Introduction
Gastrojejunostomy (GJ) is a surgical anastomosis between the stomach and the jejunum, used to restore gastrointestinal continuity in cases of gastric outlet or duodenal obstruction, in reconstruction following gastrectomy for malignancy, and in bariatric weight-loss procedures such as Roux-en-Y gastric bypass.[1][2][3] This procedure may be performed via open, laparoscopic, or robotic approaches and may use stapled or hand-sewn techniques.[4] Recent meta-analyses and randomized controlled trials have demonstrated that robotic gastrectomy, which often includes a GJ in reconstruction, yields reduced blood loss, shorter postoperative hospital stays, fewer conversions to open surgery, and lower morbidity than conventional laparoscopic approaches in appropriately selected patients.[5]
Advances in minimally invasive and robotic platforms have expanded operative options, potentially offering improved recovery and complication profiles.[6] However, outcomes depend heavily on technical execution, patient selection, and interprofessional coordination across surgery, anesthesia, nursing, and postoperative care.[7] Understanding when and how to perform GJ, the technical choices involved, and the anticipated risks is essential for optimizing patient outcomes.
Types of GJ include several reconstructive configurations. A classic Billroth II loop GJ is technically straightforward and low-tension but prone to bile reflux gastritis. Adding a Braun jejunojejunostomy, a side-to-side anastomosis between the afferent and efferent limbs, can significantly reduce bile reflux symptoms.[8]
A Roux-en-Y GJ, by contrast, creates a defunctionalized biliopancreatic limb and a separate alimentary limb, offering superior antireflux physiology and comparable or improved safety compared with Billroth II plus Braun in modern laparoscopic series.[2] In the palliative setting, GJ remains a durable solution for malignant gastric outlet obstruction when endoscopic stenting is not feasible or is expected to fail early. Contemporary reviews suggest surgical GJ offers longer-lasting relief with fewer reinterventions, particularly in patients with good functional status and longer life expectancy.[9][10]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
Anatomy and Physiology of the Stomach
The stomach is a well-vascularized organ located in the left upper quadrant of the abdomen; it begins just below the diaphragmatic hiatus, where the esophagus enters the stomach at the gastroesophageal junction (see Image. Stomach Anatomy). This most proximal part of the stomach is known as the cardia and gives rise to the main body of the stomach as well as the fundus, which is the floppy, distensible superior-most portion of the stomach. The parts of the stomach distal to the body are the antrum, followed by the pylorus, which enters the duodenum. The greater omentum is attached to the inferior border of the stomach along the greater curvature and hangs down over the viscera below. The lesser omentum connects the stomach to the liver and is also known as the gastrohepatic ligament.
The stomach receives its blood supply from branches of the celiac trunk and collateral flow from the superior mesenteric artery via the gastroduodenal arteries (see Image. Stomach Blood Supply). The venous drainage is through the left gastric and right gastric veins, which drain into the portal vein; the left gastroepiploic vein, which drains into the splenic vein; and the right gastroepiploic vein, which drains into the superior mesenteric vein. The stomach is innervated by both the right and left vagus nerves and also has a robust lymphatic drainage system. Given the proximity of the stomach to such vital structures as the pancreas, portal triad, aorta, inferior vena cava, and spleen, to name a few, any surgeon operating on the stomach must have a full understanding of all of these anatomic structures to perform a GJ safely.[11]
The antrum of the stomach contains the G cells, which produce the hormone gastrin, which increases acid production when the pH in the stomach is too high. If there is a retained antrum after resection of the stomach, the antral G cells are separated from the parietal cells in the stomach remnant and bathed in alkali fluid from the duodenum. This high-pH environment causes them to secrete excess gastrin, which, in turn, leads the stomach remnant to produce excess acid, leading to ulceration.[12]
The stomach digests food into a nutrient-rich chyme, which then passes into the duodenum for further digestion. Disrupting the natural flow of the nutrients so that they deposit directly into the jejunum can lead to dumping syndrome.[13] Basic pancreaticobiliary secretions in the duodenum typically neutralize the acid produced by the stomach. When the stomach and jejunum are directly connected, this neutralizing environment is bypassed, predisposing the jejunum closest to the stomach to develop ulcers.[14]
Anatomy and Physiology of the Jejunum
The jejunum starts at the ligament of Treitz and extends for approximately 250 cm before transitioning into the ileum. The jejunal blood supply comes from the superior mesenteric artery, and its venous drainage is via the superior mesenteric vein. The jejunum contains few Brunner glands, which are chiefly found in the duodenum, and few Peyer patches, which are primarily found in the ileum.
