Introduction
Lipemia retinalis is a retinal manifestation of chylomicronemia, a metabolic disorder that develops in the setting of severe hypertriglyceridemia. The hallmark ophthalmoscopic feature is creamy-white discoloration of the retinal vessels, which begins in the peripheral vessels in mild cases and involves central retinal vessels in established cases. In severe cases, the fundus appears salmon-colored. Though lipemia retinalis does not affect visual acuity, the associated severe but easily treatable metabolic disorders merit discussion.[1][2][3][4] This review discusses the etiology, epidemiology, pathophysiology, histopathology, evaluation, management, and prognosis of this condition.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Lipemia retinalis was first described in detail by Heyl in 1880.[5] Vinger and Sachs described different grades of lipemia retinalis in 1970.[6] Lipemia retinalis is a clinical manifestation of marked hypertriglyceridemia, most commonly due to chylomicronemia, in which triglyceride-rich lipoproteins accumulate in the circulation, altering the optical properties of retinal vessels. Accordingly, understanding the etiology of lipemia retinalis requires an appreciation of lipoprotein metabolism, the mechanisms underlying hypertriglyceridemia, and the conditions, both primary and secondary, that lead to chylomicronemia.
The 5 classes of lipid transport molecules, or lipoproteins, are distinguished by their size and composition, as described below.
- Chylomicrons: 100–1000 nm
- Very-low-density lipoproteins: 30–80 nm
- Intermediate-density lipoproteins: 25–35 nm
- Low-density lipoproteins: 18–25 nm
- High-density lipoproteins: 5–12 nm [7]
Among these, chylomicrons are the largest lipoprotein particles and play a central role in the pathogenesis of lipemia retinalis. If a sample of hyperlipidemic serum is allowed to stand, chylomicrons form a hazy surface layer, whereas smaller lipoprotein molecules remain transparent and do not scatter light. Under normal conditions, most dietary triglycerides are transported from the intestine to the systemic circulation via chylomicrons, which are then rapidly cleared from the plasma.
However, in chylomicronemia, the blood becomes turbid and appears milky. Circulating blood with high levels of chylomicrons produces the characteristic appearance of lipemia retinalis due to the light-scattering effect within retinal vessels.[8] This appearance is distinct from that seen in fat embolism (eg, after a long-bone fracture), in which large, colorless globules cause vascular occlusion, leading to different retinal manifestations, such as Purtscher-like retinopathy.[5][9] Clinically, the earliest changes in lipemia retinalis occur in the peripheral retinal vessels and gradually progress to involve the entire fundus.[6]
The high triglyceride content of chylomicrons likely underlies the strong association between elevated triglyceride levels and the development of lipemia retinalis. Chylomicronemia typically develops when plasma triglyceride levels exceed 1000 mg/dL.[10] In this setting, patients may develop chylomicronemia syndrome, defined by the presence of chylomicronemia in combination with at least 1 of the following characteristic clinical features:
- Eruptive xanthoma (see Image. Eruptive Xanthomas)
- Lipemia retinalis (see Image. Lipemia Retinalis Fundus Appearance)
- Abdominal pain ± pancreatitis [10]
However, some authors propose a higher triglyceride threshold of 2000 mg/dL to define chylomicronemia and chylomicronemia syndrome.[11] The features of chylomicronemia syndrome according to these authors (Brunzell and Bierman), and the percentages of affected patients in the study, are outlined below.
