site of compression or structural abnormality is identified intraoperatively.[14] Factors associated with less favorable outcomes include delayed diagnosis, chronic nerve irritation with perineural scarring, and coexisting pathology such as de Quervain tenosynovitis or prior surgical trauma. However, even in refractory cases, targeted intervention, including image-guided perineural procedures or surgical decompression, often results in significant symptom reduction.[5] Overall, with appropriate diagnosis and treatment, most patients experience meaningful symptom improvement and functional recovery, and long-term disability is uncommon.
Complications
Complications of cheiralgia paresthetica most often relate to delayed diagnosis, persistent mechanical irritation, or iatrogenic injury and may result in prolonged neuropathic symptoms rather than permanent disability. Because the superficial branch of the radial nerve is purely sensory, complications primarily involve pain and sensory disturbance rather than motor dysfunction.[1] The most common complication is chronic neuropathic pain, including burning pain, dysesthesia, and allodynia, that persists when the compressive mechanism is not removed or when perineural fibrosis develops. Patients may develop heightened cutaneous sensitivity and activity limitation, particularly with ongoing repetitive wrist motion or external compression.[8] Additionally, misdiagnosis is a frequent clinical pitfall and may lead to unnecessary imaging, ineffective interventions, or delayed definitive treatment. Coexisting conditions, particularly de Quervain tenosynovitis, may further complicate evaluation and contribute to persistent symptoms if not addressed concurrently.[1]
Complications can also occur from diagnostic or therapeutic interventions. Injection-related complications include transient worsening of pain, bleeding or hematoma, infection, and iatrogenic nerve injury if intraneural injection occurs. When ultrasonographic guidance is used for perineural interventions such as hydrodissection, results from studies emphasize targeted delivery around the nerve to reduce procedural risk.[5] Surgical complications may include scar sensitivity, persistent or worsened neuropathic pain, incomplete symptom resolution, neuroma formation, and recurrent symptoms because of re-adhesion or ongoing external irritation. Surgical intervention should therefore be reserved for patients with persistent symptoms despite an adequate course of nonoperative treatment and symptoms that significantly impair function or quality of life.[14] Overall, complications are minimized by early recognition, avoidance of external compression, careful technique during image-guided interventions, and appropriate patient selection for surgical procedures.
Deterrence and Patient Education
Patient education plays a critical role in both the prevention and treatment of cheiralgia paresthetica. Because this condition most often results from external compression or repetitive mechanical irritation of the superficial branch of the radial nerve, patients should be counseled on avoiding contributory factors such as tight wristbands, watches, bracelets, handcuffs, casts, or prolonged pressure on the radial forearm. Activity modification, particularly reducing repetitive pronation and supination, forceful gripping, and sustained wrist flexion, can significantly decrease symptom exacerbation.
Patients should be informed that the involved nerve is purely sensory and that the condition typically does not cause permanent weakness or muscle atrophy. Education regarding the expected course of recovery is important because many patients improve with conservative treatment. Emphasis should be placed on adherence to rest, splinting if prescribed, and appropriate medication use.
Instruction on recognizing worsening or persistent symptoms is also essential. Patients should seek reevaluation if pain becomes progressive, if new neurologic symptoms develop, or if symptoms fail to improve despite activity modification. When image-guided injections or surgical procedures are considered, patients should be counseled regarding realistic expectations, potential risks, and the importance of postoperative rehabilitation to minimize scar formation and recurrence. Through education on ergonomics, symptom monitoring, and treatment adherence, patients can actively participate in reducing the risk of recurrence and optimizing recovery outcomes.
Enhancing Healthcare Team Outcomes
Optimizing outcomes in cheiralgia paresthetica requires coordinated, interprofessional collaboration focused on accurate diagnosis, conservative treatment, and timely referral when indicated. Because the condition is frequently misdiagnosed as de Quervain tenosynovitis or cervical radiculopathy, clinicians must maintain a high index of suspicion and perform careful sensory localization to the superficial radial nerve distribution. Clear documentation of baseline neurologic findings supports continuity of care and reduces diagnostic confusion across clinical settings.[8] Additionally, nurses play a central role in patient education, reinforcement of activity modification strategies, splint adherence, medication counseling, and monitoring for symptom progression. Nurses also contribute to early recognition of complications following injections or surgical procedures, including worsening neuropathic pain or signs of infection.