The jejunum is the site where the highest amount of absorption of nutrients and vitamins takes place, except for iron, which is chiefly absorbed in the duodenum, and vitamin B12, which is absorbed in the terminal ileum. The jejunum is primarily lined with enterocytes and has long villi that increase its surface area for absorption. The motility of the jejunum is regulated by vagal stimulation, migrating myoelectric complexes, and the hormone motilin.[15]
Indications
There are 3 main indications to perform a GJ:
- A GJ can be performed to bypass an obstruction of the distal stomach or proximal small bowel, such as in the setting of cancer or scarring from an ulcer or other cause.[9]
- A GJ can be performed to bypass much of the small intestine as part of a weight-loss procedure, as is the case when a Roux-en-Y procedure is performed.[3]
- A GJ can be performed as part of a reconstruction procedure after a subtotal gastrectomy for cancer.[16]
Contraindications
The only absolute contraindication to GJ is when the procedure cannot be performed safely or when the risk of anastomotic leak is unacceptably high. Safe performance may be compromised by factors such as dense intra-abdominal adhesions, massive ascites, diffuse peritoneal carcinomatosis, extensive gastric varices, or severely distorted anatomy from prior surgery. These are considered relative contraindications, and the decision ultimately rests with the attending surgeon, who must weigh the risks and potential for complications against the benefits in each case. The most common cause of an unacceptably high risk of anastomotic leak is severe malnutrition, particularly in patients with advanced gastric malignancy or chronic ulcer disease. In patients with suspected malnutrition, nutritional status should be assessed using laboratory studies; if deficits are present, they should be corrected with enteral feeding via a distal tube or parenteral nutrition before proceeding with surgery.
Equipment
If the GJ is to be performed laparoscopically/robotically, then the following equipment is required:
- Nasogastric or orogastric tube
- Liver retractor
- A laparoscope with a light source and monitor
- Insufflation equipment
- Laparoscopic/robotic trocars
- Bowel graspers
- Harmonic scalpel or Ligasure
- Electrocautery equipment
- Laparoscopic/robotic suction irrigator
- Laparoscopic/robotic linear cutting stapler or end-to-end anastomotic stapler, depending on the planned technique
- Esophagogastroduodenal scope
- Specimen/irrigation collection system
If the GJ is to be performed open, then the following equipment is required:
- Nasogastric or orogastric tube
- Liver retractor
- Bowel clamps
- Bowel forceps
- Harmonic scalpel or Ligasure
- Electrocautery equipment
- Suction irrigator
- Linear cutting stapler, end-to-end anastomotic stapler, or appropriate suture, depending on the planned technique
- Needle driver
- Esophagogastroduodenal scope
- Specimen/irrigation collection system
Personnel
To perform a GJ, a fully staffed operating room is required, including a surgeon, assistant surgeon, scrub tech, anesthesiologist, and a circulating nurse. Additional personnel to assist in both pre- and postoperative care depend on the indication for the procedure performed and may include:
- Gastroenterologist
- Oncologist
- Dietician
- Psychiatrist
- Pharmacist
- Intensive care unit or floor nurses
- Discharge planner
Preparation
The appropriate preparation before performing a GJ varies depending on the indication for the procedure. If the GJ is performed after resection of a malignancy, preparation may include neoadjuvant chemotherapy, nutritional support, and planning for follow-up care with an oncology team. If the GJ is being performed to bypass an obstruction, such as an ulcer, ensuring that the patient is not malnourished should be the initial step in the preparation process. This could include consulting a nutritionist and potentially starting parenteral nutrition or placing a distal feeding tube. If the GJ is performed as part of a weight-loss procedure, the patient requires a comprehensive bariatric workup, including consultation with a dietitian to establish a preoperative weight-loss plan, evaluation by a psychologist or psychiatrist, and optimization of other risk factors, such as glycemic control and blood pressure management.
Technique or Treatment
GJ creation is a surgical procedure performed to establish gastric drainage and enteral access, often used in the context of gastric bypass procedures employing a Roux-en-Y anastomosis or in patients with obstructive lesions or impaired gastric emptying (see Images. Schematic of Gastric Bypass Using a Roux-en-Y Anastomosis; Roux-en-Y Gastric Bypass [RYGB]). Successful outcomes depend on careful planning of abdominal access, selection of the gastrostomy and jejunostomy sites, and tension-free bowel approximation. The following steps outline key operative techniques for both open and minimally invasive approaches, including considerations for suture- and stapler-based anastomoses.
