 Liddle Syndrome (Pseudohyperaldosteronism)
Liddle Syndrome (Pseudohyperaldosteronism)
Introduction
Liddle syndrome is one of the rare causes of resistant hypertension that can present in early childhood, although some cases are not detected until adulthood. First described in 1963 by Grant Liddle et al, this syndrome is characterized by a primary increase in sodium reabsorption in the distal nephron leading to subsequent potassium secretion. For this reason, it is also known as pseudohyperaldosteronism.
The syndrome is a rare, monogenic, autosomal dominant cause of secondary hypertension resulting from a genetic gain-of-function mutation of the epithelial sodium channel (ENaC).[1] Affected patients typically present with hypertension, hypokalemia, and metabolic alkalosis. Although these findings are similar to those seen in other disorders caused by mineralocorticoid excess, Liddle syndrome does not respond to aldosterone antagonism (eg, spironolactone). The mainstay of treatment is with ENaC blockers, including amiloride.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Liddle syndrome is a congenital disorder typically caused by a single-gene mutation. Patients inherit the disorder in an autosomal dominant pattern with variable penetrance, and diverse populations are affected by the syndrome. Results from genetic studies have determined that this syndrome results from a gain-of-function mutation in the epithelial sodium channel in the distal nephron. In 1995, Hansson et al discovered the germline mutation in the SCNN1G gene as a cause of Liddle syndrome.[2]
Later, researchers showed that the ENaC comprises 3 homologous subunits, α-, β-, and γENaC, coded by SCNN1A, SCNN1B, and SCNN1G genes.[3] Mutations in α-, β-, or γENaC subunits lead to amplified activity of this channel, independent of aldosterone activity. While these are the well-described mutations associated with Liddle syndrome, a systematic review by GranhØj et al in 2024 listed 45 unique genetic variants across 86 families (40 of which were diagnostic).[4] New cases have been described in more recent literature, including the first described case of Liddle syndrome due to two separate mutations, each with possible synergistic effects on the other.[5][6][7]
Epidemiology
Researchers have not extensively studied the incidence of Liddle syndrome in the hypertensive population. However, Lin-Ping Wang et al and Liu et al have studied the prevalence of Liddle syndrome. They found that among younger Chinese individuals with unexplained resistant hypertension, the prevalence of Liddle syndrome was 1.52% and 1.72%, respectively.[1][8] In the first study by Lin-Ping Wang et al, only participants with hypokalemia underwent genetic testing.
Notably, Liddle syndrome can also present in patients with potassium levels within the reference range. Therefore, if future studies were to evaluate the prevalence of Liddle syndrome in patients with normal serum potassium levels and resistant hypertension, the rate would likely be higher.[9] Furthermore, no predisposition based on race or sex has been identified. Researchers in one study of veterans in Northwest Louisiana, United States, concluded that approximately 6% had biochemical profiles consistent with Liddle syndrome, an unusually high prevalence for a hypertensive population.[10] Liddle syndrome may exhibit heterogeneous distribution because the gene encoding the α subunit is polymorphic.[11]
Pathophysiology
ENaCs are present in the distal colon, ducts of exocrine glands, lungs, placenta, dendritic cells, and the apical surface of the distal nephron epithelium (see Figure. Down-Regulation of Mutation in the Epithelial Sodium Channel (ENaC) Expression via Mineralocorticoid Receptors and Ubiquitylation).[3][12][13] Patients with Liddle syndrome have abnormal ENaC function in distal nephrons due to genetic mutations in 1 of the 3 subunits. In most of these mutations, the degradation of the sodium channels is impaired; therefore, the number of these channels on the apical surface of the distal nephron increases inappropriately.[14] However, a minority of cases are due to an increased open-state probability of ENaC.[15]
Under normal conditions, the regulation of the ENaC is mediated through the binding of neural precursor cell expressed developmentally down-regulated 4-2 (Nedd4-2), a ubiquitin ligase, to the proline-rich PY motif of the ENaC subunit. This interaction ensures the subunit is tagged for degradation in a ubiquitination process. Aldosterone inhibits this process by inducing serum and glucocorticoid-regulated kinase 1 (SGK-1)–mediated phosphorylation of Nedd4-2, causing increased ENaC expression, leading to increased sodium reabsorption.
