Introduction
The blood supply to the vertebral canal is critical, particularly in surgical and clinical contexts. The spinal cord, housed within the vertebral canal, serves as the essential neuronal connection between the brain and the body. Therefore, preservation of vascular supply is vital. Compromise of this circulation can result in profound and often irreversible neurologic injury.
The vascular architecture of the vertebral canal comprises a complex, highly specialized network that maintains spinal cord viability. The narrow margin for vascular injury necessitates thorough knowledge of this anatomy in neurosurgery, vascular surgery, orthopedics, and spine intervention. This activity synthesizes the arterial, venous, and lymphatic supply of the vertebral canal, incorporating structural anatomy, embryologic development, physiologic variants, and clinical and surgical relevance to enhance diagnostic accuracy and operative safety.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
General Structure
The spinal cord originates at the foramen magnum and extends caudally to the conus medullaris, which typically terminates at the vertebral levels L1 to L2, though termination may range from T12 to L2 or L3.[1][2] Three meningeal layers—dura, arachnoid, and pia mater—surround the cord, with the subarachnoid space extending to approximately the S2 vertebral level.
The vertebral canal comprises 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 4 coccygeal.[3] Perfusion of the spinal cord, nerve roots, and surrounding structures depends on an integrated system of longitudinal spinal arteries, segmental arteries, and radiculomedullary vessels.
Vertebral Anatomy
The vertebral body constitutes the primary weight-bearing component of the spinal column and increases in size in a caudal direction, with lumbar vertebrae bearing the greatest load. Intervertebral discs separate vertebral bodies, providing cushioning and flexibility. Posteriorly, the vertebral arch encloses the vertebral canal and consists of pedicles connecting to the vertebral body and laminae that converge at the midline to form the spinous process.
Superior and inferior articular processes link with adjacent vertebrae to form facet joints and contribute to the intervertebral foramina, which allow spinal nerves and blood vessels to enter and exit. Transverse processes arise at the pedicle–lamina junction and project posterolaterally. In the cervical spine, transverse processes contain transverse foramina that transmit the vertebral arteries bilaterally.
The spinal cord receives arterial supply from 1 anterior spinal artery (ASA) and 2 posterior spinal arteries (PSAs), all arising from the V4 segments of the vertebral arteries. These longitudinal arteries are reinforced by radiculomedullary arteries originating from approximately 21 pairs of segmental arteries branching from the aorta.[4] The artery of Adamkiewicz (AKA) provides a critical blood supply to the lower spinal cord. A circumferential arterial network, the vasa coronae, connects the longitudinal spinal arteries.[5][6] Venous drainage occurs through spinal veins into a valveless vertebral venous plexus, permitting bidirectional flow.
Function
The vertebral canal and spinal column protect the spinal cord, provide structural support, and facilitate the segmental passage of nerves and blood vessels. Disruption of spinal cord blood flow can cause ischemic myelopathy and permanent neurologic deficits, highlighting the clinical significance of this vascular anatomy.[7]
Embryology
Spinal vasculature develops from mesoderm. The spinal cord is initially avascular and becomes vascularized through ingrowth from the perineural vascular plexus, which surrounds the neural tube. This process is guided by vascular endothelial growth factor A signaling from neural progenitor cells.[8][9] Vascularization occurs through 2 complementary mechanisms in a ventral-to-dorsal pattern: ventral endothelial sprouting from the perineural vascular plexus and dorsal migration of isolated angioblasts. Ventral sprouts invade the neural tube adjacent to the floor plate to form the first perfused vessels, while dorsal angioblasts migrate individually to contribute to the intraneural vascular plexus. This process progresses in a craniocaudal sequence beginning caudal to the rhombencephalic neural tube.[10]
