Introduction
The epidermis is comprised of 4 or 5 layers, depending on the location of the skin sampled. These layers, from deep to superficial, are stratum basale, stratum spinosum, stratum granulosum, stratum lucidum, and stratum corneum. The stratum lucidum is typically only present in the thick skin found in areas such as the palm or soles. The basal layer of the epidermis contains keratinocytes in their least differentiated form, wherein they proliferate and undergo mitosis. As keratinocytes mature and differentiate, they migrate to the surface, produce keratin, and eventually lose their nuclei and other cellular organelles; these cells form the stratum corneum, or the horny layer of the skin. Keratin, the basic constituent protein of the skin and its appendages, is arranged in the form of keratin filament bundles. Filaggrin is one of the major intermediate filament-associated proteins that interact with keratin filaments in the skin. The precursor form, called profilaggrin, accumulates in cytoplasmic granules of the granular layer as keratohyalin granules (KHGs).
Keratohyalin granules primarily exist within the stratum granulosum, with some present in the stratum spinosum. These granules are insoluble in water and located within the cytoplasm, where they promote cellular dehydration. Their chief function seems to be cross-linking keratin filaments, which creates the tight barrier of the epidermis, providing the body with an impermeable layer that protects against invasion by foreign particles. This process of cornification of the epidermis effected by KHG is known as keratinization.
Issues of Concern
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Issues of Concern
This article examines the histology of KHG found within the epidermal layer of the skin and will discuss the following: The structure and functions of KHG, tissue preparation prior to examination of granules, histochemistry and cytochemistry, electron microscopy, and relevant pathophysiology with clinical correlation.
Structure
Skin and Mucosa
Keratohyalin granules are typically present in the stratum granulosum of the epidermal layer of the skin (and epithelium of the mucosae). KHG are protein structures found in the keratinocytes of the stratum granulosum that appear in two main variants. Globular KHG are found in quickly dividing epithelia, such as the oral mucosa, whereas stellate KHG are found in the slowly dividing normal epidermis.[1] The granules typically contain a mixture of keratin filament bundles and the filament-associated proteins loricrin, filaggrin, and trichohyalin.[2][3]
Thymus
Additionally, KHG is also present in the cytoplasm of Hassall corpuscles of the thymus gland.[4] Hassall's corpuscles, also called type VI epithelioreticular cells, are present in the medulla of the thymus gland. Apart from KHG, their cytoplasm also contains intermediate fibers and may be keratinized. Although the precise function of thymic KHG and the keratinization of Hassall corpuscles remains unknown, they have been suggested to produce IL-4 and IL-7 to support T lymphocyte development.
Function
Keratinisation
Keratohyalin granules promote the formation of the epidermal cornified cell envelope, also known as cornification or keratinization. Visualization of these granules across the various epidermal layers shows that they progressively increase in size as they move from the stratum spinosum toward the stratum corneum.[5] In the smaller keratohyalin granules located within the deeper epidermal layers, dense aggregates of ribosomes are observed at the sites of blebs, indicating protein assembly and the initial formation of keratin intermediate filaments.[6] As keratinocytes differentiate and the granules enlarge, keratohyalin granules convert keratin tonofilaments into a homogeneous keratin matrix, an important step in cornification.[7]
The name filaggrin is a contraction of filament aggregating protein. In vitro experiments have shown that filaggrin causes bundling and condensation of keratin intermediate filaments.[8] Various techniques, including immunohistochemistry, immunoelectron microscopy, and biochemical studies, have revealed that profilaggrin, the large (> 400 kDa) precursor protein of filaggrin, is the main constituent of the KHG.[9] The abundance of profilaggrin/filaggrin as constituents of the KHG renders these granules visible, allowing demarcation of stratum granulosum by low-power light microscopy in skin sections stained with hematoxylin & eosin.[10]
The process of keratinization, or the formation of the cornified cell envelope, is a complex phenomenon. Keratinization involves cross-linking of various proteins at the cell periphery, especially loricrin and involucrin, at the transition zone between the stratum granulosum and stratum corneum.[11] Profilaggrin is inactive within the KHG, but during epidermal differentiation of granular layer keratinocytes committing to form the squames of stratum corneum, these granules vanish as profilaggrin rapidly processes into free filaggrin monomers.[9] This process leads to condensation of the cytoskeleton and flattening of the terminally differentiating granular cells into corneal squames. A complex cascade of phosphatases and proteases is involved in this rapid degranulation event.[9]
Epidermal Moisturization via Water Retention in Stratum Corneum
Within the squames, filaggrin undergoes further chemical modification and proteolytic processing. Eventually, it breaks down completely into the natural moisturizing factor (NMF), a natural humectant within the residual cytoplasmic space of the squames, composed of hygroscopic amino acids and their derivatives.[10]
Other Indirect Functions
Through their contributions to keratinization and water retention in the stratum corneum, KHG and its constituent proteins support other functions, such as UV protection and modulation of stratum corneum pH (to make it hostile to pathogenic microbes). Thus, as a whole, KHG, filaggrin, and related proteins are vital for normal healthy function of the skin barrier layers.
