Introduction
Apraxia of lid opening (ALO), also referred to as apraxia of eyelid opening, is a relatively uncommon disorder characterized by bilateral difficulty initiating eyelid elevation despite normal levator palpebrae superioris function and intact oculomotor innervation. Affected patients are unable to voluntarily reopen their eyes in the absence of primary muscular or neuromuscular abnormalities, often despite sustained contraction of the frontalis muscle. The term is somewhat of a misnomer, as the condition rarely represents true apraxia.[1] ALO is distinct from blepharospasm, in which involuntary orbicularis oculi contraction forces eyelid closure, and from ptosis, which reflects eyelid droop due to muscle weakness or mechanical factors.[2] Although ALO may occur as an isolated phenomenon, it is more commonly associated with underlying neurologic disease.[3]
Max Heinrich Lewandowsky first described ALO in 1907 in his essay "Über Apraxie des Lidschlusses." Subsequent early reports were limited, including cases described by Schilder in 1927 and Riese in 1930, with additional series reported by Goldstein and Cogan in 1965.[4] ALO is often underrecognized or misdiagnosed due to its clinical subtlety and lack of pathognomonic findings.
In addition to its association with neurodegenerative disorders, ALO has also been reported in patients with focal dystonias, structural brain lesions, and metabolic or toxic encephalopathies. Neuroimaging studies have suggested abnormalities within the basal ganglia–thalamocortical circuits, which play a crucial role in the initiation and coordination of voluntary movements. Functional imaging techniques such as positron emission tomography and functional magnetic resonance imaging have demonstrated altered activity in the supplementary motor area and frontal cortex in affected individuals. These findings further support the concept that ALO represents a disorder of motor planning and execution rather than a primary muscular dysfunction.[5][6]
ALO frequently coexists with blepharospasm as part of the blepharospasm-apraxia syndrome, where patients exhibit involuntary eyelid closure followed by difficulty reopening the eyelids. This combination can significantly impair visual function and quality of life, particularly in older patients with Parkinsonian syndromes. The prevalence of ALO among patients with Parkinson disease has been reported to range between 2% and 6%, although higher rates have been described in advanced stages of the disease and in those receiving dopaminergic therapy.[7]
From an anatomical standpoint, eyelid opening requires coordinated activation of the levator palpebrae superioris muscle and simultaneous inhibition of the orbicularis oculi muscle. This process is mediated through complex supranuclear pathways involving the basal ganglia, brainstem reticular formation, and cortical motor areas. Disruption of these inhibitory pathways may result in persistent orbicularis activity or failure of levator activation, leading to the characteristic inability to initiate eyelid opening seen in ALO.[8]
Clinically, patients often describe episodes where they are aware of their inability to open their eyes despite attempting to do so. These episodes may last from seconds to minutes and can be temporarily relieved by sensory tricks such as touching the eyelids, lifting the brows, or manually elevating them. Such maneuvers, often referred to as “geste antagoniste,” are commonly observed in dystonic disorders and may reflect temporary modulation of abnormal neural circuits.[9][10]
The natural history of ALO varies depending on the underlying etiology. In idiopathic cases, symptoms may remain stable or fluctuate over time. However, when associated with progressive neurological conditions such as Parkinson disease or progressive supranuclear palsy, ALO may worsen as the underlying disease advances. Early recognition is therefore essential, as appropriate management of the underlying neurological disorder may reduce symptom severity and improve functional outcomes.[11][12]
Although ALO is considered uncommon, it may be underrecognized in clinical practice due to its overlapping features with other eyelid disorders. Increased awareness among ophthalmologists, neurologists, and movement disorder specialists is essential to ensure timely diagnosis and appropriate management. Continued research into the neurophysiological mechanisms underlying ALO may help clarify its pathogenesis and lead to more targeted therapeutic approaches.[13]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
In many patients, apraxia of lid opening (ALO) develops as part of a broader neurological disorder affecting motor planning and execution (see Table 1). Dysfunction of basal ganglia circuits, particularly the connections between the globus pallidus, thalamus, and supplementary motor cortex, is believed to play a central role in the development of ALO. Disruption of these pathways interferes with the coordinated inhibition of the orbicularis oculi muscle and activation of the levator palpebrae superioris muscle required for voluntary eyelid opening.[14]
Neurodegenerative diseases are among the most frequently reported systemic associations. ALO is commonly observed in disorders such as Parkinson disease, progressive supranuclear palsy (PSP), corticobasal degeneration, and multiple system atrophy. In these conditions, degeneration of basal ganglia structures leads to impaired initiation of voluntary movements, including eyelid opening. In particular, ALO is considered a characteristic feature of PSP and may assist clinicians in differentiating it from other Parkinsonian syndromes.[15] Additional neurodegenerative and movement disorders reported in association with ALO include Huntington disease, dystonia-related Parkinsonism, motor neuron diseases, and Shy-Drager syndrome.
Structural lesions of the central nervous system (CNS) may also lead to ALO. Tumors, traumatic brain injuries, demyelinating plaques, or vascular insults involving the frontal lobes, basal ganglia, or brainstem can disrupt neural pathways responsible for eyelid movement. Case reports have described ALO in association with lesions of the medial frontal cortex and the upper brainstem, highlighting the importance of supranuclear control mechanisms.[16] Vascular etiologies, including stroke affecting these regions, represent an important subset of structural causes.[17]
Drug-induced ALO has been reported with medications that influence dopaminergic pathways. Dopamine antagonists, antipsychotic agents, and certain mood stabilizers may trigger dystonic reactions or interfere with basal ganglia function, leading to impaired eyelid opening. Similarly, exposure to neurotoxins affecting dopaminergic neurons has been implicated in rare cases.[18] Reported agents include lithium, sulpiride, and 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine.[19]
Infectious, metabolic, autoimmune, and toxic systemic conditions may also contribute to ALO through effects on CNS function. CNS infections, including viral encephalitis, bacterial meningitis, and prion diseases, have been associated with ALO.[20] Metabolic disorders and toxic exposures, including environmental toxins and heavy metals, may disrupt neural pathways involved in eyelid movement.[21][22] Autoimmune conditions affecting the CNS, such as multiple sclerosis or autoimmune encephalitis, have also been reported in association with ALO.[21][23]
In addition to neurological causes, ocular and periocular conditions may contribute to symptoms that mimic or exacerbate ALO. Chronic ocular surface irritation, photophobia, or severe blepharospasm may lead to secondary difficulty opening the eyelids. Differentiating these conditions from true ALO is essential because the underlying pathophysiology and management strategies differ significantly.[24] Associated ocular conditions include infectious and inflammatory processes such as keratitis, blepharitis, dacryocystitis, and conjunctivitis, as well as autoimmune conditions such as keratoconjunctivitis sicca (eg, from Sjögren disease).[19] Mechanical and eyelid structural abnormalities, including ptosis and dermatochalasis, may also present with impaired eyelid opening and should be distinguished from ALO.[25][26]
Although most cases occur secondary to neurological disease or focal dystonia, truly idiopathic cases of ALO have also been described. Idiopathic focal dystonia remains one of the most commonly reported underlying etiologies. In such patients, no identifiable neurological or structural cause is found despite thorough clinical and radiological evaluation. These cases are believed to represent a primary dysfunction of eyelid motor control circuits.[27]
Table 1. Etiological Classification of Apraxia of Lid Opening
|
Etiological Category |
Examples |
Pathophysiological Mechanism |
|
Idiopathic/Primary dystonia |
Idiopathic ALO, benign essential blepharospasm |
Dysfunction of basal ganglia motor circuits affecting eyelid opening control |
|
Neurodegenerative disorders |
Parkinson disease, PSP, Huntington disease, corticobasal degeneration, multiple system atrophy |
Degeneration of the basal ganglia and motor planning pathways |
|
Structural CNS lesions |
Brain tumors, traumatic brain injury, frontal lobe lesions, basal ganglia infarction, brainstem lesions |
Disruption of supranuclear eyelid control pathways |
|
Drug-induced causes |
Lithium, sulpiride, neuroleptics, dopamine antagonists, MPTP exposure |
Dopaminergic pathway dysfunction causing dystonia or motor planning impairment |
|
Infectious causes |
Viral encephalitis, bacterial meningitis, and prion disease |
Inflammatory damage to neural circuits controlling eyelid movement |
|
Metabolic disorders |
Wilson disease, hepatic encephalopathy, and electrolyte disturbances |
Metabolic dysfunction affecting central motor pathways |
|
Autoimmune diseases |
Multiple sclerosis, autoimmune encephalitis, Sjögren syndrome |
Immune-mediated neural injury affecting motor control circuits |
|
Vascular causes |
Stroke, cerebral hemorrhage, ischemic basal ganglia lesions |
Vascular compromise affecting eyelid motor pathways |
|
Ocular or periocular conditions |
Severe blepharospasm, ocular surface disease, dermatochalasis, ptosis |
Secondary functional impairment of eyelid opening |
ALO, apraxia of lid opening; CNS, central nervous system; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine; PSP, progressive supranuclear palsy
Epidemiology
ALO is considered an uncommon neurological phenomenon, and its precise epidemiological burden remains difficult to quantify because it frequently occurs secondary to other neurological disorders such as Parkinson disease, progressive supranuclear palsy (PSP), or benign essential blepharospasm (see Table 2). Consequently, many epidemiological studies report ALO as part of the broader spectrum of eyelid dystonias rather than as a distinct condition (see Image. Epidemiology of Apraxia of Lid Opening).[15] Much of the available epidemiologic data are therefore extrapolated from studies of blepharospasm and related focal dystonias.
ALO most commonly affects middle-aged and older individuals, typically presenting in the fifth to seventh decades of life, paralleling the age distribution of the neurodegenerative diseases with which it is frequently associated. This finding is consistent with epidemiologic data from benign essential blepharospasm, which demonstrate a peak incidence between 50 and 60 years of age.[28] Cases occurring in younger patients are rare and are usually linked to structural brain lesions, genetic disorders, or secondary dystonic syndromes.[16]
Sex distribution studies indicate a slight female predominance, particularly when ALO occurs in association with benign essential blepharospasm or focal dystonia. This sex bias may reflect hormonal influences, differences in health-seeking behavior, or the higher prevalence of dystonia in women observed in several epidemiological studies.[24] Similarly, blepharospasm has been reported to occur more frequently in women (0.12%) than in men (0.07%).[28]
Geographically, most epidemiological data originate from North America, Europe, and East Asia, where movement disorder registries and neuro-ophthalmology clinics have reported higher recognition rates. However, the true prevalence is likely underestimated worldwide because ALO is frequently misdiagnosed as ptosis, blepharospasm, or functional eyelid disorders. Increased awareness among ophthalmologists and neurologists has improved diagnostic accuracy in recent years.[6]
Patients with neurodegenerative disorders represent the largest identifiable subgroup. In Parkinson disease, ALO has been reported in approximately 2% to 6% of patients, whereas in PSP, the prevalence may be significantly higher. In addition, patients with blepharospasm may develop secondary ALO as part of blepharospasm-apraxia syndrome, which can significantly impair visual function and quality of life.[29] ALO may also progress over time, and within months to several years, the condition can result in substantial functional impairment, including visual disability and reduced independence.
Occupational and environmental factors may also contribute indirectly to the epidemiology of eyelid movement disorders. Chronic ocular surface irritation, prolonged screen exposure, and environmental stressors may exacerbate underlying dystonic tendencies. These factors may partly explain the higher prevalence of eyelid dystonias observed in urban populations.[30] Increased risk has also been associated with certain comorbid conditions, including dyslipidemia, parasomnias, psychiatric disorders (eg, depression, anxiety, and obsessive-compulsive disorder), dry eye-related diseases (idiopathic or associated with Sjögren syndrome), and, to a lesser extent, Parkinson disease and rosacea.[31]
Table 2. Epidemiological Characteristics of Apraxia of Lid Opening
|
Epidemiological Factor |
Observations |
|
Age distribution |
Most common in individuals aged 50–70 years |
|
Sex distribution |
Slight female predominance |
|
Associated neurological disorders |
Parkinson disease, progressive supranuclear palsy, Huntington disease |
|
Association with dystonia |
Frequently occurs with benign essential blepharospasm |
|
Prevalence in Parkinson disease |
Approximately 2%–6% of patients |
|
Geographic distribution |
Most reported cases from North America, Europe, and East Asia |
|
Urban vs rural prevalence |
Higher recognition in urban populations |
|
Risk factors |
Neurodegenerative disease, focal dystonia, ocular surface irritation |
Pathophysiology
Apraxia of lid opening (ALO) is a disorder characterized by difficulty initiating lid elevation despite normal voluntary and reflex blinking. The pathophysiology of ALO is not entirely understood, but several mechanisms are thought to contribute to the condition (see Table 3). These mechanisms largely reflect dysfunction within corticothalamic, basal ganglia, and cranial nerve circuits involved in eyelid control, consistent with impairment of supranuclear motor pathways (see Image. Neural Mechanisms of Apraxia of Lid Opening).[32]
- Basal ganglia dysfunction: The basal ganglia play a critical role in the initiation and control of movement. In ALO, dysfunction within the basal ganglia circuitry, particularly in pathways involving the globus pallidus, is considered a significant factor. Nigrostriatal pathways may project to premotor regions responsible for eyelid coordination, further supporting a role for basal ganglia output in eyelid motor control.[32] This dysfunction can result from degenerative diseases, structural lesions, or neurochemical imbalances.[33]
- Supranuclear inhibition: ALO is thought to result from a failure to inhibit the tonic activity of the orbicularis oculi muscle, which closes the eyelids. Usually, voluntary lid opening involves a complex neural network that includes supranuclear pathways. Disruption of these pathways can impair the ability to overcome the orbicularis oculi's tonic contraction, making lid elevation difficult.[25]
- Levodopa sensitivity: Evidence suggests that ALO may be responsive to levodopa treatment in some cases, particularly when associated with Parkinson disease. This responsiveness implies a possible involvement of dopaminergic pathways in the pathophysiology of ALO.[34] At the biochemical level, abnormal dopamine neurotransmission likely contributes to disordered blinking and eyelid muscle activation.[35]
- Frontal lobe function: The frontal lobe, particularly the prefrontal cortex, is involved in planning and executing voluntary movements, including eyelid opening. Damage or dysfunction in this area can impair the ability to initiate lid opening, as seen in ALO.[36] Neuroimaging and electrophysiological studies have implicated both motor and nonmotor regions of the frontal lobe, supporting the concept of ALO as a disorder of motor intention in which the willed action does not translate into effective movement.[32]
- Abnormal blink reflex modulation: ALO may also be related to abnormalities in the blink reflex and its modulation. The reflex should be inhibited during voluntary lid opening, but this inhibition might be compromised in ALO.[37] Structures involved in the trigeminal blink reflex arc (including sensorimotor cortical regions, the substantia nigra pars reticulata, and brainstem motor nuclei) have been implicated in this process.[32]
- Sensorimotor integration: ALO can be associated with disruption of sensorimotor integration, the process by which the brain integrates sensory feedback with motor commands to produce smooth, coordinated movements.[38]
- Neurotransmitter imbalance: An imbalance in various neurotransmitters, including dopamine, may contribute to ALO, with changes in the cholinergic, serotonergic, and gamma-aminobutyric acid-ergic systems.[35]
- Neuromuscular anomalies: While not a primary factor, eyelid neuromuscular anomalies can contribute to difficulty opening the lid, especially when coexisting blepharospasm or ptosis is present.[25] These anomalies represent secondary contributors rather than primary pathophysiologic mechanisms.[35]
- Psychogenic factors: Although ALO is primarily a neurologic disorder, psychogenic factors have been considered in some cases, particularly when no clear neurologic cause can be identified.[39]
- Medication effects: Certain medications, especially those with neuromuscular blocking properties, can induce or exacerbate ALO. Understanding the adverse-effect profile of such medications is important for the clinical assessment of the condition.[40]
The combination of these factors results in the clinical presentation of ALO, in which patients are unable to open their eyelids at will despite having the necessary muscular function. Due to the disorder's complexity and overlap with other movement disorders, the exact pathophysiological mechanisms may vary between patients, and further research is needed to fully understand this condition.
Table 3. Key Pathophysiological Mechanisms in Apraxia of Lid Opening
|
Pathophysiological Mechanism |
Neuroanatomical Structures Involved |
Mechanism |
Clinical Implication |
|
Basal ganglia dysfunction |
Globus pallidus, substantia nigra, striatum |
Impaired motor initiation due to abnormal basal ganglia output |
Difficulty initiating voluntary eyelid elevation |
|
Supranuclear control failure |
Corticothalamic pathways, supplementary motor area |
Failure to inhibit tonic orbicularis oculi activity |
Persistent eyelid closure despite voluntary effort |
|
Frontal lobe involvement |
Prefrontal cortex, premotor cortex |
Impaired motor planning and execution |
Delayed or absent eyelid opening |
|
Blink reflex dysregulation |
Trigeminal nerve, facial nerve, brainstem nuclei |
Abnormal blink reflex inhibition during voluntary lid opening |
Interference with coordinated eyelid movement |
|
Dopaminergic dysfunction |
Nigrostriatal pathway |
Dopamine deficiency affects motor circuits |
Association with Parkinson disease and levodopa responsiveness |
|
Sensorimotor integration impairment |
Sensorimotor cortex, thalamus |
Disrupted coordination between sensory feedback and motor commands |
Irregular or effortful eyelid opening |
|
Neurotransmitter imbalance |
Dopamine, gamma-aminobutyric acid, and serotonin systems |
Abnormal neural excitability affecting eyelid control |
Variable clinical severity |
|
Neuromuscular contribution |
Levator palpebrae superioris, orbicularis oculi |
Secondary involvement in dystonia or ptosis |
Exacerbation of eyelid opening difficulty |
Histopathology
Although ALO is primarily considered a functional neurological disorder rather than a structural muscular pathology, histopathological findings may be observed in the central nervous system structures involved in eyelid motor control, particularly when ALO occurs secondary to neurodegenerative diseases (see Table 4).[41] Postmortem studies and neuropathological analyses in such patients often reveal abnormalities in the basal ganglia, brainstem nuclei, and frontal lobes, particularly the prefrontal cortex, all of which are key components of the neural circuitry regulating voluntary eyelid movement (see Image. Histopathological Changes in Apraxia of Lid Opening).[30][42] Importantly, ALO does not typically demonstrate primary histopathological abnormalities within the eyelid musculature itself, as the disorder reflects impaired motor control rather than intrinsic muscle disease.[25]
In patients with Parkinson disease, histopathology frequently demonstrates loss of dopaminergic neurons in the substantia nigra pars compacta, accompanied by Lewy body deposition composed of α-synuclein aggregates. These changes disrupt the nigrostriatal pathway, impairing basal ganglia modulation of voluntary movement, including eyelid opening.[15] Similar findings may be observed in other neurodegenerative conditions associated with ALO, in which neuronal loss and protein aggregation contribute to dysfunction of motor planning circuits.[43]
Also, in progressive supranuclear palsy, neuropathological examinations reveal tau-positive neurofibrillary tangles and neuronal loss in the basal ganglia, subthalamic nucleus, and brainstem, particularly in midbrain structures responsible for ocular and eyelid movement control.[44] These changes are often accompanied by gliosis and degeneration within basal ganglia circuits, further impairing supranuclear control of voluntary movement.[33] These findings contribute to disruptions in motor planning and initiation pathways, which are central to the development of ALO in affected patients.
