Indications
FDA-Approved Indications
Cimetidine is a histamine-2 (H2)-receptor antagonist indicated for the short-term treatment of duodenal and gastric ulcers.[1] The medication effectively controls excessive gastric secretion and is used to treat reflux esophagitis while also preventing stress-related gastric ulcers. With the development of proton pump inhibitors, such as omeprazole, rabeprazole, and pantoprazole, approved for similar indications, cimetidine, along with the other H2-receptor antagonists, is also available as an over-the-counter (OTC) formulation to prevent gastroesophageal reflux disease (GERD) or gastritis.
According to the American College of Gastroenterology guidelines for managing GERD, patients with an incomplete response to proton pump inhibitor therapy may benefit from the addition of a bedtime H2-receptor antagonist. This approach is recommended for patients who continue to experience nocturnal symptoms despite ongoing proton pump inhibitor treatment.[2]
In the past, before the approval of proton pump inhibitors, intravenous (IV) cimetidine was used in critically ill patients in the intensive care unit (ICU) who required prophylaxis against stress-induced ulcers through its H2-receptor antagonist. A meta-analysis concluded that several interventions, including cimetidine, are effective in preventing clinically significant upper gastrointestinal bleeding.[3][4] Cimetidine is also approved by the US Food and Drug Administration (FDA) for the treatment of pathological hypersecretory conditions, including Zollinger–Ellison syndrome, multiple endocrine neoplasia, and systemic mastocytosis.[5]
Off-Label Uses
H2-receptor antagonists, including cimetidine, have been used in the management of functional dyspepsia.[6] Recently, several studies have assessed the use of cimetidine in dermatology, including warts and ulceration. For example, cimetidine has been used for the treatment of multiple warts in pediatric heart transplant recipients.[7] In adults, cimetidine therapy appears to be beneficial with low toxicity in treating recalcitrant warts.[8][9] These effects may be related to reports of cimetidine's immunomodulatory properties, attributed to its ability to reduce regulatory (suppressor) T-cell–mediated immunosuppression.[10]
Several reports suggest that cimetidine can inhibit heme biosynthesis and result in symptomatic improvement in children with acute intermittent porphyria and porphyria cutanea tarda. Both conditions are related to erythropoietic protoporphyria, a rare hereditary disease of heme biosynthesis that manifests with severe photosensitivity and hepatotoxicity. A rapid reduction in photosensitivity has been observed within weeks of initiating systemic cimetidine therapy, along with improvements in cutaneous photosensitivity. Decreases in erythrocyte protoporphyrin levels and improvements in liver function tests have also been reported, with no adverse effects noted over up to 2 years of treatment.[11][12] Similar results were reported with combination therapy using cimetidine and lactulose.[13] However, other researchers have reported insufficient evidence to support a clinical benefit of cimetidine in protoporphyria.[14][15]
Other dermatological indications include condylomata acuminata and papillomatosis in young children; chronic idiopathic urticaria and other types of urticaria; pruritus after a burn injury; and treatment of periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) syndrome.[16][17][18][19][20]
Cimetidine has been shown to enhance cell-mediated immunity following burn injury. In animal studies, it has also mitigated damage induced by long-term, low-dose combined neutron and gamma irradiation, likely through antioxidative and immunomodulatory effects.[21][22][23]
Additional studies support the use of cimetidine for bladder pain associated with interstitial cystitis.[24] It remains unclear whether the mechanism involves a peptidergic pathway in the human bladder similar to cimetidine’s action on gastrointestinal parietal cells.[25] The American Urological Association endorses the use of cimetidine for interstitial cystitis along with other treatment options.[26] Cimetidine has been repurposed as a novel drug for colorectal carcinoma; however, additional research is required to define its role.[27] Cimetidine has also been investigated for its effect on cisplatin-induced ototoxicity and nephrotoxicity.[28][29] A recent study reported an association between long-term use of H2-receptor antagonists and a lower risk of major gynecologic cancers, with notable age- and agent-specific differences. Prospective studies are warranted to confirm causality and inform clinical application.[30]
Mechanism of Action
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Mechanism of Action
Understanding the physiology of gastric acid secretion is essential to the mechanism of action of cimetidine. The primary stimuli for gastric acid secretion include: gastrin, released from antral G cells; histamine, released from oxyntic enterochromaffin-like cells; and acetylcholine, released from antral and oxyntic neurons secondary to parasympathetic (vagal) stimulation.[31] Other stimuli for gastric secretion include ghrelin and motilin.
Gastric acid secretion is largely mediated by histamine acting on parietal cells, which is mediated by adenylate cyclase activation and the generation of cyclic AMP (cAMP).[1] The increase in cAMP activates a specific protein kinase that phosphorylates an unknown substrate, thereby propagating the stimulatory signal (see Image. Mechanism of Action of H2-Receptor Antagonists).[32]
The primary inhibitors of acid secretion include somatostatin, released from oxyntic and antral D-cells, as well as cholecystokinin, atrial natriuretic peptides, nitric oxide, and glucagon-like peptide-1.[33]
Cimetidine, an H2-receptor antagonist, competitively inhibits histamine at H2 receptors located on the gastric parietal cells, which are responsible for hydrochloric acid secretion and intrinsic factor secretion. This effect reduces gastric acid secretion in response to stimuli such as histamine, food, caffeine, and insulin. Cimetidine inhibits both daytime and nocturnal basal gastric acid secretion.[34]
Pharmacokinetics
Absorption: Cimetidine is rapidly absorbed following oral administration, with peak plasma concentrations typically reached within 45 to 90 minutes. Oral and parenteral formulations yield comparable durations of plasma concentrations sufficient to achieve approximately 80% inhibition of basal gastric acid secretion, generally lasting 4 to 5 hours after a 300 mg dose.