Tissue Preparation
Traditionally, acetic acid has been used to obtain sheet preparations of the stratum granulosum from the epidermis and oral epithelium of rodents and man.[12] Currently, a variety of effective tissue preparation methods for visualizing KHG have been proposed. Standard lab methods are typically appropriate for preparation and fixation of epidermal tissue. Reconstructed human epidermis (RHE) is a recently developed model for studying epidermal cellular kinetics, including KHGs, lamellar bodies, and other functional structures.
Standard Method
A standard method was found to be effective. Specimens should be processed immediately following surgical excision and washed once in 1X phosphate-buffered saline. Small pieces are typically best for preparation, typically sizes less than 1 mm. Tissue can then be frozen in optimal cutting temperature medium for cryosection formation, or it can be fixed in formaldehyde or ethanol prior to paraffin embedding, after which they are sliced and placed on slides for further staining or analysis.[13][14]
Reconstructed Human Epidermis
Models of RHE are useful for evaluating the physicochemical properties of the epidermis, conducting metabolic studies of pharmaceutical products, assessing epidermal responses to irritants and sensitizers, and assessing cutaneous irritancy or phototoxicity.[15] RHE prepared by culturing normal human keratinocytes at high cell density for a few weeks (average of 14 days) in a serum-free and high calcium (1.5 mM) medium on an inert polycarbonate filter at the air-liquid interface showed histological features similar to those observed in vivo in the epidermis: a proliferating basal layer and differentiating spinous, granular, and cornified layers. Electron microscopy illustrated lamellar bodies, junctions, and keratohyalin granules.[15] Such models are customizable for studies involving epidermal keratinocytes and their key constituents, including KHG, lamellar bodies, and keratin intermediate filaments.
Histochemistry and Cytochemistry
A variety of histochemical and immunohistochemical staining methods can be used to examine KHG in tissue samples. Several examples are listed below that, at the time of their publication, provided greater insight into the structure and function of keratohyalin granules.
Hematoxylin and eosin (H&E) staining is a particularly effective method for examining KHG. This is largely due to the granules' hematoxylin stainability. The stainability of KHG is thought to be due to the fibrinogen γ-chain protein found within the granules, which is demonstrably basophilic.[16] The basophilic staining of KHG makes them appear blue on H&E staining, facilitating identification of the stratum granulosum in the epidermis in an H&E-stained section (see Image. Figure 1).