Microscopic alterations may also include reactive gliosis, neuronal loss, and synaptic dysfunction within the cortico-basal ganglia-thalamic circuits, which are critical for coordinating voluntary motor initiation. Alterations in synaptic density or number within these circuits have also been proposed, although such changes are typically identifiable only through specialized ultrastructural or molecular studies.[45] Although these findings are not specific to ALO, they support the hypothesis that the disorder arises from disruption of higher-order motor planning pathways rather than intrinsic eyelid muscle pathology.[30] Additional involvement of brainstem nuclei, which contribute to reflexive and automatic eyelid movements, has also been described in some cases.[46]
Advanced molecular studies have suggested that dysregulation of dopaminergic, gamma-aminobutyric acid-ergic, and cholinergic neurotransmitter systems may further contribute to abnormal neural excitability and impaired motor control within these circuits. These neurochemical alterations are not typically identifiable on routine histopathological examination but may be demonstrated through specialized molecular or functional studies.[47] Consequently, histopathological findings in ALO often reflect the underlying neurological disorder rather than the eyelid disorder itself.[18]
Table 4. Histopathological Findings Associated With Apraxia of Lid Opening
|
Structure |
Histopathological Findings |
Associated Disorders |
Clinical Relevance |
|
Substantia nigra |
Loss of dopaminergic neurons, Lewy bodies |
Parkinson disease |
Impaired basal ganglia motor control |
|
Basal ganglia |
Neuronal loss, gliosis |
Parkinson disease, dystonia |
Disruption of movement initiation |
|
Subthalamic nucleus |
Tau deposition |
Progressive supranuclear palsy |
Abnormal motor modulation |
|
Brainstem nuclei |
Degeneration of motor nuclei |
PSP, neurodegenerative diseases |
Impaired blink reflex and eyelid control |
|
Frontal cortex |
Cortical neuronal degeneration |
Frontotemporal degeneration |
Defective motor planning |
|
Synaptic circuits |
Synaptic loss and neurotransmitter imbalance |
Movement disorders |
Altered sensorimotor integration |
|
Eyelid muscles |
Typically normal histology |
Primary ALO |
Confirms neurologic origin |
ALO, apraxia of lid opening; PSP, progressive supranuclear palsy
Toxicokinetics
Toxicokinetics is generally not a central component in the pathogenesis of ALO because the disorder primarily results from dysfunction of neural circuits that control voluntary eyelid movement rather than from direct toxic injury to eyelid tissues. However, toxicokinetic mechanisms become clinically relevant when ALO occurs secondary to exposure to certain medications or neurotoxins that interfere with neurotransmission in the basal ganglia (see Table 5).[6] Several pharmacologic agents have been implicated in the development of dystonic eyelid disorders, including dopamine receptor antagonists, antipsychotic medications, lithium, and sulpiride. These drugs can alter dopaminergic signaling in the nigrostriatal pathway, impairing the modulation of motor control circuits responsible for eyelid opening. The toxicokinetic behavior of these agents—particularly their absorption, distribution within the central nervous system, and elimination—may influence the onset and severity of symptoms (see Image. Toxicokinetic Mechanisms in Apraxia of Lid Opening).[8]
Neurotoxins such as 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) provide additional insights into the toxicokinetic mechanisms underlying basal ganglia dysfunction. After systemic exposure, MPTP crosses the blood–brain barrier, where it is metabolized into the toxic compound 1-methyl-4-phenylpyridinium, which selectively damages dopaminergic neurons within the substantia nigra. This neurotoxic process disrupts normal basal ganglia circuitry and may lead to movement abnormalities, including eyelid motor dysfunction.[10]
In drug-induced cases, symptoms of ALO may improve after dose reduction or discontinuation of the offending agent. This clinical finding highlights the importance of medication review in patients presenting with new-onset eyelid movement disorders. Because toxicokinetic processes vary depending on the specific drug involved, clinicians should consider factors such as drug half-life, metabolic pathways, and cumulative exposure when evaluating potential toxic etiologies.[16]
Table. Toxicokinetic Agents Associated With Apraxia of Lid Opening
|
Agent |
Toxicokinetic Mechanism |
Target Structure |
Clinical Effect |
|
Lithium |
CNS accumulation alters neurotransmission |
Basal ganglia |
Dystonia or eyelid movement disorders |
|
Sulpiride |
Dopamine receptor blockade |
Nigrostriatal pathway |
Drug-induced dystonia |
|
Antipsychotics (dopamine antagonists) |
Inhibition of dopamine signaling |
Basal ganglia circuits |
Extrapyramidal symptoms |
|
MPTP neurotoxin |
Conversion to MPP+ causes neuronal degeneration |
Substantia nigra |
Parkinsonian motor dysfunction |
|
Neuroleptic drugs |
Chronic dopaminergic blockade |
Motor control pathways |
Blepharospasm and ALO-like symptoms |
ALO, apraxia of lid opening; CNS, central nervous system; MPP+, 1-methyl-4-phenylpyridinium; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine
History and Physical
A careful clinical history is essential to distinguish ALO from other eyelid movement disorders (see Image. Clinical Assessment Pathway for Apraxia of Lid Opening). Patients often describe episodes in which they are unable to initiate eyelid opening after voluntary closure, despite preserved consciousness and normal ocular sensation. Symptoms most commonly occur immediately after voluntary eye closure or blinking and may be accompanied by a subjective sensation of periorbital contraction.
Patients may also notice the symptoms upon awakening or after periods of sustained eye closure. The symptoms may fluctuate throughout the day and are frequently exacerbated by fatigue, emotional stress, or prolonged visual tasks such as reading or computer use. Some patients report transient improvement with tactile stimulation of the eyelid or brow (eg, geste antagoniste), or they may employ compensatory maneuvers such as manually lifting the eyelids, exaggerated facial movements, or neck extension, reflecting the abnormal sensorimotor integration.[27][29][48]
Functional impairment is often significant. Patients may experience temporary functional blindness, particularly during activities requiring sustained attention, such as driving, walking outdoors, or performing fine visual tasks, especially when these activities involve shifting or refocusing the gaze.[15] This intermittent inability to open the eyelids can substantially affect independence and quality of life. In severe cases, patients may avoid social interaction or occupational activities because of embarrassment or disability caused by repeated episodes.[13]
A thorough history should also assess symptom onset and progression, which is typically gradual, as well as potential triggers and risk factors such as medications, prior neurologic disease, or ocular conditions. Symptoms of underlying neurological disorders, such as Parkinson disease or various forms of dystonia, may be present, manifesting as tremors, muscle stiffness, or abnormal movements. A history of exposure to dopamine antagonists, neuroleptics, or other medications affecting basal ganglia function may provide important diagnostic clues. Stress and intense concentration have been known to worsen the condition, whereas periods of relaxation and spontaneous blinking might provide transient relief.[49]
During the physical examination, clinicians should carefully observe eyelid dynamics during blinking and attempted voluntary opening. A key clinical feature is failure of levator palpebrae activation immediately after blink closure, despite normal muscle strength when the eyelids are manually elevated. Electromyographic studies have demonstrated persistent orbicularis oculi activity during attempted eyelid opening, suggesting impaired inhibition of eyelid-closing muscles.[24]
Patients may exhibit a characteristic "staring" appearance with infrequent blinking, a narrowed palpebral fissure, and compensatory frontalis overactivity, resulting in forehead wrinkling. An external evaluation of the eyelids and facial muscles is essential to assess for eyebrow and eyelid ptosis, dermatochalasis, and spasms of the orbicularis oculi, procerus, and corrugator muscles. Importantly, levator function and voluntary blink strength are preserved, helping distinguish ALO from true ptosis or primary muscle weakness.[50]
Neurologic examination may reveal associated features depending on the underlying etiology and plays a critical role in differentiating ALO from other conditions that mimic its presentation, such as ptosis due to myasthenia gravis or mechanical eyelid obstruction. In patients with Parkinson disease or other basal ganglia disorders, signs such as bradykinesia, rigidity, resting tremor, or postural instability may be present. In contrast, individuals with isolated ALO may demonstrate no other neurologic abnormalities, making diagnosis dependent primarily on clinical observation.[16] Assessment of mental status, language skills, and other cranial nerve functions may be useful when central causes are suspected.[50]
Because ALO may mimic several other ocular conditions, clinicians should systematically evaluate for mechanical, neuromuscular, and neurologic causes of eyelid dysfunction. Diagnostic workup may include neuroimaging, electromyography, or neurological consultation when secondary etiologies are suspected. A focused ophthalmologic examination is essential and may help identify alternative or contributing ocular pathology. Clinicians should assess visual acuity, visual fields, intraocular pressure, pupillary responses, and extraocular movements and should perform both a slit-lamp examination and a dilated fundoscopic evaluation.[15] Accurate differentiation is essential because treatment strategies vary significantly depending on the underlying mechanism (see Table 6).[51]
Table 6. Key History and Physical Examination Findings in Apraxia of Lid Opening
|
Clinical Domain |
Findings |
Clinical Significance |
|
Symptom onset |
Gradual onset, often after voluntary eye closure |
Suggests motor initiation disorder |
|
Primary concern |
Inability to initiate eyelid opening |
Hallmark feature of apraxia of lid opening |
|
Compensatory behaviors |
Manual lid lifting, neck extension, facial grimacing |
Attempts to overcome motor inhibition |
|
Sensory tricks (geste antagoniste) |
Touching the brow or eyelid improves opening |
Supports the dystonia-related mechanism |
|
Levator function |
Normal |
Excludes primary muscle weakness |
|
Blink reflex |
Preserved |
Differentiates from neuromuscular disorders |
|
Frontalis activity |
Increased forehead wrinkling |
Compensatory eyelid elevation |
|
Associated neurologic signs |
Tremor, rigidity, bradykinesia |
Suggest underlying Parkinsonism |
|
Ocular examination |
Normal anterior and posterior segments |
Excludes structural ocular pathology |
Evaluation
ALO is primarily a clinical diagnosis, and careful assessment of the patient’s history and physical examination remains the cornerstone of evaluation (see Image. Diagnostic Approach to Apraxia of Lid Opening). Patients typically present with difficulty initiating voluntary eyelid opening despite preserved levator muscle function. A detailed ocular and neurological history should explore symptom onset, duration, progression, triggering factors (eg, fatigue or stress), and associated neurological symptoms. The diagnostic criteria described by Defazio and Berardelli are commonly used to identify dystonia-related eyelid disorders and include characteristic features such as bilateral eyelid involvement, stereotypical spasms, high resting blink frequency, inability to voluntarily suppress eyelid closure, and partial relief with sensory tricks (geste antagoniste).[16] These criteria, originally developed for blepharospasm, have demonstrated high diagnostic utility, with reported sensitivity of approximately 93% and specificity of 90% in distinguishing dystonic eyelid disorders (see Table 7).[52]
Although no specific laboratory test confirms ALO, diagnostic investigations are often performed to exclude secondary causes or associated neurological disorders. Laboratory evaluation may include serum and cerebrospinal fluid panels to assess for systemic autoimmune, infectious, or metabolic etiologies.[53] When myasthenia gravis is part of the differential, acetylcholine receptor antibody testing, single-fiber electromyography, ice-pack testing, or edrophonium (eg, Tensilon) testing may be useful.[24][54]
A comprehensive neurological examination is essential to evaluate for conditions frequently associated with ALO, including Parkinson disease, dystonia, or progressive supranuclear palsy. Neurophysiological testing, such as electromyography of the orbicularis oculi and levator palpebrae superioris muscles, can provide supportive evidence of impaired coordination between these opposing muscles. Such studies are helpful in differentiating dystonic eyelid disorders from neuromuscular or myogenic conditions.[27][55]
Neuroimaging is not required to diagnose ALO but may be indicated to rule out structural brain lesions affecting motor control pathways, including the basal ganglia, brainstem, or frontal cortex. Magnetic resonance imaging of the brain with or without contrast is the preferred imaging modality when central nervous system pathology is suspected (eg, stroke, tumor, or demyelinating disease).[13] Computed tomography may also be used in selected cases, particularly when acute intracranial pathology is a concern.
Because ALO is rare, specific national or international guidelines dedicated solely to its evaluation are limited. Clinicians, therefore, often follow evaluation frameworks recommended for movement disorders and focal dystonias, which emphasize comprehensive clinical assessment, targeted investigations to exclude alternative diagnoses, and multidisciplinary collaboration among ophthalmologists, neurologists, and neuro-ophthalmologists.[29] Given the overlap with other eyelid and movement disorders, a tailored, patient-specific approach is recommended to ensure accurate diagnosis and appropriate management.[56]
Table 7. Diagnostic Evaluation in Apraxia of Lid Opening
|
Evaluation Component |
Purpose |
Key Findings |
|
Clinical history |
Identify symptom pattern and triggers |
Difficulty initiating eyelid opening |
|
Ocular examination |
Assess eyelid mechanics and levator function |
Normal eyelid strength with impaired initiation |
|
Neurological examination |
Identify associated movement disorders |
Parkinsonism, dystonia |
|
Laboratory tests |
Exclude autoimmune or systemic disease |
Antibody testing when indicated |
|
Myasthenia gravis testing |
Rule out neuromuscular junction disorders |
Ice pack test, ACh receptor antibodies |
|
Electromyography |
Assess muscle activity patterns |
Abnormal orbicularis–levator coordination |
|
Neuroimaging (MRI/CT) |
Exclude structural brain lesions |
Basal ganglia or brainstem pathology |
ACh, acetylcholine; CT, computed tomography; MRI, magnetic resonance imaging
Treatment / Management
Managing ALO requires a multidisciplinary, stepwise approach, particularly because the disorder is frequently associated with underlying neurological conditions (see Image. Stepwise Treatment Algorithm for Apraxia of Lid Opening). The primary therapeutic goal is to reduce abnormal orbicularis oculi activity and facilitate voluntary eyelid opening while simultaneously addressing any associated systemic or neurological disease. Treatment selection should be tailored to the individual patient, with consideration of disease severity, underlying etiology, comorbid conditions, and response to prior interventions (see Table 8).[15]
Botulinum toxin injections remain the most widely accepted and effective therapy, particularly when ALO is associated with blepharospasm or dystonic eyelid closure.[57][58] The toxin works by inhibiting acetylcholine release at the neuromuscular junction, thereby reducing involuntary contraction of the orbicularis oculi muscle and allowing the levator palpebrae superioris to elevate the eyelid more effectively.[13] Injections are typically administered to the pretarsal orbicularis oculi muscle in a targeted pattern to reduce spasm frequency and facilitate eyelid opening.[59][60](A1)
Pharmacologic therapy aimed at enhancing dopaminergic transmission may be particularly beneficial in patients with secondary ALO associated with Parkinson disease or other extrapyramidal disorders. For such patients, optimization of systemic neurological therapy may significantly improve symptoms. Adjustments in dopaminergic medications, including levodopa or dopamine agonists, have shown variable success in restoring motor coordination within the basal ganglia circuits responsible for eyelid opening.[13][58] For patients who do not respond adequately to medical therapy, surgical options may be considered. Orbicularis oculi myectomy, levator advancement procedures (eg, aponeurotic ptosis repair), blepharoplasty, and frontalis sling surgery have been described as treatment options in severe refractory cases.[16] These procedures aim to reduce the mechanical resistance to eyelid opening and facilitate alternative mechanisms of eyelid elevation.[24] (A1)
Rehabilitation strategies may also play a supportive role. Behavioral therapy, eyelid physiotherapy, and biofeedback techniques may help patients improve voluntary motor control and adapt to their symptoms.[61] Nonpharmacologic strategies, such as sensory tricks (geste antagoniste) involving tactile stimulation of the eyelid or brow, may provide transient symptomatic relief in some patients.[61] Additionally, addressing psychological stressors and improving patient education can enhance treatment adherence and overall quality of life.[44]
Because ALO is rare and heterogeneous, specific national or international guidelines dedicated solely to ALO management do not yet exist. Therefore, treatment decisions are largely guided by case series, expert consensus, and management principles derived from dystonia and blepharospasm guidelines. Collaborative care involving ophthalmologists, neurologists, and movement-disorder specialists is essential to achieve optimal outcomes.[6][62]
Table 8. Treatment Modalities for Apraxia of Lid Opening
|
Treatment Category |
Intervention |
Mechanism |
Clinical Indication |
|
Nonpharmacological |
Sensory tricks (geste antagoniste) |
Sensorimotor modulation |
Mild cases |
|
Physiotherapy/biofeedback |
Improves motor coordination |
Adjunct therapy |
|
|
Pharmacological |
Levodopa |
Enhances dopaminergic transmission |
Parkinson-related apraxia of lid opening |
|
Dopamine agonists |
Stimulate basal ganglia pathways |
Extrapyramidal disorders |
|
|
Injectable therapy |
Botulinum toxin type A |
Reduces orbicularis oculi contraction |
First-line treatment |
|
Surgical |
Orbicularis myectomy |
Removes dystonic muscle fibers |
Refractory cases |
|
Levator advancement |
Improves eyelid elevation |
Coexisting ptosis |
|
|
Frontalis sling |
Uses frontalis muscle to lift eyelid |
Severe cases |
Differential Diagnosis
ALO is a clinical diagnosis that must be distinguished from a range of neurologic, neuromuscular, structural, and functional conditions associated with impaired eyelid opening (see Table 9). These disorders share overlapping clinical features but differ in underlying mechanisms and management. The following differential diagnosis is organized by major etiologic categories, along with key clinical mimics, to facilitate systematic evaluation.
