Introduction
The 2 jugular foramina are openings in the skull base located on either side, anterolateral to the foramen magnum (see Image. Jugular Foramen, Transverse View and see Image. Jugular Foramen). The main structures that pass through this foramen are the glossopharyngeal (IX), vagus (X), and spinal accessory (XI) nerves and the internal jugular vein (IJV). Sympathetic fibers from the carotid plexus and inferior vagal (nodose) ganglion also lie adjacent but do not pass through the foramen. The hypoglossal nerve (XII) does not traverse the jugular foramen (it exits via the hypoglossal canal). However, small meningeal branches from XII lie adjacent to the foramen and may be affected in large lesions.
The foramen is divided into 2 parts by a fibro-osseous bridge connecting the jugular spine of the temporal bone and the jugular process of the occipital bone:
- The anteromedial compartment (pars nervosa)
- This contains the cranial nerve IX, the tympanic branch of IX (Jacobson nerve), and the inferior petrosal sinus.
- The posterolateral component (pars venosa or vascularis)
- This contains the IJV, jugular bulb, cranial nerves X and XI, the auricular branch of vagus (Arnold nerve), and the posterior meningeal branch of the ascending pharyngeal artery.[1]
The jugular foramen syndrome (Vernet syndrome) refers to paralysis of the IX, X, and XI cranial nerves traversing the jugular foramen. Maurice Vernet (1887–1974) first described it in the Paris Medical Journal (1917).
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The following etiologies of jugular foramen syndrome have been described in the literature:
- Congenital
- Primary cholesteatoma [2]
- Vascular
- Inflammatory
- Giant cell arteritis
- Immunoglobulin G4-related disease of the skull base
- Wegener granulomatosis
- Infectious
- Varicella-Zoster virus (VZV) infection (recent literature refers to lower-cranial-nerve VZV palsy as a Ramsay Hunt type II variant rather than mechanical compression) [5][6]
- Herpes virus infection [7]
- Parapharyngeal abscess [8]
- Acute otitis media: indirectly causing thrombosis or vascular reaction of the jugular bulb [9]
- Neoplastic
- Benign
- Malignant
- Traumatic
Epidemiology
The exact incidence of jugular foramen syndrome is challenging to estimate due to its rarity. Metastatic disease is the most common cause of jugular foramen syndrome, but it is often underdiagnosed.[20] Skull base metastasis is typically regarded as a manifestation of systemic malignancy. The most common primary cancers that are likely to metastasize to the jugular foramen are those of the breast, lung, kidney, and prostate.[21] Paragangliomas are the most frequent primary lesions, followed by schwannomas and meningiomas.[22] Recent literature suggests that primary lesions are more common than metastases.[23] This discrepancy arises because metastatic disease is more common in oncology cohorts, whereas primary tumors (especially paragangliomas and schwannomas) predominate in skull-base referral centers.
Pathophysiology
Cranial nerve IX is primarily sensory, receiving general visceral and special sensory input from the tonsils, larynx, middle ear, posterior one-third of the tongue, and carotid bodies. This nerve has a small general motor efferent to the stylopharyngeus muscle, which aids in elevating the larynx and pharynx. Cranial nerve X has a wide range of functions and controls heart rate, peristalsis, speech phonation, elevation of the palate, respiration, and autonomic visceral reflexes. Cranial nerve XI is a pure motor efferent supplying the ipsilateral sternocleidomastoid and trapezius muscles. Derangement in the functions of these nerves occurs when they become compressed in jugular foramen syndrome. The proximity of the jugular bulb and sigmoid sinus explains why venous thrombosis or jugular bulb pathology can mimic mass-related jugular foramen syndrome.
Although most cases of jugular foramen syndrome result from compression of structures within the jugular foramen, other mechanisms are implicated in viral infections. These factors can lead to the spread of the virus into the lower cranial nerves, which are as follows:
- Interconnections between upper and lower cranial nerves (spinal accessory nerve plexus)
- Simultaneous reactivation of VZV in multiple ganglia and inter-connecting nerves
- Viral spread through a common blood supply [24]
History and Physical
The most common presenting symptom of jugular foramen syndrome is hoarseness of voice or dysphagia. Pain is also a common associated symptom (persistent unilateral periauricular pain and headache).
