Introduction
The sphenopalatine artery (SPA) is a well-recognized vessel in otolaryngology and is commonly termed the "artery of epistaxis." Epistaxis is among the most frequent ear, nose, and throat–related emergencies, and approximately 60% of the population experiences at least an episode during a lifetime.[1][2] Most cases of epistaxis are anterior in origin and arise from the Kiesselbach plexus. The SPA is the most common source of posterior epistaxis, which occurs less frequently. Management is challenging because the vessel is difficult to visualize and often produces brisk hemorrhage.[3]
The SPA typically divides into 2 principal branches: septal and posterior lateral nasal. Additional branches are frequently present, and the intranasal course demonstrates considerable anatomic variability. Detailed knowledge of SPA anatomy and adjacent structures is essential for effective control of posterior epistaxis refractory to conservative measures.[4]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The SPA is a terminal branch of the maxillary artery, which arises from the external carotid artery.[5] The maxillary artery is classically divided into 3 segments: mandibular, pterygoid, and pterygopalatine. The SPA originates from the pterygopalatine segment of the maxillary artery within the pterygopalatine fossa (see Image. Plan of the Maxillary Artery Branches).[6] The pterygopalatine fossa lies posterior to the medial wall of the maxillary sinus and contains the maxillary artery and nerve, as well as the pterygopalatine ganglion, collectively forming the principal neurovascular conduit to the nasal cavity.
From its origin, the SPA courses medially and anteriorly through the pterygopalatine fossa toward the sphenopalatine foramen to enter the nasal cavity (see Image. Nasal Cavity Blood Supply).[7][8][9] The borders of the sphenopalatine foramen include the body of the sphenoid superiorly, the orbital process of the palatine bone anteriorly, the sphenoidal process posteriorly, and the perpendicular plate of the palatine bone inferiorly.
Although positional variability exists, the foramen is most commonly located at the junction between the middle and superior meatus (see Image. Sphenopalatine Foramen). This location is frequently just superior to the posterior end of the horizontal lamella of the middle turbinate. The ethmoidal crest of the palatine bone lies immediately anterior to the foramen and serves as a reliable landmark for endoscopic identification. In most individuals, the foramen is located posterior to the ethmoidal crest. Several studies describe accessory foramina, reflecting the frequent branching of the SPA before entry into the nasal cavity.
The SPA demonstrates considerable anatomic variability. About 1 to 10 branches may arise, with more than 2 present in 97% of individuals and more than 3 identified in 67%. Branching may occur before the artery reaches the sphenopalatine foramen. In approximately 42% of specimens, early division produces separate bony foramina.
Immediately medial to the crista ethmoidalis, 2 or more branches are identified in the majority of cases. At least 3 branches are present in 67% of individuals, while 4 or more branches occur in approximately 1/3. Despite variability in branch number and distribution, 2 principal vessels are consistently described: the posterior septal and posterior lateral nasal.[10]
The posterior septal artery crosses the anteroinferior margin of the sphenoid sinus and supplies the posterior nasal septum. The posterior lateral nasal artery descends along the perpendicular plate of the palatine bone toward the posterior end of the middle turbinate. This vessel continues inferiorly to supply the middle and inferior turbinates and the lateral nasal wall.[11] The posterior lateral nasal artery serves as the dominant arterial supply to the lateral nasal wall. Therefore, surgical management of refractory epistaxis requires ligation of this artery proximal to the branch supplying the middle turbinate.
The SPA provides the primary arterial supply to the nasal cavity, accounting for up to 90% of mucosal perfusion. The artery irrigates the lateral nasal wall, the superior, middle, and inferior turbinates, the fontanelle regions, and the posterior 2/3 of the nasal septum.[12] The anterior and superior portions of the septum receive blood from the anterior and posterior ethmoidal arteries. The ethmoidal artery originates from the ophthalmic artery, which derives from the internal carotid artery.