Step 1: Obtain Access to the Abdominal Cavity
The patient should be placed in a supine position with the arms abducted at right angles and a nasogastric or orogastric tube placed to decompress the stomach. The abdominal cavity can be accessed by making an incision from the xiphoid to the umbilicus, which can be extended if greater exposure is needed. If a laparoscopic/robotic technique is being used, then the abdominal cavity may be accessed using a Hasson, Veress, or Visiport technique, after which the other needed trocars are inserted. Once access is obtained, the liver should be retracted laterally in both the open and laparoscopic techniques.
Step 2: Determine the Site of the Gastrostomy
The site of the gastrostomy should be selected 3 to 5 cm from an obstructing mass, if there is one, be it an ulcer or malignancy, or from the pylorus. The chosen area should be low on the greater curvature, as selecting a site too high can lead to intractable biliary reflux and reduced gastric emptying.
Step 3: Approximating the Jejunal Loop
Next, a loop of jejunum 10 to 15 cm from the ligament of Treitz should be selected and approximated near the gastrostomy chosen site using the bowel clamps in an antecolic fashion, although retrocolic techniques exist. If a retrocolic technique is chosen, it is vital to close the transverse mesocolon defect, also known as Petersen space. Care should be taken to ensure the loop is not under tension near the stomach and is in an isoperistaltic conformation. Once an appropriate loop is in place, a permanent suture is used to fix the jejunum to the stomach using seromuscular bites.
Step 4: Creation of the Jejunostomy and Gastrostomy
Openings in the stomach and jejunum are created approximately 1 cm from the seromuscular stitches and about 5 cm in length. The suction irrigator should be at the ready for this stage to remove any leaked gastric or intestinal contents.
Step 5: Creation of the Anastomosis
Full-thickness posterior stitches using absorbable suture with the first knot placed outside the lumen of the stomach and the jejunum. The posterior and anterior segments of the anastomosis are sutured using Connel stitches, which is a running horizontal mattress stitch. The anterior outer layer is then oversewn using Lembert stitches in the seromuscular layer.
Step 6: Hemostasis and Leak Test
The anastomosis should be carefully inspected for any bleeding, and areas of significant bleeding may be oversewn. The anastomosis should then be placed underwater using the suction irrigator, and the esophagogastroduodenal scope should be advanced into the stomach. The stomach can then be inflated, and the anastomosis can be investigated for leaks.
Stapled Technique
Stapled techniques are similar, except that the stapler is used to approximate the jejunum and stomach rather than suture, and gastrostomy and jejunostomy need only be large enough to accommodate the stapler. The gastrostomy and jejunostomy sites can then be closed with suture or an additional staple load.
Postoperative Care
Patients are typically admitted after GJ creation, especially when it is combined with a gastric resection. Patients are usually started on a low-volume diet of clear liquids and gradually advanced as tolerated. Often, it takes patients a few days to tolerate sufficient oral intake to prevent dehydration.[17] The patient should be maintained on supplemental intravenous fluids until they can tolerate sufficient oral intake.
Complications
Since GJ is a complicated surgical procedure, it comes with a significant amount of possible complications, including, but not limited to:
- Postoperative nausea and emesis
- This typically resolves spontaneously with supportive treatment, although persistent nausea and emesis may indicate a technical error and possible bowel obstruction.
- Hemorrhage
- Always a possible complication for any operation. This may range from a small bleed that resolves spontaneously to a significant bleed requiring operative revision.
- Deep vein thrombosis and possible embolus
- Always a possible complication for any operation. Patients should be kept on an anticoagulation regimen until they are ambulating.
- Anastomotic leak
- Anastomotic leak is a feared complication of GJ, which most commonly presents on the third to fifth postoperative day. The first sign is typically tachycardia, followed by abdominal pain, and any patient with these symptoms should be evaluated for a possible anastomotic leak.[18]
- Bowel obstruction
- The bowel may be obstructed early due to a technical error, such as excessive kinking, or late due to adhesions or other issues. While a trial of supportive care is not unreasonable, the prolonged obstruction will require operative revision.
- Internal herniation
- After altering the native anatomy to create a GJ, there exists the possibility of a loop of bowel herniating through a non-native space, such as the Petersen space. An internal hernia is always a surgical emergency as it creates a closed-loop obstruction and can strangulate the bowel.[19]
- Nutritional or micronutrient deficiency
- By definition, a GJ bypasses at least some of the absorptive surface of the small bowel. If a significant portion of the intestine is bypassed, the patient may be unable to absorb sufficient nutrients and become malnourished. Additionally, depending on the portion of the bowel bypassed, certain micronutrients may not be adequately absorbed, leading to a specific micronutrient deficiency.[20]
- Dumping syndrome
- In anastomosing the stomach directly to the jejunum, high osmotic chyme is dumped directly from the stomach. There are early and late types of dumping syndrome, both of which can be prevented by eating multiple small meals rather than a few larger ones.[13]
- Marginal ulcer
- Bile reflux
- In connecting the stomach to the jejunum, bile from the duodenum proceeds in an antegrade fashion and can enter the stomach from the anastomotic site. This bile can then irritate the stomach, a condition known as bile reflux.