Clinical features depend on the structures affected by jugular foramen syndrome:
- Vagus nerve
- Vagal compression initially causes paralysis of the laryngeal muscles, resulting in hoarseness and a nasal timbre. If the nerve is further compressed, it results in unilateral paralysis of the soft palate and deviation of the uvula toward the normal side.
- Glossopharyngeal nerve
- Loss of sensation to the posterior ipsilateral aspect of the tongue
- Dysphagia due to reduced pharyngeal constriction
- Reduced secretions from the ipsilateral parotid gland
- Loss of the ipsilateral gag reflex
- Accessory nerve
- This manifests as drooping of the shoulder, difficulty abducting the ipsilateral arm, and contralateral rotation of the head due to weakness of the sternocleidomastoid and trapezius muscles.
- Obstruction of the traversing venous sinuses and veins
- Headache and papilledema due to intracranial venous congestion leading to cerebral edema and raised intracranial pressure [25]
The clinician should specifically note the following findings in the case of jugular foramen syndrome:
- Nasal regurgitation of liquids and aspiration are key early clinical clues of vagal dysfunction.
- Palatal and gag reflexes
- Drooping of the shoulder
- Unilateral vocal cord palsy: the most reliable sign of vagal nerve involvement
- Power of the sternocleidomastoid and trapezius muscles
- Fasciculation or winging of the scapula
- Other cranial nerves and brainstem involvement
- Cerebellar signs
- Examination of the mouth and external auditory canal for any vesicular rash or mass
- Ipsilateral palatal droop with loss of cough reflex → aspiration risk
- “Wet pillow sign” from nocturnal salivary pooling → subtle but highly specific for cranial nerve IX/X palsy
Some unique presentations include:
Evaluation
The following investigations are aimed at diagnosing the etiology of jugular foramen syndrome:
- Magnetic resonance imaging (MRI) of the head with contrast
- This is the investigation of choice when a patient presents with the clinical diagnosis of jugular foramen syndrome.
- Magnetic resonance angiography and venography may provide additional information on tumor vascularization and local venous anatomy.
- High-resolution 3-dimensional T2 sequences (constructive interference steady-state/fast imaging employing steady-state acquisition/sampling perfection with application-optimized contrasts using different flip-angle evolution) provide the best visualization of the lower cranial nerves within the jugular foramen.
- Digital subtraction angiography
- This is mandatory in patients with highly vascular lesions. Such cases may benefit from preoperative embolization.
- Computed tomography (CT) of the skull base with angiogram
- This imaging will assess the extent of bony erosion and vascular invasion or infiltration, and is necessary to plan surgery.
- 18F-Fludeoxyglucose Positron Emission Tomography (FDG-PET) CT/positron emission tomography (PET)-MRI
- This detects skull base metastases, recurrent paraganglioma, and multifocal schwannomas/neurofibromatosis.
- Ga-68 DOTATATE PET and metaiodobenzylguanidine scans are essential for staging and guiding treatment of paragangliomas.
- Indirect laryngoscopy
- This modality assesses the extent of vocal cord palsy, which may indicate the need for postoperative tracheostomy.
- A fiberoptic speech/voice evaluation (stroboscopy) is recommended to quantify glottic insufficiency and aspiration risk.
- Laboratory tests
- Total blood count, erythrocyte sedimentation rate, C-reactive protein, antinuclear antibodies, extractable-nuclear antigen antibodies, antineutrophil-cytoplasmatic antibodies
- Serum-protein electrophoresis
- VZV and herpes simplex virus
- Immunoglobulins M and G
- Cerebrospinal fluid analysis
- Checks for any hyperproteinorrachia, pleocytosis, or oligoclonal bands
- Polymerase chain reaction to detect VZV
- Nerve conduction studies and electromyography of the sternocleidomastoid and trapezius muscles are performed if there is doubt regarding the diagnosis.
