 Anatomy, Bony Pelvis and Lower Limb: Leg Posterior Compartment
Anatomy, Bony Pelvis and Lower Limb: Leg Posterior Compartment
Introduction
The leg is divided into anterior, lateral, and posterior compartments by the anterior and posterior intermuscular septa, interosseous membrane, and crural fascia.[1] Each compartment contains distinct musculature, vasculature, and innervation (see Image. Transverse Section of the Leg). The posterior compartment (calf) is subdivided into superficial and deep layers by the transverse intermuscular septum. The superficial layer includes the gastrocnemius, soleus, and plantaris. The deep layer includes the popliteus, flexor digitorum longus (FDL), flexor hallucis longus (FHL), and tibialis posterior. These muscles arise primarily from the tibia and fibula. The tibia is the principal weight-bearing bone, whereas the fibula provides minimal weight-bearing support.[2][3] The anterior compartment primarily produces dorsiflexion. The lateral compartment primarily produces eversion and assists in plantarflexion. The posterior compartment primarily produces plantarflexion.
Pathologic processes involving the posterior leg compartment include compartment syndrome, musculotendinous injuries, venous insufficiency, nerve compression syndromes, and clinically significant anatomic variants capable of producing neurovascular compromise. Surgical management frequently requires precise compartmental decompression, tendon repair, fracture stabilization, or amputation techniques, all of which carry the risk of neurovascular injury without careful anatomic orientation. Detailed understanding of compartmental organization, muscle function, and neurovascular relationships supports accurate diagnosis, timely intervention, and avoidance of iatrogenic complications, thereby improving functional outcomes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The leg compartments are defined by intermuscular septa that arise as direct extensions of the overlying deep fascia. Within the posterior compartment, an additional transverse septum further subdivides the space into superficial and deep layers. Earlier descriptions characterized fascia surrounding specialized organs and tissues as serving only a passive containment role.[4] Modern literature attributes several structural, physiological, and protective functions to fascia, including that of the posterior leg compartment: creation of osteofascial boundaries for enclosed musculature, formation of protective tunnels for neurovascular bundles across a range of limb positions, facilitation of venous return, provision of a protective sheath for underlying structures, resistance and dissipation of external compressive forces, and clinical relevance in the spread or containment of infections.[5]
The 3 muscles of the superficial posterior compartment are the gastrocnemius, soleus, and plantaris. The gastrocnemius contributes to ankle plantarflexion when the knee is in extension and additionally assists in knee flexion. In contrast, the soleus plantarflexes the ankle independently of knee position. The plantaris, a vestigial muscle thought to be absent in approximately 10% of the population, also contributes to plantarflexion, though to a far lesser degree than the gastrocnemius and soleus.
The deep posterior compartment contains 4 muscles: the FHL, FDL, tibialis posterior, and popliteus. The FHL primarily flexes the hallux (big toe) while also assisting in ankle plantarflexion and providing dynamic support to the medial longitudinal arch (MLA) of the foot. The FDL flexes the lateral 4 toes, contributes to ankle plantarflexion, and helps maintain both the MLA and lateral longitudinal arch of the foot. The tibialis posterior contributes to ankle plantarflexion and serves as both the principal inverter of the midfoot and the primary stabilizer of the MLA. During the gait cycle, the tibialis posterior maintains arch integrity, controls midfoot pronation during midstance, and locks the transverse tarsal joint at push-off, converting the midfoot into a rigid lever that facilitates efficient force transmission through the gastrocnemius-soleus complex.[6][7]
In contrast to the other deep posterior muscles, the popliteus acts exclusively at the knee, where the muscle unlocks the extended joint by internally rotating the tibia on the femur when the limb is non-weight-bearing or by laterally rotating the femur on the tibia during weight-bearing, thereby initiating knee flexion.[8][9][10] Coordinated activation of the 7 posterior compartment muscles is crucial for maintaining balance, facilitating gait, and performing functional tasks, such as stair climbing, jumping, and landing.