- Lipemia retinalis (23%)
- Flushing with alcohol (25%)
- Documented pancreatitis (28%)
- Eruptive xanthoma (40%)
- Objective dyspnea (46%)
- Abdominal pain ± pancreatitis (63%)
- Recent memory loss (85%) [11]
The development of lipemia retinalis is therefore closely linked to conditions that cause severe hypertriglyceridemia and chylomicronemia. Hypertriglyceridemia (HTG) may be primary (familial) or secondary to other conditions. Both HTG and chylomicronemia are associated with significant systemic complications, including acute pancreatitis.[12][13][14] Multiple genes involved in triglyceride metabolism have been implicated in primary HTG.[1] Familial HTG occurs due to:
- The presence of endogenous circulating lipoprotein lipase (LPL) inhibitor
- Deficiency of LPL
- Deficiency of the apoprotein of LPL (ie, APOC-II)
- LPL deficiency is an autosomal recessive trait caused by a number of LPL gene mutations, including Asp9Asn, Gly188Glu, Pro207Leu, Asp250Asn, Asn291Ser, Ser447X, Pro214Ser, and others.[15]
Secondary causes of HTG include:
- Uncontrolled type 1 or type 2 diabetes mellitus
- Endocrine disorders (obesity, metabolic syndrome, hypothyroidism, hypercortisolism)
- Medications (corticosteroids, estrogen, antipsychotics [clozapine and olanzapine], antidepressants, rosiglitazone, thiazides, beta-blockers, bile acid sequestrants, sirolimus, antiretroviral therapy, 13-cis-retinoic acid, tamoxifen)
- Pregnancy
- Renal disease (nephrotic syndrome, renal failure, renal dialysis)
- Liver disease (acute hepatitis)
- Dietary intake (high in saturated fats and carbohydrates, excessive alcohol intake)
- Systemic diseases (HIV infection, acute spinal cord injury, anorexia nervosa, organ transplant, sarcoidosis, systemic lupus erythematosus, myeloma).[16]
Epidemiology
Although the epidemiology of lipemia retinalis is unknown, the epidemiology of conditions and risk factors associated with it has been characterized. A deficiency of LPL results in familial HTG and elevated serum chylomicron levels. The incidence of LPL deficiency is less than 1 in 1 million.[17]
Lipemia retinalis may also be one of the manifestations of familial combined hyperlipidemia, which has a prevalence of 1% to 2% in the general population.[18] The National Health and Nutrition Examination Survey reports from 2001 and 2006 mention that approximately 1.7% of the total United States population (3.4 million) were estimated to have severe HTG (500 to 2,000 mg/dL). According to the survey data, individuals with severe HTG tend to be men (75.3%), aged 40 to 59 years (58.5%), who identify as non-Hispanic White (70.1%). Diabetes and hypertension were associated with 14% and 31.3% of cases of HTG, respectively.[19]
Pathophysiology
Hyperlipidemia alone, without accompanying hypertriglyceridemia, does not cause lipemia retinalis.[20] The ocular findings in lipemia retinalis result from light scatter induced by the triglyceride-laden chylomicrons in the plasma.[21] Chylomicronemia occurs when plasma triglycerides exceed more than 1000 mg/dL. Lipemia retinalis is associated with plasma triglycerides greater than 2000 mg/dL.[8][11]
At triglyceride levels of 2500 mg/dL to 3499 mg/dL, the peripheral retinal vessels appear creamy and thin. At 3500 mg/dL to 5000 mg/dL, the posterior pole vessels have a creamy color. At levels above 5000 mg/dL, the fundus appears salmon-colored. Differentiation of retinal arteries and veins by color alone may be difficult (both appear creamy); in such cases, the caliber of the vessel may aid in identification.[1]
Histopathology
The creamy appearance of the retinal vessels in lipemia retinalis is due to the presence of triglyceride-laden chylomicrons in the plasma. Optical coherence tomography through the retinal vessels shows enlarged caliber and backshadowing due to hyperreflective material within the vessel lumen.[22] Extravasated lipid material may appear as hyperreflective dots within the retinal layers.[22]
History and Physical
In the classic presentation of lipemia retinalis, the patient is visually asymptomatic. Lipemia retinalis is most often detected during a routine ophthalmic workup or during a referral case workup for lipid abnormalities. Neonates and infants have been diagnosed with lipemia retinalis during screening and treatment for retinopathy of prematurity.[23][24][25][26][27][28]
A few case reports have described abdominal pain and gastrointestinal disorders as the presenting symptoms of hyperlipidemia in infants who were then found to also have lipemia retinalis.[29] Patients may have a family history of hyperlipidemia due to various enzymatic and genetic disorders as described in the Etiology section. Clinicians must rule out secondary causes of HTG by careful history and physical examination.
The physical examination should evaluate the cardiovascular, integumentary, abdominal, and ocular systems. Examination of the cardiovascular system includes auscultation of heart sounds, assessment of carotid or renal bruits, and palpation of peripheral pulses. The characteristic skin finding in HTG is xanthomas, small yellowish papules with an erythematous base, which appear predominantly on the buttocks and elbows due to the deposition of large amounts of chylomicron triglycerides in cutaneous histiocytes.[30]
Abdominal examination is required to assess for hepatosplenomegaly and to rule out pancreatic disease.[29] A dilated fundoscopic exam is required for the diagnosis and staging of lipemia retinalis. Ophthalmic evaluation should also include the examination of the periorbital area, anterior segment, and posterior segment.