Within the nasal septum, the SPA participates in an extensive anastomotic network. The Kiesselbach plexus, or the Little area, represents the convergence of branches from both the internal (anterior and posterior ethmoidal arteries) and external (superior labial artery, greater palatine artery, and posterior septal branch of the SPA) carotid arteries (see Image. Arterial and Venous Anatomy of the Head and Neck).[13]
Embryology
During developmental weeks 4 and 5, the aortic sac gives rise to the aortic (pharyngeal) arches. The maxillary artery emerges from the mesoderm of the 1st aortic arch and subsequently gives rise to the SPA. The number of developing branches and the diameter of the SPA determine the number and morphology of the sphenopalatine foramina in the palatine bone.[14]
Nerves
The maxillary nerve constitutes the 2nd branch of the trigeminal nerve (cranial nerve V2) and courses in proximity to the maxillary artery. The nerve extends from the middle cranial fossa into the pterygopalatine fossa via the foramen rotundum.[15] Within the pterygopalatine fossa, the maxillary nerve gives rise to multiple branches, including the infraorbital, nasopalatine, zygomatic, superior alveolar, pharyngeal, and the greater and lesser palatine nerves. The maxillary nerve also establishes communication with the pterygopalatine ganglion, which is suspended by 2 small trunks termed the "pterygopalatine nerves."[16]
The pterygopalatine ganglion resides deep within the pterygopalatine fossa near the sphenopalatine foramen.[17] The ganglion is the largest parasympathetic structure associated with the maxillary nerve branches and receives preganglionic input primarily from the greater petrosal branch of the facial nerve (cranial nerve VII) via the Vidian nerve.
The Vidian nerve forms from the junction of the greater petrosal nerve, containing preganglionic parasympathetic fibers, and the deep petrosal nerve, originating from the carotid plexus and containing postganglionic sympathetic fibers. Only the preganglionic parasympathetic fibers synapse within the pterygopalatine ganglion. Postganglionic parasympathetic fibers distribute through their respective branches to provide secretomotor innervation to the lacrimal gland and mucosal glands of the oral cavity, nose, and pharynx.[18]
The nasopalatine branch courses alongside the SPA and enters the nasal cavity through the sphenopalatine foramen. This nerve travels across the roof of the nasal cavity, inferior to the sphenoid sinus orifice, to reach the septum. The nasopalatine nerve then proceeds obliquely between the periosteum and mucous membrane of the lower septum to connect with the greater palatine nerve.[19]
Physiologic Variants
SPA anatomy has been studied extensively in numerous cadaveric investigations. Around 97% of these studies demonstrate at least 2 arterial branches at the plane of the sphenopalatine foramen. These branches correspond to the posterior lateral and septal arteries, as described previously. Although 2 to 4 SPA branches are most commonly observed, studies occasionally demonstrate up to 10 branches. After exiting the sphenopalatine foramen, distal and posterolateral branches demonstrate greater variability. Some segments of the artery may course anterior to the posterior maxillary wall.
The arrangement of arterial branches exhibits considerable variability, with distributions superior or inferior to the ethmoidal spine, crisscrossing upon exiting the foramen, and demonstrating asymmetry between nasal cavities within the same cadaver. The ethmoidal crest provides a consistent landmark for orientation within the nasal cavity, independent of variation in SPA branching patterns.[20]
Surgical Considerations
Sphenopalatine Artery Ligation
Surgical management of epistaxis is indicated for patients whose bleeding is refractory to conservative therapies. Detailed knowledge of vascular anatomy and adjacent landmarks is essential to prevent surgical failure and reduce the risk of postoperative hemorrhage.
SPA exposure may be achieved endoscopically by elevating a posterolateral mucosal flap over the orbital process of the palatine bone. A vertical incision is placed inferior to the posterior portion of the middle turbinate, approximately 1 cm anterior to its posterior tip. Elevation of the mucoperiosteal flap posteriorly and superiorly exposes the ethmoid crest, which serves as a reliable landmark for SPA localization and is consistently positioned anteromedial to the sphenopalatine foramen. Resection of the ethmoid crest improves visualization of the SPA and facilitates identification of its terminal branches.
During flap elevation and ethmoid crest resection, the fibro-neurovascular bundle containing the SPA and nasopalatine nerve becomes accessible at the sphenopalatine foramen. After isolation, the artery and its branches may be managed by bipolar cauterization, clip occlusion, or a combination of both. If distal bleeding persists, SPA tracing proximally through the sphenopalatine foramen into the pterygopalatine fossa permits ligation before terminal bifurcation.
Upon achieving hemostasis, the mucoperiosteal flap is repositioned and covered with an oxidized cellulose polymer hemostatic agent. Anatomical variations in SPA branching and the presence of multiple foramina can produce variable responses to SPA ligation.