Distribution: The volume of distribution is approximately 1 L/kg, with plasma protein binding at about 20%. Cimetidine is widely distributed into tissues, including the lungs, muscles, and kidneys. Additionally, it penetrates the cerebrospinal fluid at a ratio of 0.1 to 0.2 relative to plasma levels.[35] Renal and hepatic impairment may predispose to CNS toxicity.[36]
Metabolism: Cimetidine is metabolized by several hepatic cytochrome P450 (CYP) isoforms (eg, CYP1A2, CYP2C9, and CYP2D6). The drug can also inhibit these enzymes, which can result in clinically significant drug-drug interactions.[37][38]
Excretion: Cimetidine is mainly eliminated by the kidneys. Following IV or intramuscular administration, approximately 75% of the dose is excreted unchanged in the urine within 24 hours, with an elimination half-life of about 2 hours. After oral administration, a greater proportion undergoes hepatic metabolism, with the formation of the sulfoxide as the primary metabolite. After a single oral dose, approximately half of the drug is recovered unchanged in the urine within the first 24 hours.
Administration
Available Dosage Forms and Strengths
Cimetidine is available as oral tablets in strengths of 200 mg, 300 mg, 400 mg, and 800 mg. It is also available as an oral solution (300 mg/5 mL). In addition, cimetidine can be administered parenterally via IV injection.
Dosage
The recommended dosage of cimetidine for pediatric patients is 20 to 40 mg/kg/d, administered in equally divided doses every 6 hours. Lower dosing ranges are used in younger populations, typically 5 to 10 mg/kg/d for neonates and 10 to 20 mg/kg/d for infants, given in divided doses every 6 to 8 hours.
The recommended dosage for treating peptic ulcers in adults is 300 to 400 mg twice daily or 800 mg at bedtime for up to 8 weeks. The maintenance dosage of cimetidine is 400 mg per day.
OTC dosing ranges from 200 to 400 mg daily to prevent or relieve heartburn associated with dietary triggers such as caffeine and certain foods. For optimal effect, cimetidine should be taken approximately 30 minutes before meals.
Specific Patient Populations
Hepatic impairment: No dosage adjustment of cimetidine is recommended in patients with hepatic impairment per the product labeling. However, because cimetidine has been associated with hepatotoxicity, it should be used with caution in patients with underlying hepatic dysfunction or in those receiving concomitant hepatotoxic medications.[37] According to the American Association for the Study of Liver Diseases (AASLD), patients with acute liver failure in the ICU should receive prophylaxis with H2-receptor blocking agents or proton pump inhibitors.[AASLD]
Renal impairment: Clinical experience with cimetidine in patients with severe renal impairment is limited. A reduced dose of 300 mg every 12 hours is recommended. If clinically necessary, dosing frequency may be cautiously increased to every 8 hours. In advanced renal failure, cimetidine accumulation may occur; therefore, the lowest effective dose should be used. Additional dose reductions may be required in the presence of concomitant hepatic impairment. Hemodialysis decreases circulating cimetidine concentrations; dosing should ideally be scheduled to coincide with the completion of dialysis sessions.
Pregnancy considerations: Breastfeeding considerations: According to the American College of Gastroenterology guidelines, approximately two-thirds of pregnant women experience heartburn. Management of GERD should begin with lifestyle modifications. If these are ineffective, first-line pharmacological treatments include antacids, alginates, and sucralfate. All H2-receptor antagonists and proton pump inhibitors are generally considered safe during pregnancy when guided by an appropriate maternal-fetal risk–benefit assessment.[2]
Animal reproductive studies with cimetidine at doses up to 40 times the human dose have not demonstrated impaired fertility or fetal harm. However, adequate and well-controlled studies in pregnant individuals are lacking. As animal reproductive studies may not reliably predict human response, cimetidine should be used during pregnancy only if clearly needed.
Breastfeeding considerations: Maternal doses of cimetidine ranging from 1000 to 1200 mg daily result in infant exposure levels significantly lower than the neonatal doses typically reported, which range from 5 to 10 mg/kg per day. Cimetidine is unlikely to cause adverse effects in breastfed infants, particularly those older than two months. Nonetheless, due to its potential to inhibit hepatic enzymes, alternative drugs may be preferred. Additionally, cimetidine can elevate serum prolactin levels and has been used, though not validated, as a galactogogue.[39]
Pediatric patients: According to the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN), both proton pump inhibitors and H2-receptor antagonists are effective acid-suppressing agents, and similar symptom control may be expected in GERD. Although available studies have methodological limitations, symptom relief with H2-receptor antagonists and proton pump inhibitors appears comparable between these classes. However, proton pump inhibitors are associated with higher rates of healing of erosive or histologic esophagitis after 12 weeks of therapy compared with H2-receptor antagonists.
H2-receptor antagonists are recommended for the treatment of reflux-related erosive esophagitis in infants and children when proton pump inhibitors are unavailable or contraindicated. The guidelines also recommend against using H2-receptor antagonists or proton pump inhibitors to manage crying or distress in otherwise healthy infants. For patients with GERD and typical symptoms, such as heartburn or retrosternal or epigastric pain, a 4- to 8-week course of either a proton pump inhibitor or an H2-receptor antagonist may be considered. The recommended cimetidine dosage in these guidelines is 30 to 40 mg/kg/d.[40]
Older patients: According to the American Geriatric Society 2023 Beers criteria, for potentially inappropriate medication, H2-receptor antagonists such as cimetidine should be avoided in older adults due to increased risk of delirium.[41]
Adverse Effects
High doses of cimetidine (>5 g per day) can cause reversible impotence or gynecomastia.[42] These effects are thought to result from cimetidine's antiandrogenic activity, potentially mediated by increased prolactin levels secondary to H2-receptor blockade. Cimetidine may also exert nonspecific effects that stimulate prolactin secretion, leading to dose-dependent galactorrhea in men.[43][44] These hormonal effects may also be related to inhibition of estradiol 2-hydroxylation. Notably, gynecomastia has not been reported as a significant adverse effect with other H2-receptor blockers (eg, ranitidine, famotidine, and nizatidine).[45]
A low incidence of cimetidine-induced hepatitis has been reported, suggesting a possible hypersensitivity-type reaction.[46] Reported central nervous system (CNS) adverse effects, such as headache, dizziness, delirium, drowsiness, and somnolence, can limit cimetidine's use in the geriatric population and patients with renal and hepatic disorders.[47] Therefore, monitoring renal function is critical in older patients to avoid these neuropsychiatric effects. These adverse effects, along with the availability of proton pump inhibitors approved for treating similar gastrointestinal conditions, have limited the use of cimetidine. An infrequent case of cimetidine-induced hemolytic anemia has been reported.[48]
Cimetidine may precipitate hyperuricemia and acute kidney injury in kidney transplant recipients, potentially due to impaired renal tubular secretion and drug interaction-related mechanisms. Monitoring of uric acid levels may be warranted in high-risk patients.[49]
Drug-Drug Interactions
Cytochrome P450–mediated interactions: Patients receiving drugs metabolized via the CYP pathway may experience increased drug effects when coadministered with cimetidine, a known inhibitor of several CYP450 isoforms, including CYP1A2, CYP2C9, CYP2D6, and CYP3A4. Clinically relevant is the inhibition of CYP3A4 and CYP1A2.[42][50] Inhibition of these enzymes can increase plasma levels of certain drugs, including warfarin, tricyclic antidepressants, lidocaine, calcium channel blockers, quinidine, oral sulfonylureas, phenytoin, theophylline, benzodiazepines, and beta blockers (metoprolol and propranolol). For example, patients treated with warfarin sodium and cimetidine were found to have augmented hypoprothrombinemia and higher blood concentrations of warfarin. Such effects did not occur in patients treated with ranitidine and warfarin sodium. The effect is related to cimetidine's inhibition of hepatic microsomal activity, which reduces the metabolic clearance of warfarin and augments its anticoagulant effect.[51][52]
Beta blockers: Interaction with beta blockers (eg, metoprolol or propranolol) results in significant sinus bradycardia and hypotension.[53] Such interaction does not occur with other beta blockers such as atenolol or nadolol.