- Genetic testing for paragangliomas
- SDHB mutation → malignant potential
- SDHD mutation → multiple/bilateral tumors
The characteristic finding of glomus jugulare tumors is a ‘‘moth-eaten’’ pattern of destruction of the temporal bone (on CT), a ‘‘salt-and-pepper’’ pattern on long repetition time–long echo time images (on MRI), and a ‘‘dropout’’ phenomenon in time-intensity curves on contrast MRA.
- Paragangliomas displace nerves anteromedially.
- Schwannomas displace nerves laterally/posteriorly.
Treatment / Management
Treatment of jugular foramen syndrome depends on the etiology:
- Surgery
- Safe resection is the treatment of choice and may be curative in schwannomas, meningiomas, noninfiltrative paragangliomas, and other benign tumors. However, stereotactic radiosurgery is preferred for paragangliomas less than 3.5 cm in size, with surgery reserved for young patients, rapidly growing tumors, and if there is evidence of brainstem compression. Subtotal removal may be necessary to preserve the integrity of vascular structures and the brainstem. An interprofessional approach is vital in the radical excision of large paragangliomas with intracranial extension.
- Shunt procedure, venous sinus angioplasty, and stenting, or optic nerve sheath fenestration: these are for intracranial hypertension due to venous sinus stenosis.
- Radiotherapy
- Stereotactic radiosurgery (eg, Gamma Knife, linear accelerator) is a valuable and safe treatment option for paragangliomas at this location when the diameter is less than approximately 3.5 cm (or <20 mL volume), thereby reducing morbidity.[27]
- Fractionated stereotactic radiotherapy combines the precision of stereotaxy with dose fractionation for large tumors exceeding 3 to 4 cm in diameter that are not suitable for radiosurgery.
- Postoperative radiotherapy is sometimes used to control the residual disease following subtotal resection.
- Embolization
- Preoperative embolization may be helpful for extensively vascular tumors, such as paragangliomas, to reduce blood loss during surgery.
- Anticoagulants
- Low molecular weight heparin or direct oral anticoagulants
- Used for jugular vein thrombosis unless contraindicated by intracranial hemorrhage [3]
- Low molecular weight heparin or direct oral anticoagulants
- Acyclovir and steroids (for viral infections) (B2)
Differential Diagnosis
Clinical variants of jugular foramen syndrome include:
- Jackson syndrome
- Dysfunction of IX, X, and XI cranial nerves from a medullary (brainstem) lesion
- Collet–Sicard syndrome
- Dysfunction of cranial nerves IX, X, XI, and XII
- Villaret syndrome
- Dysfunction of cranial nerves IX, X, XI, and XII, with sympathetics (causing an ipsilateral Horner syndrome)
- Tapia syndrome
- Dysfunction of X and XII nerves
- Avellis syndrome
- Vocal cord and palatal paralysis with contralateral dissociative hemianesthesia (loss of pain and temperature sensations, but with preservation of touch)
- Schmidt syndrome
- A lesion of the vagal and both the bulbar and spinal accessory nuclei
Prognosis
Prognosis depends on the specific pattern of compression at the jugular foramen. Compression arising from a benign condition may allow curative resection. Survival in patients with metastatic compression depends on the status of the primary malignancy and the extent of additional systemic metastases.[28] Infectious and vascular causes often respond well to targeted therapy. Posttraumatic lower cranial nerve palsy frequently leads to incomplete recovery in most affected patients.[18]
Complications
The main complications that are likely to occur in patients with jugular foramen syndrome, especially in the postoperative period, include:
- Vocal cord paralysis
- Aspiration pneumonia
- Prevented by delayed extubation, tracheostomy in selected cases, and early rehabilitation
- Exposure keratopathy, if the facial nerve is involved
- May need tarsorrhaphy
- Cerebrospinal fluid leakage
Modern perioperative algorithm (skull base centers) to reduce aspiration-related mortality (the leading cause of death after surgery):
- Laryngoscopy and fibreoptic endoscopic evaluation of swallowing preoperatively
- Temporary nasogastric feeding rather than early percutaneous endoscopic gastrostomy
- Early swallow therapy and vocal cord injection
Deterrence and Patient Education
Deterrence in jugular foramen syndrome focuses on mitigating preventable causes and minimizing progression-related morbidity rather than primary prevention, as many etiologies are structural or neoplastic. Clinicians play a key role in the early identification of risk factors such as head and neck malignancy, skull base tumors, chronic otitis media with skull base involvement, and traumatic or iatrogenic injury. Prompt evaluation of new lower cranial nerve deficits (IX–XI), unilateral dysphagia, hoarseness, shoulder weakness, or aspiration risk is essential to deter delayed diagnosis and irreversible neurologic injury. Adherence to evidence-based diagnostic pathways—including early MRI with skull-base protocols and timely referral to neurology, otolaryngology, or neurosurgery—reduces treatment delays and limits complications such as recurrent aspiration pneumonia, malnutrition, and permanent vocal cord paralysis.