Examination of the periorbital area may reveal:
- Xanthelasma
- Tuberous palpebral xanthomas
Anterior segment findings, though rare, include:
- Conjunctival xanthomas
- Corneal arcus senilis and arcus juvenilis
- Lipid keratopathy
- Anterior chamber lipemia
- Iris xanthomas [6][31]
Additional rare posterior segment findings of hyperlipoproteinemia include:
- Retinal xanthomas that appear like Roth spots
- Xanthomatous infiltration of the choroid
- Xanthomatous lipid deposition within the uveal tract, including the choroid, has been described in association with systemic hyperlipoproteinemia and represents the accumulation of lipid-laden macrophages (foam cells).
- Adult-onset Coats disease [6][32][33]
Evaluation
Laboratory evaluation of the fasting lipid profile is required to diagnose HTG in association with lipemia retinalis. The blood specimen for laboratory evaluation is typically lipemic, with a creamy white lipid layer visible in a standing tube.[34] The turbidity of the serum is due to the presence of chylomicrons in the plasma.[31]
Genetic evaluation can be performed to identify several mutations in the LPL gene.[15] Fundoscopy is required to diagnose lipemia retinalis, and fundus photography is helpful for documentation and follow-up. Retinal OCT in lipemia retinalis can indirectly indicate the presence of chylomicrons in the retinal vessels.[22] Prior treatment, a decrease in the amplitude of photopic and scotopic a and b waves has been documented in the electroretinogram of lipemia retinalis, while posttreatment reversal of these waves has been noted.[35] Fluorescein and indocyanine angiography testing are typically unremarkable in lipemia retinalis
Treatment / Management
Lipemia retinalis is occasionally transient and may resolve within hours.[8] However, a prompt reversal of hyperlipidemia is the key to a favorable prognosis. Various measures can achieve this outcome.(B3)
Dietary Restriction and Primary Prevention
For infants with severe lipemia retinalis associated with HTG, strict adherence to a low-fat diet without supplementation with breast milk may be effective.[36] Correction of the lipid levels may reverse the abnormal findings within 1 week. Reducing and controlling serum triglyceride levels will prevent the development of lipemia retinalis.(B3)
Medical Treatment
Lipemia retinalis itself does not require medical treatment. However, lipemia retinalis is an important ocular sign of a life-threatening but easily treatable metabolic disorder. The goal of management is to reduce serum triglyceride levels to below 500 mg/dL, which can be achieved through a range of medical treatments to lower triglycerides and cholesterol. Several lipid-lowering drugs are used to treat HTG.
First-line triglyceride-lowering medications include fibric acid derivatives (fibrates) and n-3 polyunsaturated fatty acids (PUFAs).[37] Fibrates reduce triglycerides by 50%. The use of fibrates is contraindicated in those with hepatic or renal dysfunction.[38] (A1)
PUFAs (ie, fish oil) also reduce triglycerides by 50%, with little effect on other lipid fractions.[39] Gastrointestinal symptoms are the major side effects of this drug class. Nicotinic acid can decrease triglyceride levels by 15% to 35%.[40] Strict glycemic control is necessary for patients with lipemia retinalis and diabetes.[16](B2)
Procedural and Adjunctive Therapies
Surgery is not specifically indicated for the treatment of lipemia retinalis. However, exchange transfusion has been used in cases of severe hypertriglyceridemia to reduce triglycerides in the acute setting.[41] Ileal bypass surgery has demonstrated improvement in all lipid parameters but should be reserved for refractory cases.[42]
Differential Diagnosis
The differential for lipemia retinalis includes:
- Leukemia (specifically chronic myeloid leukemia)
- Advanced diabetic eye disease with sclerotic vessels
- Intravascular calcification of retinal vessels secondary to renal failure and hyperparathyroidism
- Retinal branch, retinal artery, or vein occlusion
- Hypertensive retinopathy
- Diffuse choroidal hemangioma [5][43]
In leukemia, the veins are reddish-pale, while the arteries are pale yellow. In lipemia, arteries and veins appear the same color and can be differentiated only by their caliber, with veins being larger.[5] In intravascular calcification secondary to renal failure or hyperparathyroidism, disordered renal parameters and elevated parathyroid hormone levels are helpful in identifying the proper diagnosis. Diffuse hemangiomas may resemble the characteristic salmon fundus in lipemia retinalis. On cursory exam, retinal vasculitis may also be on the differential, but vasculitis is usually segmental and associated with perivascular infiltrates and evidence of intraocular inflammation.
