Introduction
Vertigo refers to the perception of spinning or rotary motion involving oneself or the surrounding environment in the absence of actual movement.[1] Because patient descriptions of vertigo vary widely, the condition often falls under the broad term “dizziness,” a vague yet common complaint responsible for over 3 million emergency department visits each year.[2] The term dizziness encompasses multiple sensations, creating diagnostic ambiguity that frequently misleads clinicians. Vertigo may originate from vestibular (peripheral) or nonvestibular (central) sources.
Benign paroxysmal positional vertigo (BPPV) represents the most frequent cause of peripheral vertigo, accounting for more than half of all cases. Approximately 20% of patients presenting with vertigo symptoms demonstrate BPPV, although this percentage may underestimate the true prevalence due to frequent misdiagnosis or underdiagnosis.[3][4] Differentiation of BPPV from other vertigo causes remains critical, as the diagnostic spectrum ranges from benign to potentially life-threatening conditions. Because dizziness is a nonspecific symptom, clinicians must clarify patients' descriptions during history-taking. Encouraging patients to describe sensations without using the word dizziness often yields more accurate information.[5][6][7]
Dr. Robert Bárány first described BPPV in 1921.[8] At that time, postural changes that induced characteristic vertigo and nystagmus were linked to the otolithic organs. In 1952, Dr. Margaret Dix and Dr. Charles Hallpike expanded upon this understanding by observing classic nystagmus during provocative testing and identifying the pathology within the inner ear.[9]
BPPV represents a complex vestibular disorder subclassified into posterior or lateral semicircular canal variants. Posterior semicircular canal BPPV is diagnosed when vertigo with nystagmus occurs during the Dix-Hallpike maneuver.[10] The underlying mechanisms involve canalithiasis and cupulolithiasis. In cupulolithiasis, otoconia adhere to the cupula, creating a persistent gravity-sensitive response.[11] The type of nystagmus often determines the BPPV subtype.
Diagnosis typically relies on patient reports of brief, episodic vertigo lasting 1 minute or less. Many patients adapt or restrict head movements to prevent symptom provocation.[12] Audiometric testing remains unnecessary for routine diagnosis, although many otolaryngologists obtain it to exclude other otologic causes, eg, Ménière’s disease, characterized by episodic vertigo, fluctuating hearing loss, and tinnitus.[13] Radiographic and vestibular studies provide little diagnostic value unless a central etiology is suspected. Central vertigo often presents with additional neurologic features, including gait disturbance, speech abnormalities, or autonomic dysfunction that may mimic BPPV.[14]
Treatment primarily involves canalith repositioning maneuvers, vestibular rehabilitation, and assessment of therapeutic response. Vestibulosuppressant medications play a minimal role in BPPV management.[15] Common agents include:
- Antihistamines (eg, meclizine and diphenhydramine)
- Benzodiazepines (eg, diazepam and clonazepam)
- Anticholinergics (eg, scopolamine)
Surgical intervention remains reserved for refractory cases unresponsive to repositioning maneuvers and may involve labyrinthectomy, posterior canal occlusion, singular neurectomy, vestibular nerve section, or transtympanic aminoglycoside application.[16][17]
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Approximately 50% to 70% of BPPV cases are idiopathic, with no known cause.[18] Many conflicting studies regarding BPPV risk factors have been published, but generally accepted risks include:
- Increasing age [19]
- Genetic predisposition [20]
- Female sex [21]
- Head trauma
- The most common types of trauma were motor vehicle crashes, common falls, temporal bone or stapes surgery, and head trauma.[22][23]
- Acoustic or electrical stimulation, pressure, intense physical activity, and mechanical trauma can lead to otoconial dislodgement.[24][25]
- Traumatic BPPV may involve multiple canals and requires repeated maneuvers.[25][26]
- Osteoporosis or low bone density [27]
- Vitamin D deficiency in postmenopausal women [28]
- Prolonged bed rest [29]
- Head lying down sleeping position [30]
- Chronic headache and neck pain [31]
- Diabetes mellitus mediated by hypertension [32]
- Hyperlipidemia, thyroid disorders, hearing loss, and vitamin D deficiency [33]
- Viral labyrinthitis, or vestibular neuritis, accounts for up to 15% of BPPV cases (associated with herpesviruses, Epstein–Barr virus, adenovirus, and cytomegalovirus).[34] [35]
- Ménière disease occurs in 0.5% to 44% of cases.[36][37][38]
- Endolymphatic hydrops [39]
- Migraine [40]
- Pigmentation disorders, such as vitiligo [41]
- Multiple sclerosis and Parkinson’s disease [42][43]
The most common secondary cause of BPPV is head injury, accounting for 7% to 17% of cases.[44][34] Prior research has implied that trauma to the head may cause mechanical displacement of otoconia into the endolymph, affecting the posterior canal, similar to idiopathic cases.[45][46] However, animal studies have instead demonstrated an acute disruption of the inner ear infrastructure.[47] Recent human studies show strong evidence that previous head trauma is an independent risk factor for BPPV.[46]
Epidemiology
Prevalence estimates for BPPV vary greatly, ranging from 10.7 to 140 per 100,000 in population-based studies. Reported lifetime prevalence is 2.4%, with a 1-year prevalence of 1.6% and an annual incidence of 0.6%. Women are more commonly affected, with female-to-male ratios reported between 2.2:1 and 1.5:1. BPPV is the most common vestibular disorder across all ages. However, BPPV most often begins in the fifth to seventh decades of life. Due to its high prevalence, BPPV carries significant health care and societal burdens.[48]
Pathophysiology
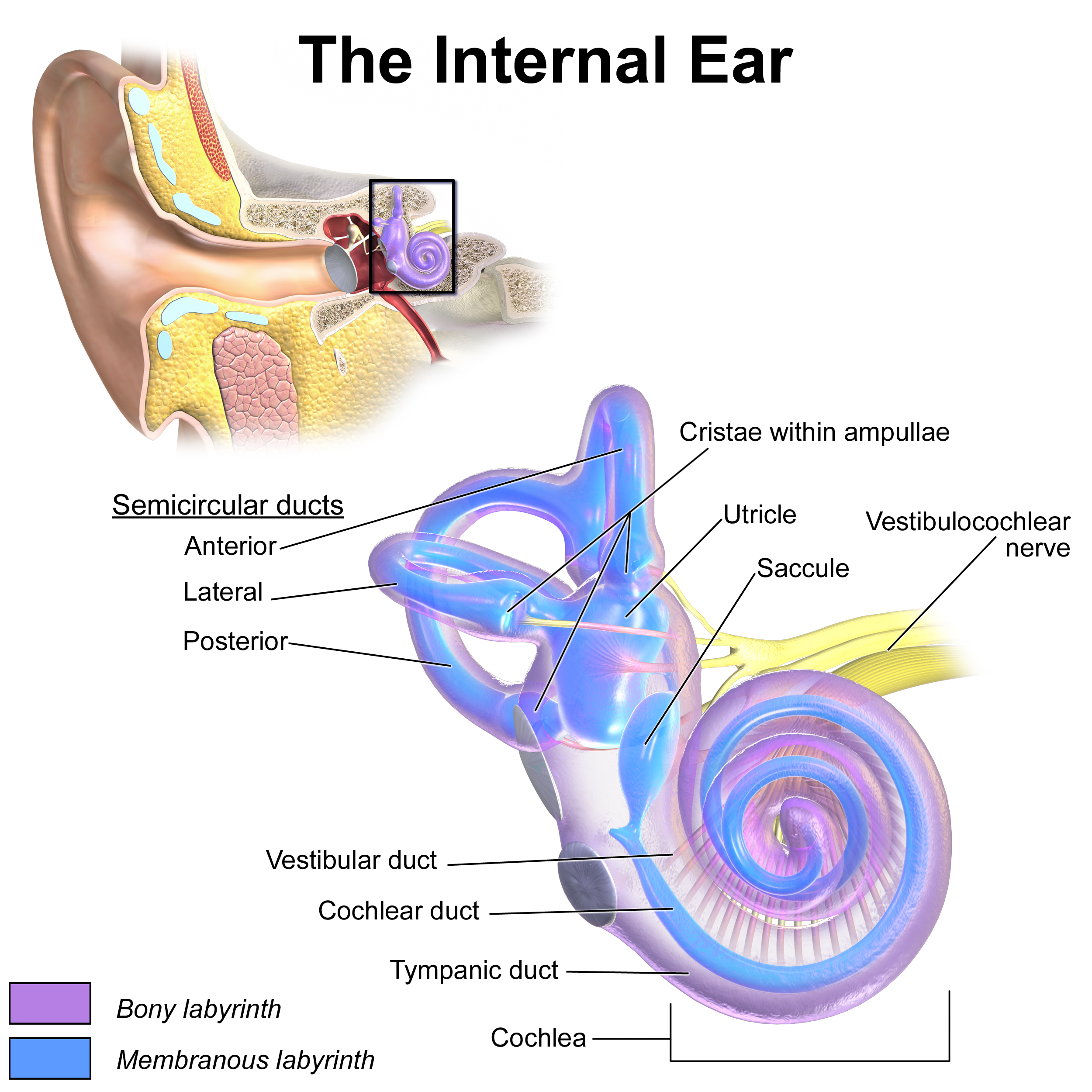