Spinal nerve roots are accompanied by radicular arteries that supply the spinal cord. Some of these vessels enlarge to supply multiple spinal levels, while others regress, accounting for the reduced number of radiculomedullary arteries observed in adults compared with the theoretical 31 levels.[11] The vertebral arteries arise from the longitudinal anastomosis of 7 cervical intersegmental arteries. Regression of the first 6 and persistence of the 7th ultimately form the vertebral artery and its connection to the subclavian artery.[12][13]
Blood Supply and Lymphatics
Arterial Supply
The primary arterial supply to the spinal cord is provided by the ASA and paired PSAs (see Image. Arterial Supply of the Spinal Cord and Vertebral Segment). The ASA is formed by branches from each vertebral artery, which arise from the 1st portion of the subclavian artery. The vertebral arteries ascend through the transverse foramina of C6 to C1 and enter the cranial cavity via the foramen magnum. Before uniting to form the basilar artery, each vertebral artery gives rise to a branch from its V4 segment that contributes to the ASA, which descends along the anterior median fissure of the spinal cord.[14]
The PSAs arise either directly from the vertebral arteries or indirectly via the posterior inferior cerebellar artery and descend along the posterolateral sulci.[15] Functionally, the ASA supplies the anterior 2/3 of the spinal cord, whereas the PSAs supply the posterior 1/3. Longitudinal vessels alone are insufficient and are reinforced by segmental spinal arteries entering through the intervertebral foramina at each level. Segmental arteries divide into anterior and posterior radicular arteries, which supply the nerve roots and contribute to the ASA and PSAs. Although 31 radicular arteries are theoretically possible, fewer persist due to embryologic regression. Some segmental arteries give rise to segmental medullary arteries that directly augment spinal cord perfusion. About 8 to 10 such arteries are typically present per individual.
Regional variation in spinal cord blood supply is well recognized. The upper cervical spinal cord is supplied primarily by paired ASAs arising directly from the vertebral arteries, whereas the midcervical region receives segmental medullary branches from the vertebral arteries. The lower cervical to upper thoracic cord is supplied by radiculomedullary arteries from the cervicothoracic trunk (C7–T1). The midthoracic region (T3–T9) is supplied by segmental arteries originating from the posterior intercostal arteries.
The largest and most clinically significant radiculomedullary artery is the AKA, which typically arises from the left side of the descending aorta between T8 and L2 and joins the ASA on the ventral surface of the spinal cord.[16] This vessel supplies a substantial portion of the thoracolumbar spinal cord and corresponds to a watershed region. Branches of the internal iliac arteries contribute to lumbosacral spinal cord perfusion.[17] A circumferential arterial network, the vasa coronae, connects the ASA and PSAs. Central branches from the ASA and penetrating vessels from the vasa coronae supply the spinal cord parenchyma directly.
Venous Drainage
Venous drainage of the spinal cord occurs via anterior and posterior spinal veins, which drain into medullary veins and, subsequently, into the internal vertebral venous (Batson) plexus located within the epidural space.[18] This valveless system permits bidirectional flow and provides a route for metastatic spread. Blood exits the internal plexus through the basivertebral veins into the external vertebral venous plexus, ultimately draining into systemic veins, such as the azygos system in the thoracic region.[19] Pelvic organs, including the bladder, prostate, and rectum, also drain into this plexus.
Lymphatic Drainage
The vertebral column contains an extensive 3-dimensional lymphatic network that drains the epidural space and dura mater.[20] Lymphatic vessels form metameric circuits connecting to peripheral sensory and sympathetic ganglia before draining into lymph nodes and the thoracic duct. Following intraventricular cerebrospinal fluid tracer injection, lymphatic outflow occurs predominantly from the sacral spine to sacral and iliac lymph nodes.[21] Lymphatic vessels are present in the periosteum and paraspinal ligaments but are absent in intact vertebrae and intervertebral discs, appearing only when pathology extends beyond normal anatomic boundaries.[22] These lymphatics play a critical role in immune surveillance and waste clearance within the central nervous system.[23][24]
Physiologic Variants
The most common vertebral artery variant involves the left vertebral artery originating from the aortic arch between the left common carotid and left subclavian arteries. This variant occurs in 2% to 5% of individuals.
