Introduction
Oral anticoagulants are foundational therapies for the prevention and treatment of thromboembolic disease, but their effectiveness depends on safe prescribing, careful patient selection, and prompt recognition of bleeding and treatment failure. Direct oral anticoagulants (DOACs) have replaced warfarin in many patients with atrial fibrillation and venous thromboembolism because they have comparable efficacy and fewer drug-drug interactions, although important safety limitations remain in selected clinical settings. See StatPearls' companion reference, "Anticoagulation Therapy," for additional information. Anticoagulation safety requires continuous reassessment of net clinical benefit rather than a binary choice between thrombosis prevention and bleeding avoidance. The most useful modern approach is practical and risk-based: confirm the indication, identify bleeding modifiers, choose the right agent and dose, anticipate procedures, understand reversal options, and reassess whether an apparent drug complication reflects true pharmacologic failure or a correctable prescribing or adherence problem.[1]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The etiology of anticoagulation-related complications is multifactorial and reflects interactions among drug pharmacology, patient comorbidities, concurrent medications, and systems-level factors that affect prescribing, monitoring, and follow-up. Complications generally result from either excess anticoagulant effect, which increases bleeding risk, or insufficient anticoagulation, which predisposes patients to recurrent thrombosis, stroke, or thromboembolism.[1][2]
Major contributors to anticoagulant-related complications include the following:
Drug-Specific Factors
Warfarin is affected by dietary vitamin K intake, hepatic metabolism, and genetic variation in cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase complex subunit 1 (VKORC1) genes. See StatPearls’ companion reference, "Warfarin Drug Interactions," for more in-depth discussion of drug-drug interactions. DOAC exposure is influenced by renal clearance, hepatic metabolism, and transporter-mediated effects such as P-glycoprotein activity. Clinically important drug interactions with DOACs are driven mainly by effects on P-glycoprotein and the CYP3A4 enzyme, as well as by additive impairment of hemostasis from other antithrombotic agents. Because DOAC plasma concentrations correlate with both bleeding and thrombotic outcomes, unrecognized interactions that increase or decrease drug levels can alter risk.
Drugs that increase DOAC levels and increase bleeding risk:
- Strong dual P-glycoprotein and CYP3A4 inhibitors: Azole antifungals (ketoconazole, itraconazole), HIV protease inhibitors, and some hepatitis C antivirals can markedly increase apixaban and rivaroxaban concentrations; these combinations are generally avoided or require dose reduction and close monitoring.
- Potent P-glycoprotein inhibitors affecting dabigatran and edoxaban: Dronedarone, verapamil (especially immediate-release given near the DOAC dose), amiodarone, and certain macrolides increase dabigatran or edoxaban exposure; label-based dose reduction or avoidance is recommended in patients with renal impairment.
- Antiplatelet agents and nonsteroidal anti-inflammatory drugs: Aspirin, purinergic P2Y12 receptor inhibitors, and nonsteroidal anti-inflammatory drugs increase bleeding risk with all DOACs via a pharmacodynamic interaction, even when pharmacokinetics are unchanged.[3][4]
Drugs that decrease DOAC levels and increase thrombosis risk:
- Strong CYP3A4 and P-glycoprotein inducers, including rifampin, carbamazepine, phenytoin, phenobarbital, primidone, and St. John’s Wort, can significantly lower DOAC concentrations and should usually be avoided.
- Some antiepileptics, including valproate and possibly levetiracetam, may reduce DOAC exposure through less well-defined mechanisms and warrant cautious use and specialist input.[3]
Patient-Related Risk Factors
Advanced age, frailty, chronic kidney disease, liver disease, thrombocytopenia, active cancer, prior bleeding, and uncontrolled hypertension increase the risk of hemorrhagic complications regardless of the anticoagulant used.[5][6]
Structural and Disease-Specific Conditions
Cerebral amyloid angiopathy, peptic ulcer disease, vascular malformations, and other lesions that impair vascular integrity increase the likelihood of major or site-specific bleeding, particularly intracranial or gastrointestinal tract hemorrhage.[7]
Adherence and Dosing Problems
Missed doses, inappropriate dose reduction, duplicate therapy, premature discontinuation, and poor follow-up can lead to recurrent venous thromboembolism, cardioembolic stroke, or apparent anticoagulant failure.[8][9]
Systems-Level Contributors
Inadequate medication reconciliation, failure to monitor renal function, inconsistent periprocedural planning, fragmented communication, and insufficient patient education frequently contribute to preventable anticoagulant-related harm.[10][11] Overall, anticoagulation complications arise not only from the anticoagulant itself but also from patient-related factors, the burden of interactions, and gaps in coordinated care.
Epidemiology
Given their efficacy and more favorable safety profile, DOACs have become the preferred choice over vitamin K antagonists for stroke prevention in atrial fibrillation and venous thromboembolism, 2 of the most common reasons for long-term anticoagulation. The 2023 American College of Cardiology, American Heart Association, American College of Clinical Pharmacy, and Heart Rhythm Society Guideline recommends DOACs as first-line therapy over warfarin for patients with atrial fibrillation, except in those with moderate-to-severe mitral stenosis or mechanical heart valves. The risk of bleeding-related complications is highest within the first 3 to 6 months of therapy.[12][13][14]
Bleeding Risk: DOACs Versus Warfarin
DOACs are associated with a lower overall risk of major bleeding, primarily driven by a consistent approximately 50% reduction in intracranial hemorrhage compared with warfarin. The annual risk of intracranial hemorrhage with DOACs is low, approximately 0.2% to 0.4%, but remains clinically significant given the high mortality associated with anticoagulant-related intracerebral hemorrhage.[15] In venous thromboembolism, major bleeding rates are lower with DOACs than with warfarin during both initial and extended treatment, with apixaban demonstrating the lowest rates among available agents.[16]
However, gastrointestinal tract bleeding risk is agent-specific and more variable. Rivaroxaban and higher-dose dabigatran and edoxaban are associated with higher rates of gastrointestinal tract bleeding compared with warfarin, whereas apixaban consistently shows a more favorable gastrointestinal safety profile, with lower bleeding risk across large observational cohorts and real-world datasets.[17] Bleeding risk increases with age and comorbidity burden. Key risk factors for anticoagulant-related bleeding include advanced age, hypertension, prior stroke, concomitant antiplatelet use, cerebral amyloid angiopathy, and renal dysfunction. Although the relative safety advantage of DOACs may diminish in older patients, they continue to offer significant reductions in intracranial hemorrhage and comparable or improved overall outcomes compared with warfarin.
In frail older adult populations, DOACs, particularly apixaban, demonstrate favorable efficacy and safety, with reduced stroke, intracranial bleeding, and mortality. However, the risk of gastrointestinal tract bleeding may remain elevated in certain subgroups, highlighting the need for individualized anticoagulant selection.[18][19] In summary, DOACs provide a more favorable bleeding profile than warfarin, though differences between agents and patient-specific risk factors should guide clinical decision-making.
Pathophysiology
Anticoagulant-related complications reflect disruption of the tightly regulated hemostatic balance among endothelium, platelets, coagulation factors, and fibrinolysis. These agents reduce thrombin generation or activity to prevent thrombosis, but complications arise when inhibition is excessive, misapplied, or occurs in patients with underlying vulnerabilities. Vitamin K antagonists, including warfarin, inhibit the synthesis of clotting factors II, VII, IX, and X, as well as proteins C and S. The early decline in protein C levels creates a transient prothrombotic state, necessitating bridging therapy in acute thrombosis. At steady state, excessive anticoagulation reduces multiple clotting factors, impairing fibrin formation and predisposing to major bleeding, including intracranial and gastrointestinal tract hemorrhage.
Direct oral anticoagulants target specific steps in the coagulation cascade. Direct thrombin inhibitors, including dabigatran, block factor IIa, while factor Xa inhibitors, including apixaban, rivaroxaban, and edoxaban, reduce thrombin generation. Although pharmacokinetically predictable, excess exposure, including from renal dysfunction or drug interactions, similarly impairs stable clot formation and increases bleeding risk. Bleeding risk depends not only on the intensity of anticoagulation but also on local vascular pathology. Conditions such as hypertension and cerebral amyloid angiopathy predispose patients to intracranial hemorrhage, while gastrointestinal tract lesions, including ulcers, angiodysplasia, and cancer, increase the risk of overt bleeding. Confined spaces, including the spinal canal, amplify the clinical impact of even small hematomas.
Nonhemorrhagic complications include anticoagulant-related nephropathy, which involves glomerular hemorrhage with tubular obstruction by red blood cell casts; cholesterol crystal embolization from dissolution of protective thrombus overlying ulcerated aortic plaques; and complications specific to vitamin K antagonists, including accelerated vascular calcification, intraplaque hemorrhage promoting plaque vulnerability, warfarin-induced skin necrosis, and purple toe syndrome.[20][21] Conversely, inadequate anticoagulation permits thrombin propagation, resulting in recurrent venous thromboembolism, cardioembolic stroke, or prosthetic valve thrombosis. Overall, complications arise from an imbalance between coagulation inhibition and patient-specific structural and systemic risk factors, determining whether bleeding or thrombosis predominates.