Nasoseptal Flap
The nasoseptal flap represents a surgical technique for skull base reconstruction following anterior skull base tumor resection, transsphenoidal pituitary adenoma removal, and repair of sella and clival cerebrospinal fluid (CSF) leaks.[21] The flap functions as an effective barrier to prevent CSF leakage. The flap is pedicled on the posterior septal artery, a terminal branch of the SPA. A midseptum mucoperiosteal flap is incised inferiorly along the maxillary crest and dorsally beneath the olfactory epithelium. The posterior septal flap, pedicled on the posterior septal branch, is rotated around the pedicle into the defect. The septal branch–based blood supply ensures reliable revascularization and robust coverage for skull base reconstruction.[22]
Clinical Significance
Posterior Epistaxis
The SPA carries the largest volume of blood to the nasal cavity and serves as the source of most posteriorly based epistaxis. Posterior epistaxis accounts for approximately 10% of cases, with 80% of bleeding originating from SPA. This type of bleeding is most often associated with atherosclerotic disease, hypertension, and diabetes but may also occur from iatrogenic or idiopathic causes. Posterior hemorrhage may remain asymptomatic or present insidiously as hematemesis, anemia, or melena.
Additional clinical features of posterior epistaxis include blood in the oropharynx, recurrent episodes of epistaxis, failure to control bleeding with nasal packing, clots near the sphenopalatine foramen, clots in the maxillary sinus ostium, and absence of anterior septal bleeding. Management of posterior epistaxis is challenging due to the inaccessible location of the bleeding vessel.[23] The SPA is not readily visualized with anterior nasal speculum examination and is often identified only through nasal endoscopy.
Traditional management of posterior epistaxis includes anteroposterior nasal packing and balloon catheterization. Posterior nasal packing involves placement of a postnasal pack in the nasopharynx, occluding the posterior choana, combined with firm anterior nasal packing extending deeply into the nasal cavity. Hemostasis is achieved through direct pressure on the bleeding vessel. Nasal balloon catheters allow easier insertion, cause less discomfort, and provide targeted pressure at the point of maximal bleeding. This method reduces the compressive effect on the entire mucosal surface, thereby lowering the risk of mucosal ischemia. In cases of severe or refractory bleeding, direct cauterization, embolization, or ligation of the responsible vessel may be required.
