Introduction
An anembryonic pregnancy is characterized by a gestational sac that forms and grows while an embryo fails to develop. People with anembryonic pregnancies usually present with symptoms of early pregnancy failure. Although the terms anembryonic pregnancy and blighted ovum are synonymous, the latter is falling out of favor with the more descriptive former term. Anembryonic pregnancy constitutes a significant but unknown proportion of miscarriages, with the American Pregnancy Association estimating anembryonic pregnancy to constitute half of all first-trimester miscarriages. Approximately 15% of all clinically recognized pregnancies end in first-trimester loss, with live births occurring in only 30% of all pregnancies.[1][2][3] Many patients with early pregnancy loss (including anembryonic pregnancies) are unaware of their miscarriage, particularly when the loss occurs in the early stages of pregnancy.
Early Pregnancy Loss
In the first trimester, the terms early pregnancy loss, miscarriage, or spontaneous abortion are often used interchangeably. Early pregnancy loss is defined as the spontaneous loss of a pregnancy before 13 weeks of gestation.[4][5] Early pregnancy loss is the preferred terminology for these pregnancies, including the anembryonic pregnancy.[6]
Miscarriage
The World Health Organization (WHO) and the Centers for Disease Control and Prevention (CDC) define miscarriage as the loss of a pregnancy before 20 weeks of gestation or the ejection or removal of an embryo or fetus that weighs 500 g or less. This definition in the United States may vary by state law.[4][7]
Biochemical Miscarriage
Biochemical miscarriage is a loss that occurs after a positive urine pregnancy test (hCG) or a raised serum beta-hCG before ultrasound or histological verification and confirmation.
Clinical Miscarriage
Clinical miscarriage is diagnosed when ultrasound examination or histologic evidence has confirmed the existence of an intrauterine pregnancy. Clinical miscarriage is classified as early (before 12 weeks of pregnancy) and late (12 to 20 weeks of pregnancy).
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
The exact etiology of anembryonic pregnancies is difficult to ascertain. The etiological factors for anembryonic pregnancies are generally understood and studied in the broader context of early pregnancy loss (EPL), which includes both embryonic and anembryonic pregnancies. Etiologies of anembryonic pregnancies include the following:
- Morphological abnormalities: Morphological abnormalities of an embryo prevent implantation or prevent long-term survival of the embryo after implantation. These morphological abnormalities are thought to be related to chromosomal abnormalities.[5]
- Chromosomal abnormalities
- Autosomal trisomy, polyploidy, sex chromosomal polysomy, and monosomy X are likely the most common etiologies of EPL. However, half of all anembryonic pregnancies have been found to have normal chromosomes.[8]
- Trisomies are the primary fetal chromosomal abnormality in sporadic cases of miscarriage (30% of all miscarriages) and represent 60% of chromosomally abnormal miscarriages (recurrent miscarriages). Trisomies with monosomy X (15% to 25%) and triploidy (12% to 20%) account for over 90% of all chromosomal abnormalities found in sporadic cases of miscarriage. According to a study by Edmonds in 1992, trisomy 16, the most common chromosomal abnormality found in 15% of anembryonic pregnancies, gave rise to rudimentary embryonic growth with an empty sac, while other trisomies often resulted in early embryonic demise.[9]
- The incidence of other trisomies in anembryonic pregnancies is as follows: trisomy 22 (9.6%), trisomy 15 (3.8%), and trisomy 19 (3.8%).[8]
- Other genetic and chromosomal abnormalities: Translocations, inversions, single-gene perturbations, and placental mosaicism are some of the other genetic abnormalities that can cause anembryonic pregnancies.[10] Consanguineous marriages resulting in anembryonic pregnancies have also been noted, suggesting the role of single-gene determinants.[11] A probable link between DNA damage in sperm and miscarriage has been noted.[12]
- Obesity and advanced maternal age: These factors are well-established contributors to EPL.[13] Aneuploidies are more commonly seen in anembryonic pregnancies in women of advanced maternal age than in younger women.[8]
- Infection: Infectious etiologies are thought to play a role in anembryonic pregnancies. Tuberculosis in the developing world, as well as reproductive tract infections worldwide, can predispose to EPL.[14] The complications of genital tract infections, including intrauterine adhesions, can impede implantation and embryo growth.
- Uterine abnormalities: Malformations of the uterus, including didelphic, bicornuate, and septate uteri, can impede or prevent the long-term implantation of an embryo.