History and Physical
The history should first determine why the patient is taking anticoagulation, which agent is being used, and whether the current problem suggests bleeding, thrombosis, or both. Important historical details include the specific anticoagulant, dose, time of the last dose, recent dose changes, missed doses, recent procedures, trauma, falls, and prior bleeding or thromboembolic events. A careful medication review should identify antiplatelet agents, nonsteroidal anti-inflammatory drugs, herbal products, and drugs that alter warfarin or DOAC levels.[22] Symptoms of bleeding may be overt or subtle. Patients should be asked about epistaxis, gingival bleeding, easy bruising, hematuria, melena, hematemesis, heavy menstrual bleeding, back or flank pain, dyspnea, and new severe headache or neurologic symptoms. The history should also assess renal disease, liver disease, thrombocytopenia, cancer, alcohol use, and adherence problems because these factors may increase either bleeding risk or treatment failure.
The physical examination should focus on hemodynamic stability, the source of bleeding, and signs of thrombosis or neurologic compromise. Vital signs may show hypotension, tachycardia, tachypnea, or hypoxia in patients with significant blood loss or thromboembolic complications. General inspection may reveal pallor, diaphoresis, ecchymoses, petechiae, or expanding hematomas. A focused neurologic examination is essential in any patient with headache, confusion, weakness, sensory change, or back pain because anticoagulation increases the risk of intracranial and spinal epidural hemorrhage. Cardiopulmonary examination may identify signs of tamponade, hemothorax, pulmonary embolism, or hypovolemia, while abdominal and rectal examination may reveal tenderness, distension, occult gastrointestinal tract bleeding, or retroperitoneal hemorrhage. The extremities should be assessed for swelling, asymmetry, compartment firmness, pain with passive stretch, pulse deficits, or unilateral tenderness, which may suggest deep venous thrombosis, extremity ischemia, or compartment syndrome.
Certain findings may point to anticoagulant-specific complications. Skin necrosis associated with vitamin K antagonists presents with petechiae that progress to ecchymoses and hemorrhagic bullae, culminating in necrosis and slow-healing eschar formation. Patients with anticoagulant-related nephropathy may present with hypertension, hematuria, signs of volume overload, and reduced urine output.[23] Livedo reticularis, gangrene, cyanosis, skin ulcers, purpura or petechiae, and firm, painful erythematous nodules are the most common clinical findings associated with cholesterol crystal emboli. Acute kidney injury is a common finding. Gastrointestinal tract emboli cause abdominal pain, diarrhea, and occasionally bleeding. Central nervous system emboli may cause amaurosis fugax, transient ischemic attack, stroke, a confusional state, headache, and dizziness.
Evaluation
DOACs are now the preferred oral anticoagulants for many patients with atrial fibrillation and venous thromboembolism, given their ease of use and lower risk of intracranial bleeding compared with warfarin.[12][24] However, safe prescribing requires clearly differentiating absolute or near-absolute contraindications, situations where DOACs are not preferred, and cases of apparent treatment failure, which often reflect modifiable clinical factors rather than true drug inefficacy (see Table 1). Even in the absence of formal contraindications, warfarin or low-molecular-weight heparin (LMWH) may be more appropriate in selected clinical scenarios.[25]
Absolute Contraindications to DOACs
- Mechanical heart valves: The RE-ALIGN trial demonstrated increased thromboembolic and bleeding complications with dabigatran compared with warfarin.[26] The safety of factor Xa inhibitors has not been established in this population; therefore, warfarin remains the only recommended oral anticoagulant.[25]
- Thrombotic antiphospholipid syndrome: A meta-analysis of randomized trials showed a significantly higher risk of arterial thrombotic events with DOACs compared with vitamin K antagonists, primarily driven by increased stroke risk. This finding was consistent across patient subgroups. Vitamin K antagonists are the preferred therapy.[27]
- Moderate to severe rheumatic mitral stenosis: Patients with rheumatic mitral valve disease were excluded from pivotal DOAC trials, and current guidelines recommend warfarin as the anticoagulant of choice.[12]
- Pregnancy and breastfeeding: DOACs cross the placenta and are detectable in breast milk. Available data suggest increased risks of miscarriage and fetal anomalies. LMWH is preferred during pregnancy, while warfarin or LMWH may be used during breastfeeding.[28]
Strong Caution: Warfarin Generally Preferred
- Postbariatric surgery: Altered gastrointestinal tract anatomy can significantly impair DOAC absorption, with studies showing subtherapeutic drug levels in a substantial proportion of patients. Warfarin is often preferred because international normalized ratio (INR) monitoring ensures therapeutic anticoagulation. In the immediate postoperative setting, parenteral anticoagulation with LMWH or fondaparinux is recommended, particularly after highly malabsorptive procedures.[29]
- Severe chronic kidney disease (creatinine clearance <30 mL/min) or dialysis: Patients with advanced renal dysfunction were largely excluded from DOAC trials. Dabigatran is contraindicated in patients with creatinine clearance less than 30 mL/min, and edoxaban is not recommended for patients on dialysis. Although apixaban is labeled for use in end-stage renal disease, the evidence is primarily observational. Anticoagulation decisions in this population should involve shared decision-making.[25]
- Significant drug interactions: Strong CYP3A4 and P-glycoprotein inducers, such as carbamazepine and phenytoin, can reduce DOAC efficacy and increase thrombotic risk, whereas inhibitors can increase bleeding risk. When such interactions cannot be avoided, warfarin is generally preferred because its effect is monitorable.[25]
Use With Caution: Individualized Assessment Required
- Liver disease: DOACs may be used in mild to moderate hepatic impairment (Child-Pugh score A to B), with a lower bleeding risk than warfarin. However, rivaroxaban should be avoided in those with a Child-Pugh score B because of increased drug exposure, and all DOACs are generally contraindicated in Child-Pugh score C, in which warfarin remains the only option.[30]
- Class 3 obesity (body mass index ≥40 kg/m²): Current evidence supports the use of DOACs, particularly apixaban and rivaroxaban, at standard doses regardless of body weight. However, dabigatran and edoxaban should be avoided due to limited supporting data.[25][31]
- Low body weight (≤60 kg): DOACs remain effective and safe when used with appropriate dose adjustments. Edoxaban requires dose reduction in this population, and adherence to labeling recommendations is essential for optimal outcomes.[32][33][34]
- Thrombosis at unusual sites: Evidence for DOAC use in unusual-site thrombosis is evolving and largely observational. DOACs are increasingly used for cerebral venous sinus thrombosis, splanchnic vein thrombosis, left ventricular thrombus, and upper-extremity deep vein thrombosis, with generally favorable safety and efficacy profiles. However, for rarer sites such as ovarian, renal, and retinal vein thrombosis, evidence remains limited, and treatment decisions should be individualized in consultation with specialists.[35][36][37]
Table 1. Anticoagulant Selection for Atrial Fibrillation and Venous Thromboembolism
| Population | Preferred strategy | Safety rationale | Practical caveat | References |
| CKD Stage 3 (CrCl 30–59 mL/min) | DOACs are preferred over warfarin at evidence-based doses | Lower ICH risk and retained efficacy in pivotal trial subgroups | Renal function must be monitored periodically; use label-specified dose adjustments | [12][38] |
| CKD Stage 4 (CrCl 15–30 mL/min) | Warfarin or labeled-dose DOACs are reasonable (Class 2a) | Limited trial data; apixaban subgroup from ARISTOTLE trial showed numerically fewer strokes and bleeds vs warfarin | Closer renal monitoring required; shared decision-making recommended | [12][38] |
| Dialysis or CrCl <15 mL/min | Warfarin (INR 2.0–3.0) or apixaban (2.5 mg twice daily) may be reasonable (Class 2b) | Evidence is limited and conflicting; VKA control is often poor in ESKD; apixaban 2.5 mg twice daily approximates normal-function drug levels | Shared decision-making is essential; specialist input is recommended; other DOACs are generally contraindicated | [12][39] |
| Frail older adults on VKA | Decision to switch should be individualized, not reflexive | FRAIL-AF trial showed more bleeding after switching (hazard ratio 1.69); however, COMBINE-AF found similar net clinical outcomes and reductions in stroke, fatal intracranial bleeding with standard-dose DOACs | Apixaban may be the safest DOAC in frail patients; reassess if TTR is poor, adherence is poor, or drug interactions are unmanageable; GI bleeding risk increases with switch | [19][40][19] |
| Pregnancy-associated VTE | LMWH (adjusted-dose) | Best-supported maternal–fetal safety profile; DOACs and warfarin cross the placenta | DOACs and warfarin (>5 mg/day) are contraindicated in pregnancy; warfarin is acceptable postpartum | [28][41] |
| Cancer-associated thrombosis with luminal GI/GU lesion | LMWH or apixaban is preferred over edoxaban/rivaroxaban | Edoxaban and rivaroxaban are associated with increased GI bleeding in GI cancers; apixaban did not show this excess risk (CARAVAGGIO) | Balance oral convenience against tumor-site bleeding risk; check drug–drug interactions with cancer therapies | [42][43] |
| Class 3 obesity (BMI ≥40 kg/m²) | DOACs are reasonable over warfarin (Class 2a per ACC/AHA) | Post hoc analyses and large observational data show comparable or better efficacy/safety vs warfarin across weight groups | Evidence is less clear than in normal-weight populations; consider DOAC level monitoring if available | [12][44] |
| Postbariatric surgery | Warfarin may be reasonable over DOACs (Class 2b per ACC/AHA) | ~42% of patients postbariatric surgery had subtherapeutic peak DOAC levels in a meta-analysis; drug absorption is unpredictable | Warfarin's therapeutic effect is routinely monitorable; if DOAC is used, consider drug-level monitoring; apixaban absorption may be less affected than other DOACs | [25][29] |
| Mechanical valve prosthesis | Warfarin | DOACs failed to show noninferiority (RE-ALIGN trial with dabigatran showed increased thromboembolic and bleeding events) | Requires robust INR monitoring infrastructure; INR target depends on valve type and position | [26][45] |
| Antiphospholipid antibody syndrome | Warfarin | DOACs (rivaroxaban) are associated with increased arterial thrombotic events in RCTs, especially in triple-positive antibody APS | Requires robust INR infrastructure; DOACs should be avoided, particularly in triple-positive APS and arterial thrombosis | [46] |
Abbreviations: ACC/AHA, American College of Cardiology/American Heart Association; AF, atrial fibrillation; APS, antiphospholipid syndrome; BMI, body mass index; CKD, chronic kidney disease; CrCl, creatinine clearance; DOAC, direct oral anticoagulant; ESKD, end-stage kidney disease; GI, gastrointestinal; GU, genitourinary; ICH, intracranial hemorrhage; INR, international normalized ratio; LMWH, low-molecular-weight heparin; RCT, randomized controlled trial; TTR, time in therapeutic range; VKA, vitamin K antagonist; VTE, venous thromboembolism.