Each inner ear contains 3 semicircular canals arranged in 3 perpendicular planes.[49] Each canal forms a fluid-filled tube lined with endolymph and terminates in an enlarged sac known as the ampulla (see Image. Inner Ear Anatomy). Within each ampulla lies the crista ampullaris, an inverted saddle-shaped sensory structure composed of hair cells. These hair cells extend into the gelatinous cupula, which shifts in response to angular accelerations of the head. The resulting displacement stimulates the hair cells, producing nerve signals that the brain interprets as indicators of angular head velocity and acceleration.[50]
Pathophysiological mechanisms responsible for BPPV include free-floating debris or otoliths within the semicircular canal (canalolithiasis) or debris or otoliths attached to the cupula (cupulolithiasis).[51] These displaced otoliths commonly originate from detachment of the utricular macula’s neuroepithelium, often secondary to degenerative changes. Any disorder of the inner ear that promotes otoconial detachment can provoke BPPV.[36] An idiopathic form, diagnosed when the underlying cause remains unidentified, is believed to develop spontaneously. BPPV frequently coexists with other pathological conditions, further complicating diagnosis and management.
History and Physical
Clinical History
A comprehensive clinical assessment is essential for assessing vertigo, as distinguishing between vestibular and central processes is crucial. Employ open-ended questions to acquire the most detailed description of symptoms. Inquire about the timing of symptoms, contextual factors, and both exacerbating and alleviating influences. Additionally, question recent viral infections due to their association with labyrinthitis, as well as any history of trauma, recent neurosurgical procedures, and medications that may possess ototoxic potential, as these may indicate alternative etiologies for diagnosis.[52] Relapses are common; consequently, a history of recurrent vertiginous episodes indicates BPPV. Due to age-related degeneration of the otolithic membrane, BPPV is common in older adults. Nonetheless, carefully considering the central causes of vertigo, which are associated with advancing age and cerebrovascular disease, is imperative. Patients with mood disorders demonstrate a propensity to develop BPPV.[53]
Patients with BPPV typically describe brief, recurrent episodes of vertigo precipitated by changes in head position relative to gravity. Common triggers include rolling over in bed, looking upward, or bending forward. These episodes are generally short, lasting less than 1 minute, and often are characterized by a spinning sensation. Some individuals report nonspecific dizziness, lightheadedness, nausea, or imbalance instead. Between episodes, many are asymptomatic; however, up to 50% may experience a sensation of unsteadiness or imbalance. The symptoms are paroxysmal and stereotyped, with patients sometimes adjusting their movements to avoid provoking attacks. A history of episodic, positionally triggered vertigo strongly indicates BPPV, although diagnosis cannot be confirmed solely based on history without supportive positional testing.[48]
Physical Examination
The physical examination in patients with BPPV is typically unremarkable. The Dix-Hallpike maneuver remains the only standardized clinical test of significant importance for diagnosing posterior canal BPPV.[54] In affected patients, this test elicits torsional, upbeating nystagmus associated with vertigo.[48] Characteristic features include a latency of approximately 5 to 20 seconds before onset, a crescendo-decrescendo pattern of intensity, and resolution within 60 seconds. Nystagmus frequently reverses direction when the patient is repositioned to an upright posture. Fatigability with repetitive testing may be observed, but is not required for diagnosis.
In the Dix-Hallpike maneuver, the patient begins in an upright position with the head rotated 45 degrees toward the ear being examined. Subsequently, with the patient's eyes open, they are smoothly moved to a supine position, with the neck extended by 20 to 30 degrees at the lower end and the head maintained in the 45-degree rotation. After 30 to 60 seconds, the patient returns to a seated position. If neither nystagmus nor vertigo occurs, the procedure is then repeated on the opposite side. Essential considerations during the performance of the Dix-Hallpike maneuver include:
- Before performing the Dix-Hallpike test, the patient should be advised that they may experience temporary vertigo and possibly nausea.
- The briskness with which the Dix-Hallpike test is performed should be individualized for each patient.[55]
- For posterior canal BPPV, the nystagmus is described as torsional (rotatory) and upbeating (toward the forehead).[48]
- With repeated testing, the nystagmus should fatigue as the canaliths disperse, reducing their mass effect.[56]
- In patients with cervical spine pathology, minimal head extension should be performed, and the examination tables may need to be tilted to allow for safe testing.
Patients with benign paroxysmal positional vertigo of the lateral canal (LC-BPPV) are diagnosed as having geotropic or apogeotropic bidirectional nystagmus during the head-roll maneuver (HRM) in the supine position. Patients’ subjective feelings of vertigo were also a helpful indicator. The head-roll maneuver identifies the affected ear in 75% of cases with apogeotropic nystagmus and 95.6% with geotropic nystagmus.[57]
The following are key considerations concerning the history and physical examination of patients with BPPV:
- Common risk factors include older age, being female, vestibular neuritis, labyrinthitis, head trauma, migraines, inner ear surgery, and Meniere's disease.[58][59][53]
- A central disorder is probably the underlying cause if vertigo occurs independently of movement. Labyrinthitis or vestibular neuritis may mimic BPPV; however, unlike BPPV, any movement in any plane can trigger an episode that typically lasts several days.
- BPPV typically endures for 30 to 60 seconds. In comparison, vertigo associated with other conditions generally persists longer. Meniere’s disease may last for several hours; vestibular neuritis or viral labyrinthitis can continue for several days; migraines exhibit variable durations, and other central disorders may be constant.
- An isolated attack should not be considered BPPV unless the Dix-Hallpike maneuver is positive.