Absorption-related interactions (gastric pH): Cimetidine raises the pH of the gastric contents. This increased pH may lead to decreased absorption of drugs that require a lower pH to dissolve, or to increased absorption of drugs whose absorption is reduced by stomach acid inactivation.[54][55]
Vitamin B12 absorption: Impairment of vitamin B12 absorption raises the possibility that long-term, full-dose therapy with cimetidine may produce B12 deficiency similar to that observed in other hypochlorhydric states.[56] This effect occurs because parietal cells produce intrinsic factor, which is necessary for vitamin B12 absorption. This effect is more common in younger female patients and will resolve with the discontinuation of cimetidine therapy.[56]
Dofetilide: Cimetidine increases dofetilide exposure by inhibiting its renal tubular secretion; therefore, concurrent administration should be avoided.[57]
Eliglustat: Eliglustat, used in Gaucher disease type 1, is metabolized by hepatic CYP2D6 and CYP3A4. Concurrent administration with cimetidine should be avoided.[58]
Iron absorption: Excessive use of H2 receptor antagonists may predispose patients to iron deficiency anemia, although direct clinical evidence is limited.[59]
Contraindications
According to the product labeling, the absolute contraindication is hypersensitivity to cimetidine or any of its excipients. Relative contraindications include severe renal or hepatic impairment and certain comorbid conditions, as outlined below.
Cimetidine may cause mild, clinically insignificant increases in serum creatinine in a substantial proportion of patients; these elevations typically resolve after discontinuation of the drug.[60] Dose adjustment is recommended in renal impairment: patients with a GFR of 10 to 50 mL/min should receive 50% of the usual dose, whereas those with a GFR below 10 mL/min should receive 300 mg every 8 to 12 hours. Older patients (aged ≥65 years and with a creatinine clearance below 50 mL/min) should be treated with lower doses to prevent the risk of mental status changes.
The use of acid-suppressing drugs during the first trimester of pregnancy is not associated with significant teratogenic risks.[61][62] Animal studies of cimetidine have not demonstrated fetal risk; however, adequate and well-controlled studies in pregnant individuals are lacking.
Warnings and Precautions
- Malignancy: Symptomatic improvement with histamine H2-receptor antagonists, such as cimetidine, does not exclude the presence of gastric malignancy.
- Dispensing error: Clozapine toxicity has been reported in pediatric patients due to a pharmacy dispensing error.[63]
- Vitamin B12 deficiency: Prolonged treatment may cause vitamin B12 malabsorption and lead to deficiency. The risk appears to be dose-dependent, with a stronger association in females and in individuals aged 30 or younger. Prevalence decreases after discontinuation of therapy.[46]
Monitoring
Because serum creatinine levels may increase during therapy, renal function should be monitored to determine whether dose adjustment or discontinuation of cimetidine is necessary. The presence of blood in the stool may indicate underlying gastrointestinal pathology or drug-related toxicity; therefore, fecal occult blood testing should be considered, particularly in patients using cimetidine without medical supervision or in those receiving dual antiplatelet therapy or anticoagulants.[64]
Although rare, bone marrow suppression has been reported; a complete blood count should be obtained if signs of infection develop. Cimetidine has also been associated with drug-induced liver injury, including a mixed hepatocellular–cholestatic pattern. Monitoring of liver function tests may be warranted in patients with preexisting hepatic impairment or in those taking concomitant hepatotoxic medications.[37]
Toxicity
Signs and Symptoms of Overdose
Cimetidine overdose is uncommon. Severe central nervous system effects, including altered mental status, have been reported following ingestion of 20 to 40 grams, which significantly exceeds therapeutic levels.[65] Rare cases have been documented when multiple CNS-active medications were used concurrently, and cimetidine was taken at doses below 20 grams.
In one report, an older, medically ill, dehydrated patient with underlying brain pathology who was receiving concurrent antipsychotics and IV cimetidine at 4,800 mg over 24 hours experienced mental decline that resolved upon discontinuation of cimetidine. Two fatalities have been reported in adults following single ingestions exceeding 40 grams.
Management of Overdose
No specific antidote for cimetidine exists. Management consists of prompt discontinuation of the drug and supportive care. In cases of significant toxicity, airway protection and cardiovascular stabilization are essential. Decontamination of cimetidine includes gastric lavage and activated charcoal administration to reduce drug absorption. Supportive therapy should be provided. For complex or severe overdoses, consultation with a poison control center or medical toxicologist is recommended for current management guidance. Please see StatPearls' companion resource, "Poison Control In The United States," for more information.