Clinical Significance
GJ is a versatile surgical procedure used in the management of conditions ranging from gastric outlet obstruction to morbid obesity. Clinicians at all levels should be familiar with its indications, techniques, and potential complications to optimize patient outcomes. Because patients with a GJ have altered gastrointestinal anatomy, they are uniquely susceptible to complications that may present in atypical ways. A thorough understanding of these anatomic and physiologic changes is essential for any provider involved in their perioperative or long-term care.
Enhancing Healthcare Team Outcomes
Effective care surrounding gastrojejunostomy requires coordinated perioperative planning, technical proficiency, and clear interprofessional communication to optimize patient outcomes and safety. Physicians and advanced practitioners must accurately identify indications, assess operative risk, and select the most appropriate surgical or endoscopic approach based on underlying pathology, nutritional status, and goals of care. Surgeons, anesthesiologists, and gastroenterologists rely on shared decision-making and preoperative planning to minimize complications such as anastomotic leak, bleeding, or delayed gastric emptying. Nurses play a critical role in preoperative education, postoperative pain control, and monitoring for return of bowel function, signs of leak or obstruction, and early mobilization, while using standardized handoffs and protocols to ensure continuity of care across settings.
Pharmacists and dietitians enhance patient-centered care by managing perioperative medications, acid suppression, analgesia, and prophylaxis while addressing nutritional optimization, micronutrient supplementation, and diet advancement following surgery. Case managers, social workers, and rehabilitation specialists facilitate discharge planning, outpatient follow-up, and coordination with oncology or palliative care teams when a gastrojejunostomy is performed for malignant disease. Regular multidisciplinary rounds and structured communication pathways improve team performance by aligning care goals, anticipating complications such as marginal ulcers or dumping syndrome, and ensuring timely intervention. This integrated, team-based approach promotes patient safety, supports informed patient participation, and leads to more reliable clinical outcomes after gastrojejunostomy.
Nursing, Allied Health, and Interprofessional Team Interventions
As emphasized earlier, the most critical element in the care of a patient with a GJ is clear, continuous communication among all members of the multidisciplinary team. When complications arise, timely recognition and prompt progression to operative management are often lifesaving. In particular, interventions commonly used for small bowel obstruction—such as nasogastric decompression—are generally ineffective in the setting of an internal hernia and should not delay surgical exploration. The guiding principle for this patient population is early recognition and decisive operative intervention; therefore, clinical focus should remain on rapid diagnosis and expeditious return to the operating room whenever significant complications are suspected.
Nursing, Allied Health, and Interprofessional Team Monitoring
Healthcare professionals at all levels must recognize that patients with a GJ have anatomy that differs significantly from that of the average patient and, therefore, require heightened vigilance. Subtle symptoms—such as difficulty passing stool or flatus, nausea, or vomiting—may signal an internal hernia and a closed-loop obstruction, which constitute surgical emergencies requiring prompt intervention. Complicating matters, these conditions may not be readily apparent on plain abdominal radiographs or even CT imaging, potentially delaying diagnosis. For this reason, even seemingly minor changes in clinical status—such as new tachycardia or persistent, moderate abdominal pain—should be promptly communicated to the entire care team to ensure timely recognition and management of potentially life-threatening complications.