Evaluation
A positive Dix-Hallpike test is considered the definitive gold standard for diagnosing posterior canal BPPV; therefore, laboratory and imaging tests are generally unnecessary to establish the diagnosis.[48] Nevertheless, BPPV exhibits a strong correlation with inner ear disorders, and further diagnostic evaluation may be warranted to identify additional pathologies.
The head-roll maneuver, also known as the supine roll test, is predominantly employed to diagnose lateral (or horizontal) canal BPPV. The clinician positions the patient in a supine posture, with the head initially maintained in a neutral position, then swiftly rotating it 90 degrees to one side. During this maneuver, the clinician observes the patient’s eyes for the presence of nystagmus. Once the nystagmus subsides, or if no nystagmus is observed, the head is returned to the neutral position. After any subsequent nystagmus has diminished, the head is rapidly rotated 90 degrees to the opposite side, and the clinician continues to monitor the eyes for nystagmus.
BPPV is primarily diagnosed through clinical assessment. Routine imaging or vestibular testing is generally not recommended for patients who satisfy the diagnostic criteria for BPPV, provided there are no additional vestibular or concerning signs and symptoms. As previously noted, obtaining a comprehensive medical history and conducting a thorough neurological examination are essential. Imaging of the head in cases of BPPV typically yields unremarkable findings. Computed tomography (CT) and magnetic resonance imaging (MRI) are valuable tools for excluding infarction, hemorrhage, masses or tumors, or other pathologies that may indicate alternative causes of vertigo accompanied by additional neurological symptoms. If tolerated, the Dix-Hallpike maneuver should be performed as a provocative test to observe for anticipated changes in symptoms and to determine the involved semicircular canal.[60][61][62]
Treatment / Management
The initial step in managing BPPV is patient education and proper understanding counseling.[48][63] In instances of lateral (also known as horizontal) canal and superior (also referred to as anterior) canal BPPV, referring the patient to a tertiary care facility is advisable. A canalith repositioning procedure, alternatively termed a particle repositioning maneuver (PRM), should be performed in cases of posterior canal BPPV unless contraindicated.[64][65][66] Repositioning maneuvers are straightforward to execute and can be mastered by clinicians across a variety of settings.[67][68] Medications typically prescribed to suppress vestibular influence are not considered an effective treatment option.[69][70][71](A1)
The Epley maneuver can be performed after the utilization of the Dix-Hallpike maneuver for the purpose of localizing the affected side. This sequence of positional modifications facilitates the dislodgement of otoconia from the otolithic membrane and their return to the utricle, thereby alleviating the disturbance and associated symptoms. As previously noted, the Dix-Hallpike and Epley maneuvers are not always well tolerated by patients with BPPV; in such cases, treatment remains focused on alleviating symptoms.
Although not standard practice for BPPV management, antihistamines may be employed in cases of severe symptoms when the patient declines the canalith repositioning procedure. These medications attenuate vertigo by suppressing labyrinthine excitability and vestibular end-organ receptors. The antihistamine most supported by the literature for vertigo is meclizine, administered at doses ranging from 25 mg to 100 mg daily. Vertigo associated with BPPV typically manifests acutely, with a brief, paroxysmal presentation, which aligns with the term's etymology; therefore, pharmacological intervention generally offers limited benefit. Consequently, routine medical management with meclizine is not recommended unless vertigo episodes are frequent and significantly impair daily activities. Nausea and vomiting are common concomitants of BPPV. They can be managed with antiemetics, eg, ondansetron, metoclopramide, or promethazine/prochlorperazine as required, but these agents have little or no impact on vertigo. Patients experiencing recurrent BPPV should be referred to an ENT specialist for comprehensive evaluation. Notably, certain lateral and horizontal canal variants of BPPV necessitate specific repositioning maneuvers distinct from the Epley procedure.[5][72](A1)
Repositioning Maneuvers
The diagnosis of BPPV is based on the character of nystagmus induced by the various positional tests.[48] The first-line treatment for posterior canal BPPV is a repositioning maneuver to clear the affected semicircular canal of debris. Repositioning maneuvers are effective for improving posterior canal BPPV.[65][66] The Dix-Hallpike test and the side-lying diagnostic Sémont maneuver are used to diagnose posterior canal BPPV, which is associated with torsional, upwardly beating nystagmus.[73] Some contraindications to their use include:(A1)
- Severe cervical disease
- Suspected vertebrobasilar disease
- Unstable cardiovascular disease
- High-grade carotid stenosis
Numerous variants of the canalith repositioning procedure have been developed, including the Epley maneuver, the Sémont (ie, the liberatory) maneuver, and the 3-position maneuver.[74] Trials have demonstrated that all these maneuvers are highly effective. The Epley and Sémont maneuvers are equally effective; however, the Epley maneuver is more commonly used in North America. Overweight and older adult patients may find the Epley maneuver easier to perform.[75][19] Postmaneuver instructions and postural restrictions are not needed.[76][77][78][79](A1)
For a patient diagnosed with right-sided BPPV, the Epley procedure is carried out as follows:
- Position 1: The patient is placed in the upright position with the head turned 45 degrees toward the affected ear (the ear that was positive on the Dix-Hallpike testing).[48]
- Position 2: The patient is rapidly laid back to the supine head-hanging 20 to 30 degree position, which is then maintained for 20 to 30 seconds.
- Position 3: The patient's head is turned 90 degrees toward the other (unaffected) side and held for about 20 seconds.
- Position 4: The patient's head is turned a further 90 degrees (usually necessitating the patient’s body moving from the supine to the lateral decubitus position) so that the patient’s head is nearly in the face-down position. This is also held for 20 to 30 seconds.
- Position 5: The patient is then brought into the upright sitting position, completing the maneuver. (A1)
Specific adverse effects associated with repositioning maneuvers that healthcare practitioners should be cognizant of include:
- Immediate falling sensation within 30 minutes after the maneuver
- Nausea
- Emesis
- Fainting
- Postural instability that can last 24 hours
- Conversion of posterior BPPV to a lateral or anterior canal BPPV during a maneuver [80] (B3)
The supine roll test is considered useful for diagnosing horizontal canal BPPV (hc-BPPV) by eliciting horizontal responses nystagmus.[81] The Bow and Lean test and Upright Roll test have also been described as diagnostic tests for hc-BPPV.[82][83] Anterior canal BPPV is diagnosed by the supine head-hanging test with the generation of characteristic downwardly beating nystagmus, which may have a torsional component.[84][85]
Surgical Treatment
The majority of patients with BPPV experience improvement following repositioning maneuvers or achieve complete resolution. Surgical intervention is contemplated solely for refractory cases after multiple sessions of the canalith repositioning procedure. Surgical procedures carry risks, including permanent hearing loss and facial nerve damage. Nonetheless, all surgical options offer a high likelihood of vertigo control in stubborn cases. Surgical options for BPPV include labyrinthectomy, posterior canal occlusion, singular neurectomy, vestibular nerve section, and transtympanic aminoglycoside application.[86] The recommended surgical procedure is posterior semicircular canal occlusion, which has demonstrated high efficacy and safety, with markedly lower risk of hearing loss.[87] Most patients benefit from postoperative vestibular rehabilitation.