- Idiopathic (primary dystonia)
- Benign essential blepharospasm: Involuntary eyelid closure that may be associated with sensory symptoms such as eye-burning pain, keratoconjunctivitis sicca, photophobia, and relief with sensory tricks (geste antagoniste) [63][64]
- Meige syndrome: Combination of blepharospasm with oromandibular and cervical dystonia
- Brueghel syndrome: Blepharospasm with oromandibular dystonia, with or without additional features such as torticollis, limb dystonia, or dystonic respiratory patterns [65][66]
- Iatrogenic
- Drug-induced movement disorders (including tardive dyskinesia): Repetitive, involuntary movements associated with medications such as antidepressants, antipsychotics, antiepileptics, antimicrobials, and antiarrhythmics [67]
- Dopaminergic therapy–related effects: Eyelid motor dysfunction secondary to levodopa or apomorphin use, particularly in patients with progressive supranuclear palsy [68]
- Deep brain stimulation: Induction or exacerbation of eyelid movement abnormalities due to stimulation of the subthalamic nucleus or globus pallidus internus in patients with Parkinson disease [69][70]
- Genetic
- Primary dystonia syndromes: Genetic forms of dystonia may include blepharospasm and cervical dystonia. Reported associations include mutations in:
- Structural lesions
- Central nervous system lesions: Vascular, traumatic, or mass lesions involving the midbrain, basal ganglia, thalamus, cerebellum, or motor cortex that disrupt eyelid motor pathways [78]
- Hemifacial spasm: Unilateral, intermittent contractions of facial muscles, including eyelid closure, typically due to facial nerve irritation
- Neuromuscular
- Myasthenia gravis: Fluctuating eyelid ptosis and oculomotor fatigue that worsen with activity and improve with rest; may respond to ice-pack or edrophonium testing [79][80]
- Bell palsy: Unilateral facial weakness with associated symptoms such as retroauricaulr pain, dysgeusia, hyperacusis, hypersalivation, and decreased lacrimation
- Movement disorders
- Parkinson disease: Bradykinesia-related impairment of eyelid opening accompanied by tremor, rigidity, and postural instability [38][39]
- Progressive supranuclear palsy: Supranuclear gaze palsy with impaired eyelid and ocular movements, often associated with early postural instability and falls [81]
- Focal, segmental, or generalized dystonia: Hyperkinetic movement disorders that may include blepharospasm and impaired eyelid coordination
- Tardive dyskinesia: Drug-induced hyperkinetic movements that may involve the eyelids and mimic ALO [82]
- Mechanical
- Ptosis: Drooping of the upper eyelid due to myogenic, neurogenic, mechanical, or traumatic causes; distinguished by impaired eyelid elevation rather than difficulty initiating the movement [83]
- Functional and physiologic mimics
- Functional eyelid disorders: Apparent inability to open the eyes without identifiable structural or neurologic pathology, often associated with psychological factors [25]
- Voluntary nystagmus: Rapid, voluntary oscillatory eye movements that may interfere with sustained eyelid opening [84]
- Orbicularis oculi fatigue: Transient difficulty opening the eyes following prolonged voluntary eyelid closure due to muscle fatigue [19]
Table 9. Differential Diagnosis of Apraxia of Lid Opening
|
Category |
Condition |
Key Clinical Features |
Distinguishing Points |
|
Idiopathic |
Benign essential blepharospasm |
Involuntary eyelid closure with photophobia and dry eye |
Spasm of the orbicularis oculi rather than inability to initiate opening |
|
Meige syndrome |
Blepharospasm with oromandibular and cervical dystonia |
Involves facial and jaw dystonia |
|
|
Brueghel syndrome |
Blepharospasm with oromandibular and limb dystonia |
Multiregional dystonia present |
|
|
Iatrogenic |
Drug-induced dystonia |
Occurs after antipsychotics, antidepressants, and antiepileptics |
History of medication exposure |
|
Levodopa/apomorphine complications |
Seen in PSP or Parkinson disease |
Associated parkinsonian features |
|
|
Deep brain stimulation |
Eyelid dysfunction following subthalamic or pallidal stimulation |
Temporal association with device activation rather than primary motor initiation failure | |
|
Genetic dystonias |
TOR1A mutation dystonia |
Early-onset generalized dystonia |
Genetic predisposition |
|
ANO3, TUBB4A mutations |
Focal or segmental dystonia |
Familial or genetic pattern |
|
|
GNAL mutation |
Adult-onset focal or segmental dystonia | Familial cranial dystonia pattern | |
|
ZNF1 mutation |
Variable focal or generalized dystonia | Rare genetic association with motor dysfunction | |
|
Structural |
CNS lesions (midbrain, basal ganglia, thalamus, cerebellum, motor cortext) |
Focal neurological deficits |
MRI may show structural pathology |
|
Hemifacial spasm |
Unilateral facial twitching |
Caused by facial nerve irritation |
|
|
Neuromuscular |
Myasthenia gravis |
Fluctuating ptosis and diplopia |
Positive ice-pack or antibody tests |
|
Bell palsy |
Unilateral facial weakness with incomplete eye closure | Facial nerve palsy causing weakness rather than impaired eyelid opening | |
|
Movement disorders |
Parkinson disease |
Tremor, rigidity, bradykinesia |
Systemic motor features |
|
Progressive supranuclear palsy |
Vertical gaze palsy, early falls |
Distinct ocular motor abnormalities |
|
|
Focal, segmental, or generalized dystonia |
Involuntary contractions with abnormal posturing, including eyelids | Dystonic closure rather than isolated failure to initiate opening | |
|
Tardive dyskinesia |
Involuntary repetitive facial movements | Associated with chronic neuroleptic use | |
|
Mechanical |
Ptosis |
Drooping eyelid due to levator weakness |
Structural eyelid abnormality |
|
Functional |
Functional eyelid disorders |
Psychogenic inability to open eyes |
No neurological abnormalities |
|
Voluntary nystagmus |
Rapid voluntary eye oscillations interfere with eye opening | Preserved eyelid initiation; symptoms due to eye movements | |
|
Physiologic mimic |
Orbicularis fatigue |
Temporary eyelid opening difficulty |
Improves with rest |
ANO3, anoctamin 3; CNS, central nervous system; GNAL, G-protein subunit alpha L; MRI, magnetic resonance imaging; PSP, progressive supranuclear palsy; TOR1A, torsin 1A; TUBB4A, tubulin beta 4A; ZNF1, zinc finger protein 1
Pertinent Studies and Ongoing Trials
Although ALO is a relatively rare disorder, several clinical studies and case series have investigated its pathophysiology and treatment strategies (see Table 10). Most evidence comes from observational studies and small clinical trials, particularly those evaluating the efficacy of botulinum toxin injections, dopaminergic therapy, and surgical interventions.[55] Early clinical observations demonstrated that ALO often occurs in association with blepharospasm and extrapyramidal disorders, including Parkinson disease and progressive supranuclear palsy. These findings suggested that dysfunction within the basal ganglia–frontal cortical network plays a central role in the disease mechanism. Electromyographic studies further showed abnormal co-contraction of the levator palpebrae superioris and orbicularis oculi muscles, supporting the hypothesis that impaired reciprocal inhibition contributes to difficulty initiating eyelid opening.[85]
Several studies have evaluated botulinum toxin type A injections as a therapeutic strategy for ALO, particularly when it coexists with blepharospasm. In a clinical study of patients with focal eyelid dystonia, approximately 83% experienced improvement in eyelid opening after botulinum toxin injections, supporting its role as the primary symptomatic treatment.[86] Further electrophysiological investigations demonstrated that botulinum toxin therapy reduces abnormal orbicularis oculi activity and improves eyelid opening latency, confirming its beneficial neuromuscular effects.[87][88]
Despite these promising results, some patients show partial or poor response to botulinum toxin therapy, particularly when ALO occurs as an independent motor initiation disorder rather than a component of blepharospasm. In such cases, adjunctive therapies including levator aponeurosis repair, orbicularis myectomy, or frontalis suspension surgery may be required. Surgical studies have demonstrated long-term improvement in patients with refractory ALO associated with dystonic eyelid disorders.[89] Recent literature continues to explore optimized injection techniques and treatment protocols for isolated ALO. Contemporary case reports and clinical reviews suggest that targeted botulinum toxin administration and multidisciplinary management strategies can significantly improve patient outcomes and functional visual ability.[90]
Because ALO is rare, large randomized controlled trials are limited. Current research focuses primarily on improving treatment protocols for dystonia-related eyelid disorders, which may indirectly benefit patients with ALO. Future studies investigating neurophysiological mechanisms, advanced imaging, and neuromodulation therapies may provide further insights into disease pathogenesis and management.[15]
Table 10. Key Clinical Studies on Apraxia of Lid Opening
|
Study |
Study Type |
Sample Size |
Key Findings |
Clinical Implication |
|
Krack et al, Movement Disorders |
Clinical observational study |
29 patients |
83% improvement with botulinum toxin |
Supports botulinum toxin as first-line therapy |
|
Piccione et al |
Electrophysiological study |
Case series |
Abnormal levator–orbicularis co-contraction |
Demonstrates neurophysiologic mechanism |
|
Forget et al, Neurology |
Clinical study |
10 patients |
Reduced orbicularis activity and improved lid opening latency after botulinum toxin |
Confirms neuromuscular benefit |
|
Dressler et al |
Surgical outcomes study |
15 patients |
Frontalis suspension effective in refractory cases |
Surgical option for severe disease |
|
Recent case reports |
Case-based evidence |
Individual cases |
Targeted botulinum toxin protocols improve outcomes |
Highlights personalized treatment approach |
Treatment Planning
Treatment planning for ALO is individualized and depends on the severity of symptoms, underlying neurological etiology, and response to prior therapies (see Table 11). Because ALO is primarily a disorder of motor initiation rather than structural eyelid pathology, treatment planning focuses on neurological evaluation, neuromuscular modulation, and functional rehabilitation.[6]
Clinical Assessment and Simulation
The initial phase of treatment planning involves a comprehensive neurological and ophthalmic evaluation to determine whether the ALO is isolated or secondary to conditions such as blepharospasm, Parkinson disease, progressive supranuclear palsy, or other dystonic disorders. High-resolution imaging, such as brain magnetic resonance imaging, may be performed when structural lesions of the basal ganglia, midbrain, or frontal cortex are suspected. Clinical observation of eyelid dynamics, electromyographic studies, and assessment of levator palpebrae superioris function can help identify the dominant mechanism underlying impaired eyelid opening.[8]
Target Muscles and Injection Strategy
In therapeutic planning, the primary targets are the orbicularis oculi muscles, particularly the pretarsal and preseptal portions, which may exhibit excessive tonic contraction in patients with ALO-associated dystonia. Botulinum toxin injections are typically planned as the first-line method to reduce this abnormal muscle activity while preserving normal eyelid closure and blink reflex. Injection sites are distributed symmetrically across the eyelid margin to optimize functional outcomes and minimize complications such as ptosis or lagophthalmos.[16]
Pharmacologic Treatment Planning
Pharmacologic therapy may be considered when ALO is associated with dopaminergic dysfunction or extrapyramidal disorders. Medications such as levodopa, dopamine agonists, anticholinergic agents, or benzodiazepines may be used depending on the underlying neurological condition. Dose titration and monitoring for adverse effects are essential components of treatment planning.[16]
Surgical Treatment Planning
For refractory cases that do not respond to conservative therapies, surgical intervention may be considered. Surgical planning typically involves procedures aimed at reducing orbicularis oculi activity or enhancing eyelid elevation. These procedures include:
- Orbicularis oculi myectomy
- Levator aponeurosis advancement
- Frontalis sling suspension
Preoperative planning requires careful evaluation of levator function, eyelid anatomy, and brow position to determine the most appropriate surgical approach.[16]
Multidisciplinary Management
Because ALO frequently occurs in association with neurological disorders, optimal treatment planning requires collaboration among ophthalmologists, neurologists, movement disorder specialists, and rehabilitation therapists. Multidisciplinary management improves treatment outcomes and helps address functional limitations affecting the patient’s daily activities.[24]
Table 11. Treatment Planning Components in Apraxia of Lid Opening
|
Planning Component |
Key Considerations |
Clinical Purpose |
|
Clinical evaluation |
Neurological and ophthalmic examination |
Identify the underlying etiology |
|
Imaging studies |
MRI brain when structural lesions are suspected |
Detect basal ganglia or brainstem pathology |
|
Injection planning |
Botulinum toxin injection sites in orbicularis oculi |
Reduce dystonic muscle activity |
|
Pharmacologic therapy |
Dopaminergic medications or muscle relaxants |
Improve motor coordination |
|
Surgical planning |
Myectomy, levator repair, frontalis sling |
Manage refractory cases |
|
Multidisciplinary care |
Neurology + ophthalmology collaboration |
Optimize long-term management |
Toxicity and Adverse Effect Management
Managing ALO frequently involves interventions such as botulinum toxin injections, pharmacologic therapy, and occasionally surgical procedures. Although these treatments are generally well tolerated, clinicians must be aware of potential adverse effects and implement appropriate management strategies to minimize complications and maintain optimal patient outcomes (see Table 12).[91]
Botulinum Toxin–Related Adverse Effects
Botulinum toxin injections are the most commonly used treatment for ALO, particularly when associated with blepharospasm or dystonia. Adverse effects are usually mild and transient but may include ptosis, diplopia, lagophthalmos (ie, inability to fully close the eyelid), dry eye, excessive tearing, and local eyelid bruising. These effects typically result from diffusion of the toxin into adjacent muscles, such as the levator palpebrae superioris or the extraocular muscles. Careful dose selection, precise injection placement, and symmetrical injection patterns help reduce these risks. If ptosis or diplopia occurs, symptoms are usually self-limited and resolve within several weeks as the toxin effect diminishes.[6]
Pharmacologic Therapy–Related Adverse Effects
Patients treated with medications such as levodopa, dopamine agonists, anticholinergic agents, or benzodiazepines may experience systemic side effects such as orthostatic hypotension, nausea, dizziness, sedation, cognitive impairment, or dyskinesias, depending on the specific medication used. Close monitoring and gradual dose titration are recommended to minimize these adverse reactions.[27]
Surgical Complications
In refractory cases requiring surgical intervention, complications may include overcorrection, eyelid asymmetry, infection, hematoma, or incomplete symptom relief. Procedures such as orbicularis myectomy, levator advancement, or frontalis sling surgery require careful surgical planning and postoperative monitoring to reduce complication rates.[92]
Ocular Surface Complications
Because eyelid function is critical for maintaining tear film stability and corneal protection, treatments affecting eyelid mechanics may lead to dry eye syndrome, exposure keratopathy, or corneal irritation. Supportive measures such as artificial tears, lubricating ointments, and eyelid hygiene can help prevent these complications.[93]
Long-Term Monitoring
Long-term management of ALO requires periodic follow-up visits to evaluate symptom control and detect treatment-related complications. In patients receiving repeated botulinum toxin injections, clinicians should monitor for reduced therapeutic response or antibody-mediated resistance, although this complication remains uncommon. A multidisciplinary approach involving ophthalmologists, neurologists, and movement disorder specialists is recommended to ensure safe and effective management while minimizing treatment-related toxicity.[94]
Table 12. Common Adverse Effects and Management Strategies in Apraxia of Lid Opening Treatment
|
Treatment Modality |
Potential Adverse Effects |
Management Strategy |
|
Botulinum toxin injection |
Ptosis, diplopia, lagophthalmos, bruising |
Dose adjustment, accurate injection technique |
|
Dopaminergic medications |
Nausea, hypotension, dyskinesia |
Gradual dose titration, monitoring |
|
Anticholinergic agents |
Dry mouth, blurred vision, and cognitive effects |
Dose reduction or alternative therapy |
|
Benzodiazepines |
Sedation, dizziness, dependence |
Dose titration, monitoring, careful patient selection |
|
Surgical procedures |
Infection, asymmetry, incomplete correction |
Surgical expertise and follow-up |
|
Eyelid dysfunction |
Dry eye, exposure keratopathy |
Lubricants, ocular surface protection |
Staging
ALO currently lacks a standardized staging system. Nevertheless, clinicians frequently classify the condition based on clinical severity, functional impairment, and associated neurological features (see Table 13). This functional staging provides a practical framework for evaluating disease severity, monitoring progression, and selecting appropriate therapeutic strategies (see Image. Functional Staging of Apraxia of Lid Opening).[91]
In the early stages of ALO, patients experience intermittent difficulty initiating eyelid opening, often triggered by fatigue, stress, or prolonged visual tasks. Symptoms may occur sporadically and are typically relieved with sensory tricks (geste antagoniste) or brief manual assistance.[6] As the disorder progresses, patients may develop persistent difficulty opening the eyelids following voluntary closure or blinking.
Compensatory mechanisms such as excessive contraction of the frontalis muscle, facial grimacing, or head movements may become more prominent. At this stage, symptoms may interfere with activities such as reading, watching television, or driving. In advanced stages, patients may experience frequent episodes of functional eyelid closure, resulting in temporary visual disability despite preserved ocular structure and muscle strength.[13] This stage is often associated with underlying neurological disorders, including Parkinson disease or dystonic syndromes, and may require more aggressive interventions such as botulinum toxin injections or surgical treatment.