Bennett reagent is a simple and rapid method of identifying free sulfhydryl groups.[17] The high number of free sulfhydryl groups in KHG also enables histochemical staining with Bennett reagent. Staining shows increased density of sulfhydryl groups within the stratum granulosum, with moderate staining in the stratum spinosum.[18] The protein filaggrin, found within KHG, has a relatively high presence of histidine. Antibodies raised against this protein have been used to visualize keratohyalin granules by immunohistochemistry.[19]
Microscopy, Electron
Electron microscopy has been shown to be an effective method for visualizing the process of cornification in human skin, in which KHG play a major role. Keratohyalin granules are apparent as electron-dense granules that appear in the cytoplasm of cells, where they can be seen forming a sheath around the tonofibrils and ultimately associating with keratin filaments in the more superficial layers of the epidermis.[20] Greater insight into the role of KHG in the cornification process initially emerged after protease treatment and electron microscopy. The findings were that the thickening of the cell membranes in the stratum corneum is not the result of the addition of material from outside the cell, but rather the deposition of protein material on the cytoplasmic side of the membrane.[21]
Pathophysiology
Unique characteristics of keratohyalin granule immunohistochemistry have been used to evaluate many pathologic conditions of the skin and have also led to a better understanding of healthy physiology. Histochemistry of the granules in human oral leukoplakia showed staining with Pauly reagent, Congo red, and hematoxylin, suggesting a high protein content within the granules; however, the keratohyalin granules did not react with Feulgen reagent, indicating the absence of DNA.[14]
Clinical Significance
The antiperinuclear factor is a rheumatoid arthritis-specific autoantibody that is present in 49% to 91% of patients with rheumatoid arthritis. Immunohistochemical staining with anti–perinuclear factor antibodies shows staining of KHG.[22] Identification of hypergranulosis or hypogranulosis on H&E staining is often helpful in the histological diagnosis of skin conditions such as psoriasis, lichen planus, Bowen disease, and actinic keratosis, among others. The presence of coarse KHG in cases of irritated seborrheic keratosis is useful to differentiate seborrheic keratosis from verruca vulgaris, as the coarse granules are a specific feature of irritated seborrheic keratosis.[23]
One of the main proteinaceous components of KHG is filaggrin, which is essential in facilitating cellular compression and the biogenesis of the stratum corneum. Loss-of-function mutations in the filaggrin gene have been shown to cause many conditions, including the monogenic genodermatosis ichthyosis vulgaris and atopic dermatitis (eczema). A number of independent and complementary genetic studies demonstrate that inheritance of a loss-of-function mutation in the filaggrin (FLG) gene confers a high risk of atopic dermatitis and related atopic diseases, such as ichthyosis vulgaris.[10]