In most cases of Liddle syndrome, the PY motif is truncated and cannot be tagged for degradation. Therefore, an increase in apical density of ENaC at the cell surface leads to increased sodium absorption, extracellular volume expansion, and hypertension. This process is similar to the effects of aldosterone, giving rise to the term pseudohyperaldosteronism.[16]
The sodium feedback inhibition system is also impaired in patients with Liddle syndrome.[17] Typically, increased intracellular sodium in distal nephron cells inhibits apical epithelial sodium channels, but in Liddle syndrome, the channel becomes insensitive to sodium concentration. Increased numbers of sodium channels cause increased sodium reabsorption, which results in chronic volume retention, hypertension, and suppression of renin and aldosterone secretion.[18] Renal biopsies show atrophy of juxtaglomerular cells due to chronically suppressed renin and aldosterone levels, even after empirical treatment with triamterene.
Additionally, the increased influx of sodium through ENaCs causes several different effects on other channels within the membrane. First, increased sodium-potassium adenosine triphosphatase (Na+/K+, ATPase pump) activity at the basolateral membrane increases potassium influx into the cell from the basolateral side. Second, the depolarization of the cell's apical membrane secondary to sodium entry causes potassium secretion through apical potassium channels. As a result, potassium is excreted in the urine, causing hypokalemia and metabolic alkalosis.[19]
History and Physical
Patients with Liddle syndrome can be symptomatic or asymptomatic. The syndrome usually presents with early-onset, resistant hypertension between ages 11 to 31 due to excess sodium reabsorption in the distal nephron; however, it may take years or decades for clinicians to establish the final diagnosis. Hypertension due to Liddle syndrome is responsive to a sodium-restricted diet and may present with headache, dizziness, retinopathy, chronic kidney disease, left ventricular hypertrophy, or sudden death.[9] Because patients have resistant hypertension, hypokalemia, and ventricular hypertrophy, they can develop cardiac arrhythmias, potentially leading to sudden death. Significant hypokalemia can cause muscle weakness, polyuria, and polydipsia. Hypokalemia and metabolic alkalosis occur due to excessive potassium loss in the urine secondary to sodium reabsorption.[20][21]
The incidence of hypertension and hypokalemia in patients with Liddle syndrome is approximately 92.2% and 69.8%, respectively.[4] About 52.6% of patients with Liddle syndrome also present with hypoaldosteronism. Therefore, clinicians should also consider genetic testing for Liddle syndrome in patients who do not have the classic signs of hypertension or hypokalemia. The genetic testing is usually completed for these individuals due to a significant family history of the syndrome.
Evaluation
Patients with Liddle syndrome often present with secondary or resistant hypertension. Laboratory investigation may reveal hypokalemia and metabolic alkalosis.[22] Primary hyperaldosteronism can present with similar clinical features and biochemical abnormalities. Renin and aldosterone levels should be measured to differentiate between true hyperaldosteronism and pseudohyperaldosteronism. In patients with Liddle syndrome, renin and aldosterone levels are low or normal. Conversely, patients with hyperaldosteronism have elevated aldosterone levels. Spironolactone is ineffective for treating Liddle syndrome due to low or normal levels of aldosterone.[23]
Ultimately, the diagnosis is confirmed by the identification of an abnormal gene regulating the ENaC. Clinicians should consider genetic testing in young patients with hyporeninemic hypertension to allow for timely diagnosis and mitigation of complications. Notably, whole-exome sequencing may be considered when multiple mutated genes are a consideration.[7]
Treatment / Management