Variants of the AKA demonstrate a characteristic distribution. In 75% of cases, the artery inserts into the dura and ASA at the T9 to T12 level. In 15% of cases, insertion occurs at T5 to T8. In 10% of cases, insertion occurs at L1 to L2.
Two variants of the ASA and AKA junction have been described. The 1st variant involves a small-caliber ASA joining a larger-caliber AKA, forming a large ASA descending from that level. This configuration represents an AKA-dominant circulation. Disruption of the AKA in patients with this circulation can result in severe neurologic injury. The 2nd variant involves ASA and AKA of equivalent calibers. Joining of these vessels does not increase the ASA diameter. In this nondominant configuration, disruption of the AKA may not produce immediate neurologic deficits.[25]
Surgical Considerations
Posterior cervical spinal procedures place patients at risk for vertebral artery injury, particularly during instrumentation involving screws near the transverse foramina.[26][27] The V2 segments of the vertebral arteries form anastomoses with spinal arteries, increasing vulnerability during cervical surgery. In cases with a unilateral hypoplastic vertebral artery and bilateral hypoplastic posterior communicating arteries, the dominant vertebral artery becomes critical for posterior circulation perfusion. Injury to this vessel can result in catastrophic outcomes.
Preoperative 3-dimensional computed tomography angiography allows identification of anomalous vertebral artery anatomy and variations in the posterior circle of Willis. Approximately 47% of patients demonstrate some degree of abnormal vertebral artery blood flow on preoperative imaging, with a higher incidence of vertebral artery anomaly in patients with concomitant bony abnormalities.[28][29]
Thoracoabdominal aortic aneurysm repair and anterior thoracolumbar spinal procedures carry a risk of spinal cord ischemia due to disruption of blood flow to the AKA.[30][31] The thoracolumbar segmental arterial network comprises approximately 21 paired arteries, with extensive intersegmental anastomoses. Unilateral ligation of segmental arteries results in an average 8% reduction in spinal blood flow, whereas bilateral ligation reduces flow by approximately 54% and abolishes pulsatility in 75% of vertebrae.
Risk factors for spinal cord ischemia include hyperkyphosis, prior spinal deformity surgery, combined anterior–posterior approaches, left-sided surgical approaches, operating on the concavity of scoliotic curves, and intraoperative or postoperative hypotension. The reported incidence of ischemic injury ranges from 0% to 0.75%.[32]
Preoperative spinal angiography can localize the AKA and determine laterality. This artery is left-sided in approximately 75% to 83% of cases and located between T9 and L1 in 83%.[33] Identification of the vessel alters surgical planning in approximately 54% of thoracolumbar corpectomy cases, often permitting selection of a contralateral approach when feasible. Since the artery most commonly originates on the left, a right-sided transthoracic approach is frequently chosen for anterior spinal surgery to reduce the risk of injury.
Alternative approaches or vessel-preserving techniques should be employed when the planned approach coincides with the artery’s location. Intraoperative neuromonitoring and maintenance of adequate perfusion pressure further reduce the risk of ischemia.[34][35] Disruption of the AKA can result in paraplegia due to ischemia of the lower thoracic and lumbar spinal cord.
Clinical Significance
The clinical importance of vertebral column vascular anatomy lies in the prevention of spinal cord ischemia, recognition of ischemic myelopathy syndromes, and understanding of patterns of vascular vulnerability and collateral compensation. Spinal cord circulation demonstrates both susceptibility to injury and resilience through extensive collateralization.
Spinal Cord Ischemia
The AKA supplies a watershed region of the spinal cord and is particularly vulnerable during episodes of severe hypotension. This vessel typically forms a characteristic hairpin turn before joining the ASA and supplies the distal thoracic and lumbar spinal cord. Since significant anastomoses generally do not exist between the ASA and PSAs, the AKA functions similarly to an end artery. Disruption of dominant radiculomedullary vessels can result in permanent neurologic damage.