Gait is conventionally subdivided into stance and swing phases, though additional phases may be defined, depending on the clinical context.[11] The stance phase is further divided into heel strike (initial ground contact), loading response (acceptance of body weight), midstance (knee stabilization), and terminal stance (forward acceleration of body mass). The ankle plantarflexors play a pivotal biomechanical role during midstance and terminal stance by eccentrically controlling dorsiflexion and concentrically propelling the foot forward.[12]
Embryology
Limb development in the human embryo originates from mesenchymal tissue derived from the lateral plate mesoderm, encased within ectoderm.[13] Limb buds emerge during the 4th week of gestation, initiated primarily by fibroblast growth factor (FGF10) signaling from the mesoderm, which induces formation of the apical ectodermal ridge.[14] The morphogenesis of limb buds depends on multiple transcription factors, with each limb bud acquiring positional value along the proximodistal, anteroposterior, and dorsoventral axes of the developing fetus.[15] Key signaling pathways, including fibroblast growth factors, sonic hedgehog, retinoic acid, and homeobox gene clusters, contribute to proximal–distal limb patterning and segmental identity.[16]
In addition to biochemical signaling, mechanical forces and cell–cell interactions contribute significantly to limb bud morphogenesis. Mechanisms include directed cell migration, oriented cell division, and convergent extension movements, all contributing to limb bud outgrowth and elongation. Subsequent aggregation of mesenchymal cells forms precursors to cartilage and bone.[17][18][19][20]
Blood Supply and Lymphatics
The posterior compartment of the leg receives arterial supply from the posterior tibial artery.[21] The posterior tibial artery is a direct continuation of the popliteal artery, which arises from the femoral artery. The posterior tibial artery supplies the posterior compartment through muscular branches and gives rise to the nutrient artery of the tibia. The fibular artery arises from the posterior tibial artery and provides muscular branches to specific posterior compartment muscles, while also giving rise to the nutrient artery of the fibula.[22] Distally, the division of the posterior tibial artery into the medial and lateral plantar arteries occurs at the level of the foot. Throughout its course, the posterior tibial artery runs deep to the triceps surae alongside the tibial nerve.
Lymphatic drainage of the posterior compartment follows the deep vascular network, with lymphatic vessels accompanying the posterior tibial and fibular arteries. Drainage ultimately occurs into the popliteal lymph nodes and subsequently into the deep inguinal lymph nodes. Superficial lymphatics of the posterior leg primarily drain into vessels associated with the small saphenous vein. Drainage from these superficial channels also reaches the popliteal lymph nodes before continuing proximally.
Nerves
The tibial nerve provides motor and sensory fibers to the entire posterior leg compartment.[23] The tibial nerve is the larger of the 2 terminal branches of the sciatic nerve, which divides into the tibial and common fibular (peroneal) nerves at or near the apex of the popliteal fossa. Muscular branches of the tibial nerve supply both the superficial and deep posterior compartments, including the popliteus. The tibial nerve descends with the posterior tibial vessels through the deep posterior compartment along the tibialis posterior. Sympathetic (vasomotor) fibers accompany the posterior tibial artery, reflecting the close functional relationship between neural and vascular structures of the posterior compartment.[24] Division of the tibial nerve into the medial and lateral plantar nerves occurs posterior to the medial malleolus. The tibial nerve also gives rise to the medial sural cutaneous nerve, which joins the sural communicating branch of the common fibular nerve to form the sural nerve. The sural nerve provides cutaneous innervation to the lateral and posterior distal leg and the lateral foot.
Muscles
Superficial Posterior Muscles
The gastrocnemius comprises distinct medial and lateral heads.[25] The medial head, the larger of the two, originates from the medial femoral condyle, while the lateral head originates from the lateral femoral condyle. The gastrocnemius overlies the soleus. Both muscles converge to form the calcaneal (Achilles) tendon, which inserts into the posterior tuberosity of the calcaneus. A subcutaneous bursa lies between the Achilles tendon and the overlying superficial fascia, permitting frictionless movement of the skin over the tendon. A deeper retrocalcaneal bursa lies between the Achilles tendon and the superior aspect of the calcaneal tuberosity, facilitating frictionless gliding of the tendon over bone. The soleus originates from the posterior surface of the fibular head, the proximal fibular shaft, and the soleal line of the posterior tibia. Collectively, the gastrocnemius and soleus are referred to as the "triceps surae."
The plantaris lies within the superficial posterior compartment between the gastrocnemius and soleus. The plantaris originates from the lateral supracondylar line of the femur and inserts adjacent to the Achilles tendon onto the tuberosity of the calcaneus. The plantaris is commonly used as a source of grafting material. The muscle provides only a minor contribution to plantarflexion.
