Introduction
The subclavian vein is a deep vein and the major venous channel draining the upper extremity (see Image. Vascular Structures of the Anterior Neck). Other deep veins of the upper limb that accompany the major arteries include the radial, ulnar, brachial, and axillary veins. The subclavian vein is a paired vessel, consisting of right and left subclavian veins, each arising as a continuation of the axillary vein at the lateral border of the 1st rib and arching posterior to the clavicle. The subclavian artery lies posterior and superior to the subclavian vein, separated by the anterior scalene muscle. The subclavian vein continues medially toward the sternoclavicular region, where it joins the internal jugular vein (IJV) posterior to the sternoclavicular joint to form the brachiocephalic vein, which then drains into the superior vena cava (SVC) and ultimately the right atrium.
Subclavian vein pathology is clinically significant due to its association with stenosis, catheter-related thrombosis, and upper extremity deep vein thrombosis (DVT), which may present with extremity swelling, pain, venous congestion, or pulmonary embolism. The subclavian vein is surgically important as a common site for central venous catheter (CVC) insertion via infraclavicular and supraclavicular approaches, procedures that carry risks of pneumothorax, arterial injury, hemothorax, and malposition due to proximity to the subclavian artery, pleura, and brachial plexus. Detailed knowledge of subclavian venous anatomy and its relationships to surrounding neurovascular and musculoskeletal structures improves procedural safety, enhances diagnostic accuracy in thoracic outlet–related disorders, and reduces complication rates during central venous access and vascular interventions.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The subclavian veins are valveless, and the anatomical course of the right and left subclavian veins is not symmetrical. The right subclavian vein forms an angled arc during its junction with the right IJV, forming the right brachiocephalic vein, which enters the SVC. The left subclavian vein lies posterior to the clavicle after crossing the 1st rib, representing the only region in which the subclavian vein is directly related to the clavicle. Both subclavian veins terminate by joining the IJVs to form the brachiocephalic veins. The angle of confluence is termed the venous angle. The right venous angle receives the right lymphatic duct, which drains lymph from the right upper quadrant of the body, including the right side of the head, neck, thorax, and right upper extremity. The left venous angle receives the thoracic duct, which drains lymph from the remainder of the body. Deoxygenated venous blood from the axillary vein passes through the subclavian veins into the brachiocephalic veins and ultimately returns to the right atrium.[1][2][3][4]
Embryology
The subclavian veins develop as part of the embryonic systemic venous system, derived from 3 paired embryonic veins that undergo major remodeling during the 4th week of human development: the vitelline veins from the yolk sac, the umbilical veins from the placenta, and the cardinal veins, which drain the embryo proper. The cardinal veins are most relevant to subclavian vein development and are divided into anterior cardinal veins, which drain the cranial portion of the embryo, and posterior cardinal veins, which drain the caudal portion. The subclavian veins arise primarily from the terminal segments of the anterior cardinal veins, with additional contribution from the developing upper extremity venous plexus. Growth of the upper limb buds is accompanied by the formation of an intralimb venous network, which establishes connections with the anterior cardinal veins. Progressive remodeling of this vascular network results in the formation of a definitive channel that becomes the subclavian vein.
Blood Supply and Lymphatics
The subclavian veins serve as the major venous channels draining the upper extremity and arise as continuations of the axillary veins. Deep lymphatic vessels of the upper limb follow the major deep venous pathways and terminate in the humoral axillary lymph nodes, which drain lymphatic fluid from joint capsules, periosteum, tendons, and musculature of the upper extremity. Efferent lymphatic vessels from the apical axillary lymph nodes pass through the cervicoaxillary canal before converging to form the subclavian lymphatic trunk. The left subclavian trunk drains directly into the thoracic duct, whereas the right subclavian trunk contributes to the formation of the right lymphatic duct, which enters the right venous angle at the junction of the IJV and subclavian vein.