Low levels of aldosterone render spironolactone ineffective in patients with Liddle syndrome. The treatment of choice is amiloride, which directly inhibits the ENaC. Amiloride is prescribed daily at doses ranging from 5 to 20 mg. Amiloride is considered safe to use in pregnancy, and doses may need to be adjusted up to a maximum of 30 mg.[24] Triamterene, another potassium-sparing diuretic with a similar mechanism of action to amiloride, can also treat Liddle syndrome. A sodium-restricted diet has a synergistic effect with these medications.[25] However, excessive sodium accumulation on the receptor makes it unavailable for elimination by the medication.[26] If renal function is normal, then hyperkalemia is very rare. Avoidance of excessive potassium in the diet is suggested, along with the use of potassium-sparing diuretics.(B3)
If blood pressure is not controlled with potassium-sparing medications, other antihypertensive agents may be used to help achieve blood pressure targets and reduce cardiovascular risk. Caution is needed when using hydrochlorothiazide as a component of fixed-dose combination medications. Other classes of medications, such as β-blockers and vasodilators, could be very effective in controlling blood pressure.[26]
Differential Diagnosis
Low plasma renin levels with associated hypertension can be classified as follows:
- Low renin level with low aldosterone level
- Low renin level with aldosterone within the reference range
- Low renin level with elevated aldosterone level [27]
Liddle syndrome is classified under low renin level with low aldosterone level. Other causes of hypertension that are classified under low renin level with low aldosterone level are as follows:
- Apparent mineralocorticoid excess
- 11β-hydroxyl deficiency
- 17α-hydroxyl deficiency
- Gordon syndrome
- Mineralocorticoid receptor-activating mutation
- Glucocorticoid resistance
- Ectopic adrenocorticotropic hormone production
- Excessive licorice use [28]
Mineralocorticoid excess is an autosomal recessive syndrome due to 11β-hydroxysteroid dehydrogenase type 2 enzyme deficiency. This enzyme converts cortisol (active) into cortisone (inactive), which cannot bind to the mineralocorticoid receptor.[29] The chronic consumption of licorice, which contains glycyrrhizic acid, also inhibits this enzyme and presents with similar effects.[30] Gordon syndrome is an autosomal dominant condition caused by a mutation in a gene responsible for ion transport in the kidney, increasing sodium reabsorption and decreasing potassium excretion.[31]
Prognosis
Patients with Liddle syndrome typically respond well to medical therapy with potassium-sparing diuretics. However, results from current studies have not adequately evaluated the long-term mortality of Liddle syndrome. Clinicians often undertreat and misdiagnose this syndrome, and further studies are needed to better define the morbidity and mortality of secondary hypertension. Prognosis may also depend on healthcare access, as described in a reported case of a patient who lacked access to ENaC blockers and exhibited a limited therapeutic response to alternative therapies.[32]
Complications
Because of resistant hypertension, patients may develop end-organ damage, including myocardial infarction, transient ischemic attack or cerebrovascular accident, pulmonary edema, congestive heart failure, and left ventricular hypertrophy.[33] Earlier diagnosis and appropriate treatment can delay or prevent end-organ damage.
Consultations
Specialist consultations include nephrology, pediatrics, endocrinology, and cardiology with a subspecialization in hypertension.
Deterrence and Patient Education
Patients should be counseled about the risks associated with resistant hypertension and educated about the importance of treatment adherence to minimize the risk of myocardial infarction and stroke. Therefore, they should be advised to maintain regular follow-up with their clinicians. Moreover, clinicians should emphasize the importance of a low-sodium and high-potassium diet, consistent medication use, and adequate blood pressure control.
Enhancing Healthcare Team Outcomes
Missed or delayed diagnosis of Liddle syndrome can lead to adverse clinical outcomes; therefore, early diagnosis is essential. Coordination between general pediatricians and pediatric nephrologists is necessary to ensure timely diagnosis and management. Genetic testing should be offered to family members of affected individuals. Genetic testing is available through the Genetic Testing Registry, and the geneticists can sequence exon 13 of the SCNN1B and SCNN1G genes to confirm the diagnosis.