Deep Posterior Muscles
The most proximal muscle of the deep posterior compartment is the popliteus.[26] This muscle originates from the lateral condyle of the femur and inserts onto the posterior tibial surface superior to the origin of the soleus. The functional activity of the popliteus is associated with the knee joint. The popliteus is responsible for “unlocking” the fully extended knee joint through internal rotation of the tibia.[27]
The FHL originates from the posterior surface of the distal 2/3 of the fibula and inserts into the base of the distal phalanx of the hallux. The FHL tendon courses beneath the sustentaculum tali and is stabilized at the ankle by the flexor retinaculum. The FHL plantarflexes the talocrural joint and also flexes the metatarsophalangeal and interphalangeal joints of the great toe.
The FDL originates from the posterior surface of the middle 1/3 of the tibia and inserts onto the distal phalanges of the 2nd through 5th digits. The FDL flexes the metatarsophalangeal and interphalangeal joints of the lateral 4 toes and assists in plantarflexion of the ankle. An accessory FDL muscle has been reported in approximately 15% of the population.[28]
The tibialis posterior originates from the posterior surface of the interosseous membrane and inserts primarily onto the navicular tuberosity and cuneiform bones of the foot. The tibialis posterior tendon courses through the tarsal tunnel posterior to the medial malleolus. The tibialis posterior contributes to plantarflexion across the talocrural joint, inversion of the subtalar joint, and maintenance of the MLA.
Surgical Considerations
Compartment Syndrome
Compartment syndrome develops when the pressure within a closed osteofascial compartment, such as the leg, exceeds the perfusion pressure of the surrounding tissue, resulting in tissue ischemia, neurovascular compression, and pain that is characteristically disproportionate to the apparent injury on examination.[29] The condition is broadly classified as acute or chronic: acute compartment syndrome (ACS) is most frequently precipitated by trauma, whereas chronic exertional compartment syndrome arises in the context of repetitive athletic activity.
ACS most commonly presents following high-energy blunt trauma, such as motor vehicle collisions. Young patients sustaining tibial diaphyseal fractures are at particularly elevated risk and require close monitoring.[30] Open tibial fractures have been identified as an independent risk factor for ACS, with a notably higher incidence compared with closed injuries. The highest rates have been observed in Gustilo-Anderson type IIIA and IIIB injuries, emphasizing the need for heightened vigilance in this subset of patients.[31]
The posterior compartment of the leg is further subdivided into superficial and deep compartments. The deep posterior compartment is particularly prone to delayed diagnosis due to its deep location and nonspecific presentation, making a high index of suspicion essential in patients with exertional calf pain.[32] The superficial posterior compartment is less commonly involved and contains the gastrocnemius and soleus, with a higher incidence in athletic injuries.
Four-Compartment Fasciotomy
For ACS, the standard of care involves emergent fasciotomy of all 4 leg compartments. The procedure carries a risk of complications, including neurovascular injury and soft tissue injury.
Pediatric Conditions Involving the Posterior Leg Compartment
Tibial fractures are among the most common fractures in the pediatric population.[33] Delayed diagnosis of these injuries, particularly those resulting from high-energy trauma, may lead to collateral vascular damage, neurovascular compromise, and development of ACS.[34] Management typically consists of closed reduction and casting. However, surgical approaches, including external fixation, intramedullary nailing, and open reduction with internal fixation using plates and screws, may be warranted in select cases.
Indications for lower extremity amputation include limb-threatening ischemia from arterial occlusion, distal extremity infection, and malignant neoplasms.[35][36] Below-knee amputation is performed using several described techniques, with the posterior myocutaneous flap approach most commonly employed. Postoperative infection rates are influenced by multiple operative factors, including the method of skin closure (skin clips versus sutures) and the use of suction drains among potential complications.[37]
Achilles Tendon Rupture
The Achilles tendon is the thickest tendon in the body and among the strongest, yet it remains susceptible to injury, degenerative change, and acute rupture. Achilles tendon ruptures most commonly occur in athletes engaged in sprinting and jumping activities. A similar predisposition has been described in recreational athletes, or “weekend warriors,” in whom acute overload of an already compromised and weakened tendon may result in rupture even with mild exertion. Degenerative Achilles tendinopathy develops gradually and manifests clinically as recurrent pain and swelling at or proximal to the tendon insertion.[38]
Conservative management of tendinopathy includes rest and activity modification, intake of nonsteroidal anti-inflammatory drugs, and physical therapy (eg, eccentric exercises).[39] While tendinopathy is generally managed nonoperatively, acute Achilles tendon ruptures may require surgical intervention. Direct end-to-end repair, performed through either open or percutaneous approaches, is commonly employed for tears near the musculotendinous junction and is most amenable to primary healing within 6 weeks of injury. Comparative outcomes of operative versus nonoperative management (ie, functional bracing and rehabilitation protocols) remain an area of ongoing debate in the current literature.