Media
(Click Image to Enlarge)
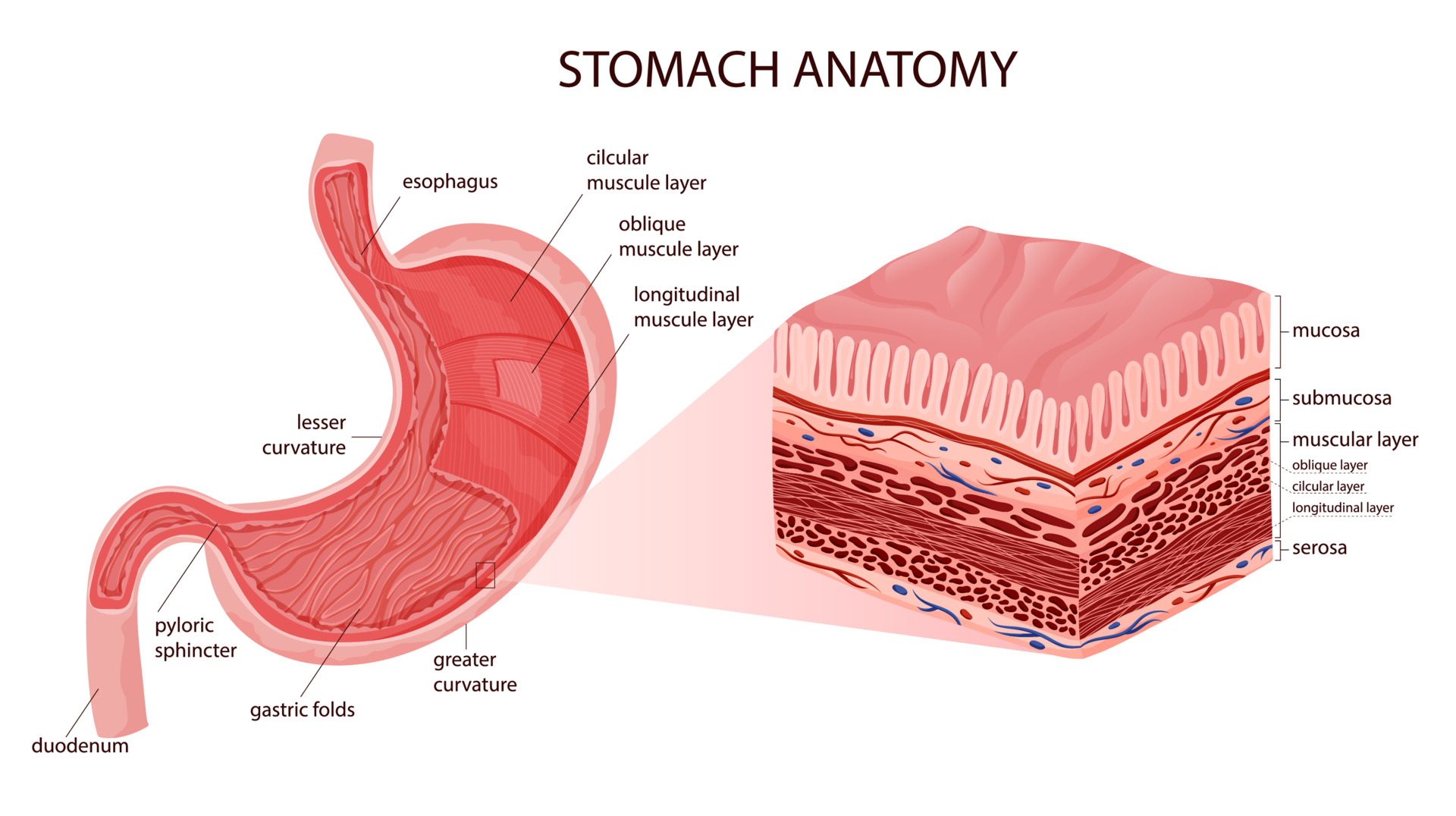
Stomach Anatomy. The greater omentum is attached to the inferior border of the stomach along the greater curvature and hangs down over the viscera below. The lesser omentum connects the stomach to the liver and is also known as the gastrohepatic ligament.
(Click Image to Enlarge)
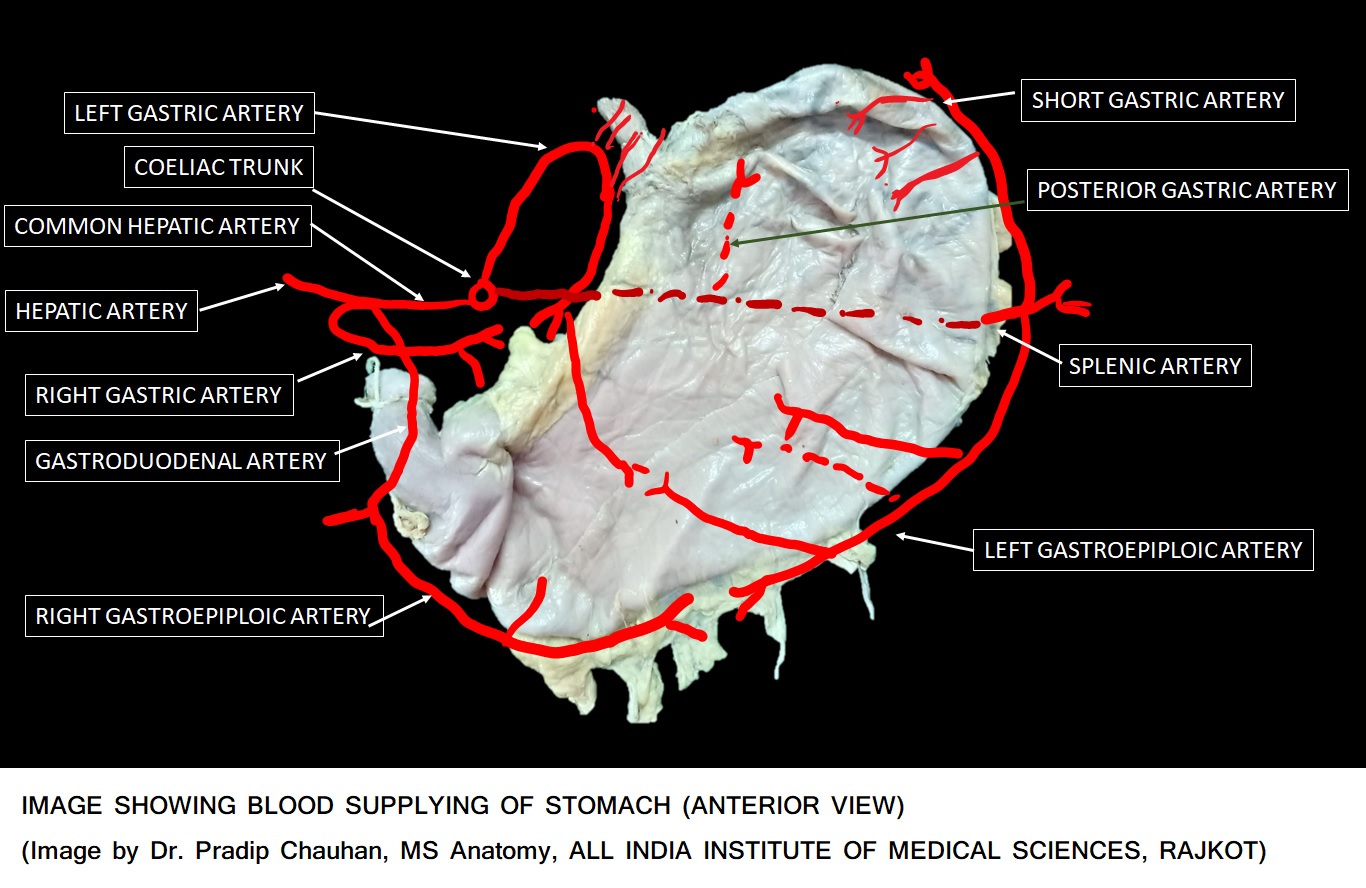
Stomach Blood Supply. The stomach receives its blood supply from branches of the celiac trunk and collateral flow from the superior mesenteric artery via the gastroduodenal arteries.
Contributed by P Chauhan, MD, MS
(Click Image to Enlarge)