Enhancing Healthcare Team Outcomes
As described above in the Beers criteria, cimetidine should be avoided in older adults with delirium or those at high risk, as H2-receptor antagonists may exacerbate mental status changes or contribute to cognitive decline.[66]
Healthcare professionals, including pharmacists, primary care clinicians, and nurse practitioners, should counsel patients to discontinue the medication promptly and report any signs of an allergic reaction or worsening gastrointestinal symptoms, especially blood in the stool, as a more thorough evaluation will be required. Clinicians, gastroenterologists, pharmacists, and nurses should carefully review the patient’s medication profile, including the use of H2-receptor antagonists, to avoid decreased metabolism of other drugs by cimetidine, which inhibits cytochrome P450 isoenzymes. This potential interaction is significant, especially since cimetidine is available OTC and patients might take it without first consulting their healthcare team.
The risk of drug–drug interactions is particularly significant in patients receiving warfarin; therefore, the interprofessional healthcare team should be vigilant regarding this combination. Nurses often obtain medication information from patients, and pharmacists can help verify nonprescription drug use. Any concerns should be communicated promptly to the broader healthcare team to support coordinated care and minimize adverse outcomes. In the event of overdose, an emergency medicine clinician should prioritize rapid stabilization. As noted, consultation with a medical toxicologist is recommended, particularly in cases involving polysubstance or unknown ingestions.[67]
Patients with suspected peptic ulcer disease should undergo evaluation with upper gastrointestinal endoscopy and gastric mucosal biopsy. Those with confirmed Helicobacter pylori infection should receive standard triple therapy (a proton pump inhibitor and 2 antibiotics—clarithromycin and amoxicillin or metronidazole—to eradicate the disease, rather than only symptomatic treatment with an H2-receptor antagonist.
Bismuth-based quadruple therapy is also highly effective and is often used as a first-line treatment to eradicate H pylori in regions with high clarithromycin resistance. This regimen includes a proton pump inhibitor, bismuth, metronidazole, and tetracycline (or doxycycline) administered for 10 to 14 days.[68] In pregnancy, patients with reflux esophagitis may be treated with H2-receptor antagonists such as cimetidine, ranitidine, or famotidine. Available data do not indicate an increased risk of spontaneous abortion, preterm labor, or low birth weight with first-trimester exposure to H2-receptor antagonists.[69] However, ranitidine has been studied more extensively, making it the preferred H2-receptor antagonist in pregnancy.[62]
The SBAR approach can help reduce the risk of adverse drug reactions and drug–drug interactions in this setting.[70]
Situation: A patient receiving cimetidine develops new-onset confusion and bradycardia.Background: Cimetidine was initiated for stress ulcer prophylaxis, and the patient is also receiving warfarin and phenytoin.Assessment: Cimetidine inhibits cytochrome P450 enzymes and may increase serum concentrations of these medications, which could explain the clinical findings.Recommendation: The healthcare team should review potential drug–drug interactions and consider switching to an alternative histamine H2-receptor antagonist, such as famotidine.
This structured SBAR format helps support clear interprofessional communication and promotes safer medication management.
Given cimetidine’s interaction profile and risk of adverse effects, along with the improved safety profiles of newer H2-receptor antagonists, it may not be the preferred initial therapeutic option for many patients. An interprofessional approach, with effective communication among physicians, advanced practice providers, pharmacists, and nurses, is essential to minimize adverse effects and optimize patient outcomes during cimetidine therapy.
Media
(Click Image to Enlarge)
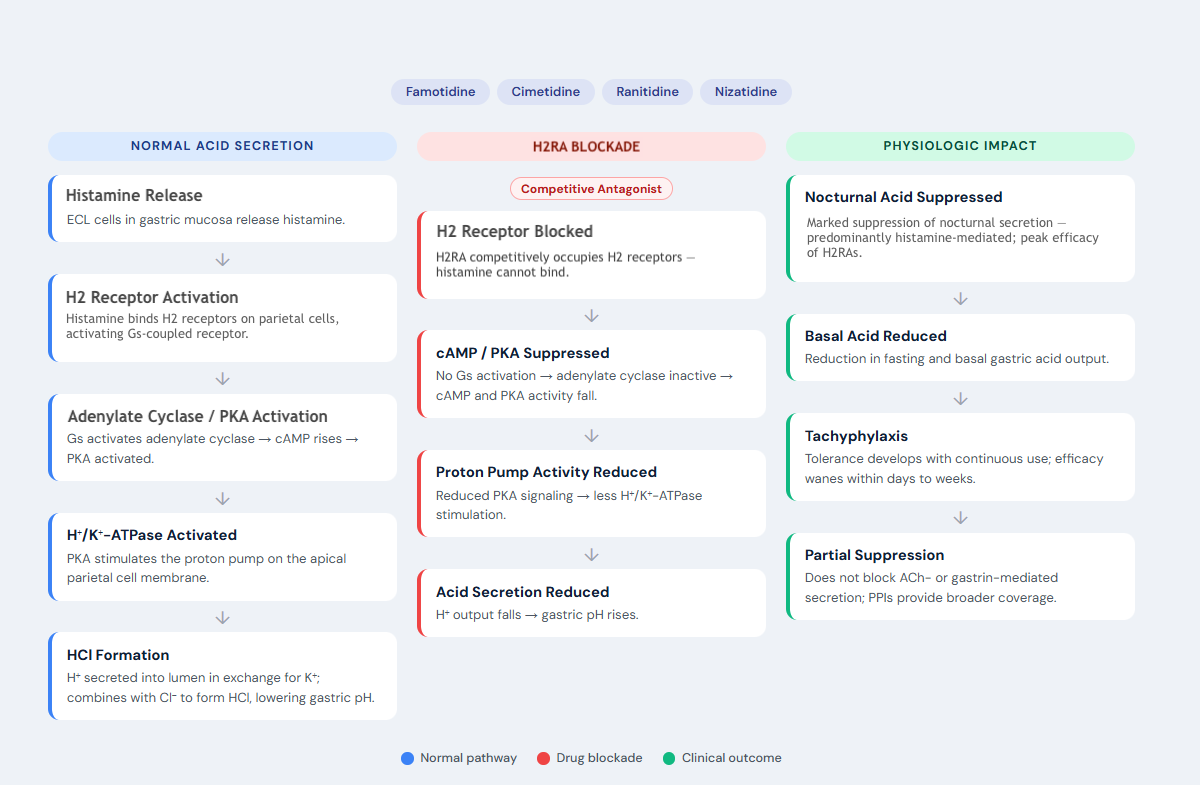
Mechanism of Action of H2-Receptor Antagonists. Abbreviations: ACh, acetylcholine; cAMP, cyclic AMP; ECL, enterochromaffin-like cells; H2, histamine-2; H2RA, H2 receptor antagonist; PKA, protein kinase A; PPI, proton pump inhibitor.