Media
(Click Image to Enlarge)
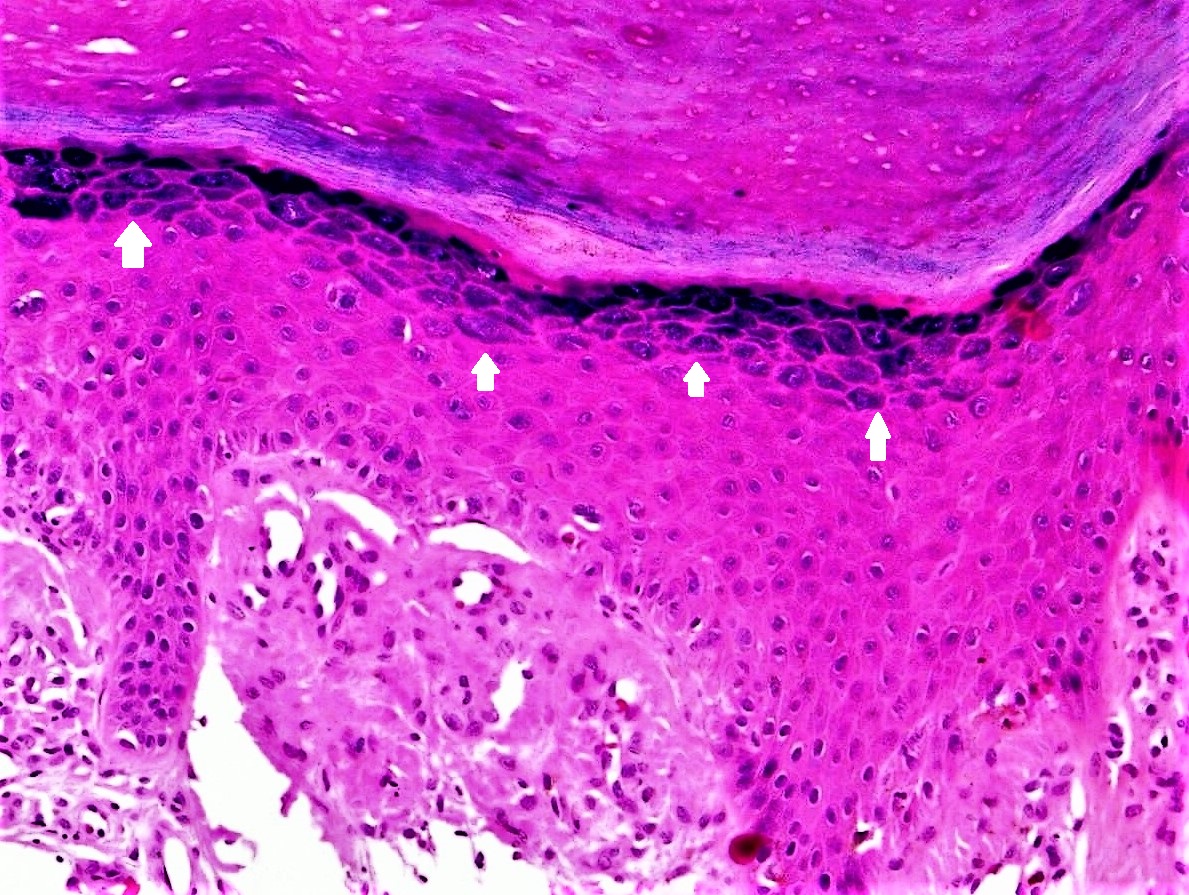
Figure 1. Histological demonstration of keratohyalin granules in a biopsy specimen obtained from the skin and stained with hematoxylin & eosin. The granules (highlighted by white arrows) appear blue owing to their basophilic nature. This section was taken from a lesion of lichen simplex chronicus, and therefore displays epidermal changes including hypergranulosis apart from hyperkeratosis (thickened stratum corneum), and irregular acanthosis (thickening of stratum spinosum). [hematoxylin & eosin, 400X] Contributed by Sidharth Sonthalia, MD, DNB, MNAMS
References
Westerhof W, Dingemans KP. The morphology of keratohyalin granules in orthokeratotic and parakeratotic skin and oral mucosa. International journal of dermatology. 1987 Jun:26(5):308-13 [PubMed PMID: 2440821]
Manabe M, O'Guin WM. Keratohyalin, trichohyalin and keratohyalin-trichohyalin hybrid granules: an overview. The Journal of dermatology. 1992 Nov:19(11):749-55 [PubMed PMID: 1284067]
Level 3 (low-level) evidenceNithya S, Radhika T, Jeddy N. Loricrin - an overview. Journal of oral and maxillofacial pathology : JOMFP. 2015 Jan-Apr:19(1):64-8. doi: 10.4103/0973-029X.157204. Epub [PubMed PMID: 26097310]
Level 3 (low-level) evidenceSauls RS, McCausland C, Taylor BN. Histology, T-Cell Lymphocyte. StatPearls. 2026 Jan:(): [PubMed PMID: 30571054]
Fukuyama K, Epstein WL. Heterogeneous ultrastructure of keratohyalin granules: a comparative study of adjacent skin and mucous membrane. The Journal of investigative dermatology. 1973 Aug:61(2):94-100 [PubMed PMID: 4125555]
Level 3 (low-level) evidenceWesterhof W, Dingemans KP. The morphological details of globular keratohyalin granules. Journal of cutaneous pathology. 1986 Oct:13(5):375-82 [PubMed PMID: 3782575]
Yousef H, Alhajj M, Fakoya AO, Sharma S. Anatomy, Skin (Integument), Epidermis. StatPearls. 2026 Jan:(): [PubMed PMID: 29262154]
Presland RB, Kuechle MK, Lewis SP, Fleckman P, Dale BA. Regulated expression of human filaggrin in keratinocytes results in cytoskeletal disruption, loss of cell-cell adhesion, and cell cycle arrest. Experimental cell research. 2001 Nov 1:270(2):199-213 [PubMed PMID: 11640884]
Level 3 (low-level) evidenceSandilands A, Sutherland C, Irvine AD, McLean WH. Filaggrin in the frontline: role in skin barrier function and disease. Journal of cell science. 2009 May 1:122(Pt 9):1285-94. doi: 10.1242/jcs.033969. Epub [PubMed PMID: 19386895]
Level 3 (low-level) evidenceMcLean WH. Filaggrin failure - from ichthyosis vulgaris to atopic eczema and beyond. The British journal of dermatology. 2016 Oct:175 Suppl 2(Suppl Suppl 2):4-7. doi: 10.1111/bjd.14997. Epub [PubMed PMID: 27667308]