Schematic of Gastric Bypass Using a Roux-en-Y Anastomosis. The transverse colon is not shown so that the Roux-en-Y can be clearly seen. The variant seen in this image is retrocolic, retrogastric, because the distal small bowel that joins the proximal segment of the stomach is behind the transverse colon and stomach.
Ethicon Endosurgery, Inc., Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
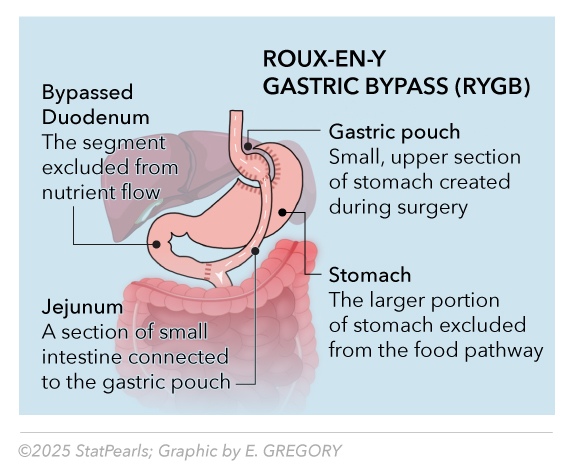
Roux-en-Y Gastric Bypass (RYGB). RYGB is a bariatric surgical procedure that creates a small gastric pouch and connects it to a segment of the jejunum, thereby bypassing most of the stomach and proximal small intestine to restrict food intake and reduce nutrient absorption.