Contributed by P Patel, PharmD
References
Shamburek RD, Schubert ML. Control of gastric acid secretion. Histamine H2-receptor antagonists and H+K(+)-ATPase inhibitors. Gastroenterology clinics of North America. 1992 Sep:21(3):527-50 [PubMed PMID: 1355465]
Katz PO, Dunbar KB, Schnoll-Sussman FH, Greer KB, Yadlapati R, Spechler SJ. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. The American journal of gastroenterology. 2022 Jan 1:117(1):27-56. doi: 10.14309/ajg.0000000000001538. Epub [PubMed PMID: 34807007]
Toews I, Hussain S, Nyirenda JLZ, Willis MA, Kantorová L, Slezáková S, Boltena MT, Peter JV, Fontes LES, Klugar M, Sadeghirad B, Meerpohl JJ. Pharmacological interventions for preventing upper gastrointestinal bleeding in people admitted to intensive care units: a network meta-analysis. BMJ evidence-based medicine. 2025 Jan 22:30(1):22-35. doi: 10.1136/bmjebm-2024-112886. Epub 2025 Jan 22 [PubMed PMID: 38997152]
Level 1 (high-level) evidenceHall WM, Ratliff TB. Intensive care experience with intravenous cimetidine. Alabama medicine : journal of the Medical Association of the State of Alabama. 1990 Oct:60(4):22, 24, 26-8 [PubMed PMID: 2281832]
Level 3 (low-level) evidencePardanani A. Systemic mastocytosis in adults: 2023 update on diagnosis, risk stratification and management. American journal of hematology. 2023 Jul:98(7):1097-1116. doi: 10.1002/ajh.26962. Epub 2023 May 22 [PubMed PMID: 37309222]
Redstone HA, Barrowman N, Veldhuyzen Van Zanten SJ. H2-receptor antagonists in the treatment of functional (nonulcer) dyspepsia: a meta-analysis of randomized controlled clinical trials. Alimentary pharmacology & therapeutics. 2001 Sep:15(9):1291-9 [PubMed PMID: 11552898]
Level 1 (high-level) evidenceDas BB, Anton K, Soares N, Riojas S, Mcdermott J, Knox L, Daneman S, Puente BN. Cimetidine: A Safe Treatment Option for Cutaneous Warts in Pediatric Heart Transplant Recipients. Medical sciences (Basel, Switzerland). 2018 Apr 8:6(2):. doi: 10.3390/medsci6020030. Epub 2018 Apr 8 [PubMed PMID: 29642499]
Glass AT, Solomon BA. Cimetidine therapy for recalcitrant warts in adults. Archives of dermatology. 1996 Jun:132(6):680-2 [PubMed PMID: 8651718]
Ramos-Arancibia N, Varas C, Rozas-Muñoz E. Severe and recalcitrant periungual warts in a child successfully treated with cimetidine. Dermatologic therapy. 2021 Nov:34(6):e15154. doi: 10.1111/dth.15154. Epub 2021 Oct 15 [PubMed PMID: 34623743]
Jafarzadeh A, Nemati M, Khorramdelazad H, Hassan ZM. Immunomodulatory properties of cimetidine: Its therapeutic potentials for treatment of immune-related diseases. International immunopharmacology. 2019 May:70():156-166. doi: 10.1016/j.intimp.2019.02.026. Epub 2019 Feb 22 [PubMed PMID: 30802678]
Tu JH, Sheu SL, Teng JM. Novel Treatment Using Cimetidine for Erythropoietic Protoporphyria in Children. JAMA dermatology. 2016 Nov 1:152(11):1258-1261. doi: 10.1001/jamadermatol.2016.2303. Epub [PubMed PMID: 27410690]
Wulf HC, Philipsen PA, Lerche CM. Cimetidine (H(2) histamine antagonist), Fexofenadine (H(1) histamine antagonist), and Zinc sulphate in the treatment of erythropoietic protoporphyria. Photodiagnosis and photodynamic therapy. 2025 Jun:53():104644. doi: 10.1016/j.pdpdt.2025.104644. Epub 2025 May 22 [PubMed PMID: 40412707]
Fujimori N, Komatsu M, Tanaka N, Iwaya M, Nakano H, Sugiura A, Yamazaki T, Shibata S, Iwaya Y, Muraki T, Ichikawa Y, Kimura T, Joshita S, Umemura T, Matsumoto A, Tanaka E. Cimetidine/lactulose therapy ameliorates erythropoietic protoporphyria-related liver injury. Clinical journal of gastroenterology. 2017 Oct:10(5):452-458. doi: 10.1007/s12328-017-0760-1. Epub 2017 Jul 4 [PubMed PMID: 28676994]
Langendonk JG, Wilson JHP. Insufficient Evidence of Cimetidine Benefit in Protoporphyria. JAMA dermatology. 2017 Feb 1:153(2):237. doi: 10.1001/jamadermatol.2016.4049. Epub [PubMed PMID: 30974454]
Teng JMC, Tu JH. Insufficient Evidence of Cimetidine Benefit in Protoporphyria-Reply. JAMA dermatology. 2017 Feb 1:153(2):238. doi: 10.1001/jamadermatol.2016.4050. Epub [PubMed PMID: 30974455]
Franco I. Oral cimetidine for the management of genital and perigenital warts in children. The Journal of urology. 2000 Sep:164(3 Pt 2):1074-5 [PubMed PMID: 10958744]
Negro-Alvarez JM, Miralles-López JC. Chronic idiopathic urticaria treatment. Allergologia et immunopathologia. 2001 Jul-Aug:29(4):129-32 [PubMed PMID: 11674926]
Baker RA, Zeller RA, Klein RL, Thornton RJ, Shuber JH, Marshall RE, Leibfarth AG, Latko JA. Burn wound itch control using H1 and H2 antagonists. The Journal of burn care & rehabilitation. 2001 Jul-Aug:22(4):263-8 [PubMed PMID: 11482684]
