 Anatomy, Abdomen and Pelvis: Epigastric Artery
Anatomy, Abdomen and Pelvis: Epigastric Artery
Introduction
The primary arterial supply to the anterior abdominal wall is provided by the epigastric arteries. Three epigastric arteries supply the abdominal wall. The superficial epigastric artery perfuses the superficial fascial and cutaneous tissues of the abdominal wall. The superior (SEA) and inferior (IEA) epigastric arteries anastomose within the rectus sheath to provide circulation to the abdominal wall musculature. Embryologically, the superior and inferior epigastric vessels arise from anastomotic networks formed by intersegmental vessels during vasculogenesis and angiogenesis. Innervation of the abdominal wall includes lateral cutaneous branches of T7 to T12, as well as the iliohypogastric and ilioinguinal nerves, with femoral and obturator nerves coursing near the IEA in the pelvis. Anatomical variations include differences in IEA position relative to the midline and the presence of clinically significant variants, such as the corona mortis.
The epigastric arteries are critical to anterior abdominal wall perfusion and collateral circulation, particularly in patients with altered central arterial flow or prior abdominal wall surgery. In surgery, preservation of the SEA, IEA, and superficial epigastric artery during laparoscopic trocar placement, hernia repair, paracentesis, and flap-based reconstructions is a key surgical priority, as avoidance of vascular damage reduces hematoma formation, hemorrhage, and loss of reconstructive options. Understanding epigastric artery anatomy and function improves clinician performance during procedural planning and execution by enabling the identification of safe entry zones, reduction of iatrogenic vascular injury, and optimization of outcomes in both emergent and elective abdominal interventions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The SEA is 1 of 2 terminal branches of the internal thoracic (internal mammary) artery, which courses just lateral and posterior to the sternum. The internal thoracic artery divides into 2 terminal branches at the level of the 6th or 7th costal cartilage. The musculophrenic artery constitutes the 1st terminal branch and supplies the muscular portions of the diaphragm. The SEA constitutes the 2nd terminal branch, crosses the diaphragm, and descends along the anterior abdominal wall between the anterior surface of the transversus abdominis muscle and the posterior surface of the rectus sheath. The SEA supplies the rectus abdominis muscle bilaterally until it anastomoses with the IEA, typically at or near the umbilicus, with variation extending more inferiorly, depending on individual anatomy.[1]
The IEA branches from the external iliac artery superior to the inguinal ligament and curves superiorly beneath the peritoneum (see Image. Inguinal Region). The inferior epigastric vessels pass posterior to the spermatic cord as the vas deferens emerges posteriorly, with lateral relation to the artery at this level. The inferior epigastric vessels form the lateral boundary of the Hesselbach triangle. The rectus abdominis muscle and the inguinal ligament form the medial and inferior boundaries of the triangle, respectively.
The IEA ascends obliquely and medially along the margin of the deep inguinal ring while being enveloped by the lateral umbilical ligament. The IEA then pierces the transversalis fascia and continues to ascend superiorly and superficially until it becomes positioned posterior to the rectus abdominis after crossing the linea semicircularis. The IEA continues superiorly until it terminates by perforating the rectus abdominis muscle and branching approximately at the level of the umbilicus to form an anastomosis with the SEAs. Variability in this course is clinically relevant for surgical planning and intraoperative risk assessment.[2]
The superficial epigastric artery supplies the superficial fascia of the lower anterior abdominal wall, consistent with its superficial course and distribution. The superficial epigastric artery typically arises from the femoral artery approximately 1 cm inferior to the inguinal ligament, pierces the cribriform fascia, and ascends within the superficial fascial plane toward the umbilicus. The vessel usually terminates before reaching the umbilical level and may contribute to anastomoses with branches of the IEA after perforation of the rectus abdominis muscle.[3]
Epigastric veins accompany their corresponding arteries. The superior epigastric vein drains into the internal thoracic vein, the inferior epigastric vein drains into the external iliac vein, and the superficial epigastric vein drains into the great saphenous vein near its junction with the femoral vein or directly into the femoral vein.[4] The epigastric arterial and venous systems are bilaterally present and demonstrate near-symmetric distribution in the human body.