Illustrated by E Gregory
References
Tamura T, Mamoru T, Terai T, Ogura T, Tani M, Shimokawa T, Kitahata Y, Matsumoto I, Mitoro A, Asakuma M, Inatomi O, Omoto S, Sho M, Ueno S, Maehira H, Kitano M. Gastrojejunostomy versus endoscopic duodenal stent placement for gastric outlet obstruction in patients with unresectable pancreatic cancer: a propensity score-matched analysis. Surgical endoscopy. 2023 Mar:37(3):1890-1900. doi: 10.1007/s00464-022-09685-x. Epub 2022 Oct 18 [PubMed PMID: 36258002]
Chen YX, Huang QZ, Wang PC, Zhu YJ, Chen LQ, Wu CY, Wang JT, Chen JX, Ye K. Short- and long-term outcomes of Roux-en-Y and Billroth II with Braun reconstruction in total laparoscopic distal gastrectomy: a retrospective analysis. World journal of surgical oncology. 2023 Nov 22:21(1):361. doi: 10.1186/s12957-023-03249-6. Epub 2023 Nov 22 [PubMed PMID: 37990273]
Level 2 (mid-level) evidenceAl-Fagih OS, Zuberi S, Niaz O, Jambulingam P, Whitelaw D, Rashid F, Adil MT, Jain V, Al-Taan O, Munasinghe A, Askari A, Iqbal FM. Impact of Gastrojejunostomy Anastomosis Diameter on Weight Loss Following Laparoscopic Gastric Bypass: A Systematic Review. Obesity surgery. 2024 Jun:34(6):2227-2236. doi: 10.1007/s11695-024-07237-x. Epub 2024 Apr 23 [PubMed PMID: 38652437]
Level 1 (high-level) evidenceLeang YJ, Mayavel N, Yang WTW, Kong JCH, Hensman C, Burton PR, Brown WA. Robotic versus laparoscopic gastric bypass in bariatric surgery: a systematic review and meta-analysis on perioperative outcomes. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2024 Jan:20(1):62-71. doi: 10.1016/j.soard.2023.08.007. Epub 2023 Aug 16 [PubMed PMID: 37730445]
Level 1 (high-level) evidenceCoco D, Leanza S. Global trends and outcomes in robotic vs. laparoscopic Roux-en-Y gastric bypass: a 25-year meta-analysis of 38,647 patients across 27 countries. Journal of robotic surgery. 2025 Sep 5:19(1):561. doi: 10.1007/s11701-025-02544-6. Epub 2025 Sep 5 [PubMed PMID: 40911141]
Level 1 (high-level) evidenceKonishi S, Manaka D, Morioka M, Ikeda A, Kudo R, Saito Y, Ota T, Kanaya Y, Okamura Y, Takahashi R, Seo S. Laparoscopic-assisted robotic distal gastrectomy for gastric cancer by Billroth II reconstruction. Langenbeck's archives of surgery. 2023 May 5:408(1):179. doi: 10.1007/s00423-023-02895-4. Epub 2023 May 5 [PubMed PMID: 37145178]
Hider AM, Johanson H, Bonham AJ, Ghaferi AA, Finks J, Ehlers AP, Carlin AM, Varban OA. Evaluating outcomes among surgeons who changed their technique for gastric bypass: a state-wide analysis from 2011 to 2021. Surgical endoscopy. 2023 Nov:37(11):8464-8472. doi: 10.1007/s00464-023-10434-x. Epub 2023 Sep 22 [PubMed PMID: 37740112]
Christodoulidis G, Kouliou MN, Koumarelas KE, Argyriou K, Karali GA, Tepetes K. Billroth II anastomosis combined with brown anastomosis reduce reflux gastritis in gastric cancer patients. World journal of methodology. 2024 Mar 20:14(1):89709. doi: 10.5662/wjm.v14.i1.89709. Epub 2024 Mar 20 [PubMed PMID: 38577202]
Martins RK, Brunaldi VO, Fernandes AL, Otoch JP, Artifon ELA. Palliative therapy for malignant gastric outlet obstruction: how does the endoscopic ultrasound-guided gastroenterostomy compare with surgery and endoscopic stenting? A systematic review and meta-analysis. Therapeutic advances in gastrointestinal endoscopy. 2023 Jan-Dec:16():26317745221149626. doi: 10.1177/26317745221149626. Epub 2023 Jan 21 [PubMed PMID: 36698443]