Level 1 (high-level) evidenceGaggiano C, Rigante D, Sota J, Grosso S, Cantarini L. Treatment options for periodic fever, aphthous stomatitis, pharyngitis, and cervical adenitis (PFAPA) syndrome in children and adults: a narrative review. Clinical rheumatology. 2019 Jan:38(1):11-17. doi: 10.1007/s10067-018-4361-2. Epub 2018 Nov 28 [PubMed PMID: 30488366]
Level 3 (low-level) evidenceRaeeskarami SR, Sadeghi P, Vahedi M, Asna Ashari K, Mousavi T M, Ziaee V. Colchicine versus cimetidine: the better choice for Periodic fever, aphthous stomatitis, pharyngitis, adenitis (PFAPA) syndrome prophylaxis, and the role of MEFV gene mutations. Pediatric rheumatology online journal. 2022 Aug 31:20(1):72. doi: 10.1186/s12969-022-00733-3. Epub 2022 Aug 31 [PubMed PMID: 36045426]
Kokhaei P, Barough MS, Hassan ZM. Cimetidine effects on the immunosuppression induced by burn injury. International immunopharmacology. 2014 Sep:22(1):273-6. doi: 10.1016/j.intimp.2014.07.003. Epub 2014 Jul 16 [PubMed PMID: 25038319]
Jiang DW, Wang QR, Shen XR, He Y, Qian TT, Liu Q, Hou DY, Liu YM, Chen W, Ren X, Li KX. Radioprotective effects of cimetidine on rats irradiated by long-term, low-dose-rate neutrons and (60)Co γ-rays. Military Medical Research. 2017:4():7. doi: 10.1186/s40779-017-0116-7. Epub 2017 Feb 27 [PubMed PMID: 28261494]
Sinha S, Gabriel VA, Arora RK, Shin W, Scott J, Bharadia SK, Verly M, Rahmani WM, Nickerson DA, Fraulin FO, Chatterjee P, Ahuja RB, Biernaskie JA. Interventions for postburn pruritus. The Cochrane database of systematic reviews. 2024 Jun 5:6(6):CD013468. doi: 10.1002/14651858.CD013468.pub2. Epub 2024 Jun 5 [PubMed PMID: 38837237]
Level 1 (high-level) evidenceLopez SR, Mangır N. Current standard of care in treatment of bladder pain syndrome/interstitial cystitis. Therapeutic advances in urology. 2021 Jan-Dec:13():17562872211022478. doi: 10.1177/17562872211022478. Epub 2021 Jun 12 [PubMed PMID: 34178118]
Level 3 (low-level) evidenceDasgupta P, Sharma SD, Womack C, Blackford HN, Dennis P. Cimetidine in painful bladder syndrome: a histopathological study. BJU international. 2001 Aug:88(3):183-6 [PubMed PMID: 11488726]
Clemens JQ, Erickson DR, Varela NP, Lai HH. Diagnosis and Treatment of Interstitial Cystitis/Bladder Pain Syndrome. The Journal of urology. 2022 Jul:208(1):34-42. doi: 10.1097/JU.0000000000002756. Epub 2022 May 10 [PubMed PMID: 35536143]
Gunasekara W, Sachindra J, Madhushika MT, Liyanage P, Lekamwasam S. Cimetidine repurposed as a potential immunomodulatory agent against colorectal carcinoma: A systematic review. Journal of oncology pharmacy practice : official publication of the International Society of Oncology Pharmacy Practitioners. 2024 Jul:30(5):930-936. doi: 10.1177/10781552241247007. Epub 2024 Apr 9 [PubMed PMID: 38592456]
Level 1 (high-level) evidenceWu H, Ning Y, Sun Z, Ji J, Lu M, Jiao X, Xu X, Ding X, Cheng X, Yu X. Both carvedilol and cimetidine alleviate cisplatin-induced nephrotoxicity via downregulating OCT2. Biochimica et biophysica acta. Molecular basis of disease. 2025 Jun:1871(5):167754. doi: 10.1016/j.bbadis.2025.167754. Epub 2025 Mar 6 [PubMed PMID: 40044066]
Sinha R, Liu SJ, Lee R, Boyd J, Geary K, Zhang D. Using cimetidine to mitigate cisplatin-induced ototoxicity. Toxicology in vitro : an international journal published in association with BIBRA. 2025 Apr:104():106025. doi: 10.1016/j.tiv.2025.106025. Epub 2025 Feb 11 [PubMed PMID: 39947413]
Chiang CJ, Nguyen NTH, Huang CW, Nguyen PA, Wang SF, Wang CH, Hung FH, Lin GL, Liu YC, Yang HC. The Potential Impact of Histamine-2 Receptor Antagonists on Gynecologic Cancer Risk: A Population-Based Study of 23 Million Individuals. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2026 Apr 1:35(4):540-547. doi: 10.1158/1055-9965.EPI-25-1306. Epub [PubMed PMID: 41575739]
Kurbel S, Kurbel B. The role of gastric mast cells, enterochromaffin-like cells and parietal cells in the regulation of acid secretion. Medical hypotheses. 1995 Dec:45(6):539-42 [PubMed PMID: 8771047]
Level 3 (low-level) evidenceWollin A. Regulation of gastric acid secretion at the cellular level. Clinical and investigative medicine. Medecine clinique et experimentale. 1987 May:10(3):209-14 [PubMed PMID: 2887322]
Level 3 (low-level) evidenceSchubert ML. Physiologic, pathophysiologic, and pharmacologic regulation of gastric acid secretion. Current opinion in gastroenterology. 2017 Nov:33(6):430-438. doi: 10.1097/MOG.0000000000000392. Epub [PubMed PMID: 28787289]
Savarino EV, Barberio B, Scarpignato C, Savarino V, Barbara G, Bertin L, Bonazzi E, de Bortoli N, Sario AD, Esposito G, Frazzoni M, Galloro G, Gatta L, Ghisa M, Londoni C, Marabotto E, Meggio A, Pisani A, Ribolsi M, Usai Satta P, Stanghellini V, Tosetti C, Visaggi P, Zingone F, Pesce M, Sarnelli G. Italian guidelines for the diagnosis and management of gastro-esophageal reflux disease: Joint consensus from the Italian Societies of: Gastroenterology and Endoscopy (SIGE), Neurogastroenterology and Motility (SINGEM), Hospital Gastroenterologists and Endoscopists (AIGO), Digestive Endoscopy (SIED), and General Medicine (SIMG). Digestive and liver disease : official journal of the Italian Society of Gastroenterology and the Italian Association for the Study of the Liver. 2025 Aug:57(8):1550-1577. doi: 10.1016/j.dld.2025.04.020. Epub 2025 May 30 [PubMed PMID: 40450492]