Media
(Click Image to Enlarge)
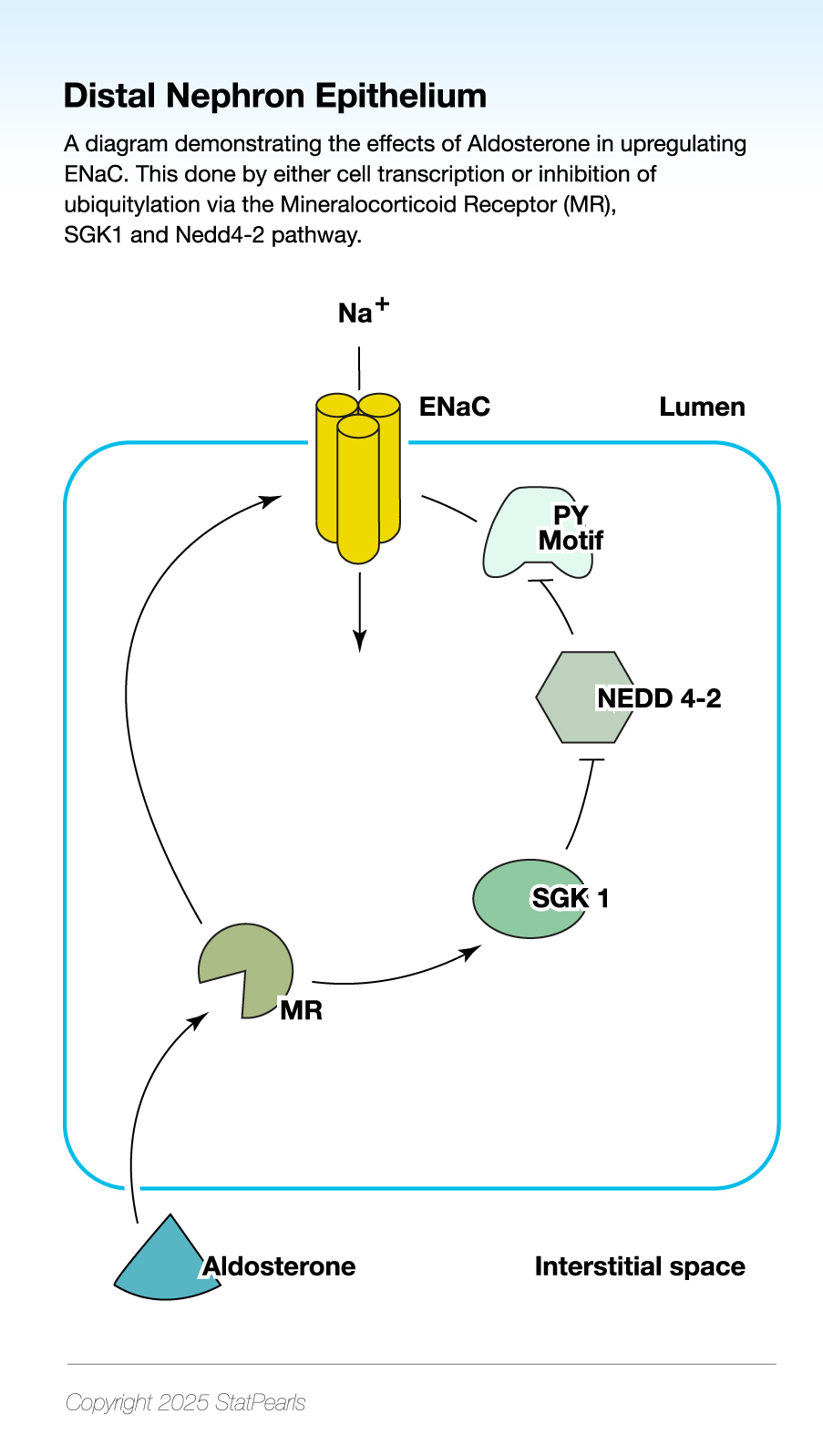
Down-Regulation of Mutation in the Epithelial Sodium Channel (ENaC) Expression via Mineralocorticoid Receptors and Ubiquitylation. The diagram demonstrates the effects of Aldosterone in upregulating ENaC. This is done through cell transcription or the inhibition of ubiquitylation via the mineralocorticoid receptor, serum and glucocorticoid-regulated kinase 1, and neural precursor cell expressed developmentally downregulated protein 4-2.