Table 13. Functional Staging of Apraxia of Lid Opening
|
Stage |
Clinical Features |
Functional Impact |
Typical Management |
|
Stage I (Mild) |
Intermittent difficulty initiating eyelid opening |
Minimal impairment |
Observation, sensory tricks |
|
Stage II (Moderate) |
Frequent episodes of delayed eyelid opening |
Mild functional limitations |
Botulinum toxin injections |
|
Stage III (Severe) |
Persistent eyelid opening difficulty with compensatory facial movements |
Significant visual impairment |
Pharmacologic therapy + injections |
|
Stage IV (Advanced) |
Functional eyelid closure causing temporary blindness |
Severe disability |
Surgical intervention |
Prognosis
The prognosis for individuals with ALO can vary widely and depends on the chronicity, underlying etiology, associated conditions, and responsiveness to first-line treatment. Because ALO is not itself a degenerative disorder, its prognosis is primarily related to management effectiveness and the disease course of any underlying neurological disorders.[61] ALO may be challenging to treat in many cases. In general, responsiveness to treatment is a good prognostic factor regarding morbidity. Chronicity and resistance to treatment can lead to more disruption in functional independence and disability.
In cases where ALO is associated with treatable conditions, such as blepharospasm or Parkinson disease, the use of botulinum toxin injections or dopaminergic medications, respectively, can offer significant symptomatic relief, leading to a relatively good prognosis. For some patients, these treatments can substantially improve their quality of life and may be effective for long periods.[95] However, if ALO is part of a more complex or progressive neurological disorder, such as progressive supranuclear palsy or certain forms of Parkinsonism, the overall prognosis may be more guarded. In these situations, ALO may persist or progress in line with the underlying disease, and management may become more challenging over time. Surgical interventions, such as levator resection or frontalis suspension, may offer a more permanent solution for some patients. However, outcomes can vary, and surgical intervention carries risks of complications and the potential need for further surgery.[96]
Despite diverse interventions, ALO often presents a significant therapeutic challenge, and patients may experience only partial improvement. The condition can profoundly impact quality of life, as affected individuals may find routine activities that require unobstructed vision challenging. Generally, ALO itself does not directly affect lifespan, but the functional impairment can significantly impact a person's daily activities and psychosocial well-being. Early recognition and appropriate treatment are vital to improving the prognosis and quality of life for those affected by ALO. Interdisciplinary care involving neurologists, ophthalmologists, and physical therapists is often required to optimize management and provide comprehensive care.[97]
Complications
Complications of ALO may arise from both the underlying disorder and its treatment, as well as from the functional consequences of impaired eyelid opening (see Table 14). Beyond the commonly reported transient adverse effects of botulinum toxin therapy, which are typically mild and self-limited, several additional complications may arise in patients with ALO.[98][99][100] These complications may result from underlying neurological dysfunction, secondary ocular surface problems, or long-term functional disability caused by impaired eyelid opening.[6]
One important complication is visual disability, including functional blindness. In severe cases, patients may be unable to keep their eyelids open long enough to sustain visual fixation, resulting in episodes of temporary visual deprivation. This phenomenon may significantly hinder activities that require continuous visual attention, such as walking in crowded environments, driving, or reading. In addition, if the upper field of vision is obstructed by an inability to fully lift the eyelids, patients may develop significant visual field impairment and experience difficulties with spatial orientation and mobility. Over time, this functional visual limitation may contribute to reduced independence and increased fall risk, particularly among older adults.[15]
Secondary ocular surface disease may also develop. Patients with ALO may exhibit irregular blinking patterns or incomplete eyelid opening, which can disrupt normal tear-film distribution. This disruption may predispose individuals to keratoconjunctivitis sicca (dry eye disease), punctate epithelial erosions, exposure keratopathy, and recurrent corneal epithelial defects.[101] Chronic ocular surface irritation may further exacerbate reflex blinking or eyelid spasms, creating a self-perpetuating cycle that worsens the clinical condition.[18]
Another complication involves postural and compensatory muscular strain. Patients frequently adopt compensatory maneuvers to overcome the difficulty opening the eyelids, such as excessive contraction of the frontalis muscle, tilting the head backward, or manually lifting the eyelids. Persistent use of these strategies can lead to forehead muscle fatigue, neck strain, and tension headaches.[29]
ALO may also contribute to psychological distress and reduced quality of life. The chronic nature of the condition, coupled with visible facial abnormalities, can result in embarrassment, social withdrawal, and reduced self-confidence.[102] Studies evaluating dystonia-related eyelid disorders have shown increased rates of anxiety, depression, and social isolation, particularly when symptoms interfere with occupational activities.[8] Functional impairment related to difficulty performing daily tasks may further compound these psychosocial effects, reinforcing the burden of disease.
In patients with neurodegenerative disorders such as Parkinson disease or progressive supranuclear palsy, ALO may represent a marker of disease progression. The presence of ALO can complicate neurological rehabilitation and worsen overall motor disability.[51] In addition, the stress of managing ALO can potentially exacerbate other symptoms of the underlying neurologic disorder.
Another potential complication is treatment resistance or symptom recurrence. Some patients may develop reduced responsiveness to repeated botulinum toxin injections due to antibody formation or disease progression, leading to persistent eyelid dysfunction. In such cases, alternative management strategies, including surgical interventions, may become necessary, which can further increase morbidity.[103] Surgical interventions carry risks including infection, scarring, and the need for repeat surgeries.[90]
Finally, long-standing cases of ALO may increase the risk of accidents or injuries due to intermittent visual obstruction. Patients may experience difficulty navigating unfamiliar environments, climbing stairs, or driving, which can increase their risk of falls and other safety hazards.[104] Early recognition and appropriate multidisciplinary management, including ophthalmologic care, neurological evaluation, and psychological support, are essential to minimize these complications and improve patient outcomes.[6][105]
Table 14. Complications of Apraxia of Lid Opening
|
Category |
Complication |
Clinical Impact |
|
Functional |
Functional visual impairment |
Difficulty performing daily tasks |
|
Ocular surface |
Exposure keratopathy |
Corneal irritation and epithelial defects |
|
Ocular surface |
Keratoconjunctivitis sicca (dry eye disease) |
Tear film instability and irritation |
|
Neuromuscular |
Frontalis muscle fatigue |
Forehead strain due to compensatory effort |
|
Musculoskeletal |
Neck and postural strain |
Chronic head tilting and muscle tension |
|
Neurological |
Progression of associated disorders |
Seen in Parkinson disease or PSP |
|
Psychological |
Anxiety and depression |
Reduced quality of life |
|
Social |
Social withdrawal |
Embarrassment due to visible eyelid dysfunction |
|
Safety |
Falls and accidents |
Impaired navigation due to transient visual obstruction |
|
Treatment related |
Botulinum toxin resistance |
Reduced therapeutic effectiveness |
PSP, progressive supranuclear palsy
Postoperative and Rehabilitation Care
Postoperative and rehabilitation care for patients with ALO is an essential component of treatment, especially if surgical interventions are involved. The goal of postoperative care is to ensure proper healing and maximize the functional outcome of the surgery. Concurrently, rehabilitation focuses on optimizing eyelid function and preventing complications.
Postoperative Care
- Monitoring for complications: After surgery, close monitoring is required to detect any signs of complications such as infection, hematoma, or adverse reactions to anesthesia.
- Wound care: Proper care of the surgical site is necessary to prevent infection and promote healing. Proactive measures may include cleaning the area and applying prescribed topical medications.
- Medication management: Patients may be prescribed medications to manage pain, reduce inflammation, and minimize the risk of infection.
- Follow-up visits: Regular follow-up with the surgical team is crucial to assess healing and the effectiveness of the intervention. The treatment plan may be adjusted based on the patient's progress.[106]
Rehabilitation Care
- Physical therapy: If indicated, physical therapy can help patients learn exercises to strengthen the eyelid muscles and improve coordination for lid opening.
- Occupational therapy: Occupational therapy may assist patients in adapting to any residual functional impairments and incorporating practical strategies into their daily activities.
- Visual aids: In some cases, patients may benefit from visual aids or environmental modifications to accommodate visual field limitations.
- Education: Patients should be educated on techniques to manually assist eyelid opening when needed and on sensory tricks to facilitate lid elevation.
- Stress management: Since stress can exacerbate ALO, stress management techniques such as relaxation exercises, biofeedback, or counseling may be beneficial.[107]
The specifics of postoperative and rehabilitation care will vary depending on the individual's condition, the type of surgery performed, and any associated neurological conditions. A multidisciplinary approach involving neurologists, ophthalmologists, surgeons, physical and occupational therapists, and, if necessary, mental health professionals provides the most comprehensive care for individuals recovering from ALO surgery. Regular assessment and appropriate adjustments in the care plan are important to address the patient's changing needs.[108]
Consultations
Consultations with various specialists may be necessary to manage ALO and ensure comprehensive care. The interdisciplinary team members may include the following:
- Neurologist: A neurologist can help diagnose ALO, primarily as it may be associated with other neurological conditions such as Parkinson disease, dystonia, or progressive supranuclear palsy. Neurologists can also assist in managing the neurological aspects of the condition and any comorbidities.[81]
- Ophthalmologist: An ophthalmologist, particularly one specializing in neuro-ophthalmology, can evaluate the structural health of the eyes and eyelids, rule out primary ocular causes of eyelid dysfunction, and participate in the management of ALO, including botulinum toxin injections if indicated.[109]
- Movement disorder specialist: If the patient has an underlying movement disorder, a movement disorder specialist can provide targeted treatment and management strategies.[110]
- Occupational therapist: An occupational therapist can assist with adaptations to daily living activities and suggest devices or strategies to compensate for any visual limitations caused by ALO.[111]
- Physical therapist: Physical therapy may be beneficial for patients who require eyelid-strengthening exercises or other modalities to improve eyelid motor control.[112]
- Plastic or reconstructive surgeon: If surgical intervention is considered, a consultation with a plastic surgeon or an oculoplastic surgeon experienced in eyelid surgery may be necessary.[113]
- Psychologist or psychiatrist: Due to the potential psychological impact of ALO, such as anxiety or depression, mental health support from a psychologist or psychiatrist may be necessary.
- Rehabilitation medicine specialist: This specialist can oversee a comprehensive postoperative rehabilitation program or as part of the long-term management of ALO.
An interdisciplinary approach involving these specialists can help formulate a holistic treatment plan tailored to the patient’s specific needs. Personalized, collaborative care can greatly improve the overall prognosis and quality of life for individuals with ALO.
Deterrence and Patient Education
Deterrence and patient education are essential components in managing ALO. Patient education should include the following:
- Understanding of ALO: Patients should be provided with clear information about ALO, its symptoms, and how it differs from other eyelid disorders. Establishing this foundation helps in setting realistic expectations about the condition and its management.[15] Clinicians should also explain that ALO may be associated with an underlying disorder which may require additional evaluation and treatment, such as Parkinson disease, Huntington disease, myasthenia gravis, Sjögren syndrome, or multiple sclerosis.[61]
- Treatment options: Patients should be educated about the available treatment modalities, including nonpharmacological approaches, pharmacological treatments, botulinum toxin injections, and possible surgical interventions. Clinicians should explain the benefits, risks, and expected outcomes of each option.[114]
- Self-help techniques: Patients may require strategies to assist with lid opening, such as using sensory tricks (eg, lightly touching the forehead or temples), maintaining good eyelid hygiene, and performing prescribed eyelid exercises.
- Medication adherence: The importance of adhering to medication regimens, if prescribed, and the potential adverse effects and importance of reporting them to the healthcare professional, should be discussed.
- Monitoring: Patients should be encouraged to monitor their symptoms regularly and keep a symptom diary, which can help them manage the condition and inform adjustments to treatment plans.
- Lifestyle modifications: Clinicians should discuss strategies to help manage symptoms, such as stress-reduction techniques, optimizing sleep, and avoiding activities that may exacerbate them.
- Regular follow-up: The importance of follow-up appointments to monitor the condition, assess treatment effectiveness, and make necessary adjustments should be emphasized.[115]
- Support networks: Patients should be informed about support groups or resources for individuals with ALO or associated conditions. Emotional and psychological support can be crucial for coping with chronic conditions.
- Complications: Patients need information about the potential complications of ALO, such as social and psychological impacts, and the importance of seeking help if they experience these issues.
- Prognosis: Information should be provided about the prognosis of ALO, including factors that can influence the condition's progression and management strategies that may improve functional outcomes.[116]
Effective patient education can empower individuals with ALO to actively participate in their care, help them better manage their condition, and improve their overall quality of life.
Pearls and Other Issues
Pertinent take-home points regarding ALO include the following:
Summary
- ALO is a nonmotor abnormality characterized by bilateral difficulty with eyelid elevation.
- This symptom commonly occurs after the patient voluntarily closes their eyes.
- ALO is a misnomer, given that the condition rarely involves pure and true apraxia.
- The condition is associated with dysfunction in the corticothalamic, basal ganglia, and focal cranial nerve circuitry.
- Structures involved include sensorimotor cortical regions, substantia nigra pars reticulata, and brainstem motor nuclei.[117]
- The most common etiology of ALO is idiopathic focal dystonia.
- Other causes include blepharospasm or focal dystonia of the eyelids, toxic exposure, face or eyebrow ptosis, dermatochalasis, fatigue, and infectious, autoimmune, neurodegenerative, neuromuscular, traumatic, iatrogenic, and psychogenic disorders.
- Patients typically demonstrate compensatory behaviors, including thrusting the head backward, manually opening the eyelids with their fingers, and rubbing the eyebrows.
- Botulinum toxin A is considered the first-line treatment.[85]
- Several disorders will present similarly to ALO and must be excluded to treat them appropriately.
- The prognosis depends on the chronicity, etiology, and responsiveness to the first-line treatment.
- Chronicity and resistance to treatment can lead to more disruption in functional independence and disability.[15]
Pearls
- Early recognition: ALO is often under-recognized. Awareness of the condition among healthcare professionals is crucial for early diagnosis and management, which can significantly improve the quality of life for affected patients.
- Multidisciplinary approach: Effective management of ALO often requires a team that includes neurologists, ophthalmologists, and sometimes neurosurgeons, as well as nurses and physical and occupational therapists.
- Customized treatment: Treatment should be tailored to the individual, as ALO can present differently in each patient, and response to treatment can vary widely.
- Potential for improvement: While challenging, ALO can often be effectively managed with treatment, including botulinum toxin A injections, physical therapy, and, in some cases, surgical intervention.
- Disposition: Patients with ALO should have a clear management plan, including regular follow-up appointments to monitor their condition and treatment response. Patients should also be provided with information on how to seek urgent care if they experience significant changes or complications related to their condition.[118]
Pitfalls
- Misdiagnosis: ALO can be mistaken for other conditions, such as blepharospasm or myasthenia gravis, leading to inappropriate treatments.
- Overlooking underlying conditions: Clinicians must be careful not to miss an underlying neurological disorder associated with ALO, as such a lapse can affect treatment and prognosis.
- One-size-fits-all approach: Given the variability in presentation and treatment response, a standardized approach may not be effective.
- Prevention: While studies have not yet identified specific measures to prevent ALO, given its association with other neurological conditions, understanding the risk factors and early signs can help with prompt diagnosis and management.[119]
Additional Information
- Patient education: Patients should be educated about the nature of ALO and the importance of adherence to treatment and follow-up schedules.
- Research advances: Clinicians must keep abreast of new research, as understanding of ALO and its treatment continues to evolve.
- Quality of life: Attention should be paid to ALO's impact on a patient's psychological and social well-being, with appropriate support provided.[120] Clinicians must address both the physical aspects of the condition and the broader impacts on the patient's life.
Enhancing Healthcare Team Outcomes
Enhancing healthcare team outcomes for patients with ALO requires a coordinated, interprofessional approach that integrates the skills and expertise of various healthcare providers to ensure comprehensive, patient-centered care. The outcomes of ALO primarily depend on its underlying cause. However, prompt consultation with an interprofessional group of specialists is recommended to improve outcomes regardless of etiology.
Shared decision-making and communication are essential elements for positive outcomes. In conjunction with occupational therapists, the neurologist plays an integral part in the diagnosis and treatment. Botulinum toxin injections are usually performed by an ophthalmologist, oculoplastic surgeon, or plastic surgeon; however, they can occasionally be administered by a neurologist or movement disorder specialist. Social worker and case management evaluation may be required, particularly for refractory cases, as ALO can impair the patient's activities of daily living and job performance.[61]
Considerations for the interprofessional team include the following:
Skills and Strategy
- Assessment skills: All team members should be skilled in assessing ALO, recognizing its signs, and distinguishing it from other conditions.
- Treatment planning: Clinicians should develop the best treatment plan, considering both nonpharmacological and pharmacological options, and tailor it to the individual patient’s needs.
- Surgical consideration: If surgery is indicated, surgeons must possess the technical skills to perform procedures that benefit ALO patients, such as eyelid crutches or levator resection.[121]
Ethics and Responsibilities
- Informed consent: The healthcare team is responsible for ensuring patients understand the benefits and risks of any proposed treatment.
- Patient autonomy: Patients should be involved in their care decisions, and the team should support their independence and choices.
- Privacy and confidentiality: Team members must maintain patient confidentiality and share health information only among the care team as necessary for patient treatment.[122]
Interprofessional Communication
- Care coordination: Effective communication among neurologists, ophthalmologists, physical therapists, nurses, and primary care physicians is essential to coordinate care and manage treatments.
- Documentation: Accurate and thorough documentation in a shared electronic health record allows all team members to access patient information, track progress, and adjust treatment plans as needed.[123]
Care Coordination
- Role clarification: Each team member should understand their role in managing ALO to avoid duplication of efforts and to ensure that all aspects of care are addressed.
- Follow-up: Coordinating follow-up appointments and ongoing care management is essential to monitor treatment effectiveness and adjust interventions as needed.
- Patient education: Team members should provide consistent, clear education to the patient and their family about ALO, including information regarding treatment options and self-help strategies.[124]
Outcomes and Patient Safety
- Monitoring for adverse events: Close monitoring of treatment-related adverse events, such as those associated with botulinum toxin, is crucial for patient safety.
- Outcome measurement: The team should use validated tools to measure patient outcomes and assess the impact of treatment on quality of life and functional status.
Team Performance
- Regular team meetings: Interprofessional team meetings can help discuss patient progress, identify issues, and plan future interventions.
- Continuing education: All team members should engage in continuing education to stay up to date with the latest evidence-based practices for ALO.[125]
By fostering an environment of mutual respect and open communication, the healthcare team can enhance care for patients with ALO, thereby improving outcomes, patient satisfaction, and team performance. Each member’s contribution is vital, from diagnosis and treatment to patient education and support.