Differential Diagnosis
Benign paroxysmal positional vertigo may have the following differential diagnoses:
- Ménière disease
- Frequently misdiagnosed as BPPV
- May occur concomitantly with BPPV
- Labyrinthitis or vestibular neuritis
- Labyrinthitis ossificans [88]
- Superior canal dehiscence
- Posttraumatic vertigo
- Perilymphatic fistula
- Inner ear lesions
- Inner ear concussion (head trauma) [89]
- Vestibular migraines
- Posterior circulation transient ischemic attack and stroke
- Demyelinating diseases, eg, multiple sclerosis
- Central nervous system lesions
- Vertebrobasilar insufficiency
- Central positional vertigo [90]
- Anxiety
- Cervicogenic vertigo [91]
- Alcohol intoxication
- Orthostatic hypotension [48][92][93]
- Vascular loop syndrome [94]
- Cerebellar degeneration (eg, Spinocerebellar ataxias, Friedreich's ataxia)
Prognosis
Overall, the prognosis is favorable. One-third of patients achieve remission by 3 weeks. The majority of patients attain remission at 6 months.[95] Recurrence rates vary in the literature, with one study reporting a 10-year recurrence rate of 18%.[96] Another study reported an annual recurrence rate of 15%, with a 50% recurrence observed at 40 months following treatment.[97] Fewer than 1% of BPPV cases necessitate surgical intervention; however, the number of potential surgical candidates remains considerable due to the prevalence of BPPV.[98]
Complications
Patients diagnosed with BPPV face an elevated risk of falls. In the older adult population, this heightened risk may lead to severe consequences. Nearly 86% of individuals with BPPV experience disruptions in daily activities and absenteeism at work attributable to the condition, while 6% choose to resign from their employment as a consequence.[48]
Deterrence and Patient Education
Deterrence of BPPV focuses on minimizing risk factors that contribute to otoconial dislodgement and subsequent vertiginous episodes. Age-related degeneration of the otolithic membrane, head trauma, vestibular neuritis, labyrinthitis, and certain inner ear surgeries increase susceptibility to BPPV. Additional contributors include prolonged bed rest, osteoporosis or low bone density, vitamin D deficiency, migraines, diabetes, and mechanical stress to the head or inner ear. Preventive strategies involve addressing modifiable risk factors, eg, optimizing bone health, correcting vitamin D deficiency, safely managing chronic conditions, and minimizing exposure to activities that might precipitate otoconial displacement. Clinicians should also emphasize caution following head injuries or surgeries to reduce the likelihood of secondary BPPV.
Patient education represents a critical component of effective BPPV management and long-term prevention. Although clinicians should clarify that BPPV is a benign condition that does not pose a threat to life. Educating patients about the characteristic triggers of positional vertigo, eg, rolling in bed, bending forward, or looking upward, empowers them to recognize early symptoms and adjust movements to prevent falls or injuries. Instruction regarding the nature and purpose of diagnostic maneuvers, including the Dix-Hallpike and head-roll tests, can alleviate anxiety during evaluation. Patients should understand the role of canalith repositioning procedures, eg, the Epley and Semont maneuvers, in resolving symptoms and reducing recurrence.
Additionally, patients with recurrent or refractory BPPV should be advised on the importance of follow-up care with otolaryngology or vestibular specialists to ensure comprehensive management and to monitor for underlying conditions that may contribute to ongoing vertigo. All patients should be advised to undergo follow-up 1 month after treatment.[48] Patients should also be informed that recurrences are common even after successful repositioning maneuvers and that additional treatment may be required.
Pearls and Other Issues
Factors that should be kept in mind when managing BPPV include:
- BPPV generally presents with a sudden onset, precipitated by abrupt movements that influence a particular region of the inner ear. Most patients do not experience persistent dizziness.
- The Dix-Hallpike maneuver is the standard clinical test for BPPV.
- Canalith repositioning offers the most significant benefits with minimal risk.
- Surgery should be reserved solely for selected patients who do not respond to conservative therapy.
Enhancing Healthcare Team Outcomes
BPPV is a frequent cause of dizziness in United States clinics, with 5.6 million visits annually and 17% to 42% of vertigo cases attributed to this disorder.[48] Early identification and management of patients with BPPV are essential to ensure safety when driving or operating machinery and to improve overall quality of life. Caring for patients diagnosed with BPPV requires a collaborative approach among healthcare professionals to deliver patient-centered care and achieve better outcomes. Family medicine doctors, internists, emergency room physicians, neurologists, otolaryngologists, advanced practitioners, nurses, audiologists, pharmacists, physical and occupational therapists, and other clinicians involved in these patients' care should possess the necessary clinical skills and knowledge to diagnose and treat BPPV accurately. Physicians and advanced practitioners determine the diagnosis and perform repositioning maneuvers. Nurses reinforce patient education, ensure safety during procedures, and coordinate follow-up care. Pharmacists review medications and reduce vestibular suppressants that might delay recovery. Therapists and audiologists can coordinate to offer vestibular rehabilitation for recurrent or refractory cases.
A strategic approach is also vital, utilizing evidence-based strategies to optimize treatment plans and minimize adverse effects. Shared decision-making ensures patients understand the benign nature of BPPV and the risk of recurrence, thereby reducing fall risk. Ethical considerations are essential for guiding decision-making, ensuring informed consent, and respecting patient autonomy in treatment decisions. Each healthcare professional must understand their responsibilities and contribute their unique skills and expertise to the patient's care plan, promoting an interprofessional approach. Effective interprofessional communication is key, enabling seamless information exchange and collaborative decision-making among team members. Care coordination is pivotal in ensuring that the patient's journey from diagnosis through treatment and follow-up is well-organized, reducing errors and enhancing safety and quality of life. By embracing these principles—skill, strategy, ethics, responsibilities, interprofessional communication, and care coordination—healthcare professionals can provide patient-centered care, ultimately improving outcomes and strengthening team performance in managing BPPV.