Staging
The staging of lipemia retinalis, given by Vinger and Sachs, is as follows:
- Grade I (early lipemia retinalis): White and creamy appearance of peripheral retinal vessels
- Grade II (moderate lipemia retinalis): Creamy colored vessels extending towards the optic disc
- Grade III (marked lipemia retinalis): Salmon colored retina, all vessels displaying a milky color [6]
Prognosis
The retinal changes seen in lipemia retinalis improve once serum triglyceride levels are normalized. Visual acuity is typically unaffected. Reduced photopic and scotopic responses in the electroretinogram may improve after HTG correction.[35] Systemically, patients with lipemia retinalis are at increased risk for coronary artery disease, myocardial infarction, and stroke. From an ophthalmic perspective, patients with lipemia retinalis are at increased risk for retinal artery and vein occlusions and retinal ischemia, and clinicians should monitor accordingly.
Complications
Systemic complications of lipidemia retinalis due to hyperlipidemia include cardiovascular disease, systemic hypertension, acute myocardial infarction, and stroke. Chylomicronemia is associated with acute pancreatitis, abdominal pain, hepatosplenomegaly, dyspnea, and recent memory loss. Direct ophthalmic complications from lipemia retinalis are less frequently reported but include retinovascular occlusions, retinal ischemia leading to neovascularization and vitreous hemorrhage, and one case of macular edema in the setting of diabetes with microaneurysms on fluorescein angiogram.[21][44] Lipemia retinalis frequently coexists with hypertensive retinopathy and diabetic retinopathy; these conditions may worsen visual outcomes.
Deterrence and Patient Education
Lipemia retinalis serves as an important clinical indicator of severe hypertriglyceridemia and warrants a combined strategy of deterrence and patient education to prevent recurrence and systemic complications.[45] Effective management focuses on strict control of serum triglyceride levels through lifestyle modification, including adherence to a low-fat diet, avoidance of alcohol, regular physical activity, and weight optimization, along with appropriate pharmacotherapy such as fibrates, omega-3 fatty acids, and statins. Identification and treatment of underlying conditions, including diabetes mellitus and genetic disorders such as familial hypertriglyceridemia, are essential.
Patient education plays a pivotal role, emphasizing that lipemia retinalis is not merely an ocular finding but a marker of potentially life-threatening metabolic derangement, particularly the risk of acute pancreatitis. Patients should be counseled regarding the reversible nature of retinal changes with proper lipid control, the importance of medication adherence, and the need for regular follow-up with both primary care clinicians and ophthalmologists. Early recognition of warning symptoms, such as sudden visual changes or systemic manifestations, should be emphasized to facilitate timely intervention and reduce morbidity.
Enhancing Healthcare Team Outcomes
The diagnosis and management of lipemia retinalis are important not only for ophthalmologic care but also because the condition may signal serious underlying genetic and metabolic disorders. The prompt diagnosis and management of the associated hyperlipidemia results in the reversal of most of the lipemia retinalis symptoms and can prevent life-threatening complications like acute pancreatitis. In cases of primary HTG, the detection of a mutation of the LPL gene can guide genetic counseling for parents of an affected child.
Secondary causes, including diabetes, hypothyroidism, obesity, and chronic alcohol use disorder, must be diagnosed and promptly treated.[46][47][48][49][50] Effective management of lipemia retinalis requires clear communication and referrals among primary care clinicians, pediatricians, geneticists, endocrinologists, and ophthalmologists. The team should also include optometrists, laboratory technicians, and ophthalmology nurses. The laboratory technicians identify any abnormal discoloration in the unprocessed blood sample, and the nurses participate in patient education and follow-up, informing the ophthalmologist of any new concerns.