- Immunologic disorders: Maternal immunologic conditions, eg, NK cell dysfunction, autoantibodies, hereditary, and acquired thrombophilia, among others, can lead to the maternal immunological rejection of the implanting embryo in the uterus, resulting in miscarriage.
- Hormonal factors: Low levels of progesterone and endocrinological disorders, including thyroid autoimmunity and thyroid dysfunction, are a few of the hormonal factors that may play a complex role in miscarriage. Polycystic ovarian syndrome is also associated with infertility and pregnancy loss.
- Alcohol consumption: Maternal alcohol use has been established to have an associated increased risk of miscarriage.[15]
Epidemiology
Although difficult to definitively establish, anembryonic pregnancy possibly represents half of all miscarriages in the first trimester of pregnancy.[16][17] The incidence of early pregnancy loss (before 12 weeks) is estimated to be about 15% of clinically evident conceptions, with significant variations in incidence based on patient age. The incidence ranges from 10% in women aged 20 to 24 years to 51% in women aged 40 to 44 years.[18] A prior history of early pregnancy loss also predisposes a patient to miscarriage.[19]
History and Physical
The signs and symptoms of an anembryonic pregnancy can potentially mirror those of an ectopic pregnancy. Anembryonic pregnancy is often incidentally noted on an initial first-trimester obstetric sonogram. If an anembryonic pregnancy progresses to an early pregnancy loss, the patient can present with abdominal cramping and vaginal bleeding. Conversely, early pregnancy loss in the setting of an anembryonic pregnancy can be clinically asymptomatic. A previous anembryonic pregnancy is a risk for another similarly abnormal pregnancy.
Evaluation
Clinical signs and symptoms, along with pregnancy testing and ultrasound evaluation, confirm the diagnosis of an anembryonic pregnancy. Pregnancy testing may be performed using urine or serum hCG levels to support clinical suspicion and guide further assessment.
Transabdominal or transvaginal ultrasound classically demonstrates an empty gestational sac without visualization of an embryo (see Image. Anembryonic Pregnancy). Diagnostic confirmation occurs when ultrasound imaging shows no discernible embryo within a gestational sac measuring 25 mm or more in mean sac diameter. Diagnosis may also be established on follow-up endovaginal imaging when no embryo is visualized by 11 days or more after a prior scan that demonstrated a gestational sac with a yolk sac but no embryo, or 14 days or longer after a scan that demonstrated a gestational sac without an embryo or a yolk sac.
Treatment / Management
The 3 treatment options for early pregnancy loss include expectant management, medical management, and surgical treatment. Medical therapy with mifepristone and/or misoprostol, as well as surgical intervention, represents effective treatment for anembryonic gestations. Selection of a management strategy depends on an informed discussion between the patient and clinician, unless a clear indication for surgical intervention exists. If the success rate for medical management were higher than 65%, then most patients would prefer to manage their anembryonic pregnancy in this manner.
Expectant Management
Expectant management is a watchful-waiting approach in which the patient undergoes close follow-up without immediate intervention to allow for spontaneous and complete passage of tissue. Repeat sonograms and serial hCG measurements help confirm complete tissue expulsion. Confirmation of a negative hCG level after vaginal passage of tissue is recommended.
Medical Management
Medical management involves administration of mifepristone and/or misoprostol through vaginal, oral, or buccal routes, using varying doses and timing regimens. Ongoing research continues to evaluate optimal dosing strategies. This option offers a more predictable clinical course.
Surgical Treatment
Surgical treatment involves uterine evacuation using manual vacuum aspiration or dilation and curettage. Clinicians frequently select this approach for patients with hemodynamic instability or for those unable to tolerate the cramping and bleeding associated with medical therapy. Uterine aspiration or evacuation provides a faster completion time, particularly in the outpatient setting.[7]
Differential Diagnosis
The differential diagnosis for an anembryonic pregnancy includes the following:
- Pseudogestational sac, which reveals a small amount of intrauterine fluid but no pregnancy tissue
- Early intrauterine pregnancy
- An ectopic pregnancy
- Implantation bleeding from an otherwise viable pregnancy
- Gestational trophoblastic disease (Please see StatPearls' companion resource, "Gestational Trophoblastic Disease," for further information)
- Complications relating to a viable pregnancy
Pertinent Studies and Ongoing Trials
Maternal amino acids are crucial for early embryonic growth because the developing embryo relies entirely on the mother’s supply, delivered through uterine secretions and later the placenta. Proper placental development and a healthy maternal–fetal interface depend on adequate amino acid levels and transport. In a normal early pregnancy, maternal amino acid concentrations typically decline as the embryo begins to use them.