Level 1 (high-level) evidenceFugazza A, Andreozzi M, Asadzadeh Aghdaei H, Insausti A, Spadaccini M, Colombo M, Carrara S, Terrin M, De Marco A, Franchellucci G, Khalaf K, Ketabi Moghadam P, Ferrari C, Anderloni A, Capretti G, Nappo G, Zerbi A, Repici A. Management of Malignant Gastric Outlet Obstruction: A Comprehensive Review on the Old, the Classic and the Innovative Approaches. Medicina (Kaunas, Lithuania). 2024 Apr 16:60(4):. doi: 10.3390/medicina60040638. Epub 2024 Apr 16 [PubMed PMID: 38674284]
Chaudhry SR, Liman MNP, Omole AE, Peterson DC. Anatomy, Abdomen and Pelvis: Stomach. StatPearls. 2025 Jan:(): [PubMed PMID: 29493959]
Chatzipanagiotou O, Schizas D, Vailas M, Tsoli M, Sakarellos P, Sotiropoulou M, Papalambros A, Felekouras E. All you need to know about gastrinoma today | Gastrinoma and Zollinger-Ellison syndrome: A thorough update. Journal of neuroendocrinology. 2023 Apr:35(4):e13267. doi: 10.1111/jne.13267. Epub 2023 Apr 11 [PubMed PMID: 37042078]
Tack J, Raymenants K, Van de Bruaene C, Scarpellini E. Dumping syndrome: Update on pathophysiology, diagnosis, and management. Neurogastroenterology and motility. 2025 Feb:37(2):e14962. doi: 10.1111/nmo.14962. Epub 2024 Nov 11 [PubMed PMID: 39529492]
Salame M, Jawhar N, Belluzzi A, Al-Kordi M, Storm AC, Abu Dayyeh BK, Ghanem OM. Marginal Ulcers after Roux-en-Y Gastric Bypass: Etiology, Diagnosis, and Management. Journal of clinical medicine. 2023 Jun 28:12(13):. doi: 10.3390/jcm12134336. Epub 2023 Jun 28 [PubMed PMID: 37445371]
Fish EM, Shumway KR, Burns B. Physiology, Small Bowel. StatPearls. 2025 Jan:(): [PubMed PMID: 30335296]
Cai Z, Mu M, Ma Q, Liu C, Jiang Z, Liu B, Ji G, Zhang B. Uncut Roux-en-Y reconstruction after distal gastrectomy for gastric cancer. The Cochrane database of systematic reviews. 2024 Feb 29:2(2):CD015014. doi: 10.1002/14651858.CD015014.pub2. Epub 2024 Feb 29 [PubMed PMID: 38421211]
Level 1 (high-level) evidenceXu D, Li J, Liu J, Wang P, Dou J. An updated systematic review and meta-analysis of the efficacy and safety of early oral feeding vs. traditional oral feeding after gastric cancer surgery. Frontiers in oncology. 2024:14():1390065. doi: 10.3389/fonc.2024.1390065. Epub 2024 Sep 4 [PubMed PMID: 39296982]
Level 1 (high-level) evidenceShuchleib A, Swartz D, Talavea Piña J, Garcia Vences E, Mercado M. Predicting Postoperative Leaks: A Preoperative Risk Index for Bariatric Surgery. Obesity surgery. 2025 Aug:35(8):3190-3196. doi: 10.1007/s11695-025-08030-0. Epub 2025 Jul 11 [PubMed PMID: 40640597]
Murakami K, Hoshino N, Hida K, Obama K, Sakai Y, Watanabe N. Closure of mesenteric defects for prevention of internal hernia after Roux-en-Y gastric bypass in bariatric surgery. The Cochrane database of systematic reviews. 2025 Apr 8:4(4):CD014612. doi: 10.1002/14651858.CD014612.pub2. Epub 2025 Apr 8 [PubMed PMID: 40197535]
Level 1 (high-level) evidenceChen L, Chen Y, Yu X, Liang S, Guan Y, Yang J, Guan B. Long-term prevalence of vitamin deficiencies after bariatric surgery: a meta-analysis. Langenbeck's archives of surgery. 2024 Jul 20:409(1):226. doi: 10.1007/s00423-024-03422-9. Epub 2024 Jul 20 [PubMed PMID: 39030449]
Level 1 (high-level) evidenceFeimster JW, Okorji L, Paul BA, Thompson KJ, Barbat S, Kuwada TS, Gersin KS, Bauman R, Mckillop IH, Nimeri A. 10-Year outcomes of marginal ulcer formation and impact of gastrojejunostomy technique in Roux-en-Y gastric bypass. Surgery for obesity and related diseases : official journal of the American Society for Bariatric Surgery. 2025 Apr:21(4):412-416. doi: 10.1016/j.soard.2024.10.039. Epub 2024 Dec 9 [PubMed PMID: 39741102]
Cun SE, Zheng JT, Wang YM. [Research Progress of Long Non-Coding RNA in Multiple Myeloma--Review]. Zhongguo shi yan xue ye xue za zhi. 2024 Feb:32(1):313-317. doi: 10.19746/j.cnki.issn.1009-2137.2024.01.051. Epub [PubMed PMID: 38387941]