Media
(Click Image to Enlarge)
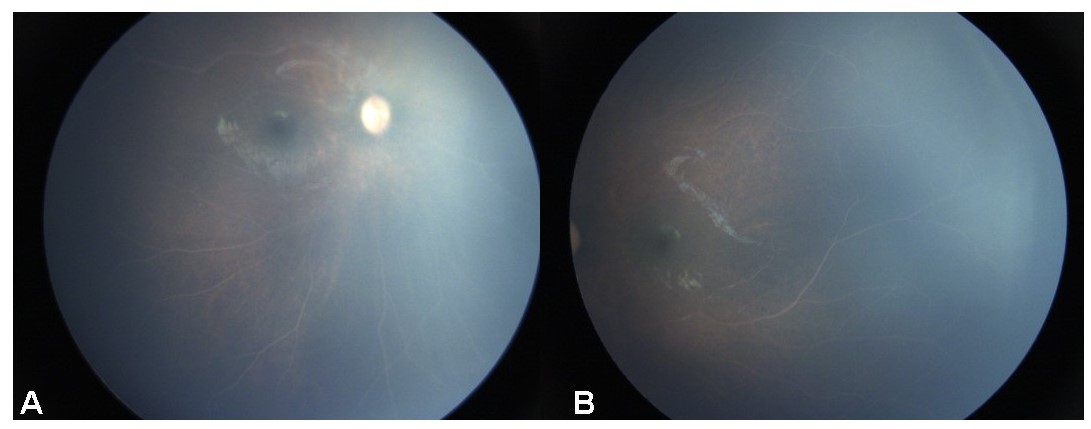
Lipemia Retinalis Fundus Appearance. Bilateral fundus photographs demonstrating diffuse creamy white retinal vessels in a 15-month-old male child, consistent with lipemia retinalis in the setting of severe hypertriglyceridemia.
Contributed by C Mishra, DNB, FICO, MRCS Ed, Aravind Eye Hospital
(Click Image to Enlarge)

Eruptive Xanthomas. Multiple erythematous papules on the lower extremity are consistent with eruptive xanthomas associated with severe hypertriglyceridemia.
References
Zahavi A, Snir M, Kella YR. Lipemia retinalis: case report and review of the literature. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2013 Feb:17(1):110-1. doi: 10.1016/j.jaapos.2012.10.010. Epub 2013 Jan 18 [PubMed PMID: 23337350]
Level 3 (low-level) evidenceJie Z, Qingmin M. Familial Chylomicronemia Syndrome-Lipemia Retinalis. Ophthalmology. Retina. 2026 Jan 23:():. pii: S2468-6530(25)00603-7. doi: 10.1016/j.oret.2025.12.022. Epub 2026 Jan 23 [PubMed PMID: 41579139]
Level 2 (mid-level) evidenceHegele RA. Approach to the Adult Patient with Chylomicronemia. The Journal of clinical endocrinology and metabolism. 2026 Feb 20:111(3):845-859. doi: 10.1210/clinem/dgaf701. Epub [PubMed PMID: 41472374]
Swaminathan VB, D'Souza HS, Starr MR. Lipemia Retinalis. Canadian journal of ophthalmology. Journal canadien d'ophtalmologie. 2025 Aug:60(4):e622-e624. doi: 10.1016/j.jcjo.2025.03.010. Epub 2025 Apr 12 [PubMed PMID: 40187367]
Heyl AG. Intra-Ocular Lipæmia. Transactions of the American Ophthalmological Society. 1880:3():54-66 [PubMed PMID: 25258848]
Vinger PF, Sachs BA. Ocular manifestations of hyperlipoproteinemia. American journal of ophthalmology. 1970 Oct:70(4):563-73 [PubMed PMID: 5505473]
Feingold KR, Adler RA, Ahmed SF, Anawalt B, Blackman MR, Chrousos G, Corpas E, de Herder WW, Dhatariya K, Dungan K, Hamilton E, Hofland J, Jan de Beur S, Kalra S, Kaltsas G, Kapoor N, Kim M, Koch C, Kopp P, Korbonits M, Kovacs CS, Kuohung W, Laferrère B, Levy M, McGee EA, McLachlan R, Muzumdar R, Purnell J, Rey R, Sahay R, Shah AS, Sperling MA, Stratakis CA, Trence DL, Wilson DP, Feingold KR. Introduction to Lipids and Lipoproteins. Endotext. 2000:(): [PubMed PMID: 26247089]
Rayner S, Lee N, Leslie D, Thompson G. Lipaemia retinalis: a question of chylomicrons? Eye (London, England). 1996:10 ( Pt 5)():603-8 [PubMed PMID: 8977790]
Level 3 (low-level) evidenceTripathy K, Patel BC. Purtscher Retinopathy. StatPearls. 2026 Jan:(): [PubMed PMID: 31194324]
Uysal E, Acar YA, Gökmen E, Kutur A, Doğan H. Hypertriglyceridemia induced pancreatitis (chylomicronemia syndrome) treated with supportive care. Case reports in critical care. 2014:2014():767831. doi: 10.1155/2014/767831. Epub 2014 Nov 23 [PubMed PMID: 25506434]
Level 3 (low-level) evidenceBrunzell JD, Bierman EL. Chylomicronemia syndrome. Interaction of genetic and acquired hypertriglyceridemia. The Medical clinics of North America. 1982 Mar:66(2):455-68 [PubMed PMID: 7040847]
Hodges BI, Yu MJ, Dirani K, Yoganathan P. Lipemia retinalis in setting of asparaginase and glucocorticoid therapy preceding acute pancreatitis. Retinal cases & brief reports. 2026 Jan 21:():. doi: 10.1097/ICB.0000000000001875. Epub 2026 Jan 21 [PubMed PMID: 41564281]