However, despite evidence that abnormal placentation contributes to anembryonic pregnancy, changes in maternal serum amino acid patterns in these pregnancies have not previously been studied. The viability of many early pregnancies is difficult to determine by ultrasound alone. Maternal serum amino acids are higher in individuals with anembryonic pregnancy. Using 17 amino acid levels, especially as a combined profile, has been shown to improve the diagnostic accuracy. This approach may offer a useful tool for early risk screening of anembryonic pregnancy in the future.[20]
Prognosis
Prognosis and successful management of an anembryonic pregnancy depend on multiple factors, including gestational age. Outcomes are generally favorable with all 3 management approaches.
Expectant management has demonstrated acceptable outcomes. A meta-analysis of 20 studies concluded that both expectant and medical management represent appropriate treatment options for incomplete abortion.[21] Medical management shows improved success with multiple-dose misoprostol regimens. Patients with incomplete abortion experience higher success rates with medical therapy compared with expectant management.
Surgical treatment demonstrates high efficacy. At least 1 large randomized controlled trial reported a higher success rate with surgical intervention than with medical management, while also concluding that both approaches maintain an overall favorable safety profile.[22]
Complications
Serious complications of anembryonic pregnancy treatment are uncommon, but can include:
- Heavy bleeding and hemorrhage
- Uterine perforation from surgical management
- Infection or septic abortion, which can be fatal
- Complications from a missed diagnosis of ectopic pregnancy [7]
Consultations
Necessary consultations in the management of an anembryonic pregnancy involve the following:
- Obstetrician
- Primary care clinician
- Psychologist/psychiatrist
- Emergency department physician
- Radiologist/sonographer (especially when clinical features of an ectopic pregnancy are noted)
Deterrence and Patient Education
The following represent critical points in patient education:
- Pregnant patients in the first trimester should be advised to present to their emergency department if they experience severe pain or heavy vaginal bleeding (2 pads per hour for approximately 2 consecutive hours).
- Signs and symptoms of infection should be discussed with patients, especially following surgical management and with those choosing expectant management.
- Treatment with mifepristone and misoprostol can cause a febrile reaction that may be misinterpreted as a sign of infection.
- Prophylactic antibiotics are not routinely administered except with surgical management.
- Patients should adhere to follow-up sonograms and outpatient appointments, particularly when additional doses of misoprostol are considered clinically necessary.
- A miscarriage can be a traumatic experience for a patient. Reassurance and empathy are vital in helping patients navigate the grieving process.
Pearls and Other Issues
Pertinent factors that should be kept in mind when managing an anembryonic pregnancy include:
- Pregnancy loss is a common complication in the first trimester of pregnancy.
- Most pregnancy losses occur in the first trimester.
- Early pregnancy loss without embryo development is likely due to chromosomal and genetic abnormalities.
- Specific sonographic criteria have been established for diagnosing an anembryonic pregnancy.
- A pseudogestational sac, an ectopic pregnancy, and an early viable pregnancy are important differential diagnoses to consider when evaluating an anembryonic pregnancy.
- Expectant management, medical treatment, and surgical treatment are the 3 primary management options.
Enhancing Healthcare Team Outcomes
Interprofessional teams are more effective when they work collaboratively and efficiently. Developing a well-defined strategy for managing anembryonic pregnancies is vital. Healthcare teams should establish standardized protocols for diagnosis, treatment options, and patient counseling. An evidence-based approach should guide decision-making, ensuring strategies align with the latest research and guidelines.
Each healthcare team member, from physicians to advanced care practitioners, nurses, and pharmacists, has distinct responsibilities. Physicians are responsible for diagnosing and developing treatment plans for anembryonic pregnancies. Nurses provide patient care, emotional support, and education. Pharmacists may be involved in prescribing or dispensing medications. All team members must respect patients' autonomy by providing clear information about their condition and available choices, including expectant management, medication, and surgery. Mental health professionals play a critical role in following up with patients and ensuring the appropriate mental health management of a possibly traumatic experience for patients.