Nerves
In normal human anatomy, the phrenic nerve (C3 through C5) lies posterior to the subclavian vein. The phrenic nerve passes anterior to the anterior scalene muscle, then courses posterior to the subclavian vein and anterior to the internal thoracic artery as it enters the thorax. Within the thorax, the phrenic nerve runs anterior to the root of the lung and courses between the fibrous pericardium and the mediastinal surface of the parietal pleura. Medial to the subclavian vein lie the brachiocephalic trunk, thoracic duct, trachea, and vagal trunks. Lateral to the subclavian vein lies the inferior trunk of the brachial plexus. The subclavius muscle is closely related to the subclavian vein, with the muscle positioned anterior to the vein. The subclavius muscle is a small, triangular muscle originating from the 1st rib and inserting on the inferior surface of the lateral clavicle. The brachial plexus, subclavian artery, and subclavian vein pass inferior to the subclavius muscle.[5][6] The subclavian vein lacks a named somatic motor or sensory nerve supply in standard gross anatomy descriptions. Autonomic innervation is present via sympathetic vasomotor fibers within perivascular plexuses, without a consistent assignment to discrete named nerves for this vessel.
Physiologic Variants
Anatomical variants of the subclavian vein are well described. The subclavian vein may course on a higher plane than usual, occasionally lying superior to the subclavian artery. The subclavian vein may also accompany the subclavian artery posterior to the anterior scalene muscle, or may course posterior to the anterior scalene muscle while the subclavian artery lies anterior to the muscle. The subclavian vein may also bifurcate, forming a venous ring encircling the clavicle, anterior scalene, or phrenic nerve, termed a clavicular loop. In some cases, the subclavian vein passes between the clavicle and the subclavius muscle. A rare variant involves the phrenic nerve crossing anterior to the subclavian vein or traversing its anterior wall, which may increase the risk of phrenic nerve injury during subclavian vein catheterization.
Surgical Considerations
The right and left subclavian veins are commonly used for central venous access. CVCs are inserted for the administration of parenteral fluids and medications and for the measurement of central venous pressure. Indications include hemodynamic instability, requirement for hyperosmolar infusions, and inadequate peripheral intravenous access. The most frequently used technique is the infraclavicular approach. In infraclavicular subclavian vein catheterization, patient positioning includes the Trendelenburg position with slight shoulder extension. The proceduralist places the thumb of one hand on the midpoint of the clavicle and the index finger on the jugular notch of the manubrium. Needle insertion occurs inferior to the thumb, approximately 1 cm lateral to the curvature of the middle one-third of the clavicle, with horizontal orientation toward the sternal notch. The catheter is advanced medially toward the tip of the index finger until access to the right venous angle posterior to the sternoclavicular joint is achieved. Bevel orientation toward the SVC is essential. Placement of a sterile finger in the ipsilateral supraclavicular fossa may assist orientation.
Another technique involves the supraclavicular approach, with puncture at the claviculo-sternocleidomastoid angle, superior to the clavicle and lateral to the insertion of the clavicular head of the sternocleidomastoid muscle. Needle trajectory is directed toward the contralateral nipple, remaining just inferior to the clavicle. Anatomical variation in lung apex position places the right lung dome slightly lower than the left, with potential extension above the first rib. Incorrect needle placement may result in pleural puncture and pneumothorax. Posterior misdirection may result in cannulation of the subclavian artery rather than the subclavian vein. Additional complications include hemothorax, chylothorax, catheter malpositioning, bleeding, infection, arrhythmia, air embolism, nerve injury, and venous thrombosis.[7][8][9][10]
Clinical Significance
Stenosis
Subclavian vein stenosis refers to the narrowing of the subclavian vein and may present with a spectrum of manifestations, ranging from asymptomatic disease to arm swelling, pain, paresthesia, neck pain, or occipital headache. Stenosis may arise from multiple intrinsic or extrinsic causes and may be further complicated by DVT. Intrinsic causes of subclavian vein stenosis include prior intravenous catheterization, including hemodialysis catheters and CVCs. Hemodialysis-related stenosis may also occur secondary to intimal hyperplasia driven by increased turbulent flow from an arteriovenous fistula. Extrinsic causes of subclavian vein stenosis include compression within the costoclavicular space (costoclavicular syndrome), Paget-Schroetter syndrome (PSS), regional tumors, lymphadenopathy, trauma, and mediastinal inflammatory pseudotumor. Costoclavicular syndrome is 1 of the 3 forms of thoracic outlet syndrome and constitutes the most common site of subclavian vein compression. Etiologies include depression of the clavicle toward the 1st rib, hypertrophy or increased tension of the subclavius muscle, congenital thoracic outlet anomalies, trauma, and external compression from tight clothing or straps.