Apparent DOAC Failure and Recurrent Thrombosis
Recurrent thrombosis during DOAC therapy should be interpreted with caution, because true anticoagulant failure is uncommon, occurring in approximately 2% of treated patients, with similar rates observed with DOACs and vitamin K antagonists.[13] Before labeling treatment failure, clinicians should confirm true recurrence with appropriate imaging and distinguish it from residual thrombosis or alternative diagnoses. Current guidelines recommend objective confirmation, with recurrence defined by involvement of a previously unaffected vascular territory.[13]
Once recurrence is established, a structured evaluation should focus on identifying modifiable contributors (see Image. Clinical Approach to Recurrent Thrombosis With DOAC Therapy). Common factors include nonadherence, inappropriate dose reduction, drug interactions, impaired absorption, and changes in renal function. Off-label underdosing is particularly important because it is associated with increased thromboembolic risk and mortality without a reduction in bleeding. Concomitant use of CYP3A4 or P-glycoprotein inducers may reduce DOAC exposure, while gastrointestinal tract conditions or prior surgical procedures can impair absorption. Additionally, underlying prothrombotic states, including cancer, antiphospholipid syndrome, or severe thrombophilia, should be considered.[13][47] Although routine monitoring of DOAC levels is not recommended, measurement may be helpful in selected clinical scenarios, including suspected treatment failure, extremes of body weight, or potential drug interactions. Both low and high drug levels have been associated with increased risks of thrombosis and bleeding, respectively.[48]
If recurrent thrombosis occurs despite confirmed therapeutic anticoagulation, current guidelines recommend transitioning to an alternative anticoagulant, typically a parenteral agent such as LMWH or fondaparinux, rather than switching between DOACs. Specialist consultation is advised in complex cases, particularly when recurrence occurs in the context of cancer, antiphospholipid syndrome, or significant renal or gastrointestinal impairment.[25][47] Mechanistically, DOAC failure in certain conditions may relate to their single-target inhibition of factor Xa or thrombin, in contrast to the broader anticoagulant effect of vitamin K antagonists. This distinction may be clinically relevant in disorders driven by intrinsic pathway activation, such as antiphospholipid syndrome or device-related thrombosis.[25]
Treatment / Management
Anticoagulation Reversal
Management of major bleeding in patients taking anticoagulants begins with immediate cessation of anticoagulants and antiplatelet agents when feasible, along with hemodynamic stabilization, local bleeding control, and transfusion support. Reversal should be reserved for life-threatening, uncontrolled, or critical-site bleeding, or when urgent procedures are required, given the associated thromboembolic risk.
Reversal strategies are agent-specific:
- Unfractionated heparin is reversed with protamine sulfate, administered at 1 mg per 100 units of heparin given in the preceding 2 to 3 hours (maximum 50 mg), infused slowly (≤5 mg/min). Repeat dosing of 0.5 mg per 100 units may be given if the activated partial thromboplastin time remains elevated.[42][49]
- Low-molecular-weight heparin is only partially reversible; protamine is given as 1 mg per 1 mg enoxaparin within 8 hours, or 0.5 mg per 1 mg if 8 to 12 hours have elapsed, with consideration of a repeat dose in ongoing bleeding.[42][49]
- Fondaparinux has no specific antidote; management is supportive, although recombinant factor VIIa (90 μg/kg) may be considered in life-threatening bleeding despite limited evidence.[49][50]
- For warfarin-associated bleeding, guidelines recommend 4-factor prothrombin complex concentrate at 50 U/kg intravenously, combined with intravenous vitamin K (5–10 mg), to achieve rapid and sustained reversal. Fresh-frozen plasma is an alternative when 4-factor prothrombin complex concentrate is unavailable, but it is less effective and associated with volume overload.[12][51]
- Reversal of DOACs depends on the specific agent. Dabigatran is reversed with idarucizumab (5 g intravenous given as 2 separate 2.5 g boluses), which rapidly neutralizes its effect; hemodialysis can remove approximately 60% of the drug in 2–3 hours if needed.[22][52] For factor Xa inhibitors (apixaban, rivaroxaban, edoxaban), 4-factor prothrombin complex concentrate at 50 U/kg IV is currently the primary reversal strategy in the United States following withdrawal of andexanet alfa, which demonstrated improved hemostasis but higher thrombotic risk without mortality benefit. Activated 4-factor prothrombin complex concentrate may be considered selectively. Adjunctive measures include activated charcoal administered within 2 to 4 hours of DOAC ingestion and supportive care tailored to the severity of bleeding.[53] Emerging agents such as ciraparantag, a potential universal reversal agent, are under investigation.[54] (A1)
Overall, anticoagulation reversal requires a careful balance between rapid hemostasis and thrombotic risk, and should follow standardized institutional protocols whenever possible.