Illustrated by K Humphreys
References
Wang LP, Yang KQ, Jiang XJ, Wu HY, Zhang HM, Zou YB, Song L, Bian J, Hui RT, Liu YX, Zhou XL. Prevalence of Liddle Syndrome Among Young Hypertension Patients of Undetermined Cause in a Chinese Population. Journal of clinical hypertension (Greenwich, Conn.). 2015 Nov:17(11):902-7. doi: 10.1111/jch.12598. Epub 2015 Jun 15 [PubMed PMID: 26075967]
Hansson JH, Nelson-Williams C, Suzuki H, Schild L, Shimkets R, Lu Y, Canessa C, Iwasaki T, Rossier B, Lifton RP. Hypertension caused by a truncated epithelial sodium channel gamma subunit: genetic heterogeneity of Liddle syndrome. Nature genetics. 1995 Sep:11(1):76-82 [PubMed PMID: 7550319]
Level 3 (low-level) evidenceHanukoglu I, Hanukoglu A. Epithelial sodium channel (ENaC) family: Phylogeny, structure-function, tissue distribution, and associated inherited diseases. Gene. 2016 Apr 1:579(2):95-132. doi: 10.1016/j.gene.2015.12.061. Epub 2016 Jan 7 [PubMed PMID: 26772908]
Granhøj J, Nøhr TK, Hinrichs GR, Rasmussen M, Svenningsen P. Reverse Phenotypes of Patients with Genetically Confirmed Liddle Syndrome. Clinical journal of the American Society of Nephrology : CJASN. 2024 May 1:19(5):610-619. doi: 10.2215/CJN.0000000000000430. Epub 2024 Jan 24 [PubMed PMID: 38265765]
Lu Y, Liu X, Sun L, Zhang D, Fan P, Yang K, Zhang L, Liu Y, Zhou X. A frameshift mutation in the SCNN1B gene in a family with Liddle syndrome: A case report and systematic review. Molecular medicine reports. 2024 Feb:29(2):. pii: 19. doi: 10.3892/mmr.2023.13142. Epub 2023 Dec 15 [PubMed PMID: 38099339]
Level 1 (high-level) evidenceTang Q, Zhou Y, Liu L, Chen M, Liu L, Wang Y, Zhou G, Xie M. Liddle syndrome with a SCNN1B mutation: a case report and systematic review. BMC nephrology. 2025 Jul 21:26(1):408. doi: 10.1186/s12882-025-04252-7. Epub 2025 Jul 21 [PubMed PMID: 40696293]
Level 1 (high-level) evidenceSteyn N, Chale-Matsau B, Abera AB, van Biljon G, Pillay TS. Neonatal presentation of a patient with Liddle syndrome, South Africa. African journal of laboratory medicine. 2023:12(1):1998. doi: 10.4102/ajlm.v12i1.1998. Epub 2023 Apr 14 [PubMed PMID: 37151815]
Liu K, Qin F, Sun X, Zhang Y, Wang J, Wu Y, Ma W, Wang W, Wu X, Qin Y, Zhang H, Zhou X, Wu H, Hui R, Zou Y, Jiang X, Song L. Analysis of the genes involved in Mendelian forms of low-renin hypertension in Chinese early-onset hypertensive patients. Journal of hypertension. 2018 Mar:36(3):502-509. doi: 10.1097/HJH.0000000000001556. Epub [PubMed PMID: 28915228]
Level 2 (mid-level) evidencePagani L, Diekmann Y, Sazzini M, De Fanti S, Rondinelli M, Farnetti E, Casali B, Caretto A, Novara F, Zuffardi O, Garagnani P, Mantero F, Thomas MG, Luiselli D, Rossi E. Three Reportedly Unrelated Families With Liddle Syndrome Inherited From a Common Ancestor. Hypertension (Dallas, Tex. : 1979). 2018 Feb:71(2):273-279. doi: 10.1161/HYPERTENSIONAHA.117.10491. Epub 2017 Dec 11 [PubMed PMID: 29229744]
Tapolyai M, Uysal A, Dossabhoy NR, Zsom L, Szarvas T, Lengvárszky Z, Fülöp T. High prevalence of liddle syndrome phenotype among hypertensive US Veterans in Northwest Louisiana. Journal of clinical hypertension (Greenwich, Conn.). 2010 Nov:12(11):856-60. doi: 10.1111/j.1751-7176.2010.00359.x. Epub 2010 Aug 20 [PubMed PMID: 21054772]