Costoclavicular syndrome is characterized by spontaneous swelling of the entire upper extremity, often accompanied by cyanotic discoloration, heaviness, and pain. Unilateral upper-extremity swelling due to subclavian vein obstruction without associated thrombosis represents an uncommon form of thoracic outlet syndrome and should be considered in cases of unilateral limb swelling in the absence of lymphatic obstruction. The diagnosis is established with contrast venography. Plain radiography of the neck and chest, including cervical spine or thoracic inlet views, may demonstrate associated bony abnormalities that support diagnosis. Treatment depends on symptom severity and clinical findings. Conservative management with anticoagulation and limb elevation may lead to chronic venous congestion. Definitive management varies according to clinical context and presence or absence of thrombosis. Surgical thoracic outlet decompression or catheter-directed thrombolytic therapy constitutes the main treatment strategy in appropriate cases. Surgical options include transaxillary or paraclavicular first rib resection, with possible adjunct balloon angioplasty or direct venous reconstruction in cases of persistent subclavian vein obstruction.[11][12]
Deep Vein Thrombosis
Increased use of CVCs has led to a rising incidence of upper extremity DVT, particularly involving the subclavian, brachial, and axillary veins. Upper extremity DVT accounts for approximately 5% to 10% of all DVT cases, with incidence increasing annually. Upper extremity DVT is classified into primary and secondary forms. Primary upper-extremity DVT is characterized by PSS, which most commonly occurs in the dominant upper extremity of young athletes engaged in repetitive overhead or forceful upper-limb activity, including gymnastics, wrestling, swimming, football, baseball, and basketball.[13] Secondary upper extremity DVT most commonly occurs in patients with indwelling CVCs or underlying malignancy. Incidence of upper extremity DVT in patients with CVCs ranges from 14% to 23%, and pulmonary embolism occurs in up to 6% of upper extremity DVT cases.
The pathophysiology of PSS involves repetitive upper-extremity motion, leading to hypertrophy of the scalene musculature and compression of the neurovascular bundle as it exits the thorax between the cervical rib and surrounding musculature. Repetitive compression of the subclavian vein produces venous stasis and microtrauma, triggering activation of the intrinsic coagulation pathway and leading to thrombosis. In secondary upper extremity DVT, catheter-related endothelial injury activates the intrinsic coagulation pathway.
Clinical presentation of upper extremity DVT commonly includes limb swelling, arm discomfort, or arm heaviness. Upper extremity DVT complicated by pulmonary embolism may present with tachycardia, chest pain, or shortness of breath. Physical examination may demonstrate upper extremity erythema and prominent superficial veins across the chest and limb (Urschel sign). PSS typically presents with sudden-onset severe pain and swelling of the dominant upper extremity. Assessment of distal pulses bilaterally is essential. Limbs that appear pale, cool, or mottled suggest risk for ischemia. Documentation of motor and sensory deficits is an important component of examination.
Diagnosis is confirmed by compression duplex ultrasonography, which has a sensitivity of 97% and a specificity of 96% and is considered the gold standard for initial imaging. Magnetic resonance venography and computed tomographic venography demonstrate higher diagnostic accuracy than ultrasonography. The clinical utility of advanced imaging may be limited by cost, radiation exposure, and availability. Coagulation studies may be indicated in patients with suspected hypercoagulable states. D-dimer testing may assist in the exclusion of DVT in patients with low clinical suspicion.
