Introduction
The foramen spinosum is a small, circular opening located posterolateral to the foramen ovale within the greater wing of the sphenoid (see Image. Skull Foramina). The greater wing of the sphenoid projects laterally from the sphenoid body, contributing to the floor of the middle cranial fossa. Jakob Benignus Winslow coined the term “foramen spinosum” due to the aperture's position adjacent to the spinous process of the greater wing of the sphenoid.[1]
The foramen spinosum conveys the middle meningeal vessels and the mandibular nerve's meningeal branch, positioning this structure as an essential reference in diagnosing epidural bleeding after head injuries. The surgical significance of this opening lies in providing orientation during middle cranial fossa approaches, skull base surgeries, and interventions involving the infratemporal fossa, where precise localization reduces the risk of vascular or neural injury. Knowledge of the foramen spinosum’s anatomy and contents allows clinicians to accurately interpret imaging, plan surgical procedures, and anticipate complications associated with trauma or iatrogenic injury.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The foramen spinosum connects the infratemporal fossa with the middle cranial fossa, along with other foramina such as the foramen ovale and foramen rotundum. Neurovascular structures traversing the foramen spinosum include the middle meningeal artery, middle meningeal vein, and nervus spinosus—the recurrent meningeal branch of the mandibular nerve (cranial nerve V3)—into the middle cranial fossa.
The middle meningeal artery represents the principal arterial supply to the meninges, dura mater, and calvaria. This blood vessel typically arises from the maxillary artery, a major branch of the external carotid artery. After entering the middle cranial fossa via the foramen spinosum, the artery divides into anterior and posterior branches. The anterior branch courses beneath the pterion. The pterion is the junction of the frontal, parietal, temporal, and sphenoid bones. Trauma to this region may rupture the vessel, resulting in an epidural hematoma. Several smaller arterial branches also emerge around the foramen spinosum.
The middle meningeal veins drain primarily into the pterygoid venous plexus and the cavernous sinus. Small emissary veins may accompany the middle meningeal vessels at the foramen spinosum, forming connections between the pterygoid venous plexus and the cavernous sinus. These venous communications are clinically relevant, providing potential pathways for the spread of infection or tumor and contributing to venous bleeding during skull base surgery.
The foramen spinosum serves as a readily identifiable anatomical landmark during neurosurgical procedures and radiography-based diagnostics. In adults, the average diameter of the foramen spinosum is 2.63 mm.[2]
Embryology
The foramen spinosum develops within the greater wing of the sphenoid, which originates from the cartilaginous ala temporalis and alar process. Ossification begins around 15 to 16 weeks of gestation and continues through the perinatal period. The foramen typically begins to form during late fetal life as the greater wing (alisphenoid) ossifies, with maturation continuing through early infancy and into early childhood.[3][4]
The 1st pharyngeal arch arises during the 4th week of development, situated between the stomodeum and the 1st pharyngeal groove. The trigeminal nerve (cranial nerve V) supplies the 1st pharyngeal arch. Most of the sphenoid bone, including the greater wings, originates from neural crest–derived mesenchyme, with a minor contribution from paraxial mesoderm.
Development of the foramen spinosum occurs around the proximal segment of the middle meningeal artery. Failure of the artery to enter the cranial cavity at this site, as may occur when it originates from a persistent stapedial artery, results in hypoplasia or absence of the foramen.
Nerves
The meningeal (recurrent) branch of the mandibular nerve, or nervus spinosus, reenters the cranial cavity via the foramen spinosum, supplying the dura mater of the middle cranial fossa along the course of the middle meningeal artery and its branches.[5][6]
Physiologic Variants
The foramen spinosum typically measures 2.4 to 2.5 mm in diameter in adults and is significantly smaller in newborns. Bilateral presence occurs in most individuals. However, unilateral or bilateral duplication may be observed. In some cases, the foramen is smaller than usual or completely absent.
When the foramen spinosum is absent, the middle meningeal vessels and the recurrent meningeal branch of the mandibular nerve may pass through the foramen ovale. Occasionally, a groove or partial bony channel connects the foramen spinosum to the foramen ovale, likely reflecting incomplete ossification of the intervening sphenoid bone. This anomaly appears to be unilateral and is not associated with other abnormalities.
Another developmental variant arises when the middle meningeal artery originates directly from a persistent stapedial artery. In such cases, the artery typically enters the cranial cavity via the foramen ovale rather than the foramen spinosum, resulting in a diminutive or absent foramen.[7][8]
Duplication of the foramen spinosum occurs in approximately 0.4% to 2.5% of skulls, whereas complete absence is observed in fewer than 1% of cases, most commonly associated with a persistent stapedial artery. Hypoplasia is more frequent unilaterally than bilaterally.
Surgical Considerations
The foramen spinosum serves as a surgical landmark and guide during microsurgery of the middle cranial fossa. Extracranially, the auriculotemporal nerve typically forms a loop around the middle meningeal artery, creating a close anatomical relationship that increases the risk of nerve injury during procedures in the infratemporal fossa.[9]
The middle meningeal artery represents a key target in the endovascular management of chronic subdural hematoma. During angiography and embolization, the osseous entry site at the foramen spinosum functions as a landmark for delineating the intracranial course of the artery while minimizing the risk of injury to adjacent neural structures.
Clinical Significance
On computed tomography (CT), the foramen spinosum appears as a small, round opening located posterolateral to the foramen ovale (see Images. Radiographic Identification of the Foramen Spinosum; Three-Dimensional Computed Tomography Reconstruction of the Middle Cranial Fossa and Foramen Spinosum). Identification of the foramen assists in confirming skull-base orientation and differentiating the greater wing of the sphenoid from adjacent foramina. Enlargement or erosion of the foramen may indicate pathology affecting the middle meningeal artery or neighboring skull-base tumors.
The foramen spinosum is clinically relevant due to its proximity to the foramen ovale and the middle meningeal artery, serving as an important landmark during neurosurgical procedures involving the middle cranial fossa. Relevant procedures include surgeries for trigeminal neuralgia, tumors, and epilepsy.
Various techniques exist for the treatment of trigeminal neuralgia, including microvascular decompression, stereotactic radiosurgery, and percutaneous procedures such as radiofrequency rhizotomy or balloon decompression. Percutaneous approaches require cannulation of the foramen ovale, which may be complicated by anatomical variation in the foramen’s shape. Although classically described as oval, the foramen ovale may appear almond-shaped, round, irregular, or slit-like. Familiarity with the anatomical location of the foramen ovale facilitates successful computed tomograph–guided percutaneous cannulation.
A study examining 100 dry human skulls (70 male, 30 female) investigated anatomical variations of the foramen ovale. The mean distance between the foramen ovale and the foramen spinosum was approximately 3 to 4 mm, with minor right–left and sex-related differences. Knowledge of this distance can assist in locating the foramen ovale for percutaneous cannulation and increase procedural success. Additional studies have evaluated the optimal angle of cannulation for the foramen ovale.[10][11]
The middle cranial fossa is frequently affected in basilar skull fractures. Such fractures often propagate through the temporal bone and middle cranial fossa, potentially involving the tegmen tympani, internal acoustic meatus, foramen ovale, and, occasionally, the foramen spinosum. Trauma to the foramen spinosum or temporal bone, whether from road traffic accidents or direct impact, can sever the middle meningeal artery along its intracranial course, including segments near the foramen spinosum. This vascular injury may result in bleeding between the skull and dura mater, producing an epidural hematoma.[12][13]
Media
(Click Image to Enlarge)