Gastrocnemius Tears
Gastrocnemius tears represent a common injury, particularly in patients older than 40 years, and are colloquially termed “tennis leg” due to high prevalence in racquet sports. The condition typically presents with acute posterior leg pain, a palpable defect in the gastrocnemius belly, diminished plantarflexion strength, and restricted ankle range of motion. The medial head of the gastrocnemius is most commonly affected, although injuries involving the plantaris or soleus tendons may present with a similar clinical picture. Diagnosis is usually established clinically, although ultrasonography may assist in characterizing the extent of injury and excluding alternative pathology. Conservative treatment includes activity restriction, crutch-assisted ambulation, rest, ice application, compression, and elevation. Surgical intervention or additional medical management may be required in cases of significant hematoma formation or development of ACS.[40]
Clinical Significance
Accessory muscles of the posterior leg compartment comprise anatomical variants of clinical importance. Reported accessory muscles include additional muscular tissue connecting the FHL to the tibialis posterior, which, in some cases, crosses the posterior tibial artery and may serve as a source of vascular entrapment. Other accessory muscles have been described arising from the interosseous membrane near the tibia and inserting into the connective tissue surrounding the posterior tibial vessels, with potential to cause vascular compression.[41]
Aside from anatomical compression, iatrogenic injury to neurovascular structures may occur during surgical procedures. Fibular graft harvests, tibial osteotomies, and fasciotomies carry an increased risk of tibial nerve injury. Knowledge of tibial nerve branching patterns into specific muscles of the posterior leg is essential to avoid such injuries and subsequent motor loss.[42] Distally, the tibial nerve is susceptible to compression as it traverses the tarsal tunnel alongside the tendons of the tibialis posterior, FDL, and FHL. Compression at this site produces tarsal tunnel syndrome, which may manifest as pain, paresthesia, and weakness in the distribution of the medial and lateral plantar nerves.[43]
Focal myositis is a rare inflammatory pseudotumor that may present within the posterior leg compartment. Diagnosis is challenging, as the lesion may be misinterpreted as other neoplastic processes or inflammatory myopathies. Specific histopathological findings include B-cell and dendritic plasmacytoid cell lesions in the absence of viral or infectious etiology. The presence of immunoglobulin G4 (IgG4) and fibrosis has also been associated with focal myositis.[44][45]
Physiologically, surface venous pressure in the leg decreases during ambulation. This decrease occurs due to the contraction of the posterior leg compartment muscles, which compress deep veins and facilitate venous return. Relaxation of these muscles allows refilling of the deep venous system via perforator veins from the superficial venous system. Venous abnormalities may impair this mechanism, resulting in inadequate reduction of surface venous pressure and ambulatory venous hypertension. Such insufficiency arises from venous destruction, incompetence, or embolization, leading to reflux and persistent elevation of venous pressure. Chronic venous hypertension contributes to hyperpigmentation, fibrosis, and ulceration of the lower limb. Impaired tissue nutrition and oxygenation are proposed mechanisms underlying cellular dysfunction in this context. Treatment of chronic venous insufficiency ranges from compression therapy to sclerotherapy or radiofrequency ablation.[46]
Restless leg syndrome (RLS) is characterized by spontaneous nocturnal leg movements and has a prevalence of approximately 5% to 10% in older individuals.[47] Sensorimotor activation of the lower limbs occurs at rest, most commonly at night, leading to significant sleep disturbance.[48] The condition most commonly involves the calf muscles. The genetic basis and pathophysiology are incompletely understood. Iron deficiency has been associated with an increased risk of RLS.[49] Management typically involves dopamine agonist therapy.