Ishida-Yamamoto A, Igawa S, Kishibe M. Molecular basis of the skin barrier structures revealed by electron microscopy. Experimental dermatology. 2018 Aug:27(8):841-846. doi: 10.1111/exd.13674. Epub 2018 Jun 28 [PubMed PMID: 29704884]
Hume WJ, Moore JK. Sheet preparations of the stratum granulosum from mammalian skin and oral epithelium. Journal of anatomy. 1985 Jun:140 ( Pt 4)(Pt 4):669-78 [PubMed PMID: 3908423]
Level 3 (low-level) evidenceDinh MH, McRaven MD, Kelley Z, Penugonda S, Hope TJ. Keratinization of the adult male foreskin and implications for male circumcision. AIDS (London, England). 2010 Mar 27:24(6):899-906. doi: 10.1097/QAD.0b013e3283367779. Epub [PubMed PMID: 20098294]
Singh B, McKinney RV, Kolas S. Histochemistry of the keratohyalin granules in human oral leukoplakia. Journal of oral pathology. 1975 Sep:4(2):59-66 [PubMed PMID: 51923]
Poumay Y, Dupont F, Marcoux S, Leclercq-Smekens M, Hérin M, Coquette A. A simple reconstructed human epidermis: preparation of the culture model and utilization in in vitro studies. Archives of dermatological research. 2004 Oct:296(5):203-11 [PubMed PMID: 15349789]
Takahashi M, Horiuchi Y, Tezuka T. Hematoxylin-stainability of keratohyalin granules is due to the novel component, fibrinogen γ-chain protein. Archives of dermatological research. 2010 Nov:302(9):679-84. doi: 10.1007/s00403-010-1077-9. Epub 2010 Sep 7 [PubMed PMID: 20821224]
BARRNETT RJ, SELIGMAN AM. Histochemical demonstration of sulfhydryl and disulfide groups of protein. Journal of the National Cancer Institute. 1954 Feb:14(4):769-803 [PubMed PMID: 13233826]
MESCON H, FLESCH P. Modification of Bennett's method for the histochemical demonstration of free sulfhydryl groups in skin. The Journal of investigative dermatology. 1952 Mar:18(3):261-6 [PubMed PMID: 14908200]
Murozuka T, Fukuyama K, Epstein WL. Immunochemical comparison of histidine-rich protein in keratohyalin granules and cornified cells. Biochimica et biophysica acta. 1979 Aug 28:579(2):334-45 [PubMed PMID: 93971]
Level 3 (low-level) evidenceCHARLES A. An electron microscope study of cornification in the human skin. The Journal of investigative dermatology. 1959 Aug:33():65-74 [PubMed PMID: 13809309]
Wolff K, Schreiner E. Differential enzymatic digestion of cytoplasmic components of keratinocytes: electron microscopic observations. Journal of ultrastructure research. 1971 Aug:36(3):437-54 [PubMed PMID: 4106436]
Hoet RM, Voorsmit RA, Van Venrooij WJ. The perinuclear factor, a rheumatoid arthritis-specific autoantigen, is not present in keratohyalin granules of cultured buccal mucosa cells. Clinical and experimental immunology. 1991 Apr:84(1):59-65 [PubMed PMID: 1849807]
Fernandez-Flores A. Irritated seborrheic keratosis with coarse keratohyalin granules. Romanian journal of morphology and embryology = Revue roumaine de morphologie et embryologie. 2009:50(4):583-7 [PubMed PMID: 19942951]