Resumption of Anticoagulation After Bleeding
Standardized bleeding definitions are essential for consistent reporting in anticoagulation studies. The International Society on Thrombosis and Hemostasis classification categorizes bleeding into major, clinically relevant nonmajor, and minor. Major bleeding includes fatal events, bleeding in critical organs, a hemoglobin drop of at least 2 g/dL, or transfusion of at least 2 units of blood. Clinically relevant nonmajor bleeding refers to overt bleeding that requires medical attention, hospitalization, or a change in therapy but does not meet the major criteria. In contrast, minor bleeding includes self-limited events that do not require intervention.[22](B3)
In patients who experience major bleeding, resumption of anticoagulation is often associated with a net clinical benefit once the bleeding source is controlled. The decision should be individualized based on thrombotic and bleeding risks, as well as the underlying indication for anticoagulation. In general, guidelines suggest resuming therapy between 2 weeks and 90 days after a major bleed, with earlier resumption considered in high thrombotic risk patients, sometimes using short-acting agents such as unfractionated heparin.[22](B3)
Timing varies by bleeding site. After gastrointestinal tract bleeding, resumption within 7 days is associated with reduced thromboembolism and mortality despite a modest increase in recurrent bleeding risk.[55] Intracranial hemorrhage requires a more cautious approach, with resumption typically delayed to 4 to 8 weeks, or longer in patients at high risk of recurrence, such as those with cerebral amyloid angiopathy. Results from emerging randomized trial data suggest that restarting anticoagulation after intracranial hemorrhage reduces ischemic events without a clear increase in recurrent bleeding, although evidence remains limited.[51][56] In selected patients, particularly those with high rebleeding risk or uncertain indications, delayed resumption or alternative strategies such as left atrial appendage occlusion may be appropriate.[57] Overall, decisions regarding anticoagulation resumption should incorporate clinical context, imaging findings, and patient preferences, emphasizing an individualized approach.(A1)
Periprocedural Management
Periprocedural management of DOACs should follow a standardized, pharmacokinetic-based approach guided by procedural bleeding risk, renal function, and the specific agent. Results from the PAUSE study supported simple interruption strategies without heparin bridging or routine drug-level testing, demonstrating low rates of thromboembolism and major bleeding. Accordingly, routine preoperative DOAC level measurement is not recommended for elective procedures, although measurement may be useful in urgent settings to guide reversal decisions.[58]
In general, DOACs are held 1 day before low to moderate-risk bleeding procedures and 2 days before high-risk procedures, with a longer interruption required in renal impairment, particularly for dabigatran. DOACs should be taken on the day of the surgical procedure. For neuraxial procedures, more conservative interruption is required, typically more than 3 days for factor Xa inhibitors and more than 4 days for dabigatran, because of the risk of spinal hematoma.[58]
Heparin bridging is not recommended because DOACs have short half-lives and a rapid onset of action, and bridging increases bleeding risk without reducing thromboembolic risk. Postoperatively, DOACs are generally resumed 24 hours after low-risk procedures and 48 to 72 hours after high-risk procedures, once hemostasis is attained. In patients at high thrombotic risk with delayed DOAC resumption, short-term prophylactic-dose LMWH may be considered.[58]
Differential Diagnosis
The differential diagnosis in patients taking anticoagulation depends on the presenting symptom and on whether the concern is bleeding, thrombosis, or another process that mimics either. Anticoagulation may worsen bleeding from an existing lesion, but clinicians should not automatically assume anticoagulation is the sole cause of the presentation.
Suspected Gastrointestinal Bleeding
- Peptic ulcer disease
- Gastrointestinal malignant tumors
- Angiodysplasia or vascular ectasia
- Diverticular bleeding, colitis, or hemorrhoidal bleeding
- Portal hypertensive bleeding in patients with liver disease
Hematuria or Genitourinary Tract Bleeding
- Urinary tract infection
- Nephrolithiasis
- Bladder or renal malignant neoplasm.
- Glomerulonephritis or other intrinsic renal disease
Acute Neurologic Symptoms
- Intracranial hemorrhage related to anticoagulation
- Ischemic stroke or transient ischemic attack
- Subarachnoid hemorrhage
- Brain mass lesion
- Migraine, seizure, or metabolic encephalopathy
Back Pain With Weakness or Sensory Change
- Spinal epidural hematoma, especially in patients receiving anticoagulation
- Spinal abscess
- Disc herniation
- Vertebral fracture
- Metastatic spinal cord compression
Chest Pain, Dyspnea, or Tachycardia
- Pulmonary embolism from treatment failure
- Acute coronary syndrome
- Heart failure exacerbation
- Pneumonia
- Hemothorax or hemopericardium
- Anxiety or other noncardiopulmonary causes
Limb Pain or Swelling
- Deep venous thrombosis despite therapy
- Cellulitis
- Superficial thrombophlebitis
- Venous insufficiency or lymphedema
- Trauma-related hematoma
- Compartment syndrome
Unexplained Anemia
- Occult gastrointestinal tract blood loss
- Iron deficiency
- Hemolysis
- Vitamin B12 or folate deficiency
- Bone marrow disease
- Chronic kidney disease or anemia of chronic inflammation
Differential Diagnoses for Warfarin-Induced Skin Necrosis
- Necrotizing fasciitis
- Venous gangrene (eg, phlegmasia cerulea dolens)
- Heparin-induced thrombocytopenia with thrombosis
- Disseminated intravascular coagulation
- Purpura fulminans (eg, severe sepsis, congenital or acquired protein C deficiency)
- Calciphylaxis (uremic or nonuremic)
- Extensive hematoma or cellulitis
- Pyoderma gangrenosum or other neutrophilic dermatoses
- Cholesterol crystal embolization (blue toe or livedo with intact pulses)
Prognosis
Direct oral anticoagulants generally have a more favorable prognosis after anticoagulant-related major bleeding compared with warfarin. Meta-analytic data findings from large phase 3 trials demonstrate lower case-fatality rates with DOACs (7.6% vs 11.0%), along with significant reductions in fatal bleeding, cardiovascular mortality, and all-cause mortality. This advantage is primarily driven by a substantially lower incidence of intracranial hemorrhage (approximately 50% lower than with warfarin), smaller hematoma volumes, and less severe neurologic injury.[59] Results from large observational cohorts further support lower in-hospital mortality with DOAC-associated intracranial hemorrhage, although some studies show comparable outcomes when patients with similar anticoagulant intensity are analyzed, suggesting a potential contribution of selection bias.[60]
In contrast, outcomes following gastrointestinal bleeding are more heterogeneous and appear to be agent-specific. Overall mortality after gastrointestinal tract bleeding is similar between DOACs and warfarin; however, DOAC resumption is associated with lower risks of recurrent bleeding and composite adverse outcomes. Among individual agents, apixaban consistently demonstrates the most favorable bleeding profile, with lower rates of both major bleeding and gastrointestinal bleeding compared with rivaroxaban and warfarin, a finding now supported by head-to-head randomized trial data. Conversely, rivaroxaban and higher-dose dabigatran and edoxaban have been associated with increased gastrointestinal tract bleeding risk.[61] Overall, the survival advantage of DOACs reflects a combination of reduced intracranial hemorrhage, lower rates of fatal bleeding, and, in many cases, less severe bleeding presentations. However, this benefit is not uniform across all bleeding types, and outcomes may be comparable in certain high-risk subgroups.
Complications
Complications of anticoagulant therapy include both hemorrhagic and nonhemorrhagic events. Major bleeding remains the most clinically important complication and may present as intracranial, gastrointestinal tract, retroperitoneal, intra-articular, intramuscular, or spinal and epidural hemorrhage; intracranial and intraspinal bleeding carry the highest risk of death and permanent neurologic disability. Anticoagulant interruption, underdosing, nonadherence, and drug interactions may also result in thromboembolic complications, including recurrent venous thromboembolism, cardioembolic stroke, and valve thrombosis in high-risk patients.
Warfarin-specific complications include skin necrosis, cholesterol embolization, teratogenicity, vascular calcification, and anticoagulant-related nephropathy. Direct oral anticoagulants are generally associated with fewer intracranial bleeding events than warfarin. However, DOACs may still cause significant gastrointestinal tract bleeding and can produce nonhemorrhagic adverse effects such as dyspepsia, particularly with dabigatran, and rare renal or hepatic injury. In patients undergoing neuraxial procedures, spinal epidural hematoma is a rare but extremity- and life-threatening complication that should be suspected in any patient taking an anticoagulant with acute back pain, weakness, sensory loss, or urinary retention.
Consultations
Consultation with appropriate specialists is essential to optimize anticoagulation safety and outcomes. Hematology or vascular medicine experts should be involved for complex indications, including mechanical heart valves, antiphospholipid syndrome, and cancer-associated thrombosis; recurrent thromboembolism or stroke on therapeutic anticoagulation; suspected drug failure; heparin-induced thrombocytopenia; or challenging decisions about resuming therapy after major bleeding. Cardiology or electrophysiology consultation is warranted for patients with atrial fibrillation and high stroke risk, mechanical or rheumatic valvular disease, left atrial appendage occlusion devices, or the need to balance triple therapy after acute coronary syndrome and stenting. Neurology and neurosurgery input is critical in anticoagulant-associated intracranial hemorrhage to guide reversal, neurosurgical interventions, and timing of anticoagulation resumption, while gastroenterology and interventional radiology should be engaged for significant gastrointestinal tract or solid-organ bleeding requiring endoscopic or radiologic intervention. Nephrology and hepatology consultation is advised in advanced chronic kidney disease or cirrhosis when drug choice and dosing are uncertain, and obstetrics and maternal-fetal medicine should guide anticoagulation in pregnancy, especially with mechanical valves or high-risk thrombophilias. Finally, coordinated input from pharmacy, nursing, and primary care or hospital medicine teams is crucial for medication reconciliation, patient education, periprocedural management, and the development of systems-level protocols that reduce preventable anticoagulant-related harm.