Leg cramps are characterized by involuntary, episodic skeletal muscle contractions of the calf muscles, with associated pain and nocturnal occurrence.[50] The etiology is incompletely understood, although links exist with electrolyte imbalances, renal disease, polyneuropathies, myopathies, and administration of certain medications. Additional associations include trauma and deep venous thrombosis.[51] Approximately 1/3 of the population older than 50 years is affected by nocturnal leg cramps, with incidence increasing with age. Similar to RLS, leg cramps may result in sleep disturbance and subsequent sequelae. Quinine was historically used for the management of nocturnal leg cramps but has fallen out of favor following a warning issued by the US Food and Drug Administration regarding potentially serious adverse effects.[52]
Media
(Click Image to Enlarge)
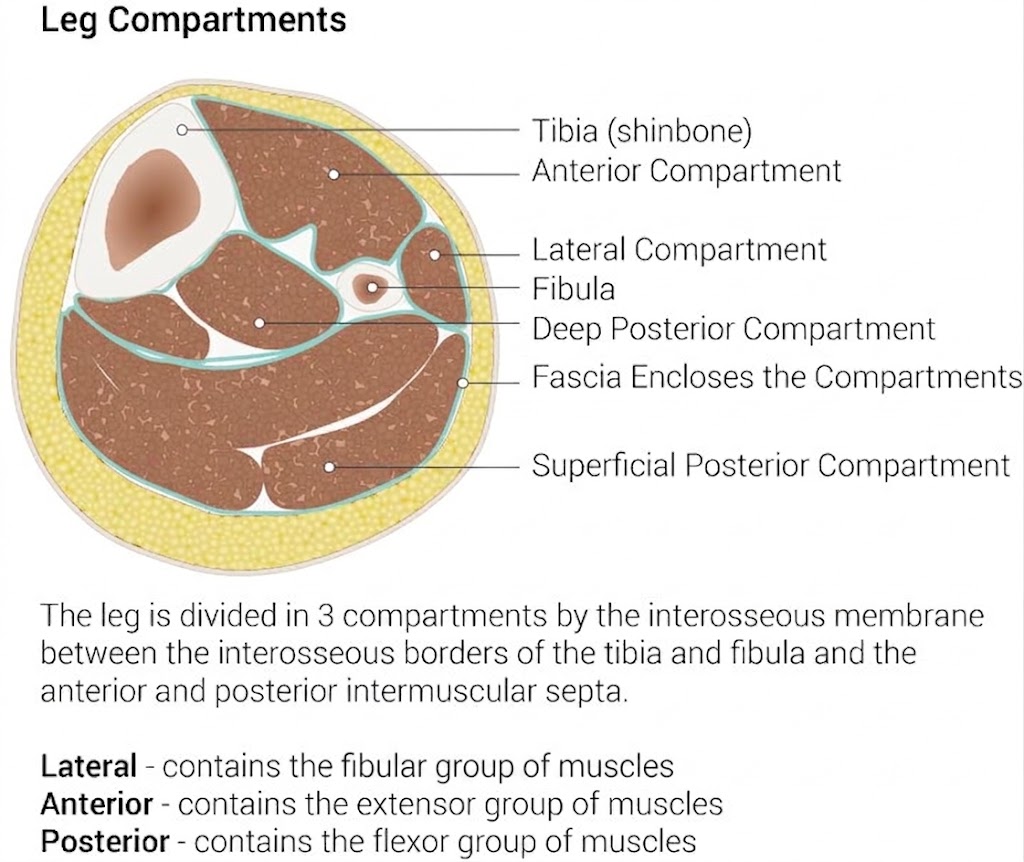
Transverse Section of the Leg. The illustration depicts the fascial boundaries that separate the leg into anterior, lateral, and posterior functional groups. Each compartment is defined by its relationship to the tibia and fibula, housing specific neurovascular bundles and synergistic muscle sets.