Patient education is central to long-term management and safety. Patients should be counseled to recognize early warning symptoms, understand the underlying cause of their syndrome, and recognize the importance of close follow-up, given the potential for progression or recurrence, particularly in tumor-related cases. Education should emphasize aspiration precautions, engagement in voice and swallow therapy, and nutritional strategies to prevent weight loss and pulmonary complications. Patients undergoing surgical or radiotherapeutic management benefit from clear expectations regarding recovery timelines, potential cranial nerve deficits, and rehabilitation needs. Reinforcing medication adherence, surveillance imaging schedules, and multidisciplinary care coordination empower patients to participate actively in their care, improve quality of life, and reduce preventable morbidity.
Enhancing Healthcare Team Outcomes
Jugular foramen syndrome arises from dysfunction of cranial nerves IX, X, and XI as they traverse the jugular foramen, leading to hoarseness, dysphagia, posterior tongue sensory loss, shoulder weakness, and signs of venous congestion. Etiologies include congenital anomalies, vascular variants, infections, inflammatory disorders, neoplasms, and trauma. Diagnosis depends on careful neurological and otolaryngologic examination supported by high-resolution radiological studies and targeted laryngeal assessment. Early recognition helps prevent aspiration, respiratory compromise, and delayed management.
Management requires coordinated interprofessional care. Physicians, neurologists, and advanced clinicians must identify early deficits, initiate appropriate imaging, and distinguish benign from malignant or vascular processes. Neuroradiologists play a central role in interpreting radiologic findings, whereas neurosurgeons, otolaryngologists, plastic surgeons, and neuroanesthesiologists collaborate when operative intervention is indicated. Nurses support postoperative airway safety, nutrition planning, thrombosis prevention, and early detection of complications, while dietitians and respiratory therapists guide feeding and tracheostomy care. Voice therapists, swallowing specialists, physiotherapists, pharmacists, social workers, and mental health professionals contribute to rehabilitation, medication safety, discharge readiness, and emotional support. Continuous communication across the team strengthens patient-centered care, enhances safety, and optimizes outcomes.