Media
(Click Image to Enlarge)
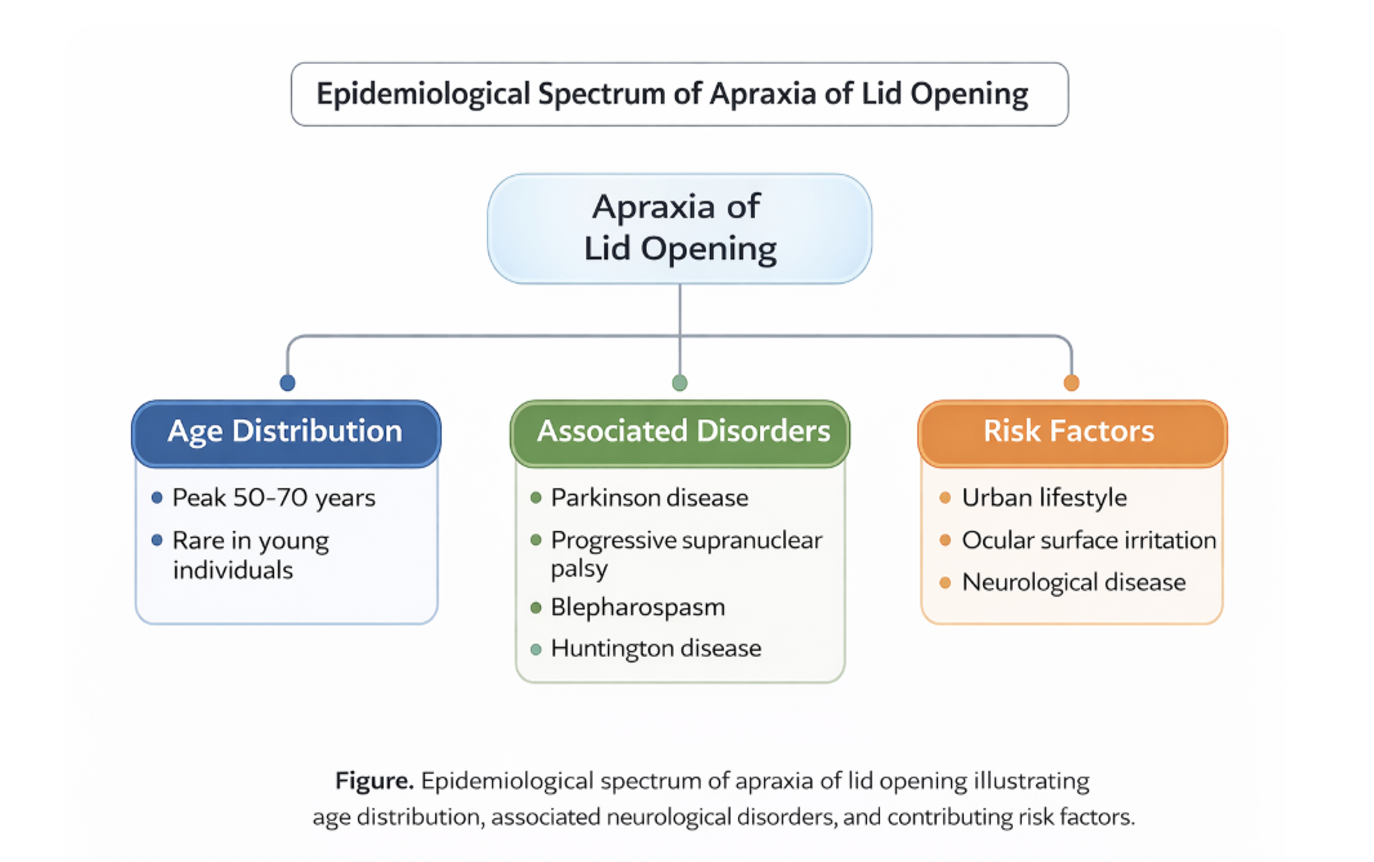
Epidemiology of Apraxia of Lid Opening. Infographic illustrating age distribution, associated neurologic disorders, and contributing risk factors.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
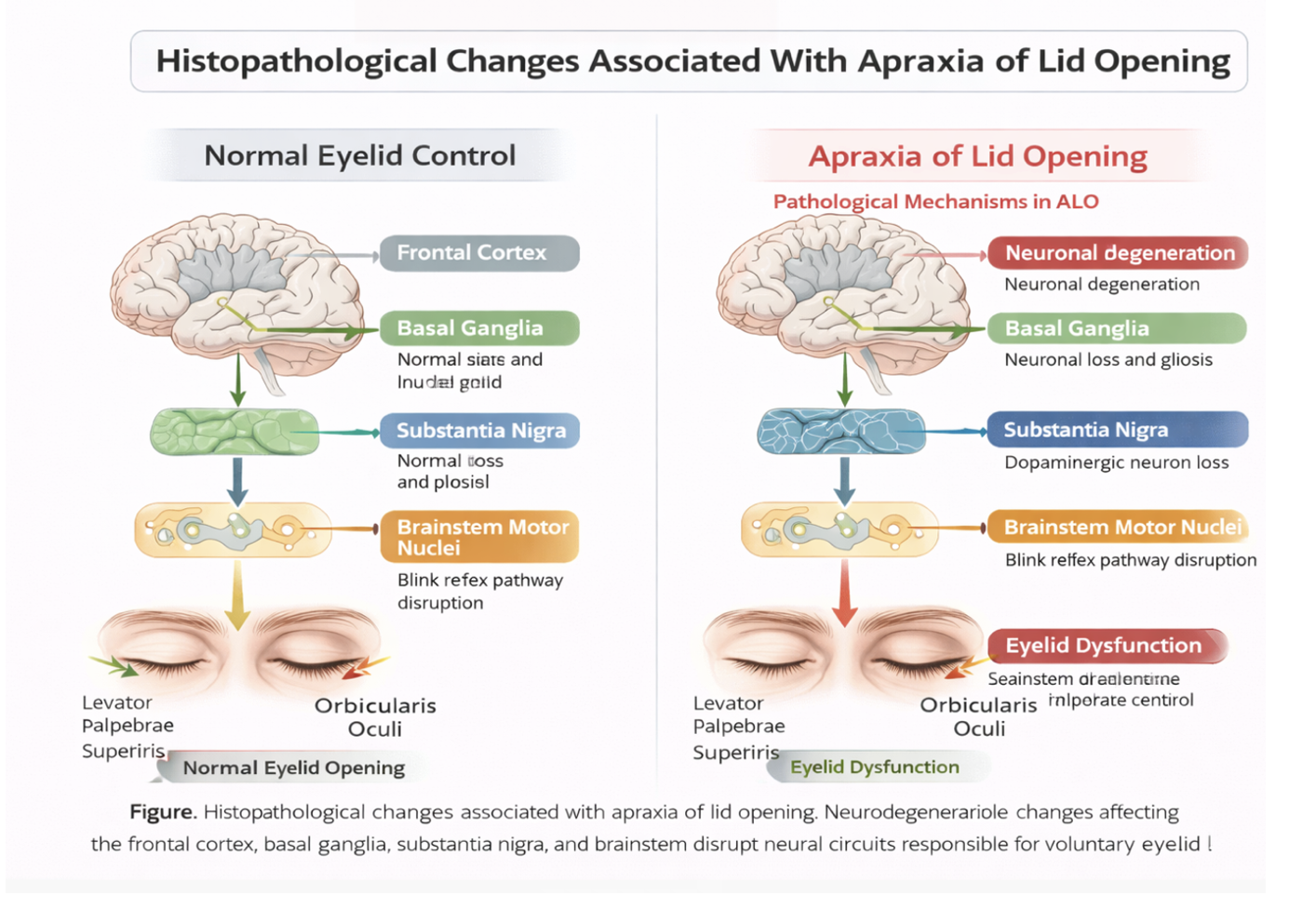
Histopathological Changes in Apraxia of Lid Opening. Diagram comparing normal eyelid control with pathological alterations in cortical, basal ganglia, substantia nigra, and brainstem pathways.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
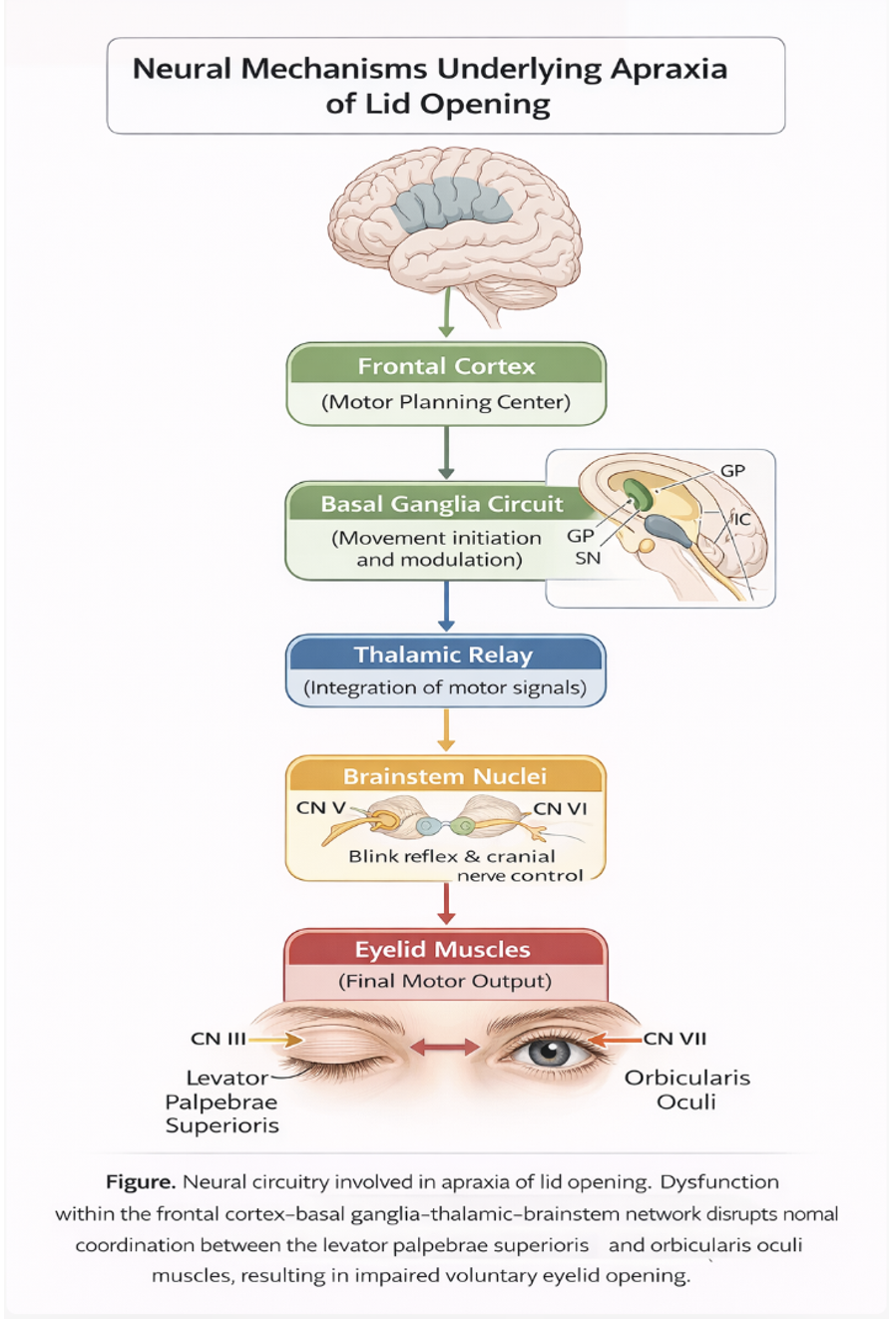
Neural Mechanisms of Apraxia of Lid Opening. Diagram illustrating disruption of the frontal cortex–basal ganglia–thalamic–brainstem network affecting eyelid motor control.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
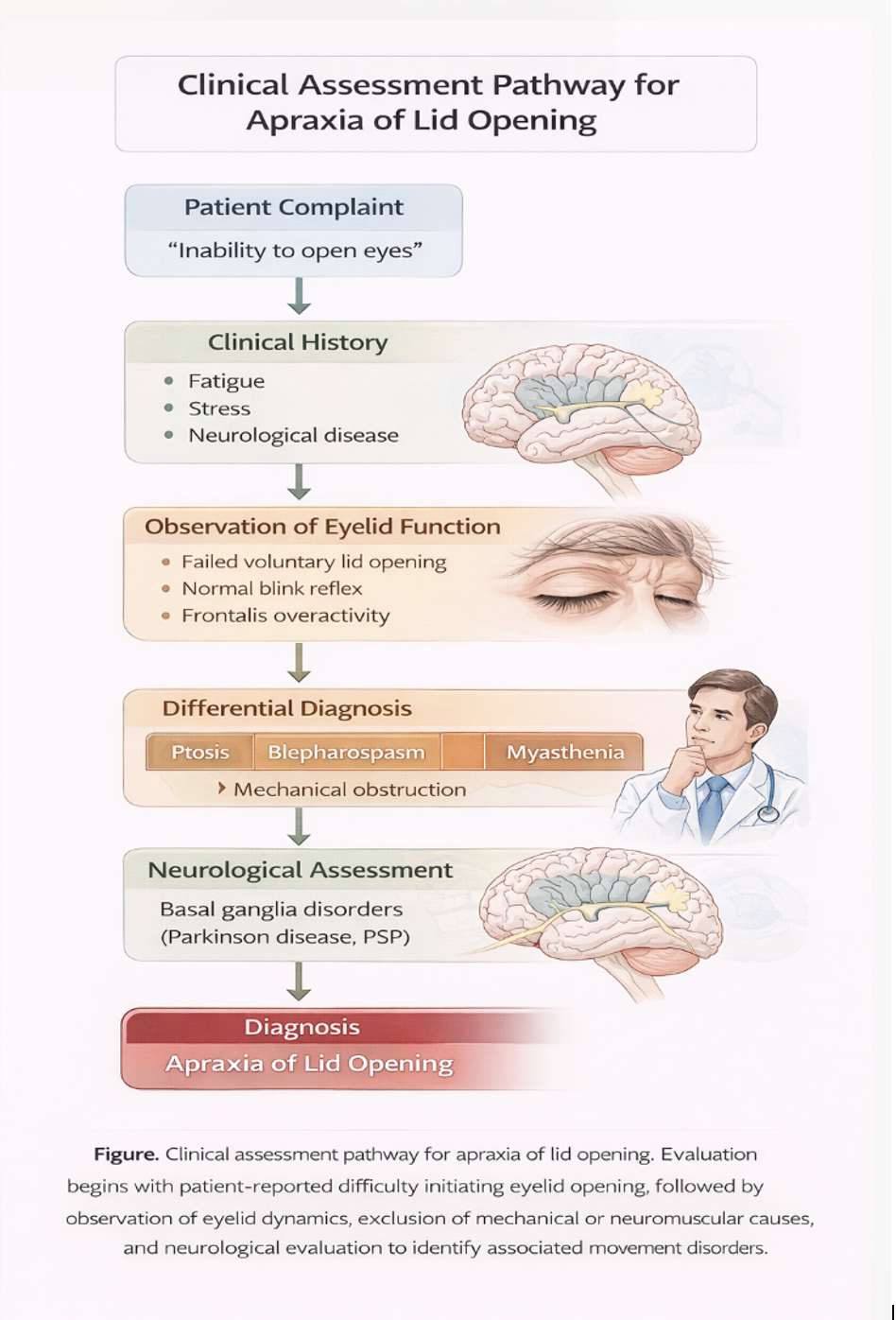
Clinical Assessment Pathway for Apraxia of Lid Opening. Flow diagram outlining history, examination, differential diagnosis, and neurologic evaluation leading to diagnosis.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