Illustrated by B Palmer
References
Binstead JT, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Calf. StatPearls. 2026 Jan:(): [PubMed PMID: 29083629]
Bourne M, Sinkler MA, Murphy PB. Anatomy, Bony Pelvis and Lower Limb: Tibia. StatPearls. 2026 Jan:(): [PubMed PMID: 30252309]
Gupton M, Munjal A, Kang M. Anatomy, Bony Pelvis and Lower Limb: Fibula. StatPearls. 2026 Jan:(): [PubMed PMID: 29261984]
Bordoni B, Mahabadi N, Jozsa F. Anatomy, Fascia. StatPearls. 2026 Jan:(): [PubMed PMID: 29630284]
Benjamin M. The fascia of the limbs and back--a review. Journal of anatomy. 2009 Jan:214(1):1-18. doi: 10.1111/j.1469-7580.2008.01011.x. Epub [PubMed PMID: 19166469]
Level 3 (low-level) evidenceDeu RS, Coslick AM, Dreher G. Tendinopathies of the Foot and Ankle. American family physician. 2022 May 1:105(5):479-486 [PubMed PMID: 35559641]
Knapp PW, Constant D. Posterior Tibial Tendon Dysfunction(Archived). StatPearls. 2026 Jan:(): [PubMed PMID: 31194317]
Yagi M, Tateuchi H, Kuriu M, Ichihashi N. The function of the popliteus muscle: An in vivo ultrasound shear wave elastography study. Human movement science. 2021 Apr:76():102751. doi: 10.1016/j.humov.2020.102751. Epub 2021 Jan 21 [PubMed PMID: 33486378]
Hyland S, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Popliteus Muscle. StatPearls. 2026 Jan:(): [PubMed PMID: 30252340]
Olewnik Ł, Landfald IC, Gonera B, Triantafyllou G, Domosławska D, Piagkou M, LaPrade RF. Popliteus Tendon Morphology: Anatomical Classification and Clinical Implications-A Narrative Review. Biomedicines. 2025 Aug 22:13(9):. doi: 10.3390/biomedicines13092053. Epub 2025 Aug 22 [PubMed PMID: 41007617]
Level 3 (low-level) evidenceTaborri J, Palermo E, Rossi S, Cappa P. Gait Partitioning Methods: A Systematic Review. Sensors (Basel, Switzerland). 2016 Jan 6:16(1):. doi: 10.3390/s16010066. Epub 2016 Jan 6 [PubMed PMID: 26751449]
Level 1 (high-level) evidenceTao W, Liu T, Zheng R, Feng H. Gait analysis using wearable sensors. Sensors (Basel, Switzerland). 2012:12(2):2255-83. doi: 10.3390/s120202255. Epub 2012 Feb 16 [PubMed PMID: 22438763]
Tickle C. How the embryo makes a limb: determination, polarity and identity. Journal of anatomy. 2015 Oct:227(4):418-30. doi: 10.1111/joa.12361. Epub 2015 Aug 7 [PubMed PMID: 26249743]
Jiang M, Fu X, Yang H, Long F, Chen J. mTORC1 Signaling Promotes Limb Bud Cell Growth and Chondrogenesis. Journal of cellular biochemistry. 2017 Apr:118(4):748-753. doi: 10.1002/jcb.25728. Epub 2016 Dec 29 [PubMed PMID: 27606668]
Wolpert L. Vertebrate limb development and malformations. Pediatric research. 1999 Sep:46(3):247-54 [PubMed PMID: 10473037]
Level 3 (low-level) evidenceCunningham TJ, Duester G. Mechanisms of retinoic acid signalling and its roles in organ and limb development. Nature reviews. Molecular cell biology. 2015 Feb:16(2):110-23. doi: 10.1038/nrm3932. Epub 2015 Jan 5 [PubMed PMID: 25560970]
Level 3 (low-level) evidenceSermeus Y, Vangheel J, Geris L, Smeets B, Tylzanowski P. Mechanical Regulation of Limb Bud Formation. Cells. 2022 Jan 26:11(3):. doi: 10.3390/cells11030420. Epub 2022 Jan 26 [PubMed PMID: 35159230]
Rolfe RA, Shea CA, Murphy P. Geometric analysis of chondrogenic self-organisation of embryonic limb bud cells in micromass culture. Cell and tissue research. 2022 Apr:388(1):49-62. doi: 10.1007/s00441-021-03564-y. Epub 2022 Jan 6 [PubMed PMID: 34988666]
Matsushita Y, Manabe H, Ohyama T, Nakamura S, Nagata M, Ono W, Ono N. Hes1 marks peri-condensation mesenchymal cells that generate both chondrocytes and perichondrial cells in early bone development. The Journal of biological chemistry. 2023 Jun:299(6):104805. doi: 10.1016/j.jbc.2023.104805. Epub 2023 May 11 [PubMed PMID: 37172728]
Sutherland A, Keller R, Lesko A. Convergent extension in mammalian morphogenesis. Seminars in cell & developmental biology. 2020 Apr:100():199-211. doi: 10.1016/j.semcdb.2019.11.002. Epub 2019 Nov 13 [PubMed PMID: 31734039]