Deterrence and Patient Education
Deterrence of anticoagulant-related harm relies heavily on structured, repeated patient education rather than one-time counseling. Patients should understand the indication for therapy, the importance of strict adherence (especially with DOACs, given their short half-lives), and what to do after a missed dose to avoid gaps in anticoagulant effect and preventable thromboembolism. Education must also cover warning signs of bleeding (eg, melena, hematemesis, hematuria, new severe headache, focal neurologic deficits), when to seek urgent care, and the need to notify clinicians before any invasive procedure or new prescription, including over-the-counter nonsteroidal anti-inflammatory drugs and herbal supplements. For warfarin, counseling should emphasize consistent vitamin K intake and avoidance of interacting drugs and alcohol; for DOACs, discussions should highlight renal function monitoring, timing with meals when relevant, and the consequences of missed doses. Use of pill organizers, alarms, written dosing calendars, and teach-back techniques, as well as pharmacist- or nurse-led education at initiation and transitions of care, has been associated with better adherence and fewer extreme INRs and adverse events.
Enhancing Healthcare Team Outcomes
Improving anticoagulation outcomes requires an interprofessional, systems-based approach that goes beyond individual prescribing decisions. Standardized protocols for DOAC initiation and warfarin management, covering agent selection, dose adjustment by renal function, documented indication, and planned follow-up, reduce prescribing errors and ensure that patients at high-risk receive appropriate therapy. Anticoagulation clinics with pharmacy services can monitor adherence, drug interactions, renal and hepatic function, and bleeding or thrombotic events at intervals, thereby reducing complications and unplanned hospitalizations. Clear periprocedural pathways, with agreed interruption and resumption strategies, help avoid both unnecessary bleeding and preventable perioperative thrombosis. Finally, the routine use of interprofessional rounds and communication among clinicians, pharmacists, nurses, and case managers (especially around discharge and transitions of care) has been shown to shorten length of stay and improve safety metrics, thereby aligning anticoagulation management with broader quality improvement goals.
Media
(Click Image to Enlarge)
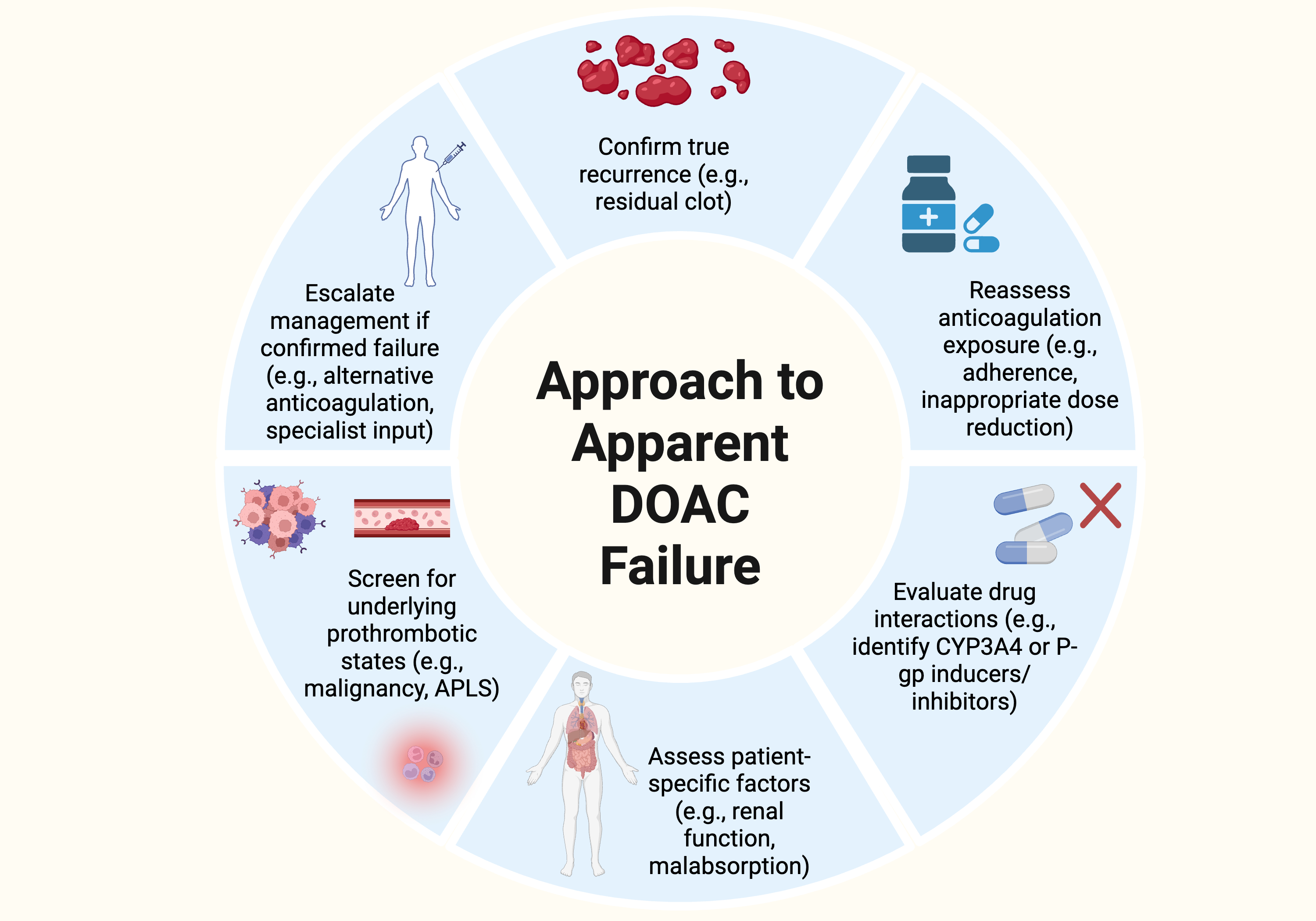
Clinical Approach to Recurrent Thrombosis With DOAC Therapy. The algorithm for investigating and managing recurrent thrombosis during direct oral anticoagulant therapy includes diagnostic confirmation, adherence, drug-drug interaction evaluation, and screening for underlying prothrombotic conditions.
Contributed by S Garg, MD
References
Gorog DA, Gue YX, Chao TF, Fauchier L, Ferreiro JL, Huber K, Konstantinidis SV, Lane DA, Marin F, Oldgren J, Potpara T, Roldan V, Rubboli A, Sibbing D, Tse HF, Vilahur G, Lip GYH. Assessment and mitigation of bleeding risk in atrial fibrillation and venous thromboembolism: A Position Paper from the ESC Working Group on Thrombosis, in collaboration with the European Heart Rhythm Association, the Association for Acute CardioVascular Care and the Asia-Pacific Heart Rhythm Society. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology. 2022 Nov 22:24(11):1844-1871. doi: 10.1093/europace/euac020. Epub [PubMed PMID: 35323922]
Nguyen UT, Nguyen MH, Duong KNC, Nguyen PTL, Cao HTT, Nguyen QN, Vu HD, Nguyen HA. Risk factors of anticoagulation-related bleeding in hospitalized patients: a systematic review and meta-analysis. Expert opinion on drug safety. 2026 Jan 23:():1-12. doi: 10.1080/14740338.2026.2612980. Epub 2026 Jan 23 [PubMed PMID: 41557588]
Level 1 (high-level) evidenceMar PL, Gopinathannair R, Gengler BE, Chung MK, Perez A, Dukes J, Ezekowitz MD, Lakkireddy D, Lip GYH, Miletello M, Noseworthy PA, Reiffel J, Tisdale JE, Olshansky B, from the American Heart Association Electrocardiography & Arrhythmias Committee of the Council of Clinical Cardiology. Drug Interactions Affecting Oral Anticoagulant Use. Circulation. Arrhythmia and electrophysiology. 2022 Jun:15(6):e007956. doi: 10.1161/CIRCEP.121.007956. Epub 2022 May 27 [PubMed PMID: 35622425]
Hanigan S, Das J, Pogue K, Barnes GD, Dorsch MP. The real world use of combined P-glycoprotein and moderate CYP3A4 inhibitors with rivaroxaban or apixaban increases bleeding. Journal of thrombosis and thrombolysis. 2020 May:49(4):636-643. doi: 10.1007/s11239-020-02037-3. Epub [PubMed PMID: 31925665]
Shoeb M, Fang MC. Assessing bleeding risk in patients taking anticoagulants. Journal of thrombosis and thrombolysis. 2013 Apr:35(3):312-9. doi: 10.1007/s11239-013-0899-7. Epub [PubMed PMID: 23479259]
Loncharich A, Gage BF, Luo S, Schoen M, Afzal A, Mahmoud A, Carson K, Chang SH, Yan Y, Sanfilippo KM. Risk factors for anticoagulant-related bleeding in cancer: traditional and cancer-specific factors. Blood vessels, thrombosis & hemostasis. 2026 Feb:3(1):100116. doi: 10.1016/j.bvth.2025.100116. Epub 2025 Oct 9 [PubMed PMID: 41458147]
Cannistraro RJ, Meschia JF. The Clinical Dilemma of Anticoagulation Use in Patients with Cerebral Amyloid Angiopathy and Atrial Fibrillation. Current cardiology reports. 2018 Sep 12:20(11):106. doi: 10.1007/s11886-018-1052-1. Epub 2018 Sep 12 [PubMed PMID: 30209626]
Holthuis E, Smits E, Spentzouris G, Beier D, Enders D, Gini R, Bartolini C, Mazzaglia G, Penning-van Beest F, Herings R. Increased Risk of Stroke Due to Non-adherence and Non-persistence with Direct Oral Anticoagulants (DOACs): Real-World Analyses Using a Nested Case-Control Study from The Netherlands, Italy and Germany. Drugs - real world outcomes. 2022 Dec:9(4):597-607. doi: 10.1007/s40801-022-00317-3. Epub 2022 Jul 5 [PubMed PMID: 35790603]
Level 2 (mid-level) evidenceLiu XQ, Li ZR, Wang CY, Jiao Z. Handling delayed or missed direct oral anticoagulant doses: model-informed individual remedial dosing. Blood advances. 2024 Nov 26:8(22):5906-5916. doi: 10.1182/bloodadvances.2024013854. Epub [PubMed PMID: 39293087]
Level 3 (low-level) evidenceMay JE, Allen AL, Samuelson Bannow BT, O'Connor C, Sylvester KW, Kaatz S. Safe and effective anticoagulation use: case studies in anticoagulation stewardship. Journal of thrombosis and haemostasis : JTH. 2025 Mar:23(3):779-789. doi: 10.1016/j.jtha.2024.11.024. Epub 2024 Dec 10 [PubMed PMID: 39667688]