Juvenile Nasopharyngeal Angiofibroma
Juvenile nasopharyngeal angiofibroma (JNA) is an uncommon benign tumor originating from the lateral nasal wall near the sphenopalatine foramen. The tumor predominantly affects adolescent boys and exhibits local aggressiveness, frequently invading surrounding structures and tissues. JNA typically presents with painless, progressive unilateral nasal obstruction, epistaxis, and rhinorrhea. The tumor receives a rich vascular supply, primarily from the SPA. Macroscopically, JNA appears as a rounded, circumscribed, nonencapsulated, mucosa-covered mass. Microscopically, the tumor demonstrates erratically arranged collagen and an irregular vascular pattern. Due to the extensive vascularization, embolization of the SPA followed by surgical resection yields a favorable prognosis when the tumor is diagnosed promptly.[24][25]
Media
(Click Image to Enlarge)
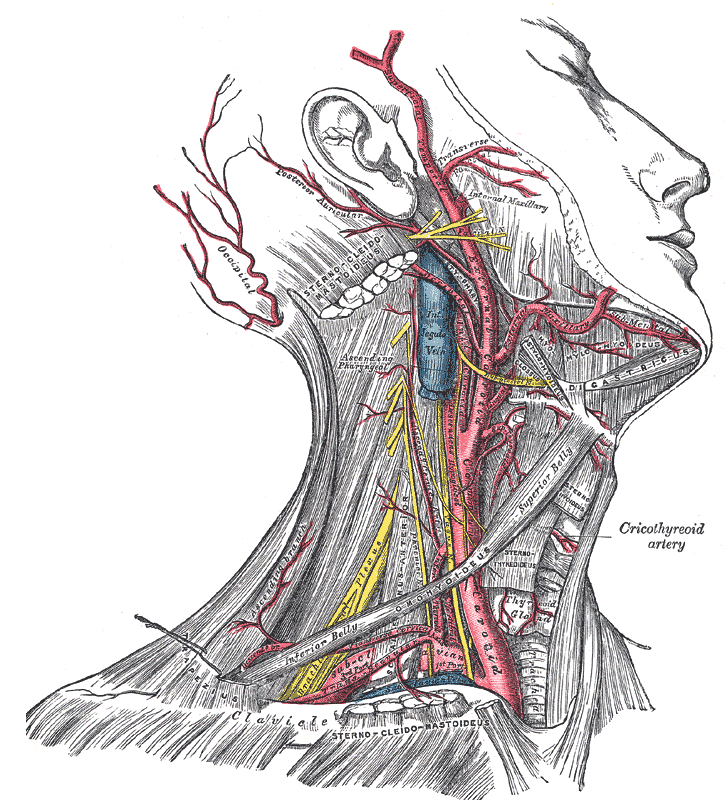
Arterial and Venous Anatomy of the Head and Neck. This illustration highlights the major vascular structures of the head and neck, including the external carotid artery, internal jugular vein, and maxillary artery. These vessels provide arterial perfusion to the facial and cranial regions and facilitate venous drainage to the heart.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
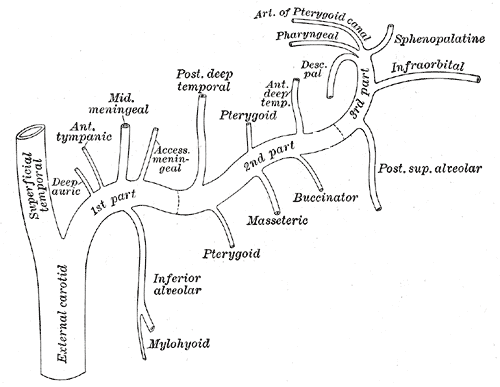
Plan of the Maxillary Artery Branches. The mandibular segment (proximal portion) of the maxillary artery gives rise to the middle meningeal and inferior alveolar arteries. The pterygoid segment (second portion) produces multiple branches, including the buccal artery, which supplies the buccinator musculomucosal flap. The pterygopalatine segment (terminal portion) traverses the pterygopalatine fossa, giving rise to the sphenopalatine, infraorbital, superior alveolar, and descending palatine arteries.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
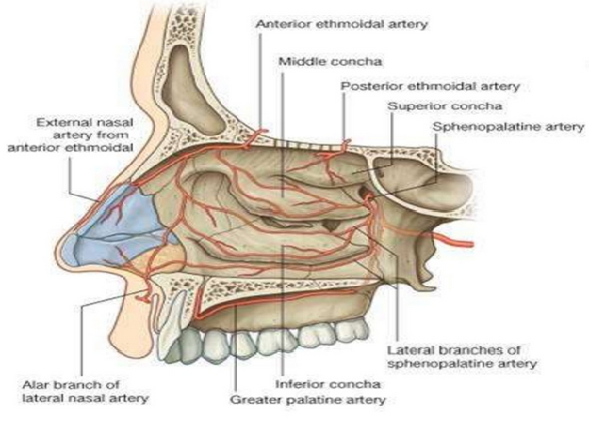
Nasal Cavity Blood Supply. This labeled diagram shows key arteries, including the anterior ethmoidal, middle posterior ethmoidal, superior sphenopalatine, sphenopalatine, external nasal, and greater palatine arteries, as well as the lateral branches of the anterior ethmoidal artery.
Used with permission from Greys Anatomy
(Click Image to Enlarge)
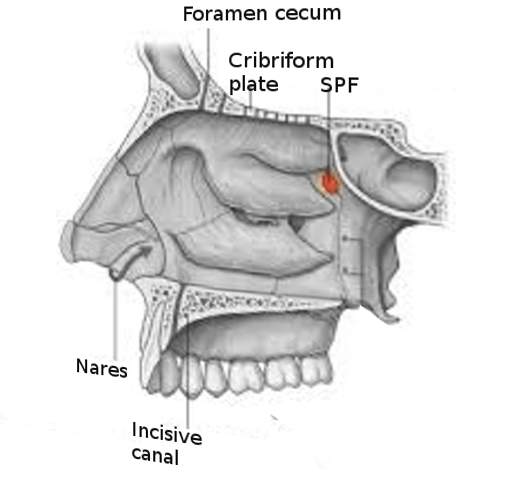
Sphenopalatine Foramen. This labeled sagittal view highlights the sphenopalatine foramen (SPF), cribriform plate, foramen cecum, nares, and incisive canal (plate).