Media
(Click Image to Enlarge)
Inner ear anatomy
Bruce Blaus - open source from Wikimedia commons
References
Basura GJ, Adams ME, Monfared A, Schwartz SR, Antonelli PJ, Burkard R, Bush ML, Bykowski J, Colandrea M, Derebery J, Kelly EA, Kerber KA, Koopman CF, Kuch AA, Marcolini E, McKinnon BJ, Ruckenstein MJ, Valenzuela CV, Vosooney A, Walsh SA, Nnacheta LC, Dhepyasuwan N, Buchanan EM. Clinical Practice Guideline: Ménière's Disease. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2020 Apr:162(2_suppl):S1-S55. doi: 10.1177/0194599820909438. Epub [PubMed PMID: 32267799]
Level 1 (high-level) evidenceMuncie HL, Sirmans SM, James E. Dizziness: Approach to Evaluation and Management. American family physician. 2017 Feb 1:95(3):154-162 [PubMed PMID: 28145669]
Kerber KA, Newman-Toker DE. Misdiagnosing Dizzy Patients: Common Pitfalls in Clinical Practice. Neurologic clinics. 2015 Aug:33(3):565-75, viii. doi: 10.1016/j.ncl.2015.04.009. Epub [PubMed PMID: 26231272]
Grill E, Strupp M, Müller M, Jahn K. Health services utilization of patients with vertigo in primary care: a retrospective cohort study. Journal of neurology. 2014 Aug:261(8):1492-8. doi: 10.1007/s00415-014-7367-y. Epub 2014 May 11 [PubMed PMID: 24817192]
Level 2 (mid-level) evidenceParker IG, Hartel G, Paratz J, Choy NL, Rahmann A. A Systematic Review of the Reported Proportions of Diagnoses for Dizziness and Vertigo. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2019 Jan:40(1):6-15. doi: 10.1097/MAO.0000000000002044. Epub [PubMed PMID: 30439765]
Level 1 (high-level) evidenceAlimoğlu Y, Altın F, Açıkalın RM, Yaşar H. Two-Hour Follow-Up is Equivalent to One-Day Follow-Up of Posterior Canal Benign Paroxysmal Positional Vertigo. The journal of international advanced otology. 2019 Apr:15(1):141-145. doi: 10.5152/iao.2018.5328. Epub [PubMed PMID: 30411707]
Male AJ, Ramdharry GM, Grant R, Davies RA, Beith ID. A survey of current management of Benign Paroxysmal Positional Vertigo (BPPV) by physiotherapists' interested in vestibular rehabilitation in the UK. Physiotherapy. 2019 Sep:105(3):307-314. doi: 10.1016/j.physio.2018.08.007. Epub 2018 Sep 5 [PubMed PMID: 30389100]
Level 3 (low-level) evidenceAndaz C, Whittet HB, Ludman H. An unusual cause of benign paroxysmal positional vertigo. The Journal of laryngology and otology. 1993 Dec:107(12):1153-4 [PubMed PMID: 8289008]
Level 3 (low-level) evidenceHornibrook J. Benign Paroxysmal Positional Vertigo (BPPV): History, Pathophysiology, Office Treatment and Future Directions. International journal of otolaryngology. 2011:2011():835671. doi: 10.1155/2011/835671. Epub 2011 Jul 25 [PubMed PMID: 21808648]
Level 3 (low-level) evidenceHizal E, Jafarov S, Erbek SH, Ozluoglu LN. Clinical Interpretation of Positional Nystagmus Provoked by both Dix-Hallpike and Supine Head-Roll Tests. The journal of international advanced otology. 2022 Jul:18(4):334-339. doi: 10.5152/iao.2022.21461. Epub [PubMed PMID: 35894530]
Kalmanson O, Foster CA. Cupulolithiasis: A Critical Reappraisal. OTO open. 2023 Jan-Mar:7(1):e38. doi: 10.1002/oto2.38. Epub 2023 Mar 1 [PubMed PMID: 36998555]
Ruckenstein MJ, Shepard NT. The canalith repositioning procedure with and without mastoid oscillation for the treatment of benign paroxysmal positional vertigo. ORL; journal for oto-rhino-laryngology and its related specialties. 2007:69(5):295-8 [PubMed PMID: 17622794]
. Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Menière's disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 1995 Sep:113(3):181-5 [PubMed PMID: 7675476]
Bertholon P, Bronstein AM, Davies RA, Rudge P, Thilo KV. Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. Journal of neurology, neurosurgery, and psychiatry. 2002 Mar:72(3):366-72 [PubMed PMID: 11861698]
Gurumukhani JK, Patel DM, Shah SV, Patel MV, Patel MM, Patel AV. Negative Impact of Vestibular Suppressant Drugs on Provocative Positional Tests of BPPV: A Study from the Western Part of India. Annals of Indian Academy of Neurology. 2021 May-Jun:24(3):367-371. doi: 10.4103/aian.AIAN_413_20. Epub 2021 Jan 8 [PubMed PMID: 34446999]
Alarcón AV, Hidalgo LO, Arévalo RJ, Diaz MP. Labyrinthectomy and Vestibular Neurectomy for Intractable Vertiginous Symptoms. International archives of otorhinolaryngology. 2017 Apr:21(2):184-190. doi: 10.1055/s-0037-1599242. Epub [PubMed PMID: 28382129]
Schoo DP, Tan GX, Ehrenburg MR, Pross SE, Ward BK, Carey JP. Intratympanic (IT) Therapies for Menière's Disease: Some Consensus Among the Confusion. Current otorhinolaryngology reports. 2017 Jun:5(2):132-141. doi: 10.1007/s40136-017-0153-5. Epub 2017 May 3 [PubMed PMID: 29568697]
Level 3 (low-level) evidenceKarabulut M, Kutlu S, Viechtbauer W, Melliti A, Meço C, Mohamad A, Özgirgin ON, Bhandari A, Kingma H, van de Berg R. Co-occurrence of Otologic Disorders and Benign Paroxysmal Positional Vertigo: A Systematic Review and Meta-Analysis. Clinical and experimental otorhinolaryngology. 2025 Nov:18(4):326-338. doi: 10.21053/ceo.2025-00030. Epub 2025 Jun 9 [PubMed PMID: 40485121]
Level 1 (high-level) evidenceBalatsouras DG, Koukoutsis G, Fassolis A, Moukos A, Apris A. Benign paroxysmal positional vertigo in the elderly: current insights. Clinical interventions in aging. 2018:13():2251-2266. doi: 10.2147/CIA.S144134. Epub 2018 Nov 5 [PubMed PMID: 30464434]
Gizzi M, Ayyagari S, Khattar V. The familial incidence of benign paroxysmal positional vertigo. Acta oto-laryngologica. 1998 Nov:118(6):774-7 [PubMed PMID: 9870618]
Kim JS, Zee DS. Clinical practice. Benign paroxysmal positional vertigo. The New England journal of medicine. 2014 Mar 20:370(12):1138-47. doi: 10.1056/NEJMcp1309481. Epub [PubMed PMID: 24645946]
Park SK, Kim SY, Han KH, Hong SK, Kim JS, Koo JW. Benign paroxysmal positional vertigo after surgical drilling of the temporal bone. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2013 Oct:34(8):1448-55. doi: 10.1097/MAO.0b013e318299b376. Epub [PubMed PMID: 24026025]
Di Girolamo S, Fetoni AR, Di Nardo W, Paludetti G. An unusual complication of cochlear implant: benign paroxysmal positional vertigo. The Journal of laryngology and otology. 1999 Oct:113(10):922-3 [PubMed PMID: 10664711]
Dan-Goor E, Eden JC, Wilson SJ, Dangoor J, Wilson BR. Benign paroxysmal positional vertigo after decompression sickness: a first case report and review of the literature. American journal of otolaryngology. 2010 Nov-Dec:31(6):476-8. doi: 10.1016/j.amjoto.2009.07.001. Epub 2009 Aug 26 [PubMed PMID: 20015792]