Chmielewski P, Warchoł Ł, Gala-Błądzińska A, Mróz I, Walocha J, Malczak M, Jaworek J, Mizia E, Walocha E, Depukat P, Bachul P, Bereza T, Kurzydło W, Gach-Kuniewicz B, Mazur M, Tomaszewski K. Blood vessels of the shin - posterior tibial artery - anatomy - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(3):5-9 [PubMed PMID: 28275266]
Tanaka K, Matsumura H, Miyaki T, Watanabe K. An anatomic study of the intermuscular septum of the lower leg; branches from the posterior tibial artery and potential for reconstruction of the lower leg and the heel. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2006:59(8):835-8 [PubMed PMID: 16876081]
Vloka JD, Hadzić A, April E, Thys DM. The division of the sciatic nerve in the popliteal fossa: anatomical implications for popliteal nerve blockade. Anesthesia and analgesia. 2001 Jan:92(1):215-7 [PubMed PMID: 11133630]
Lin R, Zhang G, Gan KY, Zhuang YH, Pan RM, Zou LB, Xie Y, Zhao XZ. An anatomical study of the tibial nerve branches innervating the posterior tibial artery. Clinical anatomy (New York, N.Y.). 2023 Sep:36(6):875-880. doi: 10.1002/ca.23997. Epub 2022 Dec 26 [PubMed PMID: 36527146]
Bordoni B, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Gastrocnemius Muscle. StatPearls. 2026 Jan:(): [PubMed PMID: 30422541]
Nyland J, Lachman N, Kocabey Y, Brosky J, Altun R, Caborn D. Anatomy, function, and rehabilitation of the popliteus musculotendinous complex. The Journal of orthopaedic and sports physical therapy. 2005 Mar:35(3):165-79 [PubMed PMID: 15839310]
Hyland S, Sinkler MA, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Popliteal Region. StatPearls. 2026 Jan:(): [PubMed PMID: 30422486]
Holzmann M, Almudallal N, Rohlck K, Singh R, Lee S, Fredieu J. Identification of a flexor digitorum accessorius longus muscle with unique distal attachments. Foot (Edinburgh, Scotland). 2009 Dec:19(4):224-6. doi: 10.1016/j.foot.2009.03.002. Epub 2009 Jun 13 [PubMed PMID: 20307482]
Varacallo M, Shirey L, Kavuri V, Harding S. Acute compartment syndrome of the hand secondary to propofol extravasation. Journal of clinical anesthesia. 2018 Jun:47():1-2. doi: 10.1016/j.jclinane.2018.01.020. Epub 2018 Feb 21 [PubMed PMID: 29476968]
Park S, Ahn J, Gee AO, Kuntz AF, Esterhai JL. Compartment syndrome in tibial fractures. Journal of orthopaedic trauma. 2009 Aug:23(7):514-8. doi: 10.1097/BOT.0b013e3181a2815a. Epub [PubMed PMID: 19633461]
Level 2 (mid-level) evidenceGamulin A, Wuarin L, Zingg M, Belinga P, Cunningham G, Gonzalez AI. Association between open tibia fractures and acute compartment syndrome: A retrospective cohort study. Orthopaedics & traumatology, surgery & research : OTSR. 2022 Sep:108(5):103188. doi: 10.1016/j.otsr.2021.103188. Epub 2021 Dec 17 [PubMed PMID: 34929394]
Level 2 (mid-level) evidenceMicicoi L, Gonzalez JF, Gauci MO, Chabrand P, Machado A, Bronsard N, Micicoi G. Acute compartment syndrome of the lower limbs: Fasciotomy or dermofasciotomy? A cadaver study of compartment pressures. Orthopaedics & traumatology, surgery & research : OTSR. 2024 Feb:110(1):103736. doi: 10.1016/j.otsr.2023.103736. Epub 2023 Oct 27 [PubMed PMID: 37890523]
Mashru RP, Herman MJ, Pizzutillo PD. Tibial shaft fractures in children and adolescents. The Journal of the American Academy of Orthopaedic Surgeons. 2005 Sep:13(5):345-52 [PubMed PMID: 16148360]
Wozasek GE, Moser KD, Haller H, Capousek M. Trauma involving the proximal tibial epiphysis. Archives of orthopaedic and trauma surgery. 1991:110(6):301-6 [PubMed PMID: 1747311]
Desai Y, Robbs JV, Keenan JP. Staged below-knee amputations for septic peripheral lesions due to ischaemia. The British journal of surgery. 1986 May:73(5):392-4 [PubMed PMID: 3708295]