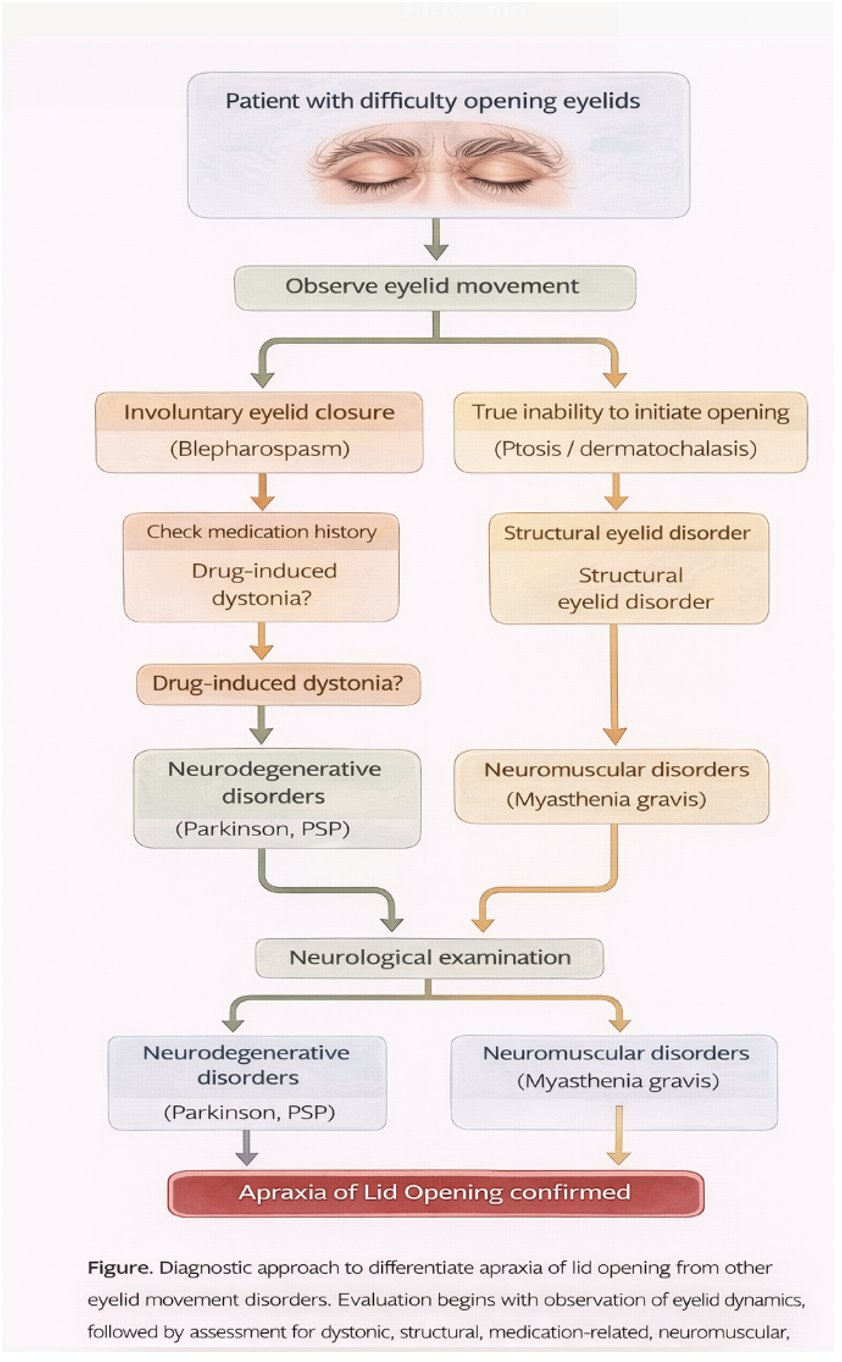
Diagnostic Approach to Apraxia of Lid Opening. Flow diagram illustrating differentiation from other eyelid movement disorders based on clinical features and underlying etiologies.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
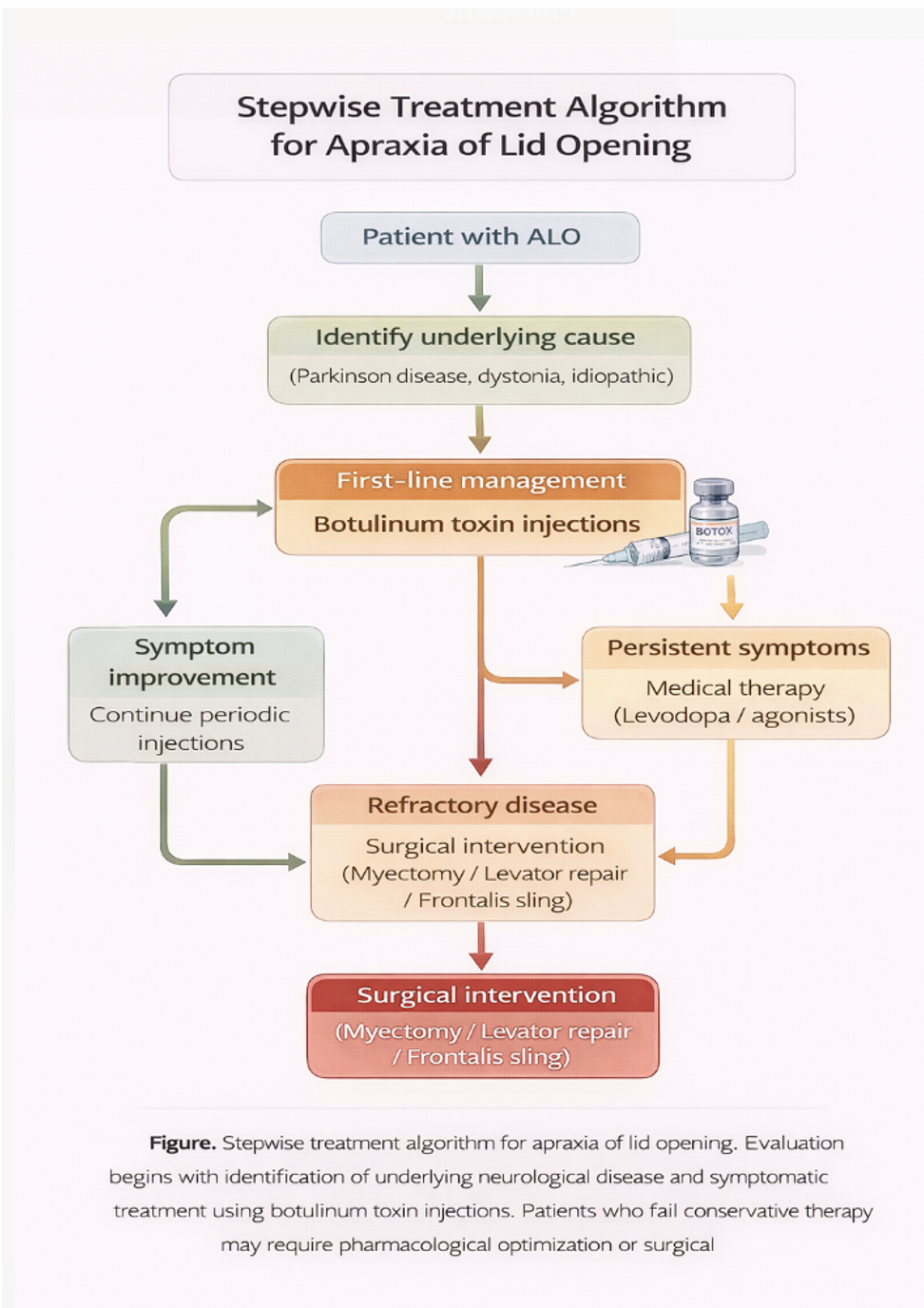
Stepwise Treatment Algorithm for Apraxia of Lid Opening. Diagram outlining escalation from botulinum toxin therapy to pharmacologic optimization and surgical intervention.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
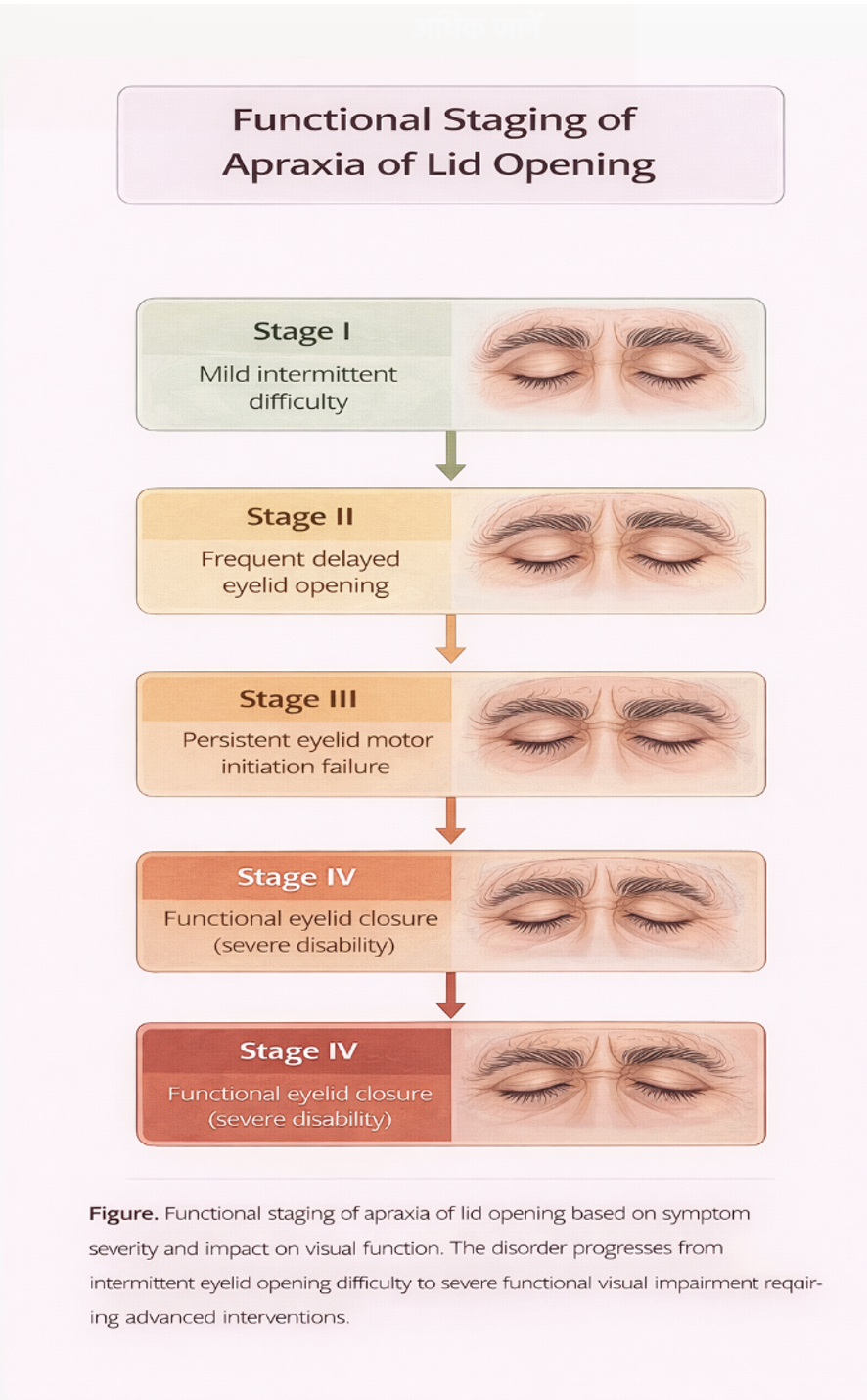
Functional Staging of Apraxia of Lid Opening. Diagram illustrating progression from intermittent eyelid opening difficulty to severe functional visual impairment.
Contributed by B Gurnani, MD
(Click Image to Enlarge)
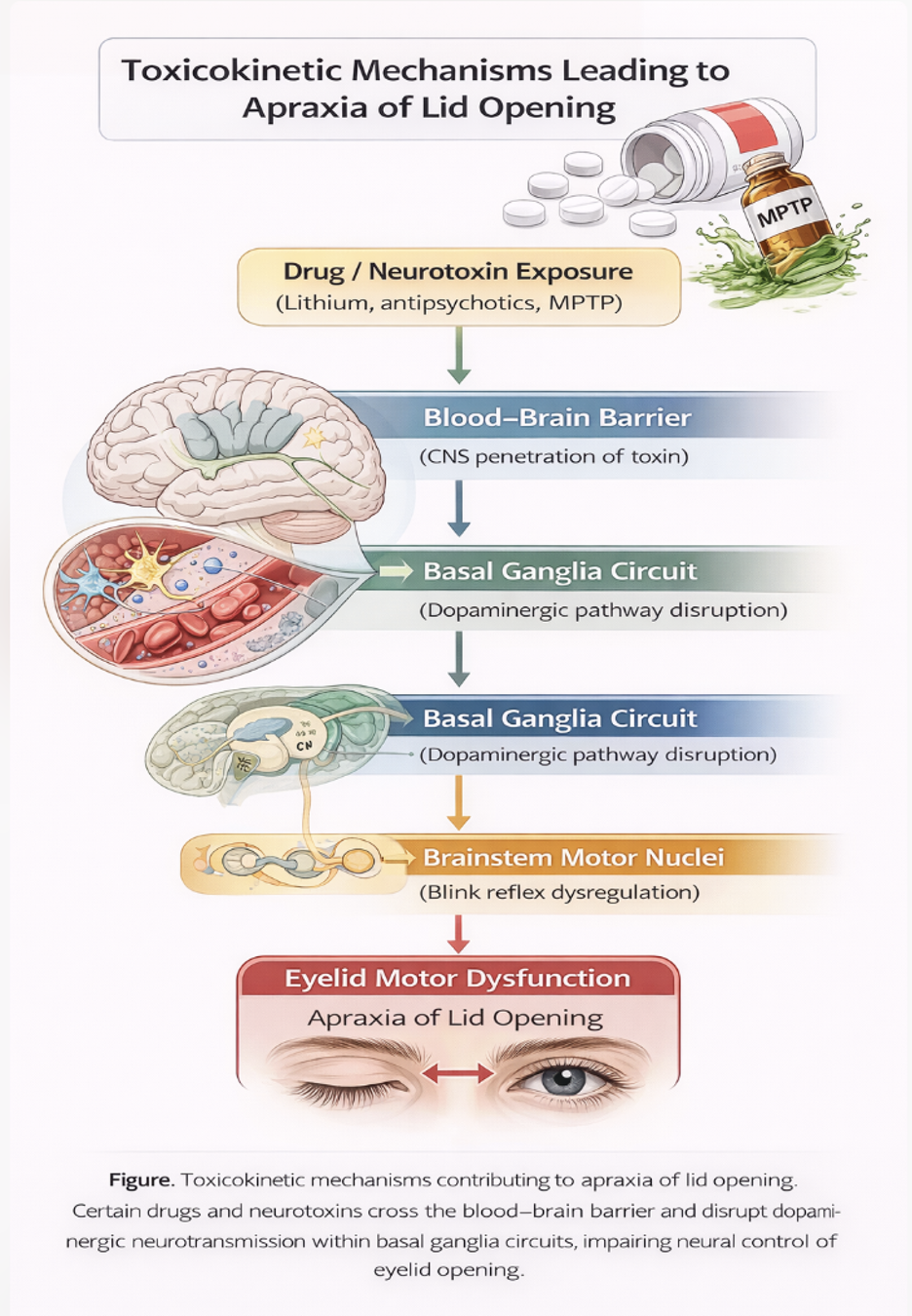
Toxicokinetic Mechanisms in Apraxia of Lid Opening. Diagram demonstrating how drugs and neurotoxins disrupt basal ganglia circuits and impair eyelid motor control.