Level 3 (low-level) evidenceChen G, Li Y, Si J, Zhao X, Zhang T, Dai X, Yu G. Treatment and recurrence of traumatic versus idiopathic benign paroxysmal positional vertigo: a meta-analysis. Acta oto-laryngologica. 2019 Sep:139(9):727-733. doi: 10.1080/00016489.2019.1632484. Epub 2019 Jul 3 [PubMed PMID: 31268396]
Level 1 (high-level) evidenceAhn SK, Jeon SY, Kim JP, Park JJ, Hur DG, Kim DW, Woo SH, Kwon OJ, Kim JY. Clinical characteristics and treatment of benign paroxysmal positional vertigo after traumatic brain injury. The Journal of trauma. 2011 Feb:70(2):442-6. doi: 10.1097/TA.0b013e3181d0c3d9. Epub [PubMed PMID: 20489667]
Jeong SH, Choi SH, Kim JY, Koo JW, Kim HJ, Kim JS. Osteopenia and osteoporosis in idiopathic benign positional vertigo. Neurology. 2009 Mar 24:72(12):1069-76. doi: 10.1212/01.wnl.0000345016.33983.e0. Epub [PubMed PMID: 19307540]
Han W, Fan Z, Zhou M, Guo X, Yan W, Lu X, Li L, Gu C, Chen C, Wu Y. Low 25-hydroxyvitamin D levels in postmenopausal female patients with benign paroxysmal positional vertigo. Acta oto-laryngologica. 2018 May:138(5):443-446. doi: 10.1080/00016489.2017.1416168. Epub 2017 Dec 22 [PubMed PMID: 29272984]
Gyo K. Benign paroxysmal positional vertigo as a complication of postoperative bedrest. The Laryngoscope. 1988 Mar:98(3):332-3 [PubMed PMID: 3343883]
Cakir BO, Ercan I, Cakir ZA, Civelek S, Turgut S. Relationship between the affected ear in benign paroxysmal positional vertigo and habitual head-lying side during bedrest. The Journal of laryngology and otology. 2006 Jul:120(7):534-6 [PubMed PMID: 16834802]
Molvær OI. Chronic Benign Paroxysmal Positional Vertigo (BPPV): A possible cause of chronic, otherwise unexplained neck-pain, headache, and widespread pain and fatigue, which may respond positively to repeated particle repositioning manoeuvres (PRM). Scandinavian journal of pain. 2013 Oct 1:4(4):231-232. doi: 10.1016/j.sjpain.2013.06.005. Epub 2013 Oct 1 [PubMed PMID: 29913647]
D'Silva LJ, Staecker H, Lin J, Sykes KJ, Phadnis MA, McMahon TM, Connolly D, Sabus CH, Whitney SL, Kluding PM. Retrospective data suggests that the higher prevalence of benign paroxysmal positional vertigo in individuals with type 2 diabetes is mediated by hypertension. Journal of vestibular research : equilibrium & orientation. 2016:25(5-6):233-9. doi: 10.3233/VES-150563. Epub [PubMed PMID: 26890424]
Level 2 (mid-level) evidenceSreenivas V, Sima NH, Philip S. The Role of Comorbidities in Benign Paroxysmal Positional Vertigo. Ear, nose, & throat journal. 2021 Jun:100(5):NP225-NP230. doi: 10.1177/0145561319878546. Epub 2019 Sep 29 [PubMed PMID: 31565984]
Baloh RW, Honrubia V, Jacobson K. Benign positional vertigo: clinical and oculographic features in 240 cases. Neurology. 1987 Mar:37(3):371-8 [PubMed PMID: 3822129]
Level 2 (mid-level) evidenceHanci D, Ulusoy S, Muluk NB, Cingi C. Do viral infections have a role in benign paroxysmal positional vertigo? B-ENT. 2015:11(3):211-8 [PubMed PMID: 26601554]
Karlberg M, Hall K, Quickert N, Hinson J, Halmagyi GM. What inner ear diseases cause benign paroxysmal positional vertigo? Acta oto-laryngologica. 2000 Mar:120(3):380-5 [PubMed PMID: 10894413]
Level 3 (low-level) evidenceHughes CA, Proctor L. Benign paroxysmal positional vertigo. The Laryngoscope. 1997 May:107(5):607-13 [PubMed PMID: 9149161]
Level 3 (low-level) evidenceTaura A, Funabiki K, Ohgita H, Ogino E, Torii H, Matsunaga M, Ito J. One-third of vertiginous episodes during the follow-up period are caused by benign paroxysmal positional vertigo in patients with Meniere's disease. Acta oto-laryngologica. 2014 Nov:134(11):1140-5. doi: 10.3109/00016489.2014.936624. Epub 2014 Aug 28 [PubMed PMID: 25166020]
Salt AN, Plontke SK. Endolymphatic hydrops: pathophysiology and experimental models. Otolaryngologic clinics of North America. 2010 Oct:43(5):971-83. doi: 10.1016/j.otc.2010.05.007. Epub [PubMed PMID: 20713237]
Level 3 (low-level) evidenceBruss D, Abouzari M, Sarna B, Goshtasbi K, Lee A, Birkenbeuel J, Djalilian HR. Migraine Features in Patients With Recurrent Benign Paroxysmal Positional Vertigo. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2021 Mar 1:42(3):461-465. doi: 10.1097/MAO.0000000000002976. Epub [PubMed PMID: 33306663]
Dawoud EAE, Ismail EI, Eltoukhy SA, El-Sharabasy AE. Assessment of auditory and vestibular functions in vitiligo patients. Journal of otology. 2017 Sep:12(3):143-149. doi: 10.1016/j.joto.2017.07.001. Epub 2017 Jul 18 [PubMed PMID: 29937850]
Frohman EM, Kramer PD, Dewey RB, Kramer L, Frohman TC. Benign paroxysmal positioning vertigo in multiple sclerosis: diagnosis, pathophysiology and therapeutic techniques. Multiple sclerosis (Houndmills, Basingstoke, England). 2003 Jun:9(3):250-5 [PubMed PMID: 12814171]
Aranke SV, Sethi KD. Benign paroxysmal positional vertigo in Parkinson's disease. Neurology. 2003 Oct 28:61(8):1156 [PubMed PMID: 14581695]
Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta oto-laryngologica. 1999:119(7):745-9 [PubMed PMID: 10687929]
Level 2 (mid-level) evidenceKim M, Jeon EK, Seo YJ, Kong TH. A Retrospective Comparison of Clinical Characteristics of Post-Traumatic and Idiopathic Benign Paroxysmal Positional Vertigo. Ear and hearing. 2025 Sep-Oct 01:46(5):1379-1384. doi: 10.1097/AUD.0000000000001675. Epub 2025 Apr 30 [PubMed PMID: 40302023]
Level 2 (mid-level) evidenceYoo DM, Yang BR, Han K, Choi HG, Choe G, Choi JW, Kim BJ. The Association Between Head Trauma and BPPV: A Nested Case-Control Study Using a National Health Screening Cohort. Diagnostics (Basel, Switzerland). 2025 Aug 27:15(17):. doi: 10.3390/diagnostics15172171. Epub 2025 Aug 27 [PubMed PMID: 40941658]
Level 2 (mid-level) evidenceYang CJ, Lee JW, Kim SJ, Lee CW, Park HJ. Development of a murine model of traumatic benign paroxysmal positional vertigo: a preliminary study. Acta oto-laryngologica. 2017 Jan:137(1):29-34 [PubMed PMID: 27564837]
Bhattacharyya N, Gubbels SP, Schwartz SR, Edlow JA, El-Kashlan H, Fife T, Holmberg JM, Mahoney K, Hollingsworth DB, Roberts R, Seidman MD, Steiner RW, Do BT, Voelker CC, Waguespack RW, Corrigan MD. Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2017 Mar:156(3_suppl):S1-S47. doi: 10.1177/0194599816689667. Epub [PubMed PMID: 28248609]
Level 1 (high-level) evidenceCárdenas-Serna M, Jeffery N. Human semicircular canal form: Ontogenetic changes and variation of shape and size. Journal of anatomy. 2022 Mar:240(3):541-555. doi: 10.1111/joa.13576. Epub 2021 Oct 21 [PubMed PMID: 34674260]
Highstein SM, Rabbitt RD, Holstein GR, Boyle RD. Determinants of spatial and temporal coding by semicircular canal afferents. Journal of neurophysiology. 2005 May:93(5):2359-70 [PubMed PMID: 15845995]