Management depends on the clinical scenario and underlying etiology. In patients with CVCs, the American College of Chest Physicians guidelines recommend assessing the necessity of the line. Required catheters may remain in place with initiation of anticoagulation therapy, whereas nonessential catheters may be removed after 3 to 5 days of anticoagulation. Anticoagulation with warfarin for 3 to 6 months is recommended following initial heparin bridging. PSS with acute thrombosis often requires urgent surgical intervention.[14][15][16][17]
Media
(Click Image to Enlarge)
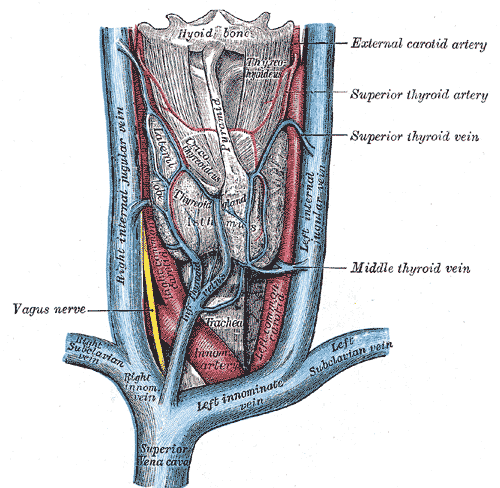
Vascular Structures of the Anterior Neck. The illustration depicts the major veins and arteries of the anterior neck, including the superior vena cava, right and left innominate veins, right and left subclavian veins, and right and left internal jugular veins. Arterial structures shown are the innominate artery and portions of the common carotid arteries. The image also indicates the relative position of the hyoid bone, thyroid gland, and trachea. Additionally, the vagus nerve and the superior, middle, and inferior thyroid veins, as well as the superior thyroid artery, are labeled.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
References
Rivard AB, Kortz MW, Burns B. Anatomy, Head and Neck: Internal Jugular Vein. StatPearls. 2026 Jan:(): [PubMed PMID: 30020630]
Ilahi M, St Lucia K, Ilahi TB. Anatomy, Thorax, Thoracic Duct. StatPearls. 2026 Jan:(): [PubMed PMID: 30020599]
Mahabadi N, Goizueta AA, Bordoni B. Anatomy, Thorax, Lung Pleura And Mediastinum. StatPearls. 2026 Jan:(): [PubMed PMID: 30085590]
Rizvi S, Wehrle CJ, Law MA. Anatomy, Thorax, Mediastinum Superior and Great Vessels. StatPearls. 2026 Jan:(): [PubMed PMID: 30137860]
Oliver KA, Ashurst JV. Anatomy, Thorax, Phrenic Nerves. StatPearls. 2026 Jan:(): [PubMed PMID: 30020697]
Hyland S, Charlick M, Varacallo MA. Anatomy, Shoulder and Upper Limb, Clavicle. StatPearls. 2026 Jan:(): [PubMed PMID: 30252246]
Daly JM, Ziegler B, Dudrick SJ. Central venous catherization. The American journal of nursing. 1975 May:75(5):820-4 [PubMed PMID: 1039271]
Björkander M, Bentzer P, Schött U, Broman ME, Kander T. Mechanical complications of central venous catheter insertions: A retrospective multicenter study of incidence and risks. Acta anaesthesiologica Scandinavica. 2019 Jan:63(1):61-68. doi: 10.1111/aas.13214. Epub 2018 Jul 11 [PubMed PMID: 29992634]
Level 2 (mid-level) evidenceKolikof J, Peterson K, Williams C, Baker AM. Central Venous Catheter Insertion. StatPearls. 2026 Jan:(): [PubMed PMID: 32491730]
Devi R. Ultrasound-Guided Subclavian Vein Catheterization: Contrasting Supraclavicular and Infraclavicular Approaches for Enhanced Procedural Precision. Cureus. 2024 May:16(5):e60974. doi: 10.7759/cureus.60974. Epub 2024 May 24 [PubMed PMID: 38910755]
White JM, Comerota AJ. Venous Compression Syndromes. Vascular and endovascular surgery. 2017 Apr:51(3):155-168. doi: 10.1177/1538574417697208. Epub [PubMed PMID: 28330436]
Judd AC, Weinkauf C, Erdrich J. Subclavian Vein Stenosis Imitating Inflammatory Breast Cancer. Cureus. 2022 Dec:14(12):e32184. doi: 10.7759/cureus.32184. Epub 2022 Dec 4 [PubMed PMID: 36620820]
Alahmadi MH, Baril DT. Paget-Schroetter Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 29494023]
Mustafa J, Asher I, Sthoeger Z. Upper Extremity Deep Vein Thrombosis: Symptoms, Diagnosis, and Treatment. The Israel Medical Association journal : IMAJ. 2018 Jan:20(1):53-57 [PubMed PMID: 29658209]
Koratala A, Bhattacharya D, Chamarthi G. Blood finds its own way: Axillary vein thrombosis with extensive chest-wall collaterals. Clinical case reports. 2018 Sep:6(9):1917-1918. doi: 10.1002/ccr3.1759. Epub 2018 Aug 13 [PubMed PMID: 30214799]
Level 3 (low-level) evidenceEvans NS, Ratchford EV. Catheter-related venous thrombosis. Vascular medicine (London, England). 2018 Aug:23(4):411-413. doi: 10.1177/1358863X18779695. Epub 2018 Jun 28 [PubMed PMID: 29952254]
Sahota RJ, Lotfollahzadeh S, Soos MP. Subclavian Vein Thrombosis. StatPearls. 2026 Jan:(): [PubMed PMID: 32644695]