Pharmacists support safe pharmacologic treatment by reviewing appropriate nonsteroidal anti-inflammatory drug use, monitoring for drug interactions, and assisting with neuropathic pain treatment when prescribed. In patients undergoing image-guided injections, pharmacists help ensure appropriate medication preparation and dosing to enhance safety. Physical and occupational therapists are essential in guiding ergonomic modifications, graded activity progression, desensitization strategies, and nerve-gliding techniques to minimize adhesion formation and improve functional recovery. Early coordinated rehabilitation following surgical decompression can reduce stiffness and scar-related complications.
Ethical, patient-centered care requires shared decision-making, transparent discussion of expected outcomes, and appropriate counseling regarding conservative and surgical treatment options. Effective communication among primary care clinicians, hand specialists, pain specialists, therapists, and nursing staff ensures unified treatment planning and avoids redundant or unnecessary interventions. Through structured collaboration and timely referral, the interprofessional team enhances patient safety, improves functional outcomes, and reduces the risk of chronic neuropathic pain associated with cheiralgia paresthetica.
Media
(Click Image to Enlarge)
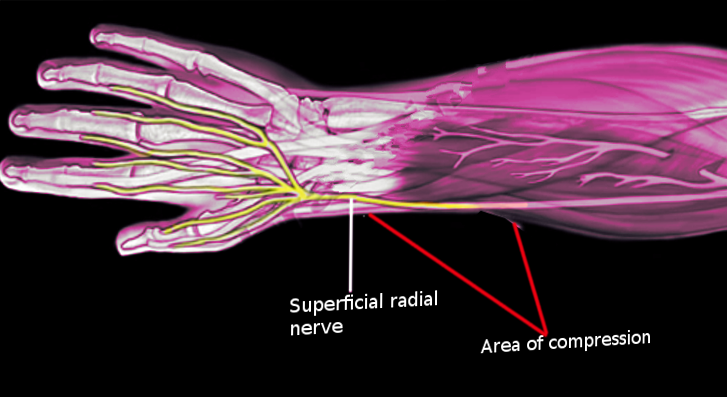
Cheiralgia Paresthetica. This image depicts entrapment of the superficial branch of the radial nerve in the distal forearm, resulting in cheiralgia paresthetica or Wartenberg syndrome.
Contributed by O Chaigasame, MD
References
Braidwood AS. Superficial radial neuropathy. The Journal of bone and joint surgery. British volume. 1975 Aug:57(3):380-3 [PubMed PMID: 1158953]
Bumbasirevic M, Palibrk T, Lesic A, Atkinson H. Radial nerve palsy. EFORT open reviews. 2016 Aug:1(8):286-294. doi: 10.1302/2058-5241.1.000028. Epub 2017 Mar 13 [PubMed PMID: 28461960]
Abrams RA, Brown RA, Botte MJ. The superficial branch of the radial nerve: an anatomic study with surgical implications. The Journal of hand surgery. 1992 Nov:17(6):1037-41 [PubMed PMID: 1430933]
Klitscher D, Müller LP, Rommens P. Anatomical Course of the Superficial Branch of the Radial Nerve and Clinical Significance for Surgical Approaches in the Distal Forearm. European journal of trauma and emergency surgery : official publication of the European Trauma Society. 2007 Feb:33(1):69. doi: 10.1007/s00068-007-6055-3. Epub 2007 Feb 27 [PubMed PMID: 26815977]
Yoon Y, Lam KHS, Castro JC, Hwang J, Lee J, Suryadi T, Suhaimi A, Kang CW, Choi J, Kim S. Ultrasound-Guided Dextrose Hydrodissection for Mixed Sensory-Motor Wartenberg's Syndrome Following a Healed Scaphoid Fracture: A Case Report. Diagnostics (Basel, Switzerland). 2026 Jan 4:16(1):. doi: 10.3390/diagnostics16010156. Epub 2026 Jan 4 [PubMed PMID: 41515651]
Level 3 (low-level) evidenceBerger O, Lomeli BA, Andrakhanov A, Talisman R. Combat-related Wartenberg Syndrome Due to Penetrating Shrapnel Injury: A Case Report. Plastic and reconstructive surgery. Global open. 2024 May:12(5):e5818. doi: 10.1097/GOX.0000000000005818. Epub 2024 May 15 [PubMed PMID: 38752214]