Level 3 (low-level) evidenceSomogyi A, Gugler R. Clinical pharmacokinetics of cimetidine. Clinical pharmacokinetics. 1983 Nov-Dec:8(6):463-95 [PubMed PMID: 6418428]
Rushton AR. Pseudohypoparathyroidism, cimetidine, and neurologic toxicity. Annals of internal medicine. 1983 May:98(5 Pt 1):677 [PubMed PMID: 6847003]
. Cimetidine. LiverTox®: Clinical and Research Information on Drug-Induced Liver Injury. 2012:(): [PubMed PMID: 31643460]
Stuijt DG, Cnossen VM, Osman AFYSM, van Gelder T, Arend SM. Use of cimetidine to enhance systemic acyclovir concentrations in patients with ineffective suppressive therapy for recurring herpes simplex virus infections: A novel purpose for an old drug. British journal of clinical pharmacology. 2025 Oct 9:():. doi: 10.1111/bcp.70313. Epub 2025 Oct 9 [PubMed PMID: 41063629]
. Cimetidine. Drugs and Lactation Database (LactMed®). 2006:(): [PubMed PMID: 30000265]
Rosen R, Vandenplas Y, Singendonk M, Cabana M, DiLorenzo C, Gottrand F, Gupta S, Langendam M, Staiano A, Thapar N, Tipnis N, Tabbers M. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition. Journal of pediatric gastroenterology and nutrition. 2018 Mar:66(3):516-554. doi: 10.1097/MPG.0000000000001889. Epub [PubMed PMID: 29470322]
Level 1 (high-level) evidenceBy the 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. Journal of the American Geriatrics Society. 2023 Jul:71(7):2052-2081. doi: 10.1111/jgs.18372. Epub 2023 May 4 [PubMed PMID: 37139824]
Sabesin SM. Safety issues relating to long-term treatment with histamine H2-receptor antagonists. Alimentary pharmacology & therapeutics. 1993:7 Suppl 2():35-40 [PubMed PMID: 8103374]
Knigge UP. Histaminergic regulation of prolactin secretion. Danish medical bulletin. 1990 Apr:37(2):109-24 [PubMed PMID: 2188799]
Level 3 (low-level) evidenceDelle Fave GF, Tamburrano G, De Magistris L, Natoli C, Santoro ML, Carratu R, Torsoli A. Gynaecomastia with cimetidine. Lancet (London, England). 1977 Jun 18:1(8025):1319 [PubMed PMID: 68422]
Level 3 (low-level) evidenceFeingold KR, Adler RA, Ahmed SF, Anawalt B, Blackman MR, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hamilton E, Hofland J, Jan de Beur S, Kalra S, Kaltsas G, Kapoor N, Kim M, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Swerdloff RS, Ng JCM. Gynecomastia: Etiology, Diagnosis, and Treatment. Endotext. 2000:(): [PubMed PMID: 25905330]
Lam JR, Schneider JL, Zhao W, Corley DA. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 2013 Dec 11:310(22):2435-42. doi: 10.1001/jama.2013.280490. Epub [PubMed PMID: 24327038]
Level 2 (mid-level) evidenceLarsson R, Erlanson P, Bodemar G, Walan A, Bertler A, Fransson L, Norlander B. The pharmacokinetics of cimetidine and its sulphoxide metabolite in patients with normal and impaired renal function. British journal of clinical pharmacology. 1982 Feb:13(2):163-70 [PubMed PMID: 7059413]
Level 2 (mid-level) evidenceWu Y, Wu Y, Ji Y, Liu Y, Wu D, Liang J, Guo G, Chen B. Case Report: Oral Cimetidine Administration Causes Drug-Induced Immune Hemolytic Anemia by Eliciting the Production of Cimetidine-Dependent Antibodies and Drug-Independent Non-specific Antibodies. Frontiers in medicine. 2021:8():723167. doi: 10.3389/fmed.2021.723167. Epub 2021 Sep 24 [PubMed PMID: 34646843]
Level 3 (low-level) evidenceNidhiry AS, Puliyanda D, Blifeld C, Pizzo H. A rare case of hyperuricemia and acute kidney injury in a kidney transplant patient. Pediatric nephrology (Berlin, Germany). 2026 Feb:41(2):365-368. doi: 10.1007/s00467-025-06975-z. Epub 2025 Oct 13 [PubMed PMID: 41081896]
Level 3 (low-level) evidenceGibaldi M. Drug interactions: Part I. The Annals of pharmacotherapy. 1992 May:26(5):709-13 [PubMed PMID: 1591436]
Level 3 (low-level) evidenceO'Reilly RA. Comparative interaction of cimetidine and ranitidine with racemic warfarin in man. Archives of internal medicine. 1984 May:144(5):989-91 [PubMed PMID: 6324710]
Level 1 (high-level) evidenceWiggins BS, Saseen JJ, Page RL 2nd, Reed BN, Sneed K, Kostis JB, Lanfear D, Virani S, Morris PB, American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology; Council on Hypertension; Council on Quality of Care and Outcomes Research; and Council on Functional Genomics and Translational Biology. Recommendations for Management of Clinically Significant Drug-Drug Interactions With Statins and Select Agents Used in Patients With Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2016 Nov 22:134(21):e468-e495 [PubMed PMID: 27754879]