Level 3 (low-level) evidenceAgeno W, Bertoletti L, Lindhoff-Last E, Lip G, Meijer K, Monreal M, Tran H, Bessada Y, Triller D, Burnett A, Ansell J. It's time to improve antithrombotic therapy! A global perspective for antithrombotic stewardship. European journal of internal medicine. 2026 May:147():106839. doi: 10.1016/j.ejim.2026.106839. Epub 2026 Mar 18 [PubMed PMID: 41856877]
Level 3 (low-level) evidenceJoglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, Deswal A, Eckhardt LL, Goldberger ZD, Gopinathannair R, Gorenek B, Hess PL, Hlatky M, Hogan G, Ibeh C, Indik JH, Kido K, Kusumoto F, Link MS, Linta KT, Marcus GM, McCarthy PM, Patel N, Patton KK, Perez MV, Piccini JP, Russo AM, Sanders P, Streur MM, Thomas KL, Times S, Tisdale JE, Valente AM, Van Wagoner DR, Peer Review Committee Members. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jan 2:149(1):e1-e156. doi: 10.1161/CIR.0000000000001193. Epub 2023 Nov 30 [PubMed PMID: 38033089]
Level 1 (high-level) evidenceWriting Committee Members, Creager MA, Barnes GD, Giri J, Mukherjee D, Jones WS, Burnett AE, Carman T, Casanegra AI, Castellucci LA, Clark SM, Cushman M, de Wit K, Eaves JM, Fang MC, Goldberg JB, Henkin S, Johnston-Cox H, Kadavath S, Kadian-Dodov D, Keeling WB, Klein AJP, Li J, McDaniel MC, Moores LK, Piazza G, Prenger KS, Pugliese SC, Ranade M, Rosovsky RP, Russo F, Secemsky EA, Sista AK, Tefera L, Weinberg I, Westafer LM, Young MN. 2026 AHA/ACC/ACCP/ACEP/CHEST/SCAI/SHM/SIR/SVM/SVN Guideline for the Evaluation and Management of Acute Pulmonary Embolism in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2026 Mar 24:153(12):e977-e1051. doi: 10.1161/CIR.0000000000001415. Epub 2026 Feb 19 [PubMed PMID: 41712677]
Level 1 (high-level) evidenceKhan F, Tritschler T, Kimpton M, Wells PS, Kearon C, Weitz JI, Büller HR, Raskob GE, Ageno W, Couturaud F, Prandoni P, Palareti G, Legnani C, Kyrle PA, Eichinger S, Eischer L, Becattini C, Agnelli G, Vedovati MC, Geersing GJ, Takada T, Cosmi B, Aujesky D, Marconi L, Palla A, Siragusa S, Bradbury CA, Parpia S, Mallick R, Lensing AWA, Gebel M, Grosso MA, Thavorn K, Hutton B, Le Gal G, Fergusson DA, Rodger MA, MAJESTIC Collaborators. Long-Term Risk for Major Bleeding During Extended Oral Anticoagulant Therapy for First Unprovoked Venous Thromboembolism : A Systematic Review and Meta-analysis. Annals of internal medicine. 2021 Oct:174(10):1420-1429. doi: 10.7326/M21-1094. Epub 2021 Sep 14 [PubMed PMID: 34516270]
Level 1 (high-level) evidenceLv M, Wu T, Jiang S, Chen W, Zhang J. Risk of Intracranial Hemorrhage Caused by Direct Oral Anticoagulants for Stroke Prevention in Patients With Atrial Fibrillation (from a Network Meta-Analysis of Randomized Controlled Trials). The American journal of cardiology. 2022 Jan 1:162():92-99. doi: 10.1016/j.amjcard.2021.09.011. Epub 2021 Oct 29 [PubMed PMID: 34756593]
Level 1 (high-level) evidenceBea S, Iyer GS, Kim DH, Lin KJ, Zhang Y, Zakoul H, Tesfaye H, Bykov K. Oral Anticoagulation and Risk of Adverse Clinical Outcomes in Venous Thromboembolism. JAMA internal medicine. 2025 Jul 1:185(7):837-846. doi: 10.1001/jamainternmed.2025.1109. Epub [PubMed PMID: 40354043]
Level 2 (mid-level) evidenceLip GYH, Benamouzig R, Martin AC, Pesce G, Gusto G, Quignot N, Khachatryan A, Dai F, Sedjelmaci F, Chaves J, Subash R, Mokgokong R. Comparative safety and effectiveness of oral anticoagulants in patients with non-valvular atrial fibrillation and high risk of gastrointestinal bleeding: A nationwide French cohort study. PloS one. 2024:19(11):e0310322. doi: 10.1371/journal.pone.0310322. Epub 2024 Nov 15 [PubMed PMID: 39546473]
Level 2 (mid-level) evidenceKim DH, Pawar A, Gagne JJ, Bessette LG, Lee H, Glynn RJ, Schneeweiss S. Frailty and Clinical Outcomes of Direct Oral Anticoagulants Versus Warfarin in Older Adults With Atrial Fibrillation : A Cohort Study. Annals of internal medicine. 2021 Sep:174(9):1214-1223. doi: 10.7326/M20-7141. Epub 2021 Jul 20 [PubMed PMID: 34280330]
Level 2 (mid-level) evidenceNicolau AM, Giugliano RP, Zimerman A, Afilalo J, Gencer B, Steffel J, Palazzolo MG, Eikelboom JW, Granger CB, Patel MR, Lopes RD, Gersh BJ, Suleiman B, de Groot JR, Scanavacca MI, Ruff CT, Antman EM, Braunwald E, Wallentin L. Outcomes in Older Patients After Switching to a Newer Anticoagulant or Remaining on Warfarin: The COMBINE-AF Substudy. Journal of the American College of Cardiology. 2025 Aug 12:86(6):426-439. doi: 10.1016/j.jacc.2025.05.060. Epub [PubMed PMID: 40769671]
Wheeler DS, Giugliano RP, Rangaswami J. Anticoagulation-related nephropathy. Journal of thrombosis and haemostasis : JTH. 2016 Mar:14(3):461-7. doi: 10.1111/jth.13229. Epub 2016 Feb 15 [PubMed PMID: 26670286]
Ryan M, Ware K, Qamri Z, Satoskar A, Wu H, Nadasdy G, Rovin B, Hebert L, Nadasdy T, Brodsky SV. Warfarin-related nephropathy is the tip of the iceberg: direct thrombin inhibitor dabigatran induces glomerular hemorrhage with acute kidney injury in rats. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2014 Dec:29(12):2228-34. doi: 10.1093/ndt/gft380. Epub 2013 Sep 5 [PubMed PMID: 24009280]
Tomaselli GF, Mahaffey KW, Cuker A, Dobesh PP, Doherty JU, Eikelboom JW, Florido R, Gluckman TJ, Hucker WJ, Mehran R, Messé SR, Perino AC, Rodriguez F, Sarode R, Siegal DM, Wiggins BS. 2020 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Solution Set Oversight Committee. Journal of the American College of Cardiology. 2020 Aug 4:76(5):594-622. doi: 10.1016/j.jacc.2020.04.053. Epub 2020 Jul 14 [PubMed PMID: 32680646]
Level 3 (low-level) evidenceBrodsky S, Eikelboom J, Hebert LA. Anticoagulant-Related Nephropathy. Journal of the American Society of Nephrology : JASN. 2018 Dec:29(12):2787-2793. doi: 10.1681/ASN.2018070741. Epub 2018 Nov 12 [PubMed PMID: 30420420]
Wheelock KM, Ross JS, Murugiah K, Lin Z, Krumholz HM, Khera R. Clinician Trends in Prescribing Direct Oral Anticoagulants for US Medicare Beneficiaries. JAMA network open. 2021 Dec 1:4(12):e2137288. doi: 10.1001/jamanetworkopen.2021.37288. Epub 2021 Dec 1 [PubMed PMID: 34870678]
Bejjani A, Khairani CD, Assi A, Piazza G, Sadeghipour P, Talasaz AH, Fanikos J, Connors JM, Siegal DM, Barnes GD, Martin KA, Angiolillo DJ, Kleindorfer D, Monreal M, Jimenez D, Middeldorp S, Elkind MSV, Ruff CT, Goldhaber SZ, Krumholz HM, Mehran R, Cushman M, Eikelboom JW, Lip GYH, Weitz JI, Lopes RD, Bikdeli B. When Direct Oral Anticoagulants Should Not Be Standard Treatment: JACC State-of-the-Art Review. Journal of the American College of Cardiology. 2024 Jan 23:83(3):444-465. doi: 10.1016/j.jacc.2023.10.038. Epub [PubMed PMID: 38233019]