Level 3 (low-level) evidenceHeath O, Allender B, Smith J, Savva E, Spencer L, Bannister EG, Brown NJ, Evans MS, Kiss S, Rozen TH, Yaplito-Lee J. Diagnosis and stabilisation of familial chylomicronemia syndrome in two infants presenting with hypertriglyceridemia-induced acute pancreatitis. JIMD reports. 2024 Jul:65(4):239-248. doi: 10.1002/jmd2.12434. Epub 2024 Jun 2 [PubMed PMID: 38974610]
Rabbani B, Moghadam MA, Esmaeili S, Rabbani A, Akbari B, Mahdieh N. Pancreatitis as a Main Consequence of APOC2-Related Hypertriglyceridemia: The Role of Nonsense and Frameshift Variants. International journal of genomics. 2024:2024():6653857. doi: 10.1155/2024/6653857. Epub 2024 May 30 [PubMed PMID: 38938447]
Gehrisch S. Common mutations of the lipoprotein lipase gene and their clinical significance. Current atherosclerosis reports. 1999 Jul:1(1):70-8 [PubMed PMID: 11122694]
Leaf DA. Chylomicronemia and the chylomicronemia syndrome: a practical approach to management. The American journal of medicine. 2008 Jan:121(1):10-2. doi: 10.1016/j.amjmed.2007.10.004. Epub [PubMed PMID: 18187065]
Cypel M, Manzano R, Dos Reis FA, Ishida N, Ayhara T. Lipemia retinalis in a 35-day-old infant with hyperlipoproteinemia: case report. Arquivos brasileiros de oftalmologia. 2008 Mar-Apr:71(2):254-6 [PubMed PMID: 18516428]
Level 3 (low-level) evidenceSriram CS, Gulati S, Chopra V, Vashist S, Menon PS. Familial combined hyperlipidemia in a North Indian kindred. Indian journal of pediatrics. 2005 Nov:72(11):987-9 [PubMed PMID: 16391457]
Level 3 (low-level) evidenceChristian JB, Bourgeois N, Snipes R, Lowe KA. Prevalence of severe (500 to 2,000 mg/dl) hypertriglyceridemia in United States adults. The American journal of cardiology. 2011 Mar 15:107(6):891-7. doi: 10.1016/j.amjcard.2010.11.008. Epub 2011 Jan 19 [PubMed PMID: 21247544]
Horton M, Thompson K. Lipemia retinalis preceding acute pancreatitis. Optometry (St. Louis, Mo.). 2011 Aug:82(8):475-80. doi: 10.1016/j.optm.2011.01.011. Epub 2011 May 12 [PubMed PMID: 21570360]
Level 3 (low-level) evidenceNagra PK, Ho AC, Dugan JD Jr. Lipemia retinalis associated with branch retinal vein occlusion. American journal of ophthalmology. 2003 Apr:135(4):539-42 [PubMed PMID: 12654375]
Level 3 (low-level) evidenceÖzturk BT, Bozkurt B, Meşen A, Gonul S, İpekci SH. Spectral-Domain Optical Coherence Tomography Findings in Lipemia Retinalis. Ophthalmic surgery, lasers & imaging retina. 2016 Jun 1:47(6):589-92. doi: 10.3928/23258160-20160601-13. Epub [PubMed PMID: 27327291]
Jain A, Mochi TB, Braganza SD, Agrawal S, Shetty BK, Pachiyappan B. Lipemia retinalis in an infant treated for retinopathy of prematurity. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2017 Jun:21(3):254-257. doi: 10.1016/j.jaapos.2017.05.021. Epub 2017 May 27 [PubMed PMID: 28558973]
Shinkre ND, Usgaonkar UPS. Lipemia retinalis in a 27 day old neonate: A case report. Indian journal of ophthalmology. 2019 Jun:67(6):954-957. doi: 10.4103/ijo.IJO_1310_18. Epub [PubMed PMID: 31124530]
Level 3 (low-level) evidenceOzturk T, Durmaz Engin C, Karatas Yigitaslan E, Yaman A, Berk T. Accidentally diagnosed ocular abnormalities identified during close screening for retinopathy of prematurity. European journal of ophthalmology. 2022 Nov:32(6):3267-3273. doi: 10.1177/11206721221086252. Epub 2022 Mar 9 [PubMed PMID: 35261269]