Ischemic injury in this region commonly manifests as anterior spinal cord syndrome, characterized by motor paralysis and loss of pain and temperature sensation, with relative preservation of vibration and proprioception mediated by the dorsal columns supplied by the PSAs.[36] Magnetic resonance imaging is diagnostic and may demonstrate the classic “owl’s eye” appearance on axial T2-weighted images.[37]
Collateral Circulation
Despite these vulnerabilities, the spinal cord receives support from a robust collateral network. The paraspinous muscular arterial network possesses approximately 25 times greater flow capacity than the combined ASA and epidural arterial systems.[38] This collateralization accounts for the observation that unilateral segmental artery ligation reduces spinal blood flow by only 8%, whereas bilateral occlusion reduces flow by approximately 54%.[39] Approximately 75% of segmental arteries supply the ASA directly, with the remainder contributing indirectly through collateral pathways.[40] Although this network provides resilience, variability in dominant vessels necessitates individualized assessment.
Vertebrobasilar Insufficiency
The V2 segments of the vertebral arteries are susceptible to extrinsic compression from cervical spondylosis due to their intraosseous course within the transverse foramina.[41] Vertebral artery dissection is an uncommon cause of stroke but occurs more frequently in patients younger than 45 years and may result from blunt cervical trauma, chiropractic manipulation, or underlying connective tissue disorders. Intimal disruption permits blood to dissect through the arterial wall, forming an intramural hematoma and luminal stenosis, thereby reducing posterior circulation perfusion.
Atherosclerotic disease most commonly affects the origins of the vertebral arteries and can produce symptoms such as dizziness, vertigo, diplopia, ataxia, and bilateral sensory deficits through hypoperfusion or atheroembolism. Anatomic variants are common and must be considered during evaluation. Overall prognosis is favorable, with approximately 80% of patients achieving full recovery.[42]
Metastatic Disease
The internal vertebral venous plexus provides a well-established route for metastatic spread due to its valveless architecture.[43] Pelvic malignancies, particularly prostate carcinoma, can spread hematogenously through this plexus to the vertebral column, spinal cord, and brain.[44]
Media
(Click Image to Enlarge)
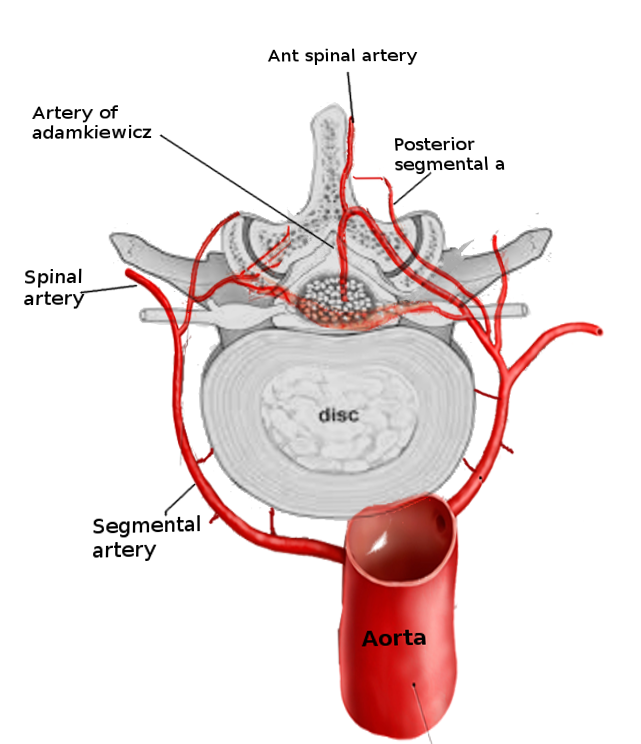
Arterial Supply of the Spinal Cord and Vertebral Segment. This illustration details the vascular network originating from the aorta and branching into the segmental artery. Labels identify the spinal artery, posterior segmental artery, and anterior spinal artery, alongside the artery of Adamkiewicz and the intervertebral disc.