Eikelboom JW, Connolly SJ, Brueckmann M, Granger CB, Kappetein AP, Mack MJ, Blatchford J, Devenny K, Friedman J, Guiver K, Harper R, Khder Y, Lobmeyer MT, Maas H, Voigt JU, Simoons ML, Van de Werf F, RE-ALIGN Investigators. Dabigatran versus warfarin in patients with mechanical heart valves. The New England journal of medicine. 2013 Sep 26:369(13):1206-14. doi: 10.1056/NEJMoa1300615. Epub 2013 Aug 31 [PubMed PMID: 23991661]
Level 1 (high-level) evidenceCelia AI, Vescovo GM, Sarto G, Alessandri C, Iaconelli A, D'Amario D, Frati G, Conti F, Sciarretta S, Angiolillo DJ, Fava A, Petri MA, Bikdeli B, Galli M. Direct oral anticoagulants versus Vitamin K antagonists in antiphospholipid syndrome: A systematic review and meta-analysis. Seminars in arthritis and rheumatism. 2025 Aug:73():152741. doi: 10.1016/j.semarthrit.2025.152741. Epub 2025 May 1 [PubMed PMID: 40344935]
Level 1 (high-level) evidenceAmerican College of Obstetricians and Gynecologists' Committee on Practice Bulletins—Obstetrics. ACOG Practice Bulletin No. 196: Thromboembolism in Pregnancy. Obstetrics and gynecology. 2018 Jul:132(1):e1-e17. doi: 10.1097/AOG.0000000000002706. Epub [PubMed PMID: 29939938]
Leong R, Chu DK, Crowther MA, Mithoowani S. Direct oral anticoagulants after bariatric surgery-What is the evidence? Journal of thrombosis and haemostasis : JTH. 2022 Sep:20(9):1988-2000. doi: 10.1111/jth.15823. Epub 2022 Jul 28 [PubMed PMID: 35844166]
Diesveld MME, Pijnenburg DWMJ, Weersink RA, Barzel I, Drenth JPH, Lisman T, Metselaar HJ, Monster-Simons MH, Mulder MB, Okel E, Taxis K, Borgsteede SD. Recommendations for the safe use of direct oral anticoagulants in patients with cirrhosis based on a systematic review of pharmacokinetic, pharmacodynamic and safety data. European journal of clinical pharmacology. 2024 Jun:80(6):797-812. doi: 10.1007/s00228-024-03648-y. Epub 2024 Mar 2 [PubMed PMID: 38430266]
Level 1 (high-level) evidenceRosovsky RP, Kline-Rogers E, Lake L, Minichiello T, Piazza G, Ragheb B, Waldron B, Witt DM, Moll S. Direct Oral Anticoagulants in Obese Patients with Venous Thromboembolism: Results of an Expert Consensus Panel. The American journal of medicine. 2023 Jun:136(6):523-533. doi: 10.1016/j.amjmed.2023.01.010. Epub 2023 Feb 16 [PubMed PMID: 36803697]
Level 3 (low-level) evidenceElshafei MN, Salem M, El-Bardissy A, Abdelmoneim MS, Khalil A, Elhadad S, Al Mistarihi M, Danjuma M. Comparative Effectiveness and Safety of Direct Oral Anticoagulants in Low Body Weight Patients with Atrial Fibrillation: A Systematic Review and Meta-analysis. Cardiovascular drugs and therapy. 2025 Jun:39(3):643-660. doi: 10.1007/s10557-023-07537-x. Epub 2024 Jan 2 [PubMed PMID: 38165553]
Level 1 (high-level) evidenceLee SR, Choi EK, Park CS, Han KD, Jung JH, Oh S, Lip GYH. Direct Oral Anticoagulants in Patients With Nonvalvular Atrial Fibrillation and Low Body Weight. Journal of the American College of Cardiology. 2019 Mar 5:73(8):919-931. doi: 10.1016/j.jacc.2018.11.051. Epub [PubMed PMID: 30819360]
Tan Y, Hubbard C, Owens H, Pitt J, Giuliano C, Haan B, Breeden T, Sirbu D, Pena K, Haddox T, Edwin SB. Efficacy and safety of factor Xa inhibitors in low body weight patients. Pharmacotherapy. 2024 Feb:44(2):131-140. doi: 10.1002/phar.2888. Epub 2023 Nov 14 [PubMed PMID: 37926690]
Saposnik G, Bushnell C, Coutinho JM, Field TS, Furie KL, Galadanci N, Kam W, Kirkham FC, McNair ND, Singhal AB, Thijs V, Yang VXD, American Heart Association Stroke Council; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; Council on Cardiovascular and Stroke Nursing; and Council on Hypertension. Diagnosis and Management of Cerebral Venous Thrombosis: A Scientific Statement From the American Heart Association. Stroke. 2024 Mar:55(3):e77-e90. doi: 10.1161/STR.0000000000000456. Epub 2024 Jan 29 [PubMed PMID: 38284265]
Levine GN, McEvoy JW, Fang JC, Ibeh C, McCarthy CP, Misra A, Shah ZI, Shenoy C, Spinler SA, Vallurupalli S, Lip GYH, American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; and Stroke Council. Management of Patients at Risk for and With Left Ventricular Thrombus: A Scientific Statement From the American Heart Association. Circulation. 2022 Oct 11:146(15):e205-e223. doi: 10.1161/CIR.0000000000001092. Epub 2022 Sep 15 [PubMed PMID: 36106537]
Ruiz-Artacho P, Lecumberri R, Trujillo-Santos J, Beddar Chaib F, Moustafa F, Lorenzo A, Gómez-Cuervo C, Bosevski M, Monreal M, RIETE Investigators. Direct Oral Anticoagulants versus Standard Therapy in Upper Extremity Deep Vein Thrombosis: Real-World Evidence. Thrombosis and haemostasis. 2026 Mar:126(3):287-296. doi: 10.1055/a-2615-4513. Epub 2025 May 19 [PubMed PMID: 40389231]
Lip GYH, Banerjee A, Boriani G, Chiang CE, Fargo R, Freedman B, Lane DA, Ruff CT, Turakhia M, Werring D, Patel S, Moores L. Antithrombotic Therapy for Atrial Fibrillation: CHEST Guideline and Expert Panel Report. Chest. 2018 Nov:154(5):1121-1201. doi: 10.1016/j.chest.2018.07.040. Epub 2018 Aug 22 [PubMed PMID: 30144419]
De Vriese AS, Heine G. Anticoagulation management in haemodialysis patients with atrial fibrillation: evidence and opinion. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association. 2022 Oct 19:37(11):2072-2079. doi: 10.1093/ndt/gfab060. Epub [PubMed PMID: 33647941]
Level 3 (low-level) evidenceJoosten LPT, van Doorn S, van de Ven PM, Köhlen BTG, Nierman MC, Koek HL, Hemels MEW, Huisman MV, Kruip M, Faber LM, Wiersma NM, Buding WF, Fijnheer R, Adriaansen HJ, Roes KC, Hoes AW, Rutten FH, Geersing GJ. Safety of Switching From a Vitamin K Antagonist to a Non-Vitamin K Antagonist Oral Anticoagulant in Frail Older Patients With Atrial Fibrillation: Results of the FRAIL-AF Randomized Controlled Trial. Circulation. 2024 Jan 23:149(4):279-289. doi: 10.1161/CIRCULATIONAHA.123.066485. Epub 2023 Aug 27 [PubMed PMID: 37634130]
Level 1 (high-level) evidenceNichols KM, Henkin S, Creager MA. Venous Thromboembolism Associated With Pregnancy: JACC Focus Seminar. Journal of the American College of Cardiology. 2020 Nov 3:76(18):2128-2141. doi: 10.1016/j.jacc.2020.06.090. Epub [PubMed PMID: 33121721]