Maitra P, Shah PK, Campbell PJ, Rishi P. The scope of artificial intelligence in retinopathy of prematurity (ROP) management. Indian journal of ophthalmology. 2024 Jul 1:72(7):931-934. doi: 10.4103/IJO.IJO_2544_23. Epub 2024 Mar 8 [PubMed PMID: 38454859]
Nikkhah H, Karrabi N, Yazdani E, Nezameslami R. Serendipitous Discovery of Lipemia Retinalis in a Premature Infant: A Case Report. Case reports in ophthalmology. 2025 Jan-Dec:16(1):1-6. doi: 10.1159/000542961. Epub 2024 Dec 3 [PubMed PMID: 39981534]
Level 3 (low-level) evidenceArya S, Saxena S. Identification of a novel pathogenic variant in the LPL gene in lipaemia retinalis in an infant. BMJ case reports. 2025 Mar 25:18(3):. pii: e259965. doi: 10.1136/bcr-2024-259965. Epub 2025 Mar 25 [PubMed PMID: 40132937]
Level 3 (low-level) evidenceSamanta R, Katoch D. Lipemia retinalis in an infant. Indian journal of ophthalmology. 2019 Jun:67(6):953. doi: 10.4103/ijo.IJO_225_19. Epub [PubMed PMID: 31124529]
Parker F, Bagdade JD, Odland GF, Bierman EL. Evidence for the chylomicron origin of lipids accumulating in diabetic eruptive xanthomas: a correlative lipid biochemical, histochemical, and electron microscopic study. The Journal of clinical investigation. 1970 Dec:49(12):2172-87 [PubMed PMID: 5480845]
Gopal L, Sunder KS, Rao SK, Soni M, Sharma S, Ramakrishnan S. Hyperlipidemia in a poorly controlled diabetic presenting with lipemic aqueous and lipemia retinalis. Retina (Philadelphia, Pa.). 2004 Apr:24(2):312-5 [PubMed PMID: 15097900]
Level 3 (low-level) evidenceWilson WS, Lee JH. Letter: Retinal xanthoma. Lancet (London, England). 1974 Jan 5:1(7845):34 [PubMed PMID: 4129022]
Level 3 (low-level) evidenceGurnani B, Tivakaran VS. Roth Spots. StatPearls. 2026 Jan:(): [PubMed PMID: 29494053]
Jain S, Goyal A, Kumar V. Lipaemia retinalis in familial chylomicronaemia syndrome. Lancet (London, England). 2018 Aug 25:392(10148):e7. doi: 10.1016/S0140-6736(18)31796-3. Epub [PubMed PMID: 30152345]
Fu V, Scanga HL, Medsinge A, Nischal KK. Improved visual function with dietary intervention in a child with lipemia retinalis. Journal of AAPOS : the official publication of the American Association for Pediatric Ophthalmology and Strabismus. 2014 Oct:18(5):488-90. doi: 10.1016/j.jaapos.2014.05.004. Epub 2014 Oct 21 [PubMed PMID: 25439305]
Level 3 (low-level) evidenceYin HY, Warman R, Suh EH, Cheng AM. Exceptionally elevated triglyceride in severe lipemia retinalis. International medical case reports journal. 2016:9():333-336 [PubMed PMID: 27799830]
Level 3 (low-level) evidenceStalenhoef AF, de Graaf J, Wittekoek ME, Bredie SJ, Demacker PN, Kastelein JJ. The effect of concentrated n-3 fatty acids versus gemfibrozil on plasma lipoproteins, low density lipoprotein heterogeneity and oxidizability in patients with hypertriglyceridemia. Atherosclerosis. 2000 Nov:153(1):129-38 [PubMed PMID: 11058707]
Level 1 (high-level) evidenceChapman MJ. Fibrates in 2003: therapeutic action in atherogenic dyslipidaemia and future perspectives. Atherosclerosis. 2003 Nov:171(1):1-13 [PubMed PMID: 14642400]