Contributed by S Bhimji, MD
References
Elfiky T, El Mansy Y, Stienen MN, Yunusa S, Elkaref E, Nafady M. Magnetic Resonance Imaging-Based Anatomy of the Conus Medullaris: Variations of Location and Morphology. World neurosurgery. 2025 Mar:195():123646. doi: 10.1016/j.wneu.2024.123646. Epub 2025 Feb 6 [PubMed PMID: 39761913]
Nakashima H, Ito K, Katayama Y, Tsushima M, Ando K, Kobayashi K, Machino M, Ito S, Koshimizu H, Segi N, Tomita H, Imagama S. The Level of Conus Medullaris in 629 Healthy Japanese Individuals. Journal of clinical medicine. 2021 Jul 19:10(14):. doi: 10.3390/jcm10143182. Epub 2021 Jul 19 [PubMed PMID: 34300348]
DeSai C, Reddy V, Agarwal A. Anatomy, Back, Vertebral Column. StatPearls. 2026 Jan:(): [PubMed PMID: 30247844]
Gao L, Wang L, Su B, Wang P, Ye J, Shen H. The vascular supply to the spinal cord and its relationship to anterior spine surgical approaches. The spine journal : official journal of the North American Spine Society. 2013 Aug:13(8):966-73. doi: 10.1016/j.spinee.2013.03.017. Epub 2013 Apr 19 [PubMed PMID: 23608560]
Alvernia JE, Simon E, Khandelwal K, Ramos CD, Perkins E, Kim P, Mertens P, Messina R, Luzardo G, Diaz O. Anatomical study of the thoracolumbar radiculomedullary arteries, including the Adamkiewicz artery and supporting radiculomedullary arteries. Journal of neurosurgery. Spine. 2023 Feb 1:38(2):233-241. doi: 10.3171/2022.5.SPINE2214. Epub 2022 Sep 23 [PubMed PMID: 36152330]
Pruidze P, Didava G, Weninger JT, Geyer SH, Neumayer C, Nanobachvili J, Eilenberg W, Czerny M, Weninger WJ. Intraspinal vascular perfusion territories of the descending thoracic aorta. European journal of cardio-thoracic surgery : official journal of the European Association for Cardio-thoracic Surgery. 2025 Jul 1:67(7):. doi: 10.1093/ejcts/ezaf212. Epub [PubMed PMID: 40576461]
Sliwa JA, Maclean IC. Ischemic myelopathy: a review of spinal vasculature and related clinical syndromes. Archives of physical medicine and rehabilitation. 1992 Apr:73(4):365-72 [PubMed PMID: 1554311]
Vieira JR, Shah B, Ruiz de Almodovar C. Cellular and Molecular Mechanisms of Spinal Cord Vascularization. Frontiers in physiology. 2020:11():599897. doi: 10.3389/fphys.2020.599897. Epub 2020 Dec 21 [PubMed PMID: 33424624]
Ruiz de Almodovar C, Dupraz S, Bonanomi D. Neurovascular dynamics in the spinal cord from development to pathophysiology. Neuron. 2025 Dec 17:113(24):4134-4157. doi: 10.1016/j.neuron.2025.09.017. Epub 2025 Oct 14 [PubMed PMID: 41092899]
Kurz H, Gärtner T, Eggli PS, Christ B. First blood vessels in the avian neural tube are formed by a combination of dorsal angioblast immigration and ventral sprouting of endothelial cells. Developmental biology. 1996 Jan 10:173(1):133-47 [PubMed PMID: 8575615]
Demondion X, Lefebvre G, Fisch O, Vandenbussche L, Cepparo J, Balbi V. Radiographic anatomy of the intervertebral cervical and lumbar foramina (vessels and variants). Diagnostic and interventional imaging. 2012 Sep:93(9):690-697. doi: 10.1016/j.diii.2012.07.008. Epub 2012 Aug 9 [PubMed PMID: 22883939]