Yetiser S. Review of the pathology underlying benign paroxysmal positional vertigo. The Journal of international medical research. 2020 Apr:48(4):300060519892370. doi: 10.1177/0300060519892370. Epub 2019 Dec 29 [PubMed PMID: 31885315]
Andersson H, Jablonski GE, Nordahl SHG, Nordfalk K, Helseth E, Martens C, Røysland K, Goplen FK. The Risk of Benign Paroxysmal Positional Vertigo After Head Trauma. The Laryngoscope. 2022 Feb:132(2):443-448. doi: 10.1002/lary.29851. Epub 2021 Sep 6 [PubMed PMID: 34487348]
Chu CH, Liu CJ, Lin LY, Chen TJ, Wang SJ. Migraine is associated with an increased risk for benign paroxysmal positional vertigo: a nationwide population-based study. The journal of headache and pain. 2015:16():62. doi: 10.1186/s10194-015-0547-z. Epub 2015 Jul 4 [PubMed PMID: 26141381]
Halker RB, Barrs DM, Wellik KE, Wingerchuk DM, Demaerschalk BM. Establishing a diagnosis of benign paroxysmal positional vertigo through the dix-hallpike and side-lying maneuvers: a critically appraised topic. The neurologist. 2008 May:14(3):201-4. doi: 10.1097/NRL.0b013e31816f2820. Epub [PubMed PMID: 18469678]
Level 3 (low-level) evidenceCox H, Frith J. Best practice assessment and management of benign paroxysmal positional vertigo in older adults. Age and ageing. 2025 Aug 1:54(8):. doi: 10.1093/ageing/afaf225. Epub [PubMed PMID: 40819291]
You P, Instrum R, Parnes L. Benign paroxysmal positional vertigo. Laryngoscope investigative otolaryngology. 2019 Feb:4(1):116-123. doi: 10.1002/lio2.230. Epub 2018 Dec 14 [PubMed PMID: 30828628]
Yetiser S, Ince D. Diagnostic Role of Head-Bending and Lying-Down Tests in Lateral Canal Benign Paroxysmal Positional Vertigo. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2015 Aug:36(7):1231-7. doi: 10.1097/MAO.0000000000000774. Epub [PubMed PMID: 25938792]
Oghalai JS, Manolidis S, Barth JL, Stewart MG, Jenkins HA. Unrecognized benign paroxysmal positional vertigo in elderly patients. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2000 May:122(5):630-4 [PubMed PMID: 10793337]
Level 2 (mid-level) evidencevon Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H. Epidemiology of benign paroxysmal positional vertigo: a population based study. Journal of neurology, neurosurgery, and psychiatry. 2007 Jul:78(7):710-5 [PubMed PMID: 17135456]
Level 2 (mid-level) evidencePower L, Murray K, Szmulewicz D. Early experience with a multi-axial, whole body positioning system in the treatment of Benign Paroxysmal Positional Vertigo (BPPV). Journal of clinical neuroscience : official journal of the Neurosurgical Society of Australasia. 2019 Mar:61():186-188. doi: 10.1016/j.jocn.2018.10.039. Epub 2018 Oct 28 [PubMed PMID: 30377044]
Lloyd M, Mackintosh A, Grant C, McManus F, Kelly AM, Karunajeewa H, Tang CY. Evidence-based management of patients with vertigo, dizziness, and imbalance at an Australian metropolitan health service: an observational study of clinical practice. Physiotherapy theory and practice. 2020 Jul:36(7):818-825. doi: 10.1080/09593985.2018.1511020. Epub 2018 Oct 17 [PubMed PMID: 30332324]
Level 2 (mid-level) evidenceLuryi AL, LaRouere M, Babu S, Bojrab DI, Zappia J, Sargent EW, Schutt CA. Traumatic versus Idiopathic Benign Positional Vertigo: Analysis of Disease, Treatment, and Outcome Characteristics. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2019 Jan:160(1):131-136. doi: 10.1177/0194599818797892. Epub 2018 Oct 16 [PubMed PMID: 30324864]
Cohen HS, Kimball KT. Effectiveness of treatments for benign paroxysmal positional vertigo of the posterior canal. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2005 Sep:26(5):1034-40 [PubMed PMID: 16151355]
Level 1 (high-level) evidenceHilton MP, Pinder DK. The Epley (canalith repositioning) manoeuvre for benign paroxysmal positional vertigo. The Cochrane database of systematic reviews. 2014 Dec 8:2014(12):CD003162. doi: 10.1002/14651858.CD003162.pub3. Epub 2014 Dec 8 [PubMed PMID: 25485940]
Level 1 (high-level) evidenceHelminski JO, Zee DS, Janssen I, Hain TC. Effectiveness of particle repositioning maneuvers in the treatment of benign paroxysmal positional vertigo: a systematic review. Physical therapy. 2010 May:90(5):663-78. doi: 10.2522/ptj.20090071. Epub 2010 Mar 25 [PubMed PMID: 20338918]
Level 1 (high-level) evidencePrim-Espada MP, De Diego-Sastre JI, Pérez-Fernández E. [Meta-analysis on the efficacy of Epley's manoeuvre in benign paroxysmal positional vertigo]. Neurologia (Barcelona, Spain). 2010 Jun:25(5):295-9 [PubMed PMID: 20643039]
Level 1 (high-level) evidenceMunoz JE, Miklea JT, Howard M, Springate R, Kaczorowski J. Canalith repositioning maneuver for benign paroxysmal positional vertigo: randomized controlled trial in family practice. Canadian family physician Medecin de famille canadien. 2007 Jun:53(6):1049-53, 1048 [PubMed PMID: 17872784]
Level 1 (high-level) evidenceChang AK, Schoeman G, Hill M. A randomized clinical trial to assess the efficacy of the Epley maneuver in the treatment of acute benign positional vertigo. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2004 Sep:11(9):918-24 [PubMed PMID: 15347540]
Level 1 (high-level) evidenceFurman JM, Cass SP. Benign paroxysmal positional vertigo. The New England journal of medicine. 1999 Nov 18:341(21):1590-6 [PubMed PMID: 10564690]
McClure JA, Willett JM. Lorazepam and diazepam in the treatment of benign paroxysmal vertigo. The Journal of otolaryngology. 1980 Dec:9(6):472-7 [PubMed PMID: 6110782]
Fujino A, Tokumasu K, Yosio S, Naganuma H, Yoneda S, Nakamura K. Vestibular training for benign paroxysmal positional vertigo. Its efficacy in comparison with antivertigo drugs. Archives of otolaryngology--head & neck surgery. 1994 May:120(5):497-504 [PubMed PMID: 8172700]
Level 1 (high-level) evidencePérez-Vázquez P, Franco-Gutiérrez V, Soto-Varela A, Amor-Dorado JC, Martín-Sanz E, Oliva-Domínguez M, Lopez-Escamez JA. Practice Guidelines for the Diagnosis and Management of Benign Paroxysmal Positional Vertigo Otoneurology Committee of Spanish Otorhinolaryngology and Head and Neck Surgery Consensus Document. Acta otorrinolaringologica espanola. 2018 Nov-Dec:69(6):345-366. doi: 10.1016/j.otorri.2017.05.001. Epub 2017 Aug 19 [PubMed PMID: 28826856]
Level 3 (low-level) evidenceCohen HS. Side-lying as an alternative to the Dix-Hallpike test of the posterior canal. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2004 Mar:25(2):130-4 [PubMed PMID: 15021771]