The regional lymphatic drainage follows venous pathways superficial to the Scarpa fascia. Lymphatic channels accompanying the superficial aspect of the superior epigastric veins above the umbilicus drain toward the anterior, or pectoral, group of axillary lymph nodes. Lymphatic channels accompanying the deep aspect of the superior epigastric veins drain toward the parasternal lymph nodes along the internal thoracic vessels. Lymphatic channels traveling with the superficial epigastric veins empty toward the superficial inguinal lymph nodes. Lymphatic channels running with the inferior epigastric veins drain toward lymph nodes surrounding the external iliac veins.[5]
No neural structures directly parallel the course of the epigastric arteries. However, clinically relevant nerves lie near these vessels. Lateral cutaneous branches of T7 to T12, along with iliohypogastric and ilioinguinal branches of L1, traverse the anterior abdominal wall from lateral to medial in a superficial plane near the skin, crossing the epigastric arterial system at near-perpendicular angles at respective dermatome levels. In the pelvic region, the femoral and obturator nerves course in proximity to the IEA.
Embryology
Angiogenesis begins at day 17 of embryonic development within the splanchnic mesoderm of the yolk sac wall, with subsequent contribution from paraxial mesoderm as vasculogenesis progresses. Hemangioblasts give rise to 2 major populations: primitive hematopoietic progenitor cells and endothelial precursor cells (EPCs), also known as angioblasts. Hematopoiesis originates in the yolk sac from extraembryonic mesoderm, while flattened EPCs initiate vasculogenesis within the embryonic disc. Hematopoietic stem cells arise from intraembryonic splanchnic mesoderm as blood islands, later migrating to the liver for expansion before relocating to lymphoid organs, such as bone marrow, as maturation progresses. Cellular derivatives ultimately populate the vascular system as arteries, veins, and capillaries.
EPCs form primitive vascular tubes that differentiate into arteries and veins, enabling blood circulation. EPC differentiation and maturation occur in response to locally secreted regulatory factors. Vessels form through coordinated vasculogenesis and angiogenesis. Flattened EPCs migrate, coalesce, and organize into primitive vascular cords during vasculogenesis. Endothelial buds sprout from preexisting vascular structures to form new vessels during angiogenesis. Vascular intussusception further remodels the vascular network through internal partitioning, followed by stabilization and maturation of vessel walls through intercalation.
As angiogenesis progresses, a primitive heart tube also begins formation at approximately day 18 of embryonic development. By week 4, embryonic body folding relocates the primitive heart tube into the ventral thorax, while the aortic arches develop and elongate in a craniocaudal sequence. Of importance is the paired dorsal aorta outflow system, which fuses in the midline by the end of the 4th week. The dorsal aorta subsequently develops ventral, lateral, and posterolateral branches.
The ventral branches are associated with the vitelline circulation in the yolk sac wall and are organized into foregut, midgut, and hindgut territories, later contributing to the gastrointestinal arterial system. Lateral branches of the descending dorsal aorta supply the suprarenal glands, gonads, and kidneys. Posterolateral branches arise from paraxial mesoderm between developing somites and subsequently fuse with the dorsal aorta. These posterolateral branches are known as intersegmental vessels and are present along cervical, thoracic, and lumbar regions by the end of the 3rd week of embryonic development. Intersegmental vessels include the intercostal arteries and veins, as well as vertebral arteries and veins. Intersegmental vessels expand their vascular network through multiple anastomoses formed via vasculogenesis and angiogenesis. The internal thoracic, superior epigastric, and inferior epigastric vessels arise among the anastomotic networks derived from intersegmental circulation.
Physiologic Variants
The SEA, IEA, internal thoracic, left and right subclavian, and right brachiocephalic arteries contribute to collateral circulation linking the thoracic and abdominal aorta. Progressive enlargement of these vessels occurs over time in severe distal arterial disease, aortic sclerosis, or coarctation of the aorta, thereby maintaining perfusion to the lower limbs.[6] Transection of the epigastric arteries in such cases may result in more severe hemorrhage and potential critical limb ischemia.