McIntyre KE Jr, Bailey SA, Malone JM, Goldstone J. Guillotine amputation in the treatment of nonsalvageable lower-extremity infections. Archives of surgery (Chicago, Ill. : 1960). 1984 Apr:119(4):450-3 [PubMed PMID: 6703902]
Coulston JE, Tuff V, Twine CP, Chester JF, Eyers PS, Stewart AH. Surgical factors in the prevention of infection following major lower limb amputation. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery. 2012 May:43(5):556-60. doi: 10.1016/j.ejvs.2012.01.029. Epub 2012 Feb 18 [PubMed PMID: 22342693]
Cohen D, Sandman E, Saran N, Petrisor B, Bhandari M, Veljkovic A, Leucht A, Downey EA, Martineau P. Evidence-based treatment of Achilles tendon rupture. Canadian journal of surgery. Journal canadien de chirurgie. 2023 Jul-Aug:66(4):E356-E357. doi: 10.1503/cjs.008321. Epub 2023 Jul 4 [PubMed PMID: 37402560]
Shamrock AG, Dreyer MA, Varacallo MA. Achilles Tendon Rupture. StatPearls. 2026 Jan:(): [PubMed PMID: 28613594]
Nsitem V. Diagnosis and rehabilitation of gastrocnemius muscle tear: a case report. The Journal of the Canadian Chiropractic Association. 2013 Dec:57(4):327-33 [PubMed PMID: 24302780]
Level 3 (low-level) evidenceNayak SB, Shetty SD. Two accessory muscles of leg: potential source of entrapment of posterior tibial vessels. Surgical and radiologic anatomy : SRA. 2019 Jan:41(1):97-99. doi: 10.1007/s00276-018-2115-0. Epub 2018 Oct 23 [PubMed PMID: 30353417]
Apaydin N, Loukas M, Kendir S, Tubbs RS, Jordan R, Tekdemir I, Elhan A. The precise localization of distal motor branches of the tibial nerve in the deep posterior compartment of the leg. Surgical and radiologic anatomy : SRA. 2008 Jun:30(4):291-5. doi: 10.1007/s00276-008-0321-x. Epub 2008 Feb 19 [PubMed PMID: 18283390]
Level 3 (low-level) evidenceSha I I. Tarsal Tunnel Syndrome - A Comprehensive Review. The Iowa orthopaedic journal. 2024:44(2):32-36 [PubMed PMID: 39811161]
Auerbach A, Fanburg-Smith JC, Wang G, Rushing EJ. Focal myositis: a clinicopathologic study of 115 cases of an intramuscular mass-like reactive process. The American journal of surgical pathology. 2009 Jul:33(7):1016-24. doi: 10.1097/PAS.0b013e31819e63fe. Epub [PubMed PMID: 19363438]
Level 3 (low-level) evidenceBordoni B, Sugumar K, Dua A. Myofascial Pain. StatPearls. 2026 Jan:(): [PubMed PMID: 30570965]
Fitridge R, Thompson M, Stacey M. Chronic Venous Insufficiency and Leg Ulceration: Principles and Vascular Biology. Mechanisms of Vascular Disease: A Reference Book for Vascular Specialists. 2011:(): [PubMed PMID: 30485035]
Trenkwalder C, Wetter TC, Stiasny K, Clarenbach P. [Restless legs syndrome and periodic limb movements in sleep]. Der Nervenarzt. 2001 Jun:72(6):425-36 [PubMed PMID: 11433701]
Stiasny K, Oertel WH, Trenkwalder C. Clinical symptomatology and treatment of restless legs syndrome and periodic limb movement disorder. Sleep medicine reviews. 2002 Aug:6(4):253-65 [PubMed PMID: 12531131]
Yeh P, Walters AS, Tsuang JW. Restless legs syndrome: a comprehensive overview on its epidemiology, risk factors, and treatment. Sleep & breathing = Schlaf & Atmung. 2012 Dec:16(4):987-1007. doi: 10.1007/s11325-011-0606-x. Epub 2011 Oct 26 [PubMed PMID: 22038683]
Level 2 (mid-level) evidenceHallegraeff J, de Greef M, Krijnen W, van der Schans C. Criteria in diagnosing nocturnal leg cramps: a systematic review. BMC family practice. 2017 Feb 28:18(1):29. doi: 10.1186/s12875-017-0600-x. Epub 2017 Feb 28 [PubMed PMID: 28241802]
Level 1 (high-level) evidenceYoung G. Leg cramps. BMJ clinical evidence. 2009 Mar 26:2009():. pii: 1113. Epub 2009 Mar 26 [PubMed PMID: 19445755]
Level 1 (high-level) evidenceDiener HC, Dethlefsen U, Dethlefsen-Gruber S, Verbeek P. Effectiveness of quinine in treating muscle cramps: a double-blind, placebo-controlled, parallel-group, multicentre trial. International journal of clinical practice. 2002 May:56(4):243-6 [PubMed PMID: 12074203]
Level 1 (high-level) evidence