Image courtesy S Bhimji MD
References
Dispenza F, Lorusso F, Di Vincenzo SA, Dolce A, Immordino A, Gallina S, Maniaci A, Lechien JR, Calvo-Henriquez C, Saibene AM, Sireci F. Management of uncontrolled/recurrent epistaxis by ligation or cauterization of the sphenopalatine artery: a scoping review. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2024 Dec:281(12):6229-6238. doi: 10.1007/s00405-024-08852-1. Epub 2024 Jul 28 [PubMed PMID: 39069575]
Level 2 (mid-level) evidenceSmall M, Murray JA, Maran AG. A study of patients with epistaxis requiring admission to hospital. Health bulletin. 1982 Jan:40(1):20-9 [PubMed PMID: 7061227]
Sireci F, Speciale R, Sorrentino R, Turri-Zanoni M, Nicolotti M, Canevari FR. Nasal packing in sphenopalatine artery bleeding: therapeutic or harmful? European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2017 Mar:274(3):1501-1505. doi: 10.1007/s00405-016-4381-y. Epub 2016 Nov 11 [PubMed PMID: 27837422]
Gras-Cabrerizo JR, Ademá-Alcover JM, Gras-Albert JR, Kolanczak K, Montserrat-Gili JR, Mirapeix-Lucas R, Del Campo FS, Massegur-Solench H. Anatomical and surgical study of the sphenopalatine artery branches. European archives of oto-rhino-laryngology : official journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2014 Jul:271(7):1947-51. doi: 10.1007/s00405-013-2825-1. Epub 2013 Nov 20 [PubMed PMID: 24253386]
Level 2 (mid-level) evidenceGras-Cabrerizo JR, García-Garrigós E, Montserrat-Gili JR, Gras-Albert JR, Mirapeix-Lucas R, Massegur-Solench H, Quer-Agusti M. Anatomical Correlation Between Nasal Vascularisation and the Design of the Endonasal Pedicle Flaps. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2018 Mar:70(1):167-173. doi: 10.1007/s12070-017-1197-z. Epub 2017 Sep 6 [PubMed PMID: 29456964]
Oz II, Aydogdu A, Yilmaz TF. Radiological evaluation of maxillary artery and descending palatine artery in the pterygopalatine fossa by 3D rotational angiography. Surgical and radiologic anatomy : SRA. 2022 Apr:44(4):535-542. doi: 10.1007/s00276-022-02916-9. Epub 2022 Mar 7 [PubMed PMID: 35254493]
Tanoue S, Kiyosue H, Mori H, Hori Y, Okahara M, Sagara Y. Maxillary artery: functional and imaging anatomy for safe and effective transcatheter treatment. Radiographics : a review publication of the Radiological Society of North America, Inc. 2013 Nov-Dec:33(7):e209-24. doi: 10.1148/rg.337125173. Epub [PubMed PMID: 24224604]
Silveira-Bertazzo G, Martinez-Perez R, Carrau RL, Prevedello DM. Surgical anatomy and nuances of the expanded transpterygoid approach to the pterygopalatine fossa and upper parapharyngeal space: a stepwise cadaveric dissection. Acta neurochirurgica. 2021 Feb:163(2):415-421. doi: 10.1007/s00701-020-04551-y. Epub 2020 Sep 4 [PubMed PMID: 32886225]
Manonmony S, Balakrishnan S, Renjit RE, Mohan A. Endoscopic Sphenopalatine Artery Cauterization in Refractory Hypertensive Epistaxis. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2022 Oct:74(Suppl 2):1298-1301. doi: 10.1007/s12070-021-02414-1. Epub 2021 Jan 30 [PubMed PMID: 36452784]
Rezende GL, Soares VY, Moraes WC, Oliveira CA, Nakanishi M. The sphenopalatine artery: a surgical challenge in epistaxis. Brazilian journal of otorhinolaryngology. 2012 Jul-Aug:78(4):42-7 [PubMed PMID: 22936135]
Eordogh M, Grimm A, Gawish I, Patonay L, Reisch R, Briner HR, Baksa G. Anatomy of the sphenopalatine artery and its implications for transnasal neurosurgery. Rhinology. 2018 Mar 1:56(1):82-88. doi: 10.4193/Rhin17.181. Epub [PubMed PMID: 29166425]