Yuan SM. Aberrant Origin of Vertebral Artery and its Clinical Implications. Brazilian journal of cardiovascular surgery. 2016 Feb:31(1):52-9. doi: 10.5935/1678-9741.20150071. Epub [PubMed PMID: 27074275]
Bueno HF, Nimchinsky EA. Mapping of Anatomic Variants of the Proximal Vertebral Artery in Relation to Embryology. AJNR. American journal of neuroradiology. 2023 Aug:44(8):943-950. doi: 10.3174/ajnr.A7942. Epub 2023 Jul 27 [PubMed PMID: 37500289]
Ali F, Reddy V, Dublin AB. Anatomy, Back, Anterior Spinal Artery. StatPearls. 2026 Jan:(): [PubMed PMID: 30422558]
Boll DT, Bulow H, Blackham KA, Aschoff AJ, Schmitz BL. MDCT angiography of the spinal vasculature and the artery of Adamkiewicz. AJR. American journal of roentgenology. 2006 Oct:187(4):1054-60 [PubMed PMID: 16985157]
Lindeire S, Hauser JM. Anatomy, Back, Artery of Adamkiewicz. StatPearls. 2026 Jan:(): [PubMed PMID: 30422566]
Singh U, Silver JR, Welply NC. Hypotensive infarction of the spinal cord. Paraplegia. 1994 May:32(5):314-22 [PubMed PMID: 8058348]
Level 3 (low-level) evidenceCarpenter K, Decater T, Iwanaga J, Maulucci CM, Bui CJ, Dumont AS, Tubbs RS. Revisiting the Vertebral Venous Plexus-A Comprehensive Review of the Literature. World neurosurgery. 2021 Jan:145():381-395. doi: 10.1016/j.wneu.2020.10.004. Epub 2020 Oct 10 [PubMed PMID: 33049379]
Nathoo N, Caris EC, Wiener JA, Mendel E. History of the vertebral venous plexus and the significant contributions of Breschet and Batson. Neurosurgery. 2011 Nov:69(5):1007-14; discussion 1014. doi: 10.1227/NEU.0b013e3182274865. Epub [PubMed PMID: 21654535]
Jacob L, Boisserand LSB, Geraldo LHM, de Brito Neto J, Mathivet T, Antila S, Barka B, Xu Y, Thomas JM, Pestel J, Aigrot MS, Song E, Nurmi H, Lee S, Alitalo K, Renier N, Eichmann A, Thomas JL. Anatomy and function of the vertebral column lymphatic network in mice. Nature communications. 2019 Oct 9:10(1):4594. doi: 10.1038/s41467-019-12568-w. Epub 2019 Oct 9 [PubMed PMID: 31597914]
Ma Q, Decker Y, Müller A, Ineichen BV, Proulx ST. Clearance of cerebrospinal fluid from the sacral spine through lymphatic vessels. The Journal of experimental medicine. 2019 Nov 4:216(11):2492-2502. doi: 10.1084/jem.20190351. Epub 2019 Aug 27 [PubMed PMID: 31455602]
Kashima TG, Dongre A, Athanasou NA. Lymphatic involvement in vertebral and disc pathology. Spine. 2011 May 15:36(11):899-904. doi: 10.1097/BRS.0b013e3182050284. Epub [PubMed PMID: 21343852]
Tamura R, Yoshida K, Toda M. Current understanding of lymphatic vessels in the central nervous system. Neurosurgical review. 2020 Aug:43(4):1055-1064. doi: 10.1007/s10143-019-01133-0. Epub 2019 Jun 18 [PubMed PMID: 31209659]
Level 3 (low-level) evidenceGonuguntla S, Herz J. Unraveling the lymphatic system in the spinal cord meninges: a critical element in protecting the central nervous system. Cellular and molecular life sciences : CMLS. 2023 Nov 20:80(12):366. doi: 10.1007/s00018-023-05013-1. Epub 2023 Nov 20 [PubMed PMID: 37985518]