Anatomical variation among epigastric arterial branches is common. However, the corona mortis is one of the most clinically significant variants, identified in 77.27% of patients studied.[7] The corona mortis arises from the deep inferior epigastric system and establishes a connection with the external iliac and obturator arteries posterior and superior to the superior pubic rami. This vessel is clinically and surgically significant due to proximity to major pelvic vessels, with transection capable of producing life-threatening hemorrhagic shock.[8]
The course of the epigastric arteries along the anterior abdominal wall demonstrates interindividual variability. The SEA is located approximately 3 to 8.5 cm lateral to the midline bilaterally. The IEA is typically located 4 to 8 cm from the midline, independent of body fat distribution or anatomical level.[9] However, findings by Rao et al indicate that the distribution of the IEA is not consistently symmetric relative to the midline. The right IEA was reported at 3.2 to 6 cm from the midline, and the left IEA at 1.2 to 5 cm from the midline. The IEA follows a lateral-to-medial course as it ascends from the external iliac artery toward the rectus sheath and umbilicus.[10]
Surgical Considerations
The course of the epigastric arteries along the abdominal wall is a critical surgical consideration in multiple procedures, including trocar placement in laparoscopic surgery, percutaneous endoscopic gastrostomy (PEG) tube placement, inguinal hernia repair, paracentesis, and drain placement during cardiothoracic surgery. Disruption of the epigastric arteries may compromise future procedures that utilize the SEA as a perforator source, including trans–rectus abdominis muscle (TRAM) flap reconstruction and sternal reconstruction. Hemorrhage may result in abdominal wall hematoma formation, with subsequent postoperative complications including infection, incisional hernia formation, or significant blood loss, depending on the level of arterial transection.[11]
Although trocar and cannula placement is generally safe, injury to anterior abdominal wall vessels may occur, with higher susceptibility involving the IEA. Such injuries occur in approximately 3 per 1,000 laparoscopic cases (0.2%–2%). In these cases, bleeding may be controlled using direct pressure, transabdominal suture ligation, or tamponade with a Foley catheter balloon through the insertion site. Hemostasis may also be achieved using a 2-handed technique, with vessel compression or clamping in one hand and ligation, clipping, or coagulation in the other. Failure of these measures necessitates wound exploration, resulting in prolonged operative time, extended duration of anesthesia, or conversion to laparotomy, with associated delays in postoperative wound healing and increased risk of additional complications, as previously described.[12][13][14]
Transillumination techniques are commonly used by surgeons to visualize major abdominal wall vessels through the skin, thereby reducing the risk of trocar-related vascular injury. However, visualization is often limited in patients with darker skin pigmentation or elevated body mass index. A study by Quintet et al demonstrated successful vessel visualization using transillumination in only 63% of 103 patients studied. Computed tomography angiography is the preferred modality for preoperative vascular mapping, although its routine use is limited by cost considerations and exposure to ionizing radiation. Abdominal wall vascular injuries are generally manageable intraoperatively. Greater clinical value lies in detailed anatomical knowledge and accurate identification of safe and high-risk zones for instrument placement.
“Safety” and “danger” zones of the epigastric arterial system have been defined across multiple cadaveric studies from different countries. Bhatti et al defined the “danger zone” of the SEA as 3 to 8.5 cm lateral to the midline and the “safety zone” as extending from the midline to 3 cm bilaterally adjacent to the midline of the abdomen.
Saber et al reported that IEAs are located 4 to 8 cm from the midline, independent of body fat habitus. Rao et al in India, as previously noted, reported that the arterial distribution is not equidistant from the midline between the left and right sides of the abdomen. The suggested “safety zone” of the IEA was 0 to 3.2 cm from the midline and 0 to 1.2 cm on the right. The IEA was observed to lie more laterally on the right abdominal wall compared with the left, particularly as it ascends toward the umbilicus. The “danger zone,” as defined by Rao et al, was 3.2 to 6 cm from the midline on the right and 1.2 to 5 cm from the midline on the left.
The midline is recognized as an avascular plane. The main stem of the IEA may be avoided when trocars are inserted at approximately 2/3 of the distance between the midline and the anterior superior iliac spine. Branching of the IEA is least prominent in the lower abdomen, lateral to the artery.[15]
Clinical Significance
Understanding the significance of the epigastric arteries is essential in surgical and clinical practice. Preservation of these vessels during common laparoscopic procedures is critical to reduce bleeding risk and procedure-related complications, as well as maintain future reconstructive options, including trans-rectus abdominis muscle flap reconstruction.[16][17][18][19] The epigastric arteries may provide highly versatile conduits for current and future flap and graft-based procedures in patients with minimal dependence on epigastric arterial anastomotic flow, such as in congenital conditions like coarctation of the aorta.