Media
(Click Image to Enlarge)
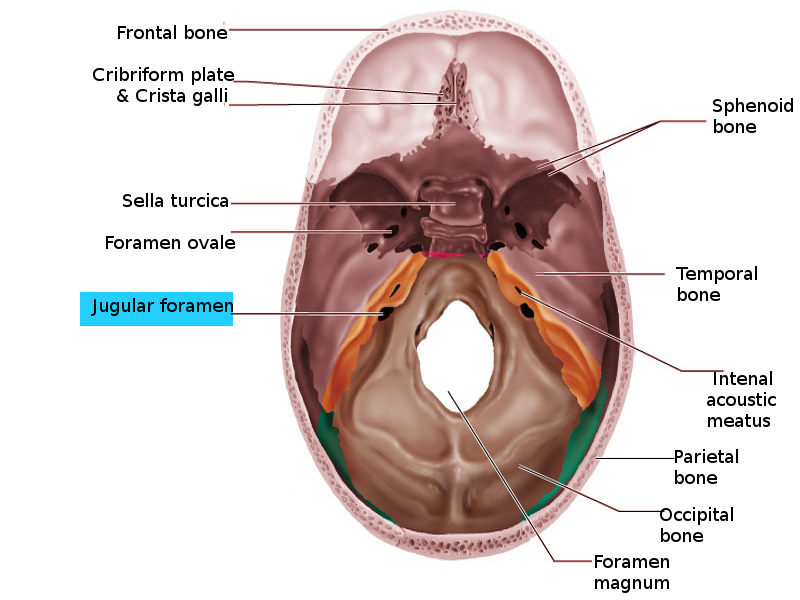
Jugular Foramen, Transverse View. This image shows the 2 jugular foramina, openings in the skull base located on either side, anterolateral to the foramen magnum.
Contributed by S Bhimji, MD
(Click Image to Enlarge)
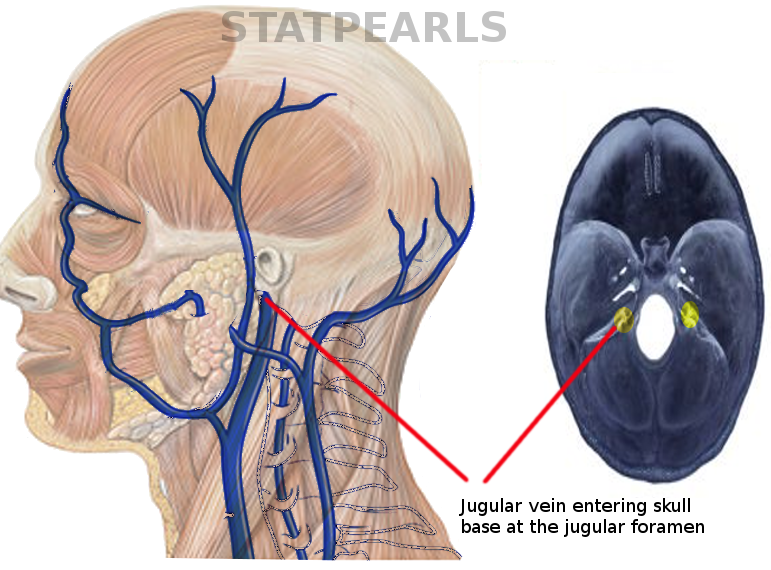
Jugular Foramen. This image shows the jugular vein entering the skull base at the jugular foramen.
Contributed by S Bhimji, MD
References
Singh O, Das JM. Anatomy, Head and Neck: Jugular Foramen. StatPearls. 2025 Jan:(): [PubMed PMID: 30860742]
Erol FS, Kaplan M, Kavakli A, Ozveren MF. Jugular foramen syndrome caused by choleastatoma. Clinical neurology and neurosurgery. 2005 Jun:107(4):342-6 [PubMed PMID: 15885397]
Level 3 (low-level) evidenceLee M, Heo Y, Kim T. Vernet's Syndrome Associated with Internal Jugular Vein Thrombosis. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2019 Feb:28(2):344-346. doi: 10.1016/j.jstrokecerebrovasdis.2018.10.008. Epub 2018 Nov 2 [PubMed PMID: 30396840]
Amano M, Ishikawa E, Kujiraoka Y, Watanabe S, Ashizawa K, Oguni E, Saito A, Nakai Y, Ikeda H, Abe T, Uekusa Y, Matsumura A. Vernet's syndrome caused by large mycotic aneurysm of the extracranial internal carotid artery after acute otitis media--case report. Neurologia medico-chirurgica. 2010 Jan:50(1):45-8 [PubMed PMID: 20098025]
Level 3 (low-level) evidenceFerreira J, Franco A, Teodoro T, Coelho M, Albuquerque L. Vernet syndrome resulting from varicella zoster virus infection-a very rare clinical presentation of a common viral infection. Journal of neurovirology. 2018 Jun:24(3):379-381. doi: 10.1007/s13365-018-0622-8. Epub 2018 Mar 12 [PubMed PMID: 29532442]
Stornaiuolo A, Iodice R, De Simone R, Russo C, Rubino M, Braca S, Miele A, Tozza S, Nolano M, Manganelli F. Multiple cranial neuropathy due to varicella zoster virus reactivation without vesicular rash: a challenging diagnosis. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology. 2023 Oct:44(10):3687-3689. doi: 10.1007/s10072-023-06833-6. Epub 2023 May 9 [PubMed PMID: 37156980]
Ono N, Sakabe A, Nakajima M. [Herpes zoster oticus-associated jugular foramen syndrome]. Brain and nerve = Shinkei kenkyu no shinpo. 2010 Jan:62(1):81-4 [PubMed PMID: 20112795]
Thomasen I, Peitersen E, Peitersen B. [Parapharyngeal abscess complicated by the jugular foramen syndrome. Report of a child aged 2]. Ugeskrift for laeger. 1987 Jul 20:149(30):2023 [PubMed PMID: 3433427]