Physicians, advanced care practitioners, nurses, and pharmacists should communicate and collaborate seamlessly to provide consistent patient-centered care. Confirming the diagnosis of an anembryonic pregnancy can be difficult by ultrasound at times. Communication with the radiologist, relaying hCG lab values and patient presentation, can help avoid a missed diagnosis of an ectopic pregnancy. The sonographer is also essential in accurately evaluating a patient to exclude an ectopic pregnancy appropriately. Patients presenting with complications on initial presentation or from treatment often present to the emergency department. Close communication between an emergency department clinician and an obstetric specialist includes providing a detailed, thorough patient history and physical exam. This particularly includes signs of sepsis and hemodynamic instability.
Regular team meetings, continuing education, and shared decision-making processes enhance team performance. Reducing the physical complications and emotional impact of these losses through a coordinated, patient-centered approach is essential for providing high-quality care. Recognizing the unique contributions of each team member and fostering a culture of mutual respect and trust further strengthens the team's ability to provide optimal care for patients with anembryonic pregnancies.
Media
(Click Image to Enlarge)
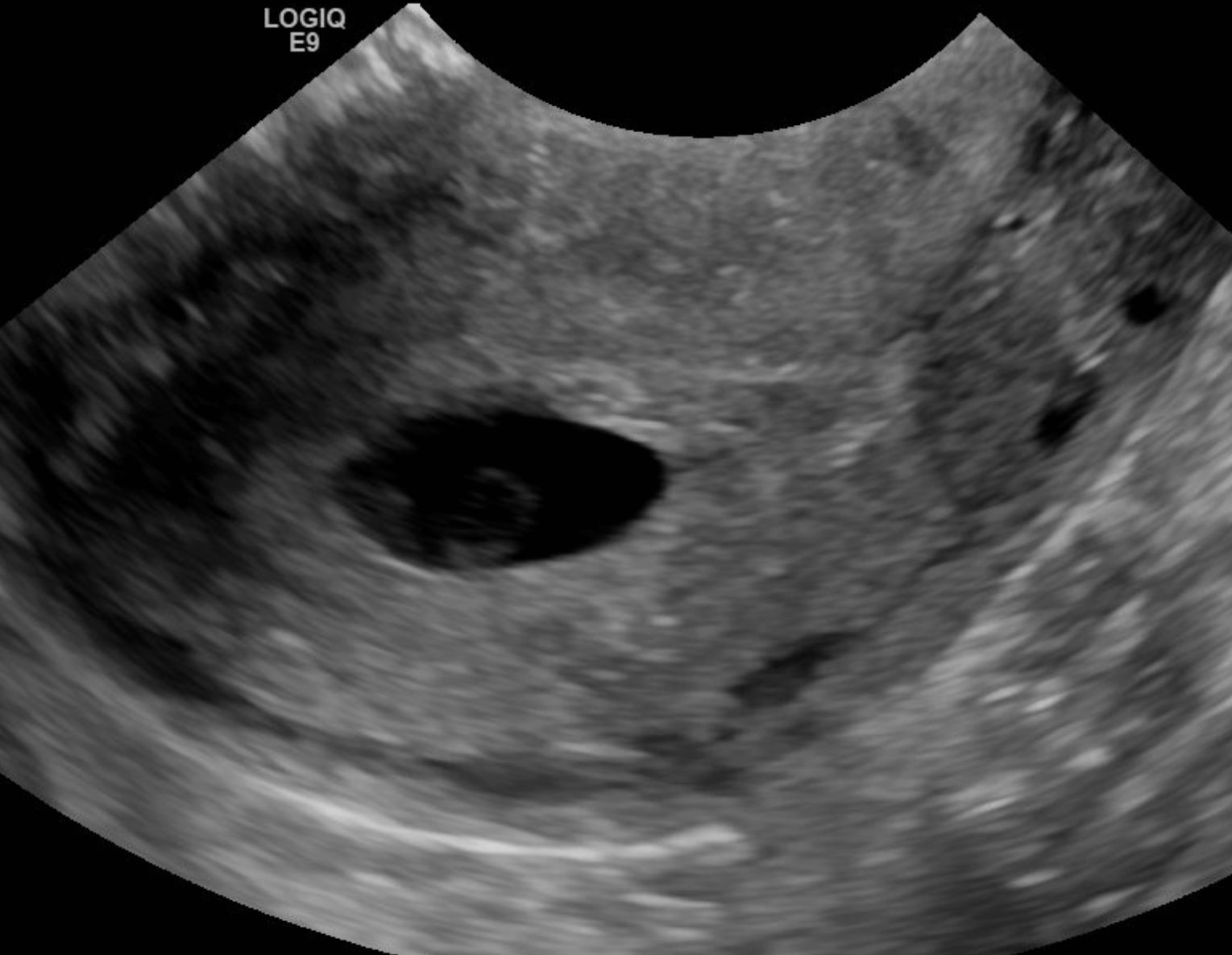
Anembryonic Pregnancy. A single sonographic image demonstrating a gestational sac with a yolk sac. No fetal pole is seen. This is representative of a blighted ovum.