N'da HA, Chenin L, Capel C, Havet E, Le Gars D, Peltier J. Microsurgical anatomy of the Adamkiewicz artery-anterior spinal artery junction. Surgical and radiologic anatomy : SRA. 2016 Jul:38(5):563-7. doi: 10.1007/s00276-015-1596-3. Epub 2015 Dec 1 [PubMed PMID: 26627692]
Simon LV, Nassar AK, Mohseni M. Vertebral Artery Injury. StatPearls. 2026 Jan:(): [PubMed PMID: 29262106]
Turgut M, Akhaddar A, Turgut AT, Hall WA. Iatrogenic Vascular Injury Associated with Cervical Spine Surgery: A Systematic Literature Review. World neurosurgery. 2022 Mar:159():83-106. doi: 10.1016/j.wneu.2021.12.068. Epub 2021 Dec 24 [PubMed PMID: 34958995]
Level 1 (high-level) evidenceSano A, Hirano T, Watanabe K, Izumi T, Endo N, Ito T, Inagawa S. Preoperative evaluation of the vertebral arteries and posterior portion of the circle of Willis for cervical spine surgery using 3-dimensional computed tomography angiography. Spine. 2013 Jul 1:38(15):E960-7. doi: 10.1097/BRS.0b013e318296e542. Epub [PubMed PMID: 23609201]
Lin X, Zhu HJ, Xu Y, Zheng T, Lin FY, Yin XM. Prevalence of Vertebral artery anomaly in upper cervical and its surgical implications: a systematic review. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2021 Dec:30(12):3607-3613. doi: 10.1007/s00586-021-07015-8. Epub 2021 Oct 3 [PubMed PMID: 34601625]
Level 1 (high-level) evidenceLella SK, Waller HD, Pendleton A, Latz CA, Boitano LT, Dua A. A systematic review of spinal cord ischemia prevention and management after open and endovascular aortic repair. Journal of vascular surgery. 2022 Mar:75(3):1091-1106. doi: 10.1016/j.jvs.2021.10.039. Epub 2021 Nov 2 [PubMed PMID: 34740806]
Level 1 (high-level) evidencePini R, Faggioli G, Paraskevas KI, Alaidroos M, Palermo S, Gallitto E, Gargiulo M. A systematic review and meta-analysis of the occurrence of spinal cord ischemia after endovascular repair of thoracoabdominal aortic aneurysms. Journal of vascular surgery. 2022 Apr:75(4):1466-1477.e8. doi: 10.1016/j.jvs.2021.10.015. Epub 2021 Nov 1 [PubMed PMID: 34736999]
Level 1 (high-level) evidenceShlobin NA, Raz E, Shapiro M, Clark JR, Hoffman SC, Shaibani A, Hurley MC, Ansari SA, Jahromi BS, Dahdaleh NS, Potts MB. Spinal neurovascular complications with anterior thoracolumbar spine surgery: a systematic review and review of thoracolumbar vascular anatomy. Neurosurgical focus. 2020 Sep:49(3):E9. doi: 10.3171/2020.6.FOCUS20373. Epub [PubMed PMID: 32871559]
Level 1 (high-level) evidenceFanous AA, Lipinski LJ, Krishna C, Roger EP, Siddiqui AH, Levy EI, Leonardo J, Pollina J. The Impact of Preoperative Angiographic Identification of the Artery of Adamkiewicz on Surgical Decision Making in Patients Undergoing Thoracolumbar Corpectomy. Spine. 2015 Aug 1:40(15):1194-9. doi: 10.1097/BRS.0000000000000909. Epub [PubMed PMID: 25816140]
Buhl LK, Bastos AB, Pollard RJ, Arle JE, Thomas GP, Song Y, Boone MD. Neurophysiologic Intraoperative Monitoring for Spine Surgery: A Practical Guide From Past to Present. Journal of intensive care medicine. 2021 Nov:36(11):1237-1249. doi: 10.1177/0885066620962453. Epub 2020 Sep 28 [PubMed PMID: 32985340]