Level 2 (mid-level) evidenceFeely J, Wilkinson GR, Wood AJ. Reduction of liver blood flow and propranolol metabolism by cimetidine. The New England journal of medicine. 1981 Mar 19:304(12):692-5 [PubMed PMID: 7464861]
Schwinghammer TL. Drug interactions with cimetidine. American journal of hospital pharmacy. 1981 Dec:38(12):1976-8 [PubMed PMID: 7325185]
Martínez C, Albet C, Agúndez JA, Herrero E, Carrillo JA, Márquez M, Benítez J, Ortiz JA. Comparative in vitro and in vivo inhibition of cytochrome P450 CYP1A2, CYP2D6, and CYP3A by H2-receptor antagonists. Clinical pharmacology and therapeutics. 1999 Apr:65(4):369-76 [PubMed PMID: 10223772]
Level 1 (high-level) evidenceSalom IL, Silvis SE, Doscherholmen A. Effect of cimetidine on the absorption of vitamin B12. Scandinavian journal of gastroenterology. 1982 Jan:17(1):129-31 [PubMed PMID: 7134827]
Abel S, Nichols DJ, Brearley CJ, Eve MD. Effect of cimetidine and ranitidine on pharmacokinetics and pharmacodynamics of a single dose of dofetilide. British journal of clinical pharmacology. 2000 Jan:49(1):64-71 [PubMed PMID: 10606839]
Pratt VM, Scott SA, Pirmohamed M, Esquivel B, Kattman BL, Malheiro AJ, Kane M, Dean L. Eliglustat Therapy and CYP2D6 Genotype. MINI Medical Genetics Summaries. 2012:(): [PubMed PMID: 33351401]
Vinnakota RD, Brett AS. Iron Deficiency Anemia Associated With Acid-Modifying Medications: Two Cases and Literature Review. The American journal of the medical sciences. 2019 Feb:357(2):160-163. doi: 10.1016/j.amjms.2018.10.014. Epub 2018 Nov 1 [PubMed PMID: 30528320]
Level 3 (low-level) evidenceDelpre G, Kadish U, Livni E. Hepatitis following cimetidine administration. The American journal of the medical sciences. 1982 May-Jun:283(3):153-6 [PubMed PMID: 7081289]
Level 3 (low-level) evidenceKruss DM, Littman A. Safety of cimetidine. Gastroenterology. 1978 Feb:74(2 Pt 2):478-83 [PubMed PMID: 620916]
Matok I, Gorodischer R, Koren G, Sheiner E, Wiznitzer A, Uziel E, Levy A. The safety of H(2)-blockers use during pregnancy. Journal of clinical pharmacology. 2010 Jan:50(1):81-7. doi: 10.1177/0091270009350483. Epub 2009 Sep 29 [PubMed PMID: 19789371]
Level 2 (mid-level) evidenceSt Francis H, Renny MH, Biary R, Howland MA, Su MK. Clozapine Toxicity in Two Young Siblings Due to a Pharmacy Dispensing Error: a Pediatric Case Report. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2022 Oct:18(4):340-343. doi: 10.1007/s13181-022-00909-z. Epub 2022 Aug 26 [PubMed PMID: 36018467]
Level 3 (low-level) evidenceVallurupalli NG, Goldhaber SZ. Gastrointestinal complications of dual antiplatelet therapy. Circulation. 2006 Mar 28:113(12):e655-8 [PubMed PMID: 16567572]
Tawadrous D, Dixon S, Shariff SZ, Fleet J, Gandhi S, Jain AK, Weir MA, Gomes T, Garg AX. Altered mental status in older adults with histamine2-receptor antagonists: a population-based study. European journal of internal medicine. 2014 Oct:25(8):701-9. doi: 10.1016/j.ejim.2014.06.021. Epub 2014 Jul 16 [PubMed PMID: 25044092]
van der Hooft CS, Jong GW, Dieleman JP, Verhamme KM, van der Cammen TJ, Stricker BH, Sturkenboom MC. Inappropriate drug prescribing in older adults: the updated 2002 Beers criteria--a population-based cohort study. British journal of clinical pharmacology. 2005 Aug:60(2):137-44 [PubMed PMID: 16042666]
Level 2 (mid-level) evidenceWax PM, Kolian TM, Pizon AF. The Value of Medical Toxicologists. Journal of medical toxicology : official journal of the American College of Medical Toxicology. 2025 Jul:21(3):336-342. doi: 10.1007/s13181-025-01082-9. Epub 2025 Jun 19 [PubMed PMID: 40536638]
Costigan C, Comerford M, Whitmarsh R, Van Der Merwe K, Madders G, O'Connell J, Butler T, Molloy S, O'Hara F, Ryan B, Breslin N, O'Donnell S, O'Connor A, Smith S, Ismail S, Parihar V, McNamara D. Bismuth Quadruple Therapy with Doxycycline Is an Effective First-Line Therapy for Helicobacter pylori in an Irish Cohort. Antibiotics (Basel, Switzerland). 2025 Jul 28:14(8):. doi: 10.3390/antibiotics14080757. Epub 2025 Jul 28 [PubMed PMID: 40867952]
Ruigómez A, García Rodríguez LA, Cattaruzzi C, Troncon MG, Agostinis L, Wallander MA, Johansson S. Use of cimetidine, omeprazole, and ranitidine in pregnant women and pregnancy outcomes. American journal of epidemiology. 1999 Sep 1:150(5):476-81 [PubMed PMID: 10472947]
Level 2 (mid-level) evidenceMüller M, Jürgens J, Redaèlli M, Klingberg K, Hautz WE, Stock S. Impact of the communication and patient hand-off tool SBAR on patient safety: a systematic review. BMJ open. 2018 Aug 23:8(8):e022202. doi: 10.1136/bmjopen-2018-022202. Epub 2018 Aug 23 [PubMed PMID: 30139905]
Level 1 (high-level) evidence