Media
(Click Image to Enlarge)
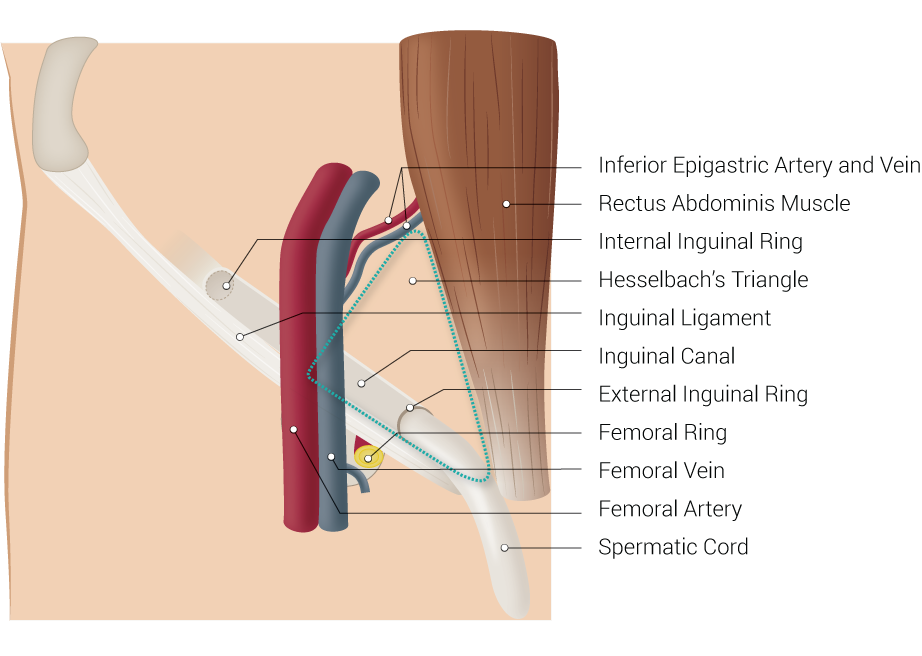
Inguinal Region. This image demonstrates the anatomic relationships between the inferior epigastric artery and vein, rectus abdominis muscle, internal inguinal ring, Hesselbach triangle, inguinal ligament, inguinal canal, external inguinal ring, femoral ring, femoral vein, femoral artery, and spermatic cord.
Illustrated by B Palmer
References
Bhatti AF, Iqbal S, Lee TC. Variation in surface marking of superior epigastric vessels. A guide to safe laparoscopic port insertion. The surgeon : journal of the Royal Colleges of Surgeons of Edinburgh and Ireland. 2008 Feb:6(1):50-2 [PubMed PMID: 18318089]
Joy P, Prithishkumar IJ, Isaac B. Clinical anatomy of the inferior epigastric artery with special relevance to invasive procedures of the anterior abdominal wall. Journal of minimal access surgery. 2017 Jan-Mar:13(1):18-21. doi: 10.4103/0972-9941.181331. Epub [PubMed PMID: 27251822]
Rozen WM, Chubb D, Grinsell D, Ashton MW. The variability of the Superficial Inferior Epigastric Artery (SIEA) and its angiosome: A clinical anatomical study. Microsurgery. 2010 Jul:30(5):386-91. doi: 10.1002/micr.20750. Epub [PubMed PMID: 20058298]
Level 2 (mid-level) evidenceJoseph A, Scharbach S, Samant H. Anatomy, Anterolateral Abdominal Wall Veins. StatPearls. 2026 Jan:(): [PubMed PMID: 29939686]
Hsu MC, Itkin M. Lymphatic Anatomy. Techniques in vascular and interventional radiology. 2016 Dec:19(4):247-254. doi: 10.1053/j.tvir.2016.10.003. Epub 2016 Oct 8 [PubMed PMID: 27993319]
Yurdakul M, Tola M, Ozdemir E, Bayazit M, Cumhur T. Internal thoracic artery-inferior epigastric artery as a collateral pathway in aortoiliac occlusive disease. Journal of vascular surgery. 2006 Apr:43(4):707-13 [PubMed PMID: 16616225]
Pungpapong SU, Thum-umnauysuk S. Incidence of corona mortis; preperitoneal anatomy for laparoscopic hernia repair. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2005 Sep:88 Suppl 4():S51-3 [PubMed PMID: 16623002]
Al Talalwah W. A new concept and classification of corona mortis and its clinical significance. Chinese journal of traumatology = Zhonghua chuang shang za zhi. 2016 Oct 1:19(5):251-254 [PubMed PMID: 27780502]
Saber AA, Meslemani AM, Davis R, Pimentel R. Safety zones for anterior abdominal wall entry during laparoscopy: a CT scan mapping of epigastric vessels. Annals of surgery. 2004 Feb:239(2):182-5 [PubMed PMID: 14745325]