Ikwuegbuenyi CA, Willett N, Elsayed G, Kashlan O, Härtl R. Next-Generation Neuromonitoring in Minimally Invasive Spine Surgery: Indications, Techniques, and Clinical Outcomes. Neurosurgery. 2025 Mar 1:96(3S):S111-S118. doi: 10.1227/neu.0000000000003330. Epub 2025 Feb 14 [PubMed PMID: 39950791]
Level 2 (mid-level) evidenceZedde M, De Falco A, Zanferrari C, Guarino M, Pezzella FR, Haggiag S, Cossu G, Quatrale R, Micieli G, Del Sette M, Pascarella R. Spinal Cord Infarction: Clinical and Neuroradiological Clues of a Rare Stroke Subtype. Journal of clinical medicine. 2025 Feb 15:14(4):. doi: 10.3390/jcm14041293. Epub 2025 Feb 15 [PubMed PMID: 40004823]
Kaiser JT, Reddy V, Lugo-Pico JG. Anatomy, Back, Spinal Cord Arteries. StatPearls. 2026 Jan:(): [PubMed PMID: 30725904]
Etz CD, Kari FA, Mueller CS, Silovitz D, Brenner RM, Lin HM, Griepp RB. The collateral network concept: a reassessment of the anatomy of spinal cord perfusion. The Journal of thoracic and cardiovascular surgery. 2011 Apr:141(4):1020-8. doi: 10.1016/j.jtcvs.2010.06.023. Epub [PubMed PMID: 21419903]
Level 3 (low-level) evidenceMiller LK, Patel VI, Wagener G. Spinal Cord Protection for Thoracoabdominal Aortic Surgery. Journal of cardiothoracic and vascular anesthesia. 2022 Feb:36(2):577-586. doi: 10.1053/j.jvca.2021.06.024. Epub 2021 Jun 26 [PubMed PMID: 34366215]
Ouzounian M, Tadros RO, Svensson LG, Lyden SP, Oderich GS, Coselli JS. Thoracoabdominal Aortic Disease and Repair: JACC Focus Seminar, Part 3. Journal of the American College of Cardiology. 2022 Aug 23:80(8):845-856. doi: 10.1016/j.jacc.2021.05.056. Epub [PubMed PMID: 35981828]
Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL, Cates CU, Creager MA, Fowler SB, Friday G, Hertzberg VS, McIff EB, Moore WS, Panagos PD, Riles TS, Rosenwasser RH, Taylor AJ, American College of Cardiology Foundation, American Stroke Association, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, Society for Vascular Surgery. 2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery. Circulation. 2011 Jul 26:124(4):489-532. doi: 10.1161/CIR.0b013e31820d8d78. Epub 2011 Jan 31 [PubMed PMID: 21282505]
Level 1 (high-level) evidenceTavakoli SG, Britt TB, Agarwal S. Vertebral Artery Dissection. StatPearls. 2026 Jan:(): [PubMed PMID: 28722857]
Kenzhegulov YN, Zhamoldin DK, Aleinikov VG, Kerimbayev TT, Zhetpisbaev B, Akshulakov S. Extensive thoracic vertebral and chest wall metastases as the initial presentation of breast cancer: a case report and literature review. Frontiers in oncology. 2025:15():1632700. doi: 10.3389/fonc.2025.1632700. Epub 2025 Jul 17 [PubMed PMID: 40746598]
Level 3 (low-level) evidenceMaccauro G, Spinelli MS, Mauro S, Perisano C, Graci C, Rosa MA. Physiopathology of spine metastasis. International journal of surgical oncology. 2011:2011():107969. doi: 10.1155/2011/107969. Epub 2011 Aug 10 [PubMed PMID: 22312491]