Contributed by B Gurnani, MD
References
Boghen D. Apraxia of lid opening: a review. Neurology. 1997 Jun:48(6):1491-4 [PubMed PMID: 9191752]
Ugarte M, Teimory M. Apraxia of lid opening. The British journal of ophthalmology. 2007 Jul:91(7):854 [PubMed PMID: 17576707]
Knight B, Fakoya AO, Lopez MJ, Patel BC. Anatomy, Head and Neck: Levator Palpebrae Superioris Muscle. StatPearls. 2026 Jan:(): [PubMed PMID: 30725606]
GOLDSTEIN JE, COGAN DG. APRAXIA OF LID OPENING. Archives of ophthalmology (Chicago, Ill. : 1960). 1965 Feb:73():155-9 [PubMed PMID: 14237780]
Mustafa MM, Akram H, Oliva-Domínguez M, Kaski D. Functional positional eye and eyelid movements. Journal of neurology. 2020 Nov:267(11):3425-3428. doi: 10.1007/s00415-020-10071-7. Epub 2020 Jul 15 [PubMed PMID: 32671528]
Spadaro JZ, Patel N, Kahana A. Frontalis muscle flap eyelid reanimation technique in adults with severe ptosis or apraxia of eyelid opening. Orbit (Amsterdam, Netherlands). 2025 Jun:44(3):306-313. doi: 10.1080/01676830.2024.2381240. Epub 2024 Jul 29 [PubMed PMID: 39072581]
Rocha Cabrero F, De Jesus O. Apraxia of Lid Opening. StatPearls. 2026 Jan:(): [PubMed PMID: 32809377]
Hayashi K, Asano R, Sato M, Nakaya Y, Suzuki A, Takaku N, Hayashi K, Kobayashi Y. Efficacy of Trihexyphenidyl on Apraxia of Eyelid Opening in Parkinsonism: A Case Report. Cureus. 2024 Mar:16(3):e56232. doi: 10.7759/cureus.56232. Epub 2024 Mar 15 [PubMed PMID: 38618350]
Level 3 (low-level) evidencePhokaewvarangkul O, Bhidayasiri R. How to spot ocular abnormalities in progressive supranuclear palsy? A practical review. Translational neurodegeneration. 2019:8():20. doi: 10.1186/s40035-019-0160-1. Epub 2019 Jul 10 [PubMed PMID: 31333840]
Ting MA, Manta AI, Samia-Aly E, Lai M, de Carvalho ER, Buttery P, Ezra DG. Blepharospasm Secondary to Deep Brain Stimulation of the Subthalamic Nucleus in Parkinson Disease: Clinical Characteristics and Management Outcomes. Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society. 2024 Dec 1:44(4):517-522. doi: 10.1097/WNO.0000000000002064. Epub 2023 Dec 20 [PubMed PMID: 38117577]
Lamptey RNL, Chaulagain B, Trivedi R, Gothwal A, Layek B, Singh J. A Review of the Common Neurodegenerative Disorders: Current Therapeutic Approaches and the Potential Role of Nanotherapeutics. International journal of molecular sciences. 2022 Feb 6:23(3):. doi: 10.3390/ijms23031851. Epub 2022 Feb 6 [PubMed PMID: 35163773]
Wotipka E, Mortensen P, Charoenkijkajorn C, Pakravan M, Lee AG. Apraxia of lid opening in multiple sclerosis. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2023 Jun:58(3):e139-e141. doi: 10.1016/j.jcjo.2022.10.004. Epub 2022 Oct 19 [PubMed PMID: 36272441]
Thulasidas M, Patyal S, Narula R, Tiple SG. Spontaneous posterior dislocation of the cataractous lens in a patient with Parkinson-plus syndrome. American journal of ophthalmology case reports. 2022 Mar:25():101286. doi: 10.1016/j.ajoc.2022.101286. Epub 2022 Jan 22 [PubMed PMID: 35146184]
Level 3 (low-level) evidenceWarren S, May PJ. Macaque monkey trigeminal blink reflex circuits targeting levator palpebrae superioris motoneurons. The Journal of comparative neurology. 2021 Oct:529(14):3389-3409. doi: 10.1002/cne.25198. Epub 2021 Jun 11 [PubMed PMID: 34101199]
Level 2 (mid-level) evidenceKrishnan S, Shetty K, Puthanveedu DK, Kesavapisharady K, Thulaseedharan JV, Sarma G, Kishore A. Apraxia of Lid Opening in Subthalamic Nucleus Deep Brain Stimulation for Parkinson's Disease-Frequency, Risk Factors and Response to Treatment. Movement disorders clinical practice. 2021 May:8(4):587-593. doi: 10.1002/mdc3.13206. Epub 2021 Apr 12 [PubMed PMID: 33981792]
Lai HT, Chen AD, Lee SS, Lin YH, Lai CS. Myotomy In Situ for Essential Blepharospasm Refractory to Botulinum Toxin. Annals of plastic surgery. 2020 Jan:84(1S Suppl 1):S74-S79. doi: 10.1097/SAP.0000000000002182. Epub [PubMed PMID: 31833891]
Pula JH, Yuen CA. Eyes and stroke: the visual aspects of cerebrovascular disease. Stroke and vascular neurology. 2017 Dec:2(4):210-220. doi: 10.1136/svn-2017-000079. Epub 2017 Jul 6 [PubMed PMID: 29507782]
Han J, Lee SH, Shin HJ. Mini-incisional entropion repair for correcting involutional entropion: Full description and surgical outcome. Medicine. 2019 Aug:98(33):e16731. doi: 10.1097/MD.0000000000016731. Epub [PubMed PMID: 31415368]
Zeppieri M, Patel BC. Benign Essential Blepharospasm. StatPearls. 2026 Jan:(): [PubMed PMID: 32809668]
Dorsett M, Liang SY. Diagnosis and Treatment of Central Nervous System Infections in the Emergency Department. Emergency medicine clinics of North America. 2016 Nov:34(4):917-942. doi: 10.1016/j.emc.2016.06.013. Epub [PubMed PMID: 27741995]
Swarup S, Ahmed I, Grigorova Y, Zeltser R. Metabolic Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 29083742]
Jaishankar M, Tseten T, Anbalagan N, Mathew BB, Beeregowda KN. Toxicity, mechanism and health effects of some heavy metals. Interdisciplinary toxicology. 2014 Jun:7(2):60-72. doi: 10.2478/intox-2014-0009. Epub 2014 Nov 15 [PubMed PMID: 26109881]
Bhagavati S. Autoimmune Disorders of the Nervous System: Pathophysiology, Clinical Features, and Therapy. Frontiers in neurology. 2021:12():664664. doi: 10.3389/fneur.2021.664664. Epub 2021 Apr 14 [PubMed PMID: 33935958]
Fernández E, Latasiewicz M, Pelegrin L, Romera M, Schellini S, Galindo-Ferreiro A. Botulinum toxin for treating unilateral apraxia of eyelid opening in a patient with congenital myotonia. Arquivos brasileiros de oftalmologia. 2017 Sep-Oct:80(5):330-331. doi: 10.5935/0004-2749.20170081. Epub [PubMed PMID: 29160548]
Hamedani AG, Gold DR. Eyelid Dysfunction in Neurodegenerative, Neurogenetic, and Neurometabolic Disease. Frontiers in neurology. 2017:8():329. doi: 10.3389/fneur.2017.00329. Epub 2017 Jul 18 [PubMed PMID: 28769865]
Bhattacharjee K, Misra DK, Deori N. Updates on upper eyelid blepharoplasty. Indian journal of ophthalmology. 2017 Jul:65(7):551-558. doi: 10.4103/ijo.IJO_540_17. Epub [PubMed PMID: 28724810]
Wang ZF. A case of Parkinson's disease with apraxia of lid opening and freezing of gait. Chinese medical journal. 2011 Nov:124(21):3600 [PubMed PMID: 22340186]
Level 3 (low-level) evidenceSun Y, Tsai PJ, Chu CL, Huang WC, Bee YS. Epidemiology of benign essential blepharospasm: A nationwide population-based retrospective study in Taiwan. PloS one. 2018:13(12):e0209558. doi: 10.1371/journal.pone.0209558. Epub 2018 Dec 26 [PubMed PMID: 30586395]
Level 2 (mid-level) evidenceDressler D, Karapantzou C, Rohrbach S, Schneider S, Laskawi R. Frontalis suspension surgery to treat patients with blepharospasm and eyelid opening apraxia: long-term results. Journal of neural transmission (Vienna, Austria : 1996). 2017 Feb:124(2):253-257. doi: 10.1007/s00702-016-1641-3. Epub 2016 Nov 5 [PubMed PMID: 27816991]
Karapantzou C, Dressler D, Rohrbach S, Laskawi R. Frontalis suspension surgery to treat patients with essential blepharospasm and apraxia of eyelid opening-technique and results. Head & face medicine. 2014 Oct 22:10():44. doi: 10.1186/1746-160X-10-44. Epub 2014 Oct 22 [PubMed PMID: 25338619]
Level 2 (mid-level) evidenceIyengar SS, Narasingan SN, Gandhi P, Jaipuriar N, Mahilmaran A, Patil S, Abhyankar MV, Revankar S. Risk factors, comorbiditiEs and Atherogenic dysLipidaemia in Indian YOUNG patients with dyslipidaemia attending hospital/clinic: REAL YOUNG (dyslipidaemia) study. Journal of family medicine and primary care. 2020 Aug:9(8):4156-4164. doi: 10.4103/jfmpc.jfmpc_546_20. Epub 2020 Aug 25 [PubMed PMID: 33110825]
Weiss D, Wächter T, Breit S, Jacob SN, Pomper JK, Asmus F, Valls-Solé J, Plewnia C, Gasser T, Gharabaghi A, Krüger R. Involuntary eyelid closure after STN-DBS: evidence for different pathophysiological entities. Journal of neurology, neurosurgery, and psychiatry. 2010 Sep:81(9):1002-7. doi: 10.1136/jnnp.2009.196691. Epub 2010 Jun 20 [PubMed PMID: 20562465]
Yanagisawa N. Functions and dysfunctions of the basal ganglia in humans. Proceedings of the Japan Academy. Series B, Physical and biological sciences. 2018:94(7):275-304. doi: 10.2183/pjab.94.019. Epub [PubMed PMID: 30078828]
Beckers M, Bloem BR, Verbeek MM. Mechanisms of peripheral levodopa resistance in Parkinson's disease. NPJ Parkinson's disease. 2022 May 11:8(1):56. doi: 10.1038/s41531-022-00321-y. Epub 2022 May 11 [PubMed PMID: 35546556]
Teleanu RI, Niculescu AG, Roza E, Vladâcenco O, Grumezescu AM, Teleanu DM. Neurotransmitters-Key Factors in Neurological and Neurodegenerative Disorders of the Central Nervous System. International journal of molecular sciences. 2022 May 25:23(11):. doi: 10.3390/ijms23115954. Epub 2022 May 25 [PubMed PMID: 35682631]
Pirau L, Lui F. Frontal Lobe Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30422576]
Wallwork SB, Talbot K, Camfferman D, Moseley GL, Iannetti GD. The blink reflex magnitude is continuously adjusted according to both current and predicted stimulus position with respect to the face. Cortex; a journal devoted to the study of the nervous system and behavior. 2016 Aug:81():168-75. doi: 10.1016/j.cortex.2016.04.009. Epub 2016 Apr 22 [PubMed PMID: 27236372]
Asan AS, McIntosh JR, Carmel JB. Targeting Sensory and Motor Integration for Recovery of Movement After CNS Injury. Frontiers in neuroscience. 2021:15():791824. doi: 10.3389/fnins.2021.791824. Epub 2022 Jan 21 [PubMed PMID: 35126040]
Peckham EL, Hallett M. Psychogenic movement disorders. Neurologic clinics. 2009 Aug:27(3):801-19, vii. doi: 10.1016/j.ncl.2009.04.008. Epub [PubMed PMID: 19555832]
Adeyinka A, Layer DA. Neuromuscular Blocking Agents. StatPearls. 2026 Jan:(): [PubMed PMID: 30725853]
Mohseni M, Gurnani B, Blair K. Blunt Eye Trauma. StatPearls. 2026 Jan:(): [PubMed PMID: 29261988]
Hoffmann M. The human frontal lobes and frontal network systems: an evolutionary, clinical, and treatment perspective. ISRN neurology. 2013:2013():892459. doi: 10.1155/2013/892459. Epub 2013 Mar 14 [PubMed PMID: 23577266]
Level 3 (low-level) evidenceStoker TB, Greenland JC, Kouli A, Torsney KM, Kuan WL. Parkinson’s Disease: Etiology, Neuropathology, and Pathogenesis. Parkinson’s Disease: Pathogenesis and Clinical Aspects. 2018 Dec 21:(): [PubMed PMID: 30702842]
Dimitriou J, Montoute T, Levivier M, Borruat FX, Diserens K. Bilateral ptosis: Lesion in the oculomotor nuclei or supranuclear lesion? NeuroRehabilitation. 2015:36(3):323-7. doi: 10.3233/NRE-151220. Epub [PubMed PMID: 26409335]
Lepeta K, Lourenco MV, Schweitzer BC, Martino Adami PV, Banerjee P, Catuara-Solarz S, de La Fuente Revenga M, Guillem AM, Haidar M, Ijomone OM, Nadorp B, Qi L, Perera ND, Refsgaard LK, Reid KM, Sabbar M, Sahoo A, Schaefer N, Sheean RK, Suska A, Verma R, Vicidomini C, Wright D, Zhang XD, Seidenbecher C. Synaptopathies: synaptic dysfunction in neurological disorders - A review from students to students. Journal of neurochemistry. 2016 Sep:138(6):785-805. doi: 10.1111/jnc.13713. Epub 2016 Sep 8 [PubMed PMID: 27333343]
Level 2 (mid-level) evidenceBenghanem S, Mazeraud A, Azabou E, Chhor V, Shinotsuka CR, Claassen J, Rohaut B, Sharshar T. Brainstem dysfunction in critically ill patients. Critical care (London, England). 2020 Jan 6:24(1):5. doi: 10.1186/s13054-019-2718-9. Epub 2020 Jan 6 [PubMed PMID: 31907011]
Juárez Olguín H, Calderón Guzmán D, Hernández García E, Barragán Mejía G. The Role of Dopamine and Its Dysfunction as a Consequence of Oxidative Stress. Oxidative medicine and cellular longevity. 2016:2016():9730467. doi: 10.1155/2016/9730467. Epub 2015 Dec 6 [PubMed PMID: 26770661]
Rabiu TB. Revisiting the eye opening response of the Glasgow Coma Scale. Indian journal of critical care medicine : peer-reviewed, official publication of Indian Society of Critical Care Medicine. 2011 Jan:15(1):58-9. doi: 10.4103/0972-5229.78231. Epub [PubMed PMID: 21633551]
Stoker TB, Greenland JC, Greenland JC, Barker RA. The Differential Diagnosis of Parkinson’s Disease. Parkinson’s Disease: Pathogenesis and Clinical Aspects. 2018 Dec 21:(): [PubMed PMID: 30702839]
Meer E, Grob S, Antonsen EL, Sawyer A. Ocular conditions and injuries, detection and management in spaceflight. NPJ microgravity. 2023 May 16:9(1):37. doi: 10.1038/s41526-023-00279-y. Epub 2023 May 16 [PubMed PMID: 37193709]
Kohsaka M, Oeda T, Umemura A, Tomita S, Park K, Yamamoto K, Sugiyama H, Sawada H. Oxybuprocaine for apraxia of lid opening in Parkinson's disease: A placebo-controlled pilot trial. Movement disorders : official journal of the Movement Disorder Society. 2018 Mar:33(3):494-495. doi: 10.1002/mds.27243. Epub 2017 Nov 23 [PubMed PMID: 29168901]
Level 3 (low-level) evidenceDefazio G, Hallett M, Jinnah HA, Berardelli A. Development and validation of a clinical guideline for diagnosing blepharospasm. Neurology. 2013 Jul 16:81(3):236-40. doi: 10.1212/WNL.0b013e31829bfdf6. Epub 2013 Jun 14 [PubMed PMID: 23771487]
Level 1 (high-level) evidenceLi S, Nguyen IP, Urbanczyk K. Common infectious diseases of the central nervous system-clinical features and imaging characteristics. Quantitative imaging in medicine and surgery. 2020 Dec:10(12):2227-2259. doi: 10.21037/qims-20-886. Epub [PubMed PMID: 33269224]
Level 2 (mid-level) evidenceChalela JA, Kidwell CS, Nentwich LM, Luby M, Butman JA, Demchuk AM, Hill MD, Patronas N, Latour L, Warach S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison. Lancet (London, England). 2007 Jan 27:369(9558):293-8 [PubMed PMID: 17258669]
Krack P, Marion MH. "Apraxia of lid opening," a focal eyelid dystonia: clinical study of 32 patients. Movement disorders : official journal of the Movement Disorder Society. 1994 Nov:9(6):610-5 [PubMed PMID: 7845400]
Scorr LM, Cho HJ, Kilic-Berkmen G, McKay JL, Hallett M, Klein C, Baumer T, Berman BD, Feuerstein JS, Perlmutter JS, Berardelli A, Ferrazzano G, Wagle-Shukla A, Malaty IA, Jankovic J, Bellows ST, Barbano RL, Vidailhet M, Roze E, Bonnet C, Mahajan A, LeDoux MS, Fung VSC, Chang FCF, Defazio G, Ercoli T, Factor S, Wojno T, Jinnah HA. Clinical Features and Evolution of Blepharospasm: A Multicenter International Cohort and Systematic Literature Review. Dystonia (Lausanne, Switzerland). 2022:1():. pii: 10359. doi: 10.3389/dyst.2022.10359. Epub 2022 May 16 [PubMed PMID: 36248010]
Level 1 (high-level) evidenceWilkes J. AAN Updates Guidelines on the Uses of Botulinum Neurotoxin. American family physician. 2017 Feb 1:95(3):198-199 [PubMed PMID: 28145664]
Simpson DM, Hallett M, Ashman EJ, Comella CL, Green MW, Gronseth GS, Armstrong MJ, Gloss D, Potrebic S, Jankovic J, Karp BP, Naumann M, So YT, Yablon SA. Practice guideline update summary: Botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache [RETIRED]: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2016 May 10:86(19):1818-26. doi: 10.1212/WNL.0000000000002560. Epub 2016 Apr 18 [PubMed PMID: 27164716]
Level 1 (high-level) evidenceConnolly BS, Lang AE. Pharmacological treatment of Parkinson disease: a review. JAMA. 2014 Apr 23-30:311(16):1670-83. doi: 10.1001/jama.2014.3654. Epub [PubMed PMID: 24756517]
Hellman A, Torres-Russotto D. Botulinum toxin in the management of blepharospasm: current evidence and recent developments. Therapeutic advances in neurological disorders. 2015 Mar:8(2):82-91. doi: 10.1177/1756285614557475. Epub [PubMed PMID: 25922620]
Level 3 (low-level) evidenceKerty E, Eidal K. Apraxia of eyelid opening: clinical features and therapy. European journal of ophthalmology. 2006 Mar-Apr:16(2):204-8 [PubMed PMID: 16703535]
Azuma R, Aoki S, Aizawa T, Kuwabara M, Kiyosawa T. The vertical orbicularis oculi muscle turn-over procedure for the correction of paralytic ectropion of the lower eyelid. Archives of plastic surgery. 2018 Mar:45(2):135-139. doi: 10.5999/aps.2017.01235. Epub 2018 Mar 5 [PubMed PMID: 29506332]
Patel N, Jankovic J, Hallett M. Sensory aspects of movement disorders. The Lancet. Neurology. 2014 Jan:13(1):100-12. doi: 10.1016/S1474-4422(13)70213-8. Epub [PubMed PMID: 24331796]
Level 3 (low-level) evidenceRamos VF, Karp BI, Hallett M. Tricks in dystonia: ordering the complexity. Journal of neurology, neurosurgery, and psychiatry. 2014 Sep:85(9):987-93. doi: 10.1136/jnnp-2013-306971. Epub 2014 Jan 31 [PubMed PMID: 24487380]
Marsden CD. Blepharospasm-oromandibular dystonia syndrome (Brueghel's syndrome). A variant of adult-onset torsion dystonia? Journal of neurology, neurosurgery, and psychiatry. 1976 Dec:39(12):1204-9 [PubMed PMID: 1011031]