Level 3 (low-level) evidenceEl-Saied S, Ziv O, Sapir A, Yafit D, Kaplan DM. A Case Study and Concise Literature Review: Adult Patient's Initial Manifestation of Complicated Acute Otitis Media Presenting as Jugular Foramen Syndrome. Clinics and practice. 2025 Feb 12:15(2):. doi: 10.3390/clinpract15020034. Epub 2025 Feb 12 [PubMed PMID: 39996704]
Level 3 (low-level) evidenceDqbrowska A, Jałowiński R, Tarnowska C, Stankiewicz J, Deptuła-Jarosz M. [Paralysis of vocal fold as the first symptom of Vernet's syndrome in the course of jugular chemodectoma]. Otolaryngologia polska = The Polish otolaryngology. 2006:60(5):773-7 [PubMed PMID: 17263253]
Level 3 (low-level) evidenceBinns PM. Jugular foramen syndrome caused by meningioma. Transactions - American Academy of Ophthalmology and Otolaryngology. American Academy of Ophthalmology and Otolaryngology. 1972 Sep-Oct:76(5):1368-70 [PubMed PMID: 4666587]
Aghaghazvini L, Sedighi N, Karami P, Yeganeh O. Skull base aneurysmal bone cyst presented with foramen jugular syndrome and multi-osseous involvement. Iranian journal of radiology : a quarterly journal published by the Iranian Radiological Society. 2012 Sep:9(3):157-60. doi: 10.5812/iranjradiol.7952. Epub 2012 Sep 17 [PubMed PMID: 23329983]
Level 3 (low-level) evidenceRupa V, Rajshekhar V, Bhanu TS, Chandi SM. Primary chondroid chordoma of the base of the petrous temporal bone. The Journal of laryngology and otology. 1989 Aug:103(8):771-3 [PubMed PMID: 2769048]
Level 3 (low-level) evidenceSchweinfurth JM, Johnson JT, Weissman J. Jugular foramen syndrome as a complication of metastatic melanoma. American journal of otolaryngology. 1993 May-Jun:14(3):168-74 [PubMed PMID: 8338200]
Level 3 (low-level) evidenceSenda A, Kaku Y, Komori T, Ueda M, Yonekura S, Yoshikawa Y, Kabashima K. Recurrent cutaneous squamous cell carcinoma in the occipital scalp with clinical perineural invasion developing jugular foramen syndrome. JAAD case reports. 2023 Aug:38():35-37. doi: 10.1016/j.jdcr.2023.05.038. Epub 2023 Jun 8 [PubMed PMID: 37600733]
Level 3 (low-level) evidenceLi Y, Wang Y, Zhao H. Mucoepidermoid carcinoma of the parotid gland with invasion of the jugular foramen region: A case report. Medicine. 2025 Apr 18:104(16):e41925. doi: 10.1097/MD.0000000000041925. Epub [PubMed PMID: 40258716]
Level 3 (low-level) evidenceVaradharajan R, Janarthan S. A Rare Case of Nasopharyngeal Adenocarcinoma Presenting with Vernet's Syndrome. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2025 Jan:77(1):521-524. doi: 10.1007/s12070-024-05155-z. Epub 2024 Oct 30 [PubMed PMID: 40066415]
Level 3 (low-level) evidenceAlberio N, Cultrera F, Antonelli V, Servadei F. Isolated glossopharyngeal and vagus nerves palsy due to fracture involving the left jugular foramen. Acta neurochirurgica. 2005 Jul:147(7):791-4; discussion 794 [PubMed PMID: 15891807]