Streiff MB, Holmstrom B, Angelini D, Ashrani A, Buckner T, Diep R, Fertrin KY, Fogerty AE, Crestani NG, Gangaraju R, Rojas-Hernandez C, Goldhaber SZ, Ibrahim I, Kubal T, Leavitt AD, Lim M, Mann J, Mantha S, Morton C, Nester A, O'Brien A, Ortel TL, Pine A, Pishko A, Ranade M, Salmasi A, Schaefer J, Williams E, Wool G, Wun T, Montgomery S, Nguyen J, Freedman-Cass D, Sliker B. Cancer-Associated Venous Thromboembolic Disease, Version 2.2024, NCCN Clinical Practice Guidelines in Oncology. Journal of the National Comprehensive Cancer Network : JNCCN. 2024 Sep:22(7):483-506. doi: 10.6004/jnccn.2024.0046. Epub [PubMed PMID: 39236759]
Level 1 (high-level) evidenceKey NS, Khorana AA, Kuderer NM, Bohlke K, Lee AYY, Arcelus JI, Wong SL, Balaban EP, Flowers CR, Gates LE, Kakkar AK, Tempero MA, Gupta S, Lyman GH, Falanga A. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Guideline Update. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2023 Jun 1:41(16):3063-3071. doi: 10.1200/JCO.23.00294. Epub 2023 Apr 19 [PubMed PMID: 37075273]
Wang TF, Carrier M, Fournier K, Siegal DM, Le Gal G, Delluc A. Oral Anticoagulant Use in Patients with Morbid Obesity: A Systematic Review and Meta-Analysis. Thrombosis and haemostasis. 2022 May:122(5):830-841. doi: 10.1055/a-1588-9155. Epub 2021 Oct 12 [PubMed PMID: 34399433]
Level 1 (high-level) evidenceOtto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O'Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Feb 2:143(5):e35-e71. doi: 10.1161/CIR.0000000000000932. Epub 2020 Dec 17 [PubMed PMID: 33332149]
Level 1 (high-level) evidenceRuiz-Irastorza G, Tektonidou MG, Khamashta M. Anticoagulant and non-anticoagulant therapy in thrombotic antiphospholipid syndrome: old drugs and new treatment targets. Rheumatology (Oxford, England). 2024 Feb 6:63(SI):SI96-SI106. doi: 10.1093/rheumatology/kead538. Epub [PubMed PMID: 38320592]
Mount HR, Rich M, Putnam MS. Recurrent Venous Thromboembolism. American family physician. 2022 Apr 1:105(4):377-385 [PubMed PMID: 35426644]
Swan D, Roberts L, Thachil J. In a nutshell: Testing DOAC levels-when, why and what it means? British journal of haematology. 2026 Feb:208(2):442-445. doi: 10.1111/bjh.70313. Epub 2026 Jan 2 [PubMed PMID: 41482473]
Frontera JA, Lewin JJ 3rd, Rabinstein AA, Aisiku IP, Alexandrov AW, Cook AM, del Zoppo GJ, Kumar MA, Peerschke EI, Stiefel MF, Teitelbaum JS, Wartenberg KE, Zerfoss CL. Guideline for Reversal of Antithrombotics in Intracranial Hemorrhage: A Statement for Healthcare Professionals from the Neurocritical Care Society and Society of Critical Care Medicine. Neurocritical care. 2016 Feb:24(1):6-46. doi: 10.1007/s12028-015-0222-x. Epub [PubMed PMID: 26714677]
Elmer J, Wittels KA. Emergency reversal of pentasaccharide anticoagulants: a systematic review of the literature. Transfusion medicine (Oxford, England). 2012 Apr:22(2):108-15. doi: 10.1111/j.1365-3148.2011.01125.x. Epub 2011 Dec 16 [PubMed PMID: 22171588]
Level 1 (high-level) evidenceGreenberg SM, Ziai WC, Cordonnier C, Dowlatshahi D, Francis B, Goldstein JN, Hemphill JC 3rd, Johnson R, Keigher KM, Mack WJ, Mocco J, Newton EJ, Ruff IM, Sansing LH, Schulman S, Selim MH, Sheth KN, Sprigg N, Sunnerhagen KS, American Heart Association/American Stroke Association. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. Stroke. 2022 Jul:53(7):e282-e361. doi: 10.1161/STR.0000000000000407. Epub 2022 May 17 [PubMed PMID: 35579034]
Eikelboom JW, van Ryn J, Reilly P, Hylek EM, Elsaesser A, Glund S, Pollack CV, Weitz JI. Dabigatran Reversal With Idarucizumab in Patients With Renal Impairment. Journal of the American College of Cardiology. 2019 Oct 8:74(14):1760-1768. doi: 10.1016/j.jacc.2019.07.070. Epub [PubMed PMID: 31582135]
Crawley RM, Sheikh-Taha M. Comparison of activated and 4-factor prothrombin complex concentrates for reversal of apixaban- and rivaroxaban-associated major bleeding. Journal of thrombosis and thrombolysis. 2026 Jan 12:():. doi: 10.1007/s11239-025-03232-w. Epub 2026 Jan 12 [PubMed PMID: 41525014]
Ng JX, Tan SC, Koh PL, Yap ES. Anticoagulation Stewardship Program in the DOAC Era. Journal of clinical medicine. 2026 Mar 29:15(7):. doi: 10.3390/jcm15072597. Epub 2026 Mar 29 [PubMed PMID: 41976898]
Sengupta N, Feuerstein JD, Jairath V, Shergill AK, Strate LL, Wong RJ, Wan D. Management of Patients With Acute Lower Gastrointestinal Bleeding: An Updated ACG Guideline. The American journal of gastroenterology. 2023 Feb 1:118(2):208-231. doi: 10.14309/ajg.0000000000002130. Epub 2022 Sep 21 [PubMed PMID: 36735555]
Hilkens NA, Casolla B, Leung TW, de Leeuw FE. Stroke. Lancet (London, England). 2024 Jun 29:403(10446):2820-2836. doi: 10.1016/S0140-6736(24)00642-1. Epub 2024 May 14 [PubMed PMID: 38759664]
Mavridis T, Archontakis-Barakakis P, Chlorogiannis DD, Charidimou A. Left atrial appendage occlusion in patients with atrial fibrillation and previous Intracranial Hemorrhage or Cerebral Amyloid Angiopathy: A systematic review and meta-analysis. International journal of stroke : official journal of the International Stroke Society. 2025 Oct:20(9):1049-1059. doi: 10.1177/17474930251360076. Epub 2025 Jul 10 [PubMed PMID: 40641042]
Level 1 (high-level) evidenceDouketis JD, Spyropoulos AC. Perioperative Management of Patients Taking Direct Oral Anticoagulants: A Review. JAMA. 2024 Sep 10:332(10):825-834. doi: 10.1001/jama.2024.12708. Epub [PubMed PMID: 39133476]
Chai-Adisaksopha C, Hillis C, Isayama T, Lim W, Iorio A, Crowther M. Mortality outcomes in patients receiving direct oral anticoagulants: a systematic review and meta-analysis of randomized controlled trials. Journal of thrombosis and haemostasis : JTH. 2015 Nov:13(11):2012-20. doi: 10.1111/jth.13139. Epub 2015 Oct 5 [PubMed PMID: 26356595]
Level 1 (high-level) evidenceKurogi R, Nishimura K, Nakai M, Kada A, Kamitani S, Nakagawara J, Toyoda K, Ogasawara K, Ono J, Shiokawa Y, Aruga T, Miyachi S, Nagata I, Matsuda S, Yoshimura S, Okuchi K, Suzuki A, Nakamura F, Onozuka D, Ido K, Kurogi A, Mukae N, Nishimura A, Arimura K, Kitazono T, Hagihara A, Iihara K, J-ASPECT Study Collaborators. Comparing intracerebral hemorrhages associated with direct oral anticoagulants or warfarin. Neurology. 2018 Mar 27:90(13):e1143-e1149. doi: 10.1212/WNL.0000000000005207. Epub 2018 Feb 28 [PubMed PMID: 29490916]
Gouriou C, Bouguen G, Lahmek P, Pelaquier A, Arotcarena R, Garioud A, De Montigny-Lenhardt S, Pauwels A, Zanditenas D, Charpignon C, Combes R, Nahon S, Quentin V. Outcomes of upper gastrointestinal bleeding are similar between direct oral anticoagulants and vitamin K antagonists. Alimentary pharmacology & therapeutics. 2021 Mar:53(6):688-695. doi: 10.1111/apt.16236. Epub 2021 Jan 5 [PubMed PMID: 33400827]