Level 2 (mid-level) evidenceSugiyama T, Kato N, Ishinaga Y, Yamori Y, Yazaki Y. Evaluation of selected polymorphisms of the Mendelian hypertensive disease genes in the Japanese population. Hypertension research : official journal of the Japanese Society of Hypertension. 2001 Sep:24(5):515-21 [PubMed PMID: 11675945]
Canessa CM, Schild L, Buell G, Thorens B, Gautschi I, Horisberger JD, Rossier BC. Amiloride-sensitive epithelial Na+ channel is made of three homologous subunits. Nature. 1994 Feb 3:367(6462):463-7 [PubMed PMID: 8107805]
Level 3 (low-level) evidenceVan Beusecum JP, Barbaro NR, McDowell Z, Aden LA, Xiao L, Pandey AK, Itani HA, Himmel LE, Harrison DG, Kirabo A. High Salt Activates CD11c(+) Antigen-Presenting Cells via SGK (Serum Glucocorticoid Kinase) 1 to Promote Renal Inflammation and Salt-Sensitive Hypertension. Hypertension (Dallas, Tex. : 1979). 2019 Sep:74(3):555-563. doi: 10.1161/HYPERTENSIONAHA.119.12761. Epub 2019 Jul 8 [PubMed PMID: 31280647]
Lu C, Pribanic S, Debonneville A, Jiang C, Rotin D. The PY motif of ENaC, mutated in Liddle syndrome, regulates channel internalization, sorting and mobilization from subapical pool. Traffic (Copenhagen, Denmark). 2007 Sep:8(9):1246-64 [PubMed PMID: 17605762]
Level 3 (low-level) evidenceSalih M, Gautschi I, van Bemmelen MX, Di Benedetto M, Brooks AS, Lugtenberg D, Schild L, Hoorn EJ. A Missense Mutation in the Extracellular Domain of αENaC Causes Liddle Syndrome. Journal of the American Society of Nephrology : JASN. 2017 Nov:28(11):3291-3299. doi: 10.1681/ASN.2016111163. Epub 2017 Jul 14 [PubMed PMID: 28710092]
Enslow BT, Stockand JD, Berman JM. Liddle's syndrome mechanisms, diagnosis and management. Integrated blood pressure control. 2019:12():13-22. doi: 10.2147/IBPC.S188869. Epub 2019 Sep 3 [PubMed PMID: 31564964]
Kellenberger S, Gautschi I, Rossier BC, Schild L. Mutations causing Liddle syndrome reduce sodium-dependent downregulation of the epithelial sodium channel in the Xenopus oocyte expression system. The Journal of clinical investigation. 1998 Jun 15:101(12):2741-50 [PubMed PMID: 9637708]
Level 3 (low-level) evidenceNakada T, Koike H, Akiya T, Katayama T, Kawamata S, Takaya K, Shigematsu H. Liddle's syndrome, an uncommon form of hyporeninemic hypoaldosteronism: functional and histopathological studies. The Journal of urology. 1987 Apr:137(4):636-40 [PubMed PMID: 3550146]
Level 3 (low-level) evidenceBubien JK. Epithelial Na+ channel (ENaC), hormones, and hypertension. The Journal of biological chemistry. 2010 Jul 30:285(31):23527-31. doi: 10.1074/jbc.R109.025049. Epub 2010 May 11 [PubMed PMID: 20460373]
Level 3 (low-level) evidenceUnwin RJ, Luft FC, Shirley DG. Pathophysiology and management of hypokalemia: a clinical perspective. Nature reviews. Nephrology. 2011 Feb:7(2):75-84. doi: 10.1038/nrneph.2010.175. Epub [PubMed PMID: 21278718]
Level 3 (low-level) evidenceAmlal H, Krane CM, Chen Q, Soleimani M. Early polyuria and urinary concentrating defect in potassium deprivation. American journal of physiology. Renal physiology. 2000 Oct:279(4):F655-63 [PubMed PMID: 10997915]