Parnes LS, Price-Jones RG. Particle repositioning maneuver for benign paroxysmal positional vertigo. The Annals of otology, rhinology, and laryngology. 1993 May:102(5):325-31 [PubMed PMID: 8489160]
Level 2 (mid-level) evidenceStrupp M, Mandala M, Vinck AS, Van Breda L, Salerni L, Gerb J, Bayer O, Mavrodiev V, Goldschagg N. The Semont-Plus Maneuver or the Epley Maneuver in Posterior Canal Benign Paroxysmal Positional Vertigo: A Randomized Clinical Study. JAMA neurology. 2023 Aug 1:80(8):798-804. doi: 10.1001/jamaneurol.2023.1408. Epub [PubMed PMID: 37358870]
Level 1 (high-level) evidenceGordon CR, Gadoth N. Repeated vs single physical maneuver in benign paroxysmal positional vertigo. Acta neurologica Scandinavica. 2004 Sep:110(3):166-9 [PubMed PMID: 15285773]
Devaiah AK, Andreoli S. Postmaneuver restrictions in benign paroxysmal positional vertigo: an individual patient data meta-analysis. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2010 Feb:142(2):155-9. doi: 10.1016/j.otohns.2009.09.013. Epub 2009 Nov 25 [PubMed PMID: 20115966]
Level 1 (high-level) evidenceToupet M, Ferrary E, Bozorg Grayeli A. Effect of repositioning maneuver type and postmaneuver restrictions on vertigo and dizziness in benign positional paroxysmal vertigo. TheScientificWorldJournal. 2012:2012():162123. doi: 10.1100/2012/162123. Epub 2012 Sep 2 [PubMed PMID: 22973168]
Level 1 (high-level) evidenceMostafa BE, Youssef TA, Hamad AS. The necessity of post-maneuver postural restriction in treating benign paroxysmal positional vertigo: a meta-analytic study. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2013 Mar:270(3):849-52. doi: 10.1007/s00405-012-2046-z. Epub 2012 May 16 [PubMed PMID: 22588196]
Level 1 (high-level) evidenceHerdman SJ, Tusa RJ. Complications of the canalith repositioning procedure. Archives of otolaryngology--head & neck surgery. 1996 Mar:122(3):281-6 [PubMed PMID: 8607956]
Level 3 (low-level) evidenceGiannoni B, Pecci R, Pollastri F, Mininni S, Licci G, Santimone R, Di Giustino F, Mandalà M. Treating benign paroxysmal positional vertigo of the lateral semicircular canal with a shortened forced position. Frontiers in neurology. 2023:14():1153491. doi: 10.3389/fneur.2023.1153491. Epub 2023 Apr 6 [PubMed PMID: 37090986]
Choung YH, Shin YR, Kahng H, Park K, Choi SJ. 'Bow and lean test' to determine the affected ear of horizontal canal benign paroxysmal positional vertigo. The Laryngoscope. 2006 Oct:116(10):1776-81 [PubMed PMID: 17003735]
Malara P, Castellucci A, Martellucci S. Upright head roll test: A new contribution for the diagnosis of lateral semicircular canal benign paroxysmal positional vertigo. Audiology research. 2020 Jul 7:10(1):236. doi: 10.4081/audiores.2020.236. Epub 2020 Jul 7 [PubMed PMID: 32676175]
Califano L, Salafia F, Mazzone S, Melillo MG, Califano M. Anterior canal BPPV and apogeotropic posterior canal BPPV: two rare forms of vertical canalolithiasis. Acta otorhinolaryngologica Italica : organo ufficiale della Societa italiana di otorinolaringologia e chirurgia cervico-facciale. 2014 Jun:34(3):189-97 [PubMed PMID: 24882928]
Bhandari A, Bhandari R, Kingma H, Strupp M. Diagnostic and Therapeutic Maneuvers for Anterior Canal BPPV Canalithiasis: Three-Dimensional Simulations. Frontiers in neurology. 2021:12():740599. doi: 10.3389/fneur.2021.740599. Epub 2021 Sep 24 [PubMed PMID: 34630309]
Corvera Behar G, García de la Cruz MA. Surgical Treatment for Recurrent Benign Paroxysmal Positional Vertigo. International archives of otorhinolaryngology. 2017 Apr:21(2):191-194. doi: 10.1055/s-0037-1599784. Epub [PubMed PMID: 28382130]
Leveque M, Labrousse M, Seidermann L, Chays A. Surgical therapy in intractable benign paroxysmal positional vertigo. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2007 May:136(5):693-8 [PubMed PMID: 17478200]
Kaya S, Paparella MM, Cureoglu S. Pathologic Findings of the Cochlea in Labyrinthitis Ossificans Associated with the Round Window Membrane. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2016 Oct:155(4):635-40. doi: 10.1177/0194599816651245. Epub 2016 May 24 [PubMed PMID: 27221575]
Choi MS, Shin SO, Yeon JY, Choi YS, Kim J, Park SK. Clinical characteristics of labyrinthine concussion. Korean journal of audiology. 2013 Apr:17(1):13-7. doi: 10.7874/kja.2013.17.1.13. Epub 2013 Apr 16 [PubMed PMID: 24653897]
Renga V. Clinical Evaluation of Patients with Vestibular Dysfunction. Neurology research international. 2019:2019():3931548. doi: 10.1155/2019/3931548. Epub 2019 Feb 3 [PubMed PMID: 30863640]
Cherchi M, DiLiberto FE, Yacovino DA, Das S. The Enduring Controversy of Cervicogenic Vertigo, and Its Place among Positional Vertigo Syndromes. Audiology research. 2021 Sep 26:11(4):491-507. doi: 10.3390/audiolres11040045. Epub 2021 Sep 26 [PubMed PMID: 34698085]
Level 3 (low-level) evidenceParnes LS, Agrawal SK, Atlas J. Diagnosis and management of benign paroxysmal positional vertigo (BPPV). CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2003 Sep 30:169(7):681-93 [PubMed PMID: 14517129]
Swartz R, Longwell P. Treatment of vertigo. American family physician. 2005 Mar 15:71(6):1115-22 [PubMed PMID: 15791890]
Rajesh R, Naveen R, Anderson WT, Nolan R, Rangaswamy R. Vascular Loop Syndrome As the Etiology of Abducens Nerve Palsy: A Case Report. Cureus. 2025 Jan:17(1):e77483. doi: 10.7759/cureus.77483. Epub 2025 Jan 15 [PubMed PMID: 39958021]
Level 3 (low-level) evidenceWhite J, Savvides P, Cherian N, Oas J. Canalith repositioning for benign paroxysmal positional vertigo. Otology & neurotology : official publication of the American Otological Society, American Neurotology Society [and] European Academy of Otology and Neurotology. 2005 Jul:26(4):704-10 [PubMed PMID: 16015173]
Level 1 (high-level) evidenceProkopakis EP, Chimona T, Tsagournisakis M, Christodoulou P, Hirsch BE, Lachanas VA, Helidonis ES, Plaitakis A, Velegrakis GA. Benign paroxysmal positional vertigo: 10-year experience in treating 592 patients with canalith repositioning procedure. The Laryngoscope. 2005 Sep:115(9):1667-71 [PubMed PMID: 16148714]
Nunez RA, Cass SP, Furman JM. Short- and long-term outcomes of canalith repositioning for benign paroxysmal positional vertigo. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2000 May:122(5):647-52 [PubMed PMID: 10793340]
Shaia WT, Zappia JJ, Bojrab DI, LaRouere ML, Sargent EW, Diaz RC. Success of posterior semicircular canal occlusion and application of the dizziness handicap inventory. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2006 Mar:134(3):424-30 [PubMed PMID: 16500439]
Level 2 (mid-level) evidence