Level 3 (low-level) evidenceHarris WS, Pottala JV, Thiselton DL, A Varvel S, Baedke AM, Dayspring TD, Warnick GR, McConnell JP. Does APOE genotype modify the relations between serum lipid and erythrocyte omega-3 fatty acid levels? Journal of cardiovascular translational research. 2014 Jul:7(5):526-32. doi: 10.1007/s12265-014-9554-8. Epub 2014 Mar 5 [PubMed PMID: 24595593]
Level 2 (mid-level) evidenceMcKenney J. New perspectives on the use of niacin in the treatment of lipid disorders. Archives of internal medicine. 2004 Apr 12:164(7):697-705 [PubMed PMID: 15078639]
Level 3 (low-level) evidenceCapitena CE, Wagoner HJ, Ruzas CM, Bennett TD, Baker PR 2nd, Jung JL, Weisfeld-Adams JD. Rapid resolution of infantile lipemia retinalis following exchange transfusion. Journal of inherited metabolic disease. 2016 Nov:39(6):889-890 [PubMed PMID: 27518769]
Schaap-Fogler M, Schurr D, Schaap T, Leitersdorf E, Rund D. Long-term plasma exchange for severe refractory hypertriglyceridemia: a decade of experience demonstrates safety and efficacy. Journal of clinical apheresis. 2009:24(6):254-8. doi: 10.1002/jca.20224. Epub [PubMed PMID: 19927362]
Patel DV, Snead MP, Satchi K. Retinal arteriolar calcification in a patient with chronic renal failure. The British journal of ophthalmology. 2002 Sep:86(9):1063 [PubMed PMID: 12185140]
Level 3 (low-level) evidenceHinkle JW, Relhan N, Flynn HW Jr. Lipemia Retinalis, Macular Edema, and Vision Loss in a Diabetic Patient with a History of Type IV Hypertriglyceridemia and Pancreatitis. Case reports in ophthalmology. 2018 Sep-Dec:9(3):425-430. doi: 10.1159/000493384. Epub 2018 Oct 2 [PubMed PMID: 30386228]
Level 3 (low-level) evidenceIsmail FF, Md Redzuan A, Wen CW. Patient-centered education in dyslipidemia management: a systematic review. Asian biomedicine : research, reviews and news. 2022 Oct:16(5):214-236. doi: 10.2478/abm-2022-0026. Epub 2023 Jun 16 [PubMed PMID: 37551316]
Level 1 (high-level) evidenceXu S, Zhang X, Jiang B, Sun D. Lipid-rich vitreous hemorrhage associated with lipemia retinalis in a young patient with proliferative diabetic retinopathy. BMC ophthalmology. 2026 Jan 16:26(1):71. doi: 10.1186/s12886-026-04618-x. Epub 2026 Jan 16 [PubMed PMID: 41546032]
Park SC, Park HS, Jung WH, Park JH, Han JW, Park TK. Lipemia Retinalis with Proliferative Diabetic Retinopathy: A Case Report. Korean journal of ophthalmology : KJO. 2026 Apr:40(2):209-211. doi: 10.3341/kjo.2025.0136. Epub 2026 Jan 8 [PubMed PMID: 41502312]
Kimber K, Crawley E, Jones S. Severe hypertriglyceridaemia and lipaemia retinalis in a child presenting with diabetic ketoacidosis. Diabetic medicine : a journal of the British Diabetic Association. 2025 Jun:42(6):e70026. doi: 10.1111/dme.70026. Epub 2025 Apr 14 [PubMed PMID: 40223777]
Hansa C, Vijayakumar V, Chinnasami B, Sundar S. Lipemic Serum in a Child With New-Onset Type 1 Diabetes Mellitus Presenting With Diabetic Ketoacidosis: A Case Report. Cureus. 2023 Sep:15(9):e45777. doi: 10.7759/cureus.45777. Epub 2023 Sep 22 [PubMed PMID: 37872901]
Level 3 (low-level) evidenceMajeed GM, Valor Suárez C, Mann S. Incidental diagnosis of asymptomatic lipaemia retinalis in a patient with uncontrolled type 2 diabetes mellitus: 'white lines'. BMJ case reports. 2023 Jul 6:16(7):. doi: 10.1136/bcr-2022-253363. Epub 2023 Jul 6 [PubMed PMID: 37419497]