Lee HY, Kim HU, Kim SS, Son EJ, Kim JW, Cho NH, Kim KS, Lee JG, Chung IH, Yoon JH. Surgical anatomy of the sphenopalatine artery in lateral nasal wall. The Laryngoscope. 2002 Oct:112(10):1813-8 [PubMed PMID: 12368621]
Krulewitz NA, Fix ML. Epistaxis. Emergency medicine clinics of North America. 2019 Feb:37(1):29-39. doi: 10.1016/j.emc.2018.09.005. Epub [PubMed PMID: 30454778]
El-Shaarawy EAA, Hassan SS. The sphenopalatine foramen in man: anatomical, radiological and endoscopic study. Folia morphologica. 2018:77(2):345-355. doi: 10.5603/FM.a2017.0104. Epub 2017 Nov 13 [PubMed PMID: 29131280]
Gibelli D, Cellina M, Gibelli S, Cappella A, Panzeri MM, Oliva AG, Termine G, Dolci C, Sforza C. Anatomy of the pterygopalatine fossa: an innovative metrical assessment based on 3D segmentation on head CT-scan. Surgical and radiologic anatomy : SRA. 2019 May:41(5):523-528. doi: 10.1007/s00276-018-2153-7. Epub 2018 Dec 12 [PubMed PMID: 30542926]
Cappello ZJ, Arbor TC, Potts KL. Anatomy, Pterygopalatine Fossa. StatPearls. 2025 Jan:(): [PubMed PMID: 30020641]
Plzák J, Kratochvil V, Kešner A, Šurda P, Vlasák A, Zvěřina E. Endoscopic endonasal approach for mass resection of the pterygopalatine fossa. Clinics (Sao Paulo, Brazil). 2017 Oct:72(9):554-561. doi: 10.6061/clinics/2017(09)06. Epub [PubMed PMID: 29069259]
Konno A, Togawa K. Role of the vidian nerve in nasal allergy. The Annals of otology, rhinology, and laryngology. 1979 Mar-Apr:88(2 Pt 1):258-66 [PubMed PMID: 443720]
Fitzpatrick TH, Brizuela M, Downs BW. Anatomy, Head and Neck, Nasopalatine Nerve. StatPearls. 2025 Jan:(): [PubMed PMID: 30860693]
Simmen DB, Raghavan U, Briner HR, Manestar M, Groscurth P, Jones NS. The anatomy of the sphenopalatine artery for the endoscopic sinus surgeon. American journal of rhinology. 2006 Sep-Oct:20(5):502-5 [PubMed PMID: 17063746]
Barger J, Siow M, Kader M, Phillips K, Fatterpekar G, Kleinberg D, Zagzag D, Sen C, Golfinos JG, Lebowitz R, Placantonakis DG. The posterior nasoseptal flap: A novel technique for closure after endoscopic transsphenoidal resection of pituitary adenomas. Surgical neurology international. 2018:9():32. doi: 10.4103/sni.sni_192_17. Epub 2018 Feb 14 [PubMed PMID: 29527390]
Reuter G, Bouchain O, Demanez L, Scholtes F, Martin D. Skull base reconstruction with pedicled nasoseptal flap: Technique, indications, and limitations. Journal of cranio-maxillo-facial surgery : official publication of the European Association for Cranio-Maxillo-Facial Surgery. 2019 Jan:47(1):29-32. doi: 10.1016/j.jcms.2018.11.012. Epub 2018 Nov 16 [PubMed PMID: 30527383]
Iimura J, Hatano A, Ando Y, Arai C, Arai S, Shigeta Y, Kojima H, Otori N, Wada K. Study of hemostasis procedures for posterior epistaxis. Auris, nasus, larynx. 2016 Jun:43(3):298-303. doi: 10.1016/j.anl.2015.09.015. Epub 2015 Oct 31 [PubMed PMID: 26527519]
Bakshi SS, Bhattacharjee S. Juvenile Nasopharyngeal Angiofibroma. Journal of pediatric hematology/oncology. 2016 Aug:38(6):491-2. doi: 10.1097/MPH.0000000000000568. Epub [PubMed PMID: 27164528]
Makhasana JA, Kulkarni MA, Vaze S, Shroff AS. Juvenile nasopharyngeal angiofibroma. Journal of oral and maxillofacial pathology : JOMFP. 2016 May-Aug:20(2):330. doi: 10.4103/0973-029X.185908. Epub [PubMed PMID: 27601836]