Level 3 (low-level) evidencePotter DC, Wendler DE, Hrycko ER, Puckett HD, Lourie GM. Split Brachioradialis Tendon Causing Wartenberg Syndrome in a Professional Baseball Pitcher. Journal of hand surgery global online. 2023 Mar:5(2):239-241. doi: 10.1016/j.jhsg.2022.11.001. Epub 2023 Jan 18 [PubMed PMID: 36974288]
Shields LBE, Iyer VG, Zhang YP, Shields CB. Etiological study of superficial radial nerve neuropathy: series of 34 patients. Frontiers in neurology. 2023:14():1175612. doi: 10.3389/fneur.2023.1175612. Epub 2023 Apr 20 [PubMed PMID: 37153666]
Stevens JC, Sun S, Beard CM, O'Fallon WM, Kurland LT. Carpal tunnel syndrome in Rochester, Minnesota, 1961 to 1980. Neurology. 1988 Jan:38(1):134-8 [PubMed PMID: 3336444]
Zhang JY, Manirajan A, Wolf JM. The Epidemiology of Radial Tunnel Syndrome and Its Overlap With Lateral Epicondylitis. The Journal of hand surgery. 2023 Nov:48(11):1172.e1-1172.e7. doi: 10.1016/j.jhsa.2023.03.007. Epub 2023 Apr 13 [PubMed PMID: 37923487]
Lanzetta M, Foucher G. Entrapment of the superficial branch of the radial nerve (Wartenberg's syndrome). A report of 52 cases. International orthopaedics. 1993 Dec:17(6):342-5 [PubMed PMID: 8163306]
Level 3 (low-level) evidenceZeng Z, Chen CX. Ultrasound-guided needle release plus corticosteroid injection of superficial radial nerve: A case report. World journal of clinical cases. 2022 Feb 6:10(4):1320-1325. doi: 10.12998/wjcc.v10.i4.1320. Epub [PubMed PMID: 35211565]
Level 3 (low-level) evidenceMaroc M, Lachhab A, Rhoul A, Harmouche M, El Oumri AA. Wartenberg's Syndrome: A Case of Ultrasound Revealing a Diagnosis Missed by Electromyography With Hydrodissection Offering Pain Relief and Functional Recovery. Cureus. 2025 Jul:17(7):e88503. doi: 10.7759/cureus.88503. Epub 2025 Jul 22 [PubMed PMID: 40851692]
Level 3 (low-level) evidenceSpies CK, Müller LP, Oppermann J, Neiss WF, Hahn P, Unglaub F. [Surgical decompression of the superficial radial nerve: Wartenberg syndrome]. Operative Orthopadie und Traumatologie. 2016 Apr:28(2):145-52. doi: 10.1007/s00064-015-0431-7. Epub 2015 Oct 26 [PubMed PMID: 26497308]
Gaspar MP, Kane PM, Vosbikian MM, Ketonis C, Rekant MS. Neurolysis with Amniotic Membrane Nerve Wrapping for Treatment of Secondary Wartenberg Syndrome: A Preliminary Report. The journal of hand surgery Asian-Pacific volume. 2017 Jun:22(2):222-228. doi: 10.1142/S0218810417200015. Epub [PubMed PMID: 28506176]
Normand M, Tang TS, Brismée JM, Sobczak S. Clinical evaluation of thumb base osteoarthritis: A scoping review. Hand therapy. 2021 Jun:26(2):63-78. doi: 10.1177/17589983211002560. Epub 2021 Mar 21 [PubMed PMID: 37969172]
Level 2 (mid-level) evidenceNaredo E, Murillo-González J, Mérida Velasco JR, Olivas Vergara O, Kalish RA, Gómez-Moreno C, García-Carpintero Blas E, Fuensalida-Novo G, Canoso JJ. Examining the Forearm Intersection through Palpation and Ultrasonography. Diagnostics (Basel, Switzerland). 2024 Jan 4:14(1):. doi: 10.3390/diagnostics14010116. Epub 2024 Jan 4 [PubMed PMID: 38201426]