Rao MP, Swamy V, Arole V, Mishra P. Study of the course of inferior epigastric artery with reference to laparoscopic portal. Journal of minimal access surgery. 2013 Oct:9(4):154-8. doi: 10.4103/0972-9941.118826. Epub [PubMed PMID: 24250060]
Vasquez JM, Demarque AM, Diamond MP. Vascular complications of laparoscopic surgery. The Journal of the American Association of Gynecologic Laparoscopists. 1994 Feb:1(2):163-7 [PubMed PMID: 9050482]
Level 3 (low-level) evidenceNordestgaard AG, Bodily KC, Osborne RW Jr, Buttorff JD. Major vascular injuries during laparoscopic procedures. American journal of surgery. 1995 May:169(5):543-5 [PubMed PMID: 7747836]
Spitzer M, Golden P, Rehwaldt L, Benjamin F. Repair of laparoscopic injury to abdominal wall arteries complicated by cutaneous necrosis. The Journal of the American Association of Gynecologic Laparoscopists. 1996 May:3(3):449-52 [PubMed PMID: 9050673]
Level 3 (low-level) evidenceMechchat A, Bagan P. Management of major vascular complications of laparoscopic surgery. Journal of visceral surgery. 2010 Jun:147(3):e145-53. doi: 10.1016/j.jviscsurg.2010.08.002. Epub 2010 Sep 6 [PubMed PMID: 20822965]
Epstein J, Arora A, Ellis H. Surface anatomy of the inferior epigastric artery in relation to laparoscopic injury. Clinical anatomy (New York, N.Y.). 2004 Jul:17(5):400-8 [PubMed PMID: 15176037]
Pignatti M, Pinto V, Giorgini FA, Lozano Miralles ME, Cannamela G, D'Arpa S, Cipriani R, De Santis G. Meta-analysis of the effects of venous super-drainage in deep inferior epigastric artery perforator flaps for breast reconstruction. Microsurgery. 2021 Feb:41(2):186-195. doi: 10.1002/micr.30682. Epub 2020 Nov 10 [PubMed PMID: 33170970]
Level 1 (high-level) evidenceCheung MY, Chae MP, Shepherd HM, Hsieh F, Soliman BAB. Deep Inferior Epigastric Artery (DIEP) anomaly in autologous breast reconstruction. ANZ journal of surgery. 2023 Apr:93(4):1082-1083. doi: 10.1111/ans.18113. Epub 2022 Oct 17 [PubMed PMID: 36251399]
Soliman B, Sedaghat N, Yuen L, Harish V, French J. Laparoscopic-assisted deep inferior epigastric artery perforator (DIEP) flap in breast reconstruction. ANZ journal of surgery. 2022 Sep:92(9):2365-2367. doi: 10.1111/ans.17485. Epub 2022 Jan 24 [PubMed PMID: 35075753]
Zhu Y, Yoo H, Min S, Chang H. Efficacy of superficial inferior epigastric vein superdrainage in free TRAM and DIEP flap: An indocyanine green angiography study of 68 cases. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2023 Sep:84():385-391. doi: 10.1016/j.bjps.2023.06.006. Epub 2023 Jun 8 [PubMed PMID: 37399658]
Level 3 (low-level) evidence