Contributed by Dawood Tafti, MD
References
Macklon NS, Geraedts JP, Fauser BC. Conception to ongoing pregnancy: the 'black box' of early pregnancy loss. Human reproduction update. 2002 Jul-Aug:8(4):333-43 [PubMed PMID: 12206468]
Level 3 (low-level) evidenceGoldhaber MK, Fireman BH. The fetal life table revisited: spontaneous abortion rates in three Kaiser Permanente cohorts. Epidemiology (Cambridge, Mass.). 1991 Jan:2(1):33-9 [PubMed PMID: 2021664]
Level 2 (mid-level) evidenceMurugesu S, Braun E, Saso S, Bourne T. Predictors of successful expectant and medical management of miscarriage: A systematic review. Acta obstetricia et gynecologica Scandinavica. 2024 Dec:103(12):2348-2372. doi: 10.1111/aogs.14934. Epub 2024 Aug 9 [PubMed PMID: 39119791]
Level 1 (high-level) evidenceYin Y, Zhang T, Dai Y, Bao Y, Chen X, Lu X. The effect of plasma lead on anembryonic pregnancy. Annals of the New York Academy of Sciences. 2008 Oct:1140():184-9. doi: 10.1196/annals.1454.042. Epub [PubMed PMID: 18991916]
Hertig AT, Rock J. Searching for early fertilized human ova. Gynecologic investigation. 1973:4(3):121-39 [PubMed PMID: 4593973]
Jackson T, Watkins E. Early pregnancy loss. JAAPA : official journal of the American Academy of Physician Assistants. 2021 Mar 1:34(3):22-27. doi: 10.1097/01.JAA.0000733216.66078.ac. Epub [PubMed PMID: 33528169]
Sakko Y, Turesheva A, Gaipov A, Aimagambetova G, Ukybassova T, Marat A, Kaldygulova L, Amanzholkyzy A, Nogay A, Khamidullina Z, Mussenov Y, Almawi WY, Atageldiyeva K. Epidemiology of spontaneous pregnancy loss in Kazakhstan: A national population-based cohort analysis during 2014-2019 using the national electronic healthcare system. Acta obstetricia et gynecologica Scandinavica. 2023 Dec:102(12):1682-1693. doi: 10.1111/aogs.14669. Epub 2023 Sep 4 [PubMed PMID: 37667510]
Onsod P, Jaranasaksakul W, Chareonsirisuthigul T, Parinayok R, Rerkamnuaychoke B, Areesirisuk P. Chromosomal abnormalities study for anembryonic pregnancy by BACs-on-Beads technique. European journal of obstetrics, gynecology, and reproductive biology. 2024 Jul:298():31-34. doi: 10.1016/j.ejogrb.2024.04.041. Epub 2024 Apr 30 [PubMed PMID: 38705011]
Nikitina TV, Sazhenova EA, Tolmacheva EN, Sukhanova NN, Vasilyev SA, Lebedev IN. Comparative cytogenetics of anembryonic pregnancies and missed abortions in human. Vavilovskii zhurnal genetiki i selektsii. 2023 Mar:27(1):28-35. doi: 10.18699/VJGB-23-05. Epub [PubMed PMID: 36923481]
Level 2 (mid-level) evidenceBerglund G. Preparation of antiserum to an antigen of low molecular weight. Nature. 1965 May 1:206(983):523-4 [PubMed PMID: 4953500]
Level 3 (low-level) evidenceShekoohi S, Mojarrad M, Raoofian R, Ahmadzadeh S, Mirzaie S, Hassanzadeh-Nazarabadi M. Chromosomal study of couples with the history of recurrent spontaneous abortions with diagnosed blightded ovum. International journal of molecular and cellular medicine. 2013 Fall:2(4):164-8 [PubMed PMID: 24551808]
Robinson L, Gallos ID, Conner SJ, Rajkhowa M, Miller D, Lewis S, Kirkman-Brown J, Coomarasamy A. The effect of sperm DNA fragmentation on miscarriage rates: a systematic review and meta-analysis. Human reproduction (Oxford, England). 2012 Oct:27(10):2908-17. doi: 10.1093/humrep/des261. Epub 2012 Jul 12 [PubMed PMID: 22791753]