Level 3 (low-level) evidenceMonticone S, Buffolo F, Tetti M, Veglio F, Pasini B, Mulatero P. GENETICS IN ENDOCRINOLOGY: The expanding genetic horizon of primary aldosteronism. European journal of endocrinology. 2018 Mar:178(3):R101-R111. doi: 10.1530/EJE-17-0946. Epub 2018 Jan 18 [PubMed PMID: 29348113]
Baudrand R, Vaidya A. The Low-Renin Hypertension Phenotype: Genetics and the Role of the Mineralocorticoid Receptor. International journal of molecular sciences. 2018 Feb 11:19(2):. doi: 10.3390/ijms19020546. Epub 2018 Feb 11 [PubMed PMID: 29439489]
Awadalla M, Patwardhan M, Alsamsam A, Imran N. Management of Liddle Syndrome in Pregnancy: A Case Report and Literature Review. Case reports in obstetrics and gynecology. 2017:2017():6279460. doi: 10.1155/2017/6279460. Epub 2017 Mar 15 [PubMed PMID: 28396810]
Level 3 (low-level) evidenceYang KQ, Lu CX, Fan P, Zhang Y, Meng X, Dong XQ, Luo F, Liu YX, Zhang HM, Wu HY, Cai J, Zhang X, Zhou XL. Genetic screening of SCNN1B and SCNN1G genes in early-onset hypertensive patients helps to identify Liddle syndrome. Clinical and experimental hypertension (New York, N.Y. : 1993). 2018:40(2):107-111. doi: 10.1080/10641963.2017.1334799. Epub 2017 Jul 18 [PubMed PMID: 28718682]
Warnock DG. Liddle syndrome: an autosomal dominant form of human hypertension. Kidney international. 1998 Jan:53(1):18-24 [PubMed PMID: 9452995]
Mulatero P, Verhovez A, Morello F, Veglio F. Diagnosis and treatment of low-renin hypertension. Clinical endocrinology. 2007 Sep:67(3):324-34 [PubMed PMID: 17573898]
Penninkilampi R, Eslick EM, Eslick GD. The association between consistent licorice ingestion, hypertension and hypokalaemia: a systematic review and meta-analysis. Journal of human hypertension. 2017 Nov:31(11):699-707. doi: 10.1038/jhh.2017.45. Epub 2017 Jun 29 [PubMed PMID: 28660884]
Level 1 (high-level) evidenceWilson RC, Nimkarn S, New MI. Apparent mineralocorticoid excess. Trends in endocrinology and metabolism: TEM. 2001 Apr:12(3):104-11 [PubMed PMID: 11306334]
Awad N, Makar G, Burroughs V, Ravi P, Burroughs SR. Licorice-induced apparent mineralocorticoid excess causing persistent hypertension and hypokalemia. Acta endocrinologica (Bucharest, Romania : 2005). 2020 Oct-Dec:16(4):508-510. doi: 10.4183/aeb.2020.508. Epub [PubMed PMID: 34084245]
Kahle KT, Wilson FH, Lifton RP. Regulation of diverse ion transport pathways by WNK4 kinase: a novel molecular switch. Trends in endocrinology and metabolism: TEM. 2005 Apr:16(3):98-103 [PubMed PMID: 15808806]
Level 3 (low-level) evidencePrabowo NA, Putranto W, Myrtha R, Ardyanto TD, Gautama CS, Wulandari EL, Hermawati BD, Putri DP, Ramadhani A, Dewi HK. Challenges in diagnosing and treating Liddle syndrome in resource-limited settings: A case report from Indonesia. Narra J. 2024 Dec:4(3):e1000. doi: 10.52225/narra.v4i3.1000. Epub 2024 Oct 25 [PubMed PMID: 39816126]
Level 3 (low-level) evidenceGohri J, Bakhle R, Calhoun AE, Sajja A, Bhatt KN. Heart Transplantation in a Patient With Liddle Syndrome. JACC. Case reports. 2025 Mar 5:30(5):103079. doi: 10.1016/j.jaccas.2024.103079. Epub [PubMed PMID: 40054894]
Level 3 (low-level) evidence