Marsden CD. The problem of adult-onset idiopathic torsion dystonia and other isolated dyskinesias in adult life (including blepharospasm, oromandibular dystonia, dystonic writer's cramp, and torticollis, or axial dystonia). Advances in neurology. 1976:14():259-76 [PubMed PMID: 941774]
Level 3 (low-level) evidenceZádori D, Veres G, Szalárdy L, Klivényi P, Vécsei L. Drug-induced movement disorders. Expert opinion on drug safety. 2015 Jun:14(6):877-90. doi: 10.1517/14740338.2015.1032244. Epub [PubMed PMID: 25981904]
Level 3 (low-level) evidenceDefazio G, De Mari M, De Salvia R, Lamberti P, Giorelli M, Livrea P. "Apraxia of eyelid opening" induced by levodopa therapy and apomorphine in atypical parkinsonism (possible progressive supranuclear palsy): a case report. Clinical neuropharmacology. 1999 Sep-Oct:22(5):292-4 [PubMed PMID: 10516881]
Level 3 (low-level) evidenceUmemura A, Toyoda T, Yamamoto K, Oka Y, Ishii F, Yamada K. Apraxia of eyelid opening after subthalamic deep brain stimulation may be caused by reduction of levodopa. Parkinsonism & related disorders. 2008 Dec:14(8):655-7. doi: 10.1016/j.parkreldis.2007.12.008. Epub 2008 Mar 3 [PubMed PMID: 18316231]
Level 3 (low-level) evidenceVagefi MR, Lin CC, McCann JD, Anderson RL. Exacerbation of blepharospasm associated with craniocervical dystonia after placement of bilateral globus pallidus internus deep brain stimulator. Movement disorders : official journal of the Movement Disorder Society. 2008 Feb 15:23(3):454-6 [PubMed PMID: 18074391]
Level 3 (low-level) evidenceDefazio G, Matarin M, Peckham EL, Martino D, Valente EM, Singleton A, Crawley A, Aniello MS, Brancati F, Abbruzzese G, Girlanda P, Livrea P, Hallett M, Berardelli A. The TOR1A polymorphism rs1182 and the risk of spread in primary blepharospasm. Movement disorders : official journal of the Movement Disorder Society. 2009 Mar 15:24(4):613-6. doi: 10.1002/mds.22471. Epub [PubMed PMID: 19202559]
Level 2 (mid-level) evidenceSiokas V, Dardiotis E, Tsironi EE, Tsivgoulis G, Rikos D, Sokratous M, Koutsias S, Paterakis K, Deretzi G, Hadjigeorgiou GM. The Role of TOR1A Polymorphisms in Dystonia: A Systematic Review and Meta-Analysis. PloS one. 2017:12(1):e0169934. doi: 10.1371/journal.pone.0169934. Epub 2017 Jan 12 [PubMed PMID: 28081261]
Level 1 (high-level) evidenceChen Y, Chen K, Burgunder JM, Song W, Huang R, Zhao B, Cao B, Chen X, Jiang Y, Shang HF. Association of rs1182 polymorphism of the DYT1 gene with primary dystonia in Chinese population. Journal of the neurological sciences. 2012 Dec 15:323(1-2):228-31. doi: 10.1016/j.jns.2012.09.025. Epub 2012 Oct 9 [PubMed PMID: 23058565]
Level 2 (mid-level) evidenceFuchs T, Saunders-Pullman R, Masuho I, Luciano MS, Raymond D, Factor S, Lang AE, Liang TW, Trosch RM, White S, Ainehsazan E, Hervé D, Sharma N, Ehrlich ME, Martemyanov KA, Bressman SB, Ozelius LJ. Mutations in GNAL cause primary torsion dystonia. Nature genetics. 2013 Jan:45(1):88-92. doi: 10.1038/ng.2496. Epub 2012 Dec 9 [PubMed PMID: 23222958]
Charlesworth G, Plagnol V, Holmström KM, Bras J, Sheerin UM, Preza E, Rubio-Agusti I, Ryten M, Schneider SA, Stamelou M, Trabzuni D, Abramov AY, Bhatia KP, Wood NW. Mutations in ANO3 cause dominant craniocervical dystonia: ion channel implicated in pathogenesis. American journal of human genetics. 2012 Dec 7:91(6):1041-50. doi: 10.1016/j.ajhg.2012.10.024. Epub 2012 Nov 29 [PubMed PMID: 23200863]
Hersheson J, Mencacci NE, Davis M, MacDonald N, Trabzuni D, Ryten M, Pittman A, Paudel R, Kara E, Fawcett K, Plagnol V, Bhatia KP, Medlar AJ, Stanescu HC, Hardy J, Kleta R, Wood NW, Houlden H. Mutations in the autoregulatory domain of β-tubulin 4a cause hereditary dystonia. Annals of neurology. 2013 Apr:73(4):546-53. doi: 10.1002/ana.23832. Epub 2013 Feb 19 [PubMed PMID: 23424103]
Level 3 (low-level) evidenceXiao J, Uitti RJ, Zhao Y, Vemula SR, Perlmutter JS, Wszolek ZK, Maraganore DM, Auburger G, Leube B, Lehnhoff K, LeDoux MS. Mutations in CIZ1 cause adult onset primary cervical dystonia. Annals of neurology. 2012 Apr:71(4):458-69. doi: 10.1002/ana.23547. Epub 2012 Mar 23 [PubMed PMID: 22447717]
Khooshnoodi MA, Factor SA, Jinnah HA. Secondary blepharospasm associated with structural lesions of the brain. Journal of the neurological sciences. 2013 Aug 15:331(1-2):98-101. doi: 10.1016/j.jns.2013.05.022. Epub 2013 Jun 6 [PubMed PMID: 23747003]
Level 1 (high-level) evidenceHara K, Matsuda A, Kitsukawa Y, Tanaka K, Nishizawa M, Tagawa A. Botulinum toxin treatment for blepharospasm associated with myasthenia gravis. Movement disorders : official journal of the Movement Disorder Society. 2007 Jul 15:22(9):1363-4 [PubMed PMID: 17486596]
Level 3 (low-level) evidenceKurlan R, Jankovic J, Rubin A, Patten B, Griggs R, Shoulson I. Coexistent Meige's syndrome and myasthenia gravis. A relationship between blinking and extraocular muscle fatigue? Archives of neurology. 1987 Oct:44(10):1057-60 [PubMed PMID: 3632379]
Level 3 (low-level) evidenceAgarwal S, Gilbert R. Progressive Supranuclear Palsy. StatPearls. 2026 Jan:(): [PubMed PMID: 30252354]
Cornett EM, Novitch M, Kaye AD, Kata V, Kaye AM. Medication-Induced Tardive Dyskinesia: A Review and Update. Ochsner journal. 2017 Summer:17(2):162-174 [PubMed PMID: 28638290]
Finsterer J. Ptosis: causes, presentation, and management. Aesthetic plastic surgery. 2003 May-Jun:27(3):193-204 [PubMed PMID: 12925861]
Jarrett A, Emery JM, Coats AC, Justice J Jr. Voluntary nystagmus. Annals of ophthalmology. 1977 Jul:9(7):853-9 [PubMed PMID: 900720]
Yoon WT, Chung EJ, Lee SH, Kim BJ, Lee WY. Clinical analysis of blepharospasm and apraxia of eyelid opening in patients with parkinsonism. Journal of clinical neurology (Seoul, Korea). 2005 Oct:1(2):159-65. doi: 10.3988/jcn.2005.1.2.159. Epub 2005 Oct 20 [PubMed PMID: 20396463]
Krack P, Volkmann J, Tinkhauser G, Deuschl G. Deep Brain Stimulation in Movement Disorders: From Experimental Surgery to Evidence-Based Therapy. Movement disorders : official journal of the Movement Disorder Society. 2019 Dec:34(12):1795-1810. doi: 10.1002/mds.27860. Epub 2019 Oct 3 [PubMed PMID: 31580535]
Skopljak-Salkica A, Gabric I, Jagic M, Bejdic N, Biscevic A, Ahmedbegovic-Pjano M. Clinical Study on the Use of Botulinum Toxin for Blepharospasm and Hemifacial Spasm. Medical archives (Sarajevo, Bosnia and Herzegovina). 2024:78(4):326-328. doi: 10.5455/medarh.2024.78.326-328. Epub [PubMed PMID: 39981145]
Forget R, Tozlovanu V, Iancu A, Boghen D. Botulinum toxin improves lid opening delays in blepharospasm-associated apraxia of lid opening. Neurology. 2002 Jun 25:58(12):1843-6 [PubMed PMID: 12084888]
Horwath-Winter J, Bergloeff J, Floegel I, Haller-Schober EM, Schmut O. Botulinum toxin A treatment in patients suffering from blepharospasm and dry eye. The British journal of ophthalmology. 2003 Jan:87(1):54-6 [PubMed PMID: 12488263]
Witmanowski H, Błochowiak K. The whole truth about botulinum toxin - a review. Postepy dermatologii i alergologii. 2020 Dec:37(6):853-861. doi: 10.5114/ada.2019.82795. Epub 2019 Feb 5 [PubMed PMID: 33603602]
Suzuki Y, Kiyosawa M, Mochizuki M, Ishiwata K, Ishii K. The pre-supplementary and primary motor areas generate rhythm for voluntary eye opening and closing movements. The Tohoku journal of experimental medicine. 2010 Oct:222(2):97-104 [PubMed PMID: 20877165]
Tommasi G, Krack P, Fraix V, Pollak P. Effects of varying subthalamic nucleus stimulation on apraxia of lid opening in Parkinson's disease. Journal of neurology. 2012 Sep:259(9):1944-50. doi: 10.1007/s00415-012-6447-0. Epub 2012 Feb 17 [PubMed PMID: 22349870]
Mezaki T. [Clinical characteristics and treatment of dystonia]. Rinsho shinkeigaku = Clinical neurology. 2011 Jul:51(7):465-70 [PubMed PMID: 21823504]
Mezaki T. Dystonia redefined as central non-paretic loss of control of muscle action: a concept including inability to activate muscles required for a specific movement, or 'negative dystonia'. Medical hypotheses. 2007:69(6):1309-12 [PubMed PMID: 17548169]
Duarte GS, Rodrigues FB, Marques RE, Castelão M, Ferreira J, Sampaio C, Moore AP, Costa J. Botulinum toxin type A therapy for blepharospasm. The Cochrane database of systematic reviews. 2020 Nov 19:11(11):CD004900. doi: 10.1002/14651858.CD004900.pub3. Epub 2020 Nov 19 [PubMed PMID: 33211907]
Level 1 (high-level) evidenceCoughlin DG, Litvan I. Progressive supranuclear palsy: Advances in diagnosis and management. Parkinsonism & related disorders. 2020 Apr:73():105-116. doi: 10.1016/j.parkreldis.2020.04.014. Epub 2020 May 25 [PubMed PMID: 32487421]
Level 3 (low-level) evidenceRowe JB, Holland N, Rittman T. Progressive supranuclear palsy: diagnosis and management. Practical neurology. 2021 Oct:21(5):376-383. doi: 10.1136/practneurol-2020-002794. Epub 2021 Jul 2 [PubMed PMID: 34215700]
Ramirez-Castaneda J, Jankovic J. Long-term efficacy, safety, and side effect profile of botulinum toxin in dystonia: a 20-year follow-up. Toxicon : official journal of the International Society on Toxinology. 2014 Nov:90():344-8. doi: 10.1016/j.toxicon.2014.07.009. Epub 2014 Aug 15 [PubMed PMID: 25130293]
Level 2 (mid-level) evidenceJochim A, Meindl T, Huber C, Mantel T, Zwirner S, Castrop F, Haslinger B. Treatment of blepharospasm and Meige's syndrome with abo- and onabotulinumtoxinA: long-term safety and efficacy in daily clinical practice. Journal of neurology. 2020 Jan:267(1):267-275. doi: 10.1007/s00415-019-09581-w. Epub 2019 Oct 19 [PubMed PMID: 31630241]
Diep D, Ko J, Lan J, Koprowicz KT, Ko G. Benefits, Safety, and Adjunct Modality Prevalences of Long-Term Botulinum Toxin Injections for Cervical Dystonia and Myofascial Neck Pain: A Retrospective Cohort Study. Journal of pain research. 2020:13():1297-1304. doi: 10.2147/JPR.S254032. Epub 2020 Jun 3 [PubMed PMID: 32581571]
Level 2 (mid-level) evidenceMiller DD, Hasan SA, Simmons NL, Stewart MW. Recurrent corneal erosion: a comprehensive review. Clinical ophthalmology (Auckland, N.Z.). 2019:13():325-335. doi: 10.2147/OPTH.S157430. Epub 2019 Feb 11 [PubMed PMID: 30809089]
Lee D, Lee S. The influence of social withdrawal and depression on the self-esteem of female adolescents: The mediating effect of grit. PloS one. 2023:18(7):e0288530. doi: 10.1371/journal.pone.0288530. Epub 2023 Jul 12 [PubMed PMID: 37437061]
Armstrong RA. Visual signs and symptoms of progressive supranuclear palsy. Clinical & experimental optometry. 2011 Mar:94(2):150-60. doi: 10.1111/j.1444-0938.2010.00504.x. Epub [PubMed PMID: 20629667]
Noda K, Kobayashi T, Matsuoka S, Takanashi M, Kanazawa A, Mizuno Y. [A 65-year-old man with rigid-bradykinetic parkinsonism, vertical gaze palsy, difficulty of eye-lid opening, and marked pseudo-bulbar palsy]. No to shinkei = Brain and nerve. 2005 Jan:57(1):73-86 [PubMed PMID: 15782604]
An SH, Jin SW, Kwon YH, Ryu WY, Jeong WJ, Ahn HB. Effects of upper lid blepharoplasty on visual quality in patients with lash ptosis and dermatochalasis. International journal of ophthalmology. 2016:9(9):1320-4. doi: 10.18240/ijo.2016.09.15. Epub 2016 Sep 18 [PubMed PMID: 27672599]
Level 2 (mid-level) evidenceAkhtar A, Macfarlane RJ, Waseem M. Pre-operative assessment and post-operative care in elective shoulder surgery. The open orthopaedics journal. 2013:7():316-22. doi: 10.2174/1874325001307010316. Epub 2013 Sep 6 [PubMed PMID: 24093051]
Pollock A, Baer G, Campbell P, Choo PL, Forster A, Morris J, Pomeroy VM, Langhorne P. Physical rehabilitation approaches for the recovery of function and mobility following stroke. The Cochrane database of systematic reviews. 2014 Apr 22:2014(4):CD001920. doi: 10.1002/14651858.CD001920.pub3. Epub 2014 Apr 22 [PubMed PMID: 24756870]
Level 1 (high-level) evidencePomeroy V, Aglioti SM, Mark VW, McFarland D, Stinear C, Wolf SL, Corbetta M, Fitzpatrick SM. Neurological principles and rehabilitation of action disorders: rehabilitation interventions. Neurorehabilitation and neural repair. 2011 Jun:25(5 Suppl):33S-43S. doi: 10.1177/1545968311410942. Epub [PubMed PMID: 21613536]
Heckmann JG, Vachalova I, Lang CJG, Pitz S. Neuro-Ophthalmology at the Bedside: A Clinical Guide. Journal of neurosciences in rural practice. 2018 Oct-Dec:9(4):561-573. doi: 10.4103/jnrp.jnrp_145_18. Epub [PubMed PMID: 30271051]
Yap Y, Morris R, Adapa R. Movement disorder surgery Part I: historical background and principle of surgery. BJA education. 2021 Apr:21(4):133-139. doi: 10.1016/j.bjae.2020.11.008. Epub 2021 Jan 21 [PubMed PMID: 33777411]
Legg LA, Lewis SR, Schofield-Robinson OJ, Drummond A, Langhorne P. Occupational therapy for adults with problems in activities of daily living after stroke. The Cochrane database of systematic reviews. 2017 Jul 19:7(7):CD003585. doi: 10.1002/14651858.CD003585.pub3. Epub 2017 Jul 19 [PubMed PMID: 28721691]
Level 1 (high-level) evidenceGittins J, Martin K, Sheldrick J, Reddy A, Thean L. Electrical stimulation as a therapeutic option to improve eyelid function in chronic facial nerve disorders. Investigative ophthalmology & visual science. 1999 Mar:40(3):547-54 [PubMed PMID: 10067956]
Klapper SR, Patrinely JR. Management of cosmetic eyelid surgery complications. Seminars in plastic surgery. 2007 Feb:21(1):80-93. doi: 10.1055/s-2007-967753. Epub [PubMed PMID: 20567662]
Ketenci A, Zure M. Pharmacological and non-pharmacological treatment approaches to chronic lumbar back pain. Turkish journal of physical medicine and rehabilitation. 2021 Mar:67(1):1-10. doi: 10.5606/tftrd.2021.8216. Epub 2021 Mar 4 [PubMed PMID: 33948537]
Jimmy B, Jose J. Patient medication adherence: measures in daily practice. Oman medical journal. 2011 May:26(3):155-9. doi: 10.5001/omj.2011.38. Epub [PubMed PMID: 22043406]
Reblin M, Uchino BN. Social and emotional support and its implication for health. Current opinion in psychiatry. 2008 Mar:21(2):201-5. doi: 10.1097/YCO.0b013e3282f3ad89. Epub [PubMed PMID: 18332671]
Level 3 (low-level) evidenceOrcutt T, Vitek J, Patriat R, Harel N, Matsumoto J. Apraxia of Eyelid Opening Improved by Pallidal Stimulation in Progressive Supranuclear Palsy. Movement disorders clinical practice. 2020 Aug:7(6):698-700. doi: 10.1002/mdc3.13001. Epub 2020 Jul 16 [PubMed PMID: 32775519]
Lee JH, Han HS, Lee JK. The Importance of Early Recognition, Timely Management, and the Role of Healthcare Providers in Multisystem Inflammatory Syndrome in Children. Journal of Korean medical science. 2021 Jan 11:36(2):e17. doi: 10.3346/jkms.2021.36.e17. Epub 2021 Jan 11 [PubMed PMID: 33429476]
Al-Asmi A, Nandhagopal R, Jacob PC, Gujjar A. Misdiagnosis of Myasthenia Gravis and Subsequent Clinical Implication: A case report and review of literature. Sultan Qaboos University medical journal. 2012 Feb:12(1):103-8 [PubMed PMID: 22375266]
Level 3 (low-level) evidencePaterick TE, Patel N, Tajik AJ, Chandrasekaran K. Improving health outcomes through patient education and partnerships with patients. Proceedings (Baylor University. Medical Center). 2017 Jan:30(1):112-113 [PubMed PMID: 28152110]
Rosen MA, DiazGranados D, Dietz AS, Benishek LE, Thompson D, Pronovost PJ, Weaver SJ. Teamwork in healthcare: Key discoveries enabling safer, high-quality care. The American psychologist. 2018 May-Jun:73(4):433-450. doi: 10.1037/amp0000298. Epub [PubMed PMID: 29792459]
Level 2 (mid-level) evidenceKadam RA. Informed consent process: A step further towards making it meaningful! Perspectives in clinical research. 2017 Jul-Sep:8(3):107-112. doi: 10.4103/picr.PICR_147_16. Epub [PubMed PMID: 28828304]
Level 3 (low-level) evidenceSheehan J, Laver K, Bhopti A, Rahja M, Usherwood T, Clemson L, Lannin NA. Methods and Effectiveness of Communication Between Hospital Allied Health and Primary Care Practitioners: A Systematic Narrative Review. Journal of multidisciplinary healthcare. 2021:14():493-511. doi: 10.2147/JMDH.S295549. Epub 2021 Feb 22 [PubMed PMID: 33654406]
Level 1 (high-level) evidenceBrault I, Kilpatrick K, D'Amour D, Contandriopoulos D, Chouinard V, Dubois CA, Perroux M, Beaulieu MD. Role clarification processes for better integration of nurse practitioners into primary healthcare teams: a multiple-case study. Nursing research and practice. 2014:2014():170514. doi: 10.1155/2014/170514. Epub 2014 Dec 1 [PubMed PMID: 25692039]
Level 3 (low-level) evidenceShaw L, Bazzell AF, Dains JE. Botulinum Toxin for Side-Effect Management and Prevention of Surgical Complications in Patients Treated for Head and Neck Cancers and Esophageal Cancer. Journal of the advanced practitioner in oncology. 2019 Jan-Feb:10(1):40-52 [PubMed PMID: 31308987]