Level 2 (mid-level) evidenceCavalcante MB, Sarno M, Peixoto AB, Araujo Júnior E, Barini R. Obesity and recurrent miscarriage: A systematic review and meta-analysis. The journal of obstetrics and gynaecology research. 2019 Jan:45(1):30-38. doi: 10.1111/jog.13799. Epub 2018 Aug 28 [PubMed PMID: 30156037]
Level 1 (high-level) evidencePatki A, Chauhan N. An Epidemiology Study to Determine the Prevalence and Risk Factors Associated with Recurrent Spontaneous Miscarriage in India. Journal of obstetrics and gynaecology of India. 2016 Oct:66(5):310-5. doi: 10.1007/s13224-015-0682-0. Epub 2015 Mar 17 [PubMed PMID: 27486274]
Sundermann AC, Zhao S, Young CL, Lam L, Jones SH, Velez Edwards DR, Hartmann KE. Alcohol Use in Pregnancy and Miscarriage: A Systematic Review and Meta-Analysis. Alcoholism, clinical and experimental research. 2019 Aug:43(8):1606-1616. doi: 10.1111/acer.14124. Epub 2019 Jul 3 [PubMed PMID: 31194258]
Level 1 (high-level) evidenceAndersen LB, Dechend R, Karumanchi SA, Nielsen J, Joergensen JS, Jensen TK, Christesen HT. Early pregnancy angiogenic markers and spontaneous abortion: an Odense Child Cohort study. American journal of obstetrics and gynecology. 2016 Nov:215(5):594.e1-594.e11. doi: 10.1016/j.ajog.2016.06.007. Epub 2016 Jun 8 [PubMed PMID: 27287686]
Homan G, Brown S, Moran J, Homan S, Kerin J. Human chorionic gonadotropin as a predictor of outcome in assisted reproductive technology pregnancies. Fertility and sterility. 2000 Feb:73(2):270-4 [PubMed PMID: 10685527]
Level 2 (mid-level) evidenceMagnus MC, Wilcox AJ, Morken NH, Weinberg CR, Håberg SE. Role of maternal age and pregnancy history in risk of miscarriage: prospective register based study. BMJ (Clinical research ed.). 2019 Mar 20:364():l869. doi: 10.1136/bmj.l869. Epub 2019 Mar 20 [PubMed PMID: 30894356]
Regan L, Braude PR, Trembath PL. Influence of past reproductive performance on risk of spontaneous abortion. BMJ (Clinical research ed.). 1989 Aug 26:299(6698):541-5 [PubMed PMID: 2507063]
Zhang M, Lu X, Mi L, Song M, Wang L, Wang X. Investigation of amino acid profile alterations in maternal serum for early diagnosis of anembryonic pregnancy with high performance liquid chromatography-mass spectrometry. European journal of obstetrics, gynecology, and reproductive biology. 2024 Mar:294():49-54. doi: 10.1016/j.ejogrb.2024.01.007. Epub 2024 Jan 8 [PubMed PMID: 38215601]
Kim C, Barnard S, Neilson JP, Hickey M, Vazquez JC, Dou L. Medical treatments for incomplete miscarriage. The Cochrane database of systematic reviews. 2017 Jan 31:1(1):CD007223. doi: 10.1002/14651858.CD007223.pub4. Epub 2017 Jan 31 [PubMed PMID: 28138973]
Level 1 (high-level) evidenceZhang J, Gilles JM, Barnhart K, Creinin MD, Westhoff C, Frederick MM, National Institute of Child Health Human Development (NICHD) Management of Early Pregnancy Failure Trial. A comparison of medical management with misoprostol and surgical management for early pregnancy failure. The New England journal of medicine. 2005 Aug 25:353(8):761-9 [PubMed PMID: 16120856]
Level 1 (high-level) evidence