Level 3 (low-level) evidenceCaldemeyer KS, Mathews VP, Azzarelli B, Smith RR. The jugular foramen: a review of anatomy, masses, and imaging characteristics. Radiographics : a review publication of the Radiological Society of North America, Inc. 1997 Sep-Oct:17(5):1123-39 [PubMed PMID: 9308106]
Hayward D, Morgan C, Emami B, Biller J, Prabhu VC. Jugular foramen syndrome as initial presentation of metastatic lung cancer. Journal of neurological surgery reports. 2012 Oct:73(1):14-8. doi: 10.1055/s-0032-1301406. Epub 2012 Feb 17 [PubMed PMID: 23946920]
Greenberg HS, Deck MD, Vikram B, Chu FC, Posner JB. Metastasis to the base of the skull: clinical findings in 43 patients. Neurology. 1981 May:31(5):530-7 [PubMed PMID: 6972014]
Fayad JN, Keles B, Brackmann DE. Jugular foramen tumors: clinical characteristics and treatment outcomes. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2010 Feb:31(2):299-305. doi: 10.1097/MAO.0b013e3181be6495. Epub [PubMed PMID: 19779386]
Level 2 (mid-level) evidenceCiavarro G, Bozzetti F, Falcioni M. Jugular Foramen Metastasis from Lung Cancer: A Case of "A Mass without His Syndrome". The journal of international advanced otology. 2019 Dec:15(3):469-471. doi: 10.5152/iao.2019.6540. Epub [PubMed PMID: 31257193]
Level 3 (low-level) evidenceJo YR, Chung CW, Lee JS, Park HJ. Vernet syndrome by varicella-zoster virus. Annals of rehabilitation medicine. 2013 Jun:37(3):449-52. doi: 10.5535/arm.2013.37.3.449. Epub 2013 Jun 30 [PubMed PMID: 23869347]
Wilson M, Browne JD, Martin T, Geer C. Case report: atypical presentation of jugular foramen mass. American journal of otolaryngology. 2012 May-Jun:33(3):370-4. doi: 10.1016/j.amjoto.2011.10.006. Epub 2011 Dec 6 [PubMed PMID: 22154064]
Level 3 (low-level) evidenceSaman Y, Whitehead D, Gleeson M. Jugular foramen schwannoma presenting with glossopharyngeal neuralgia syncope syndrome. The Journal of laryngology and otology. 2010 Dec:124(12):1305-8. doi: 10.1017/S0022215110001556. Epub 2010 Jul 6 [PubMed PMID: 20602849]
Level 3 (low-level) evidenceGandía-González ML, Kusak ME, Moreno NM, Sárraga JG, Rey G, Álvarez RM. Jugulotympanic paragangliomas treated with Gamma Knife radiosurgery: a single-center review of 58 cases. Journal of neurosurgery. 2014 Nov:121(5):1158-65. doi: 10.3171/2014.5.JNS131880. Epub 2014 Jun 13 [PubMed PMID: 24926654]
Level 2 (mid-level) evidenceSoffietti R, Rudā R, Mutani R. Management of brain metastases. Journal of neurology. 2002 Oct:249(10):1357-69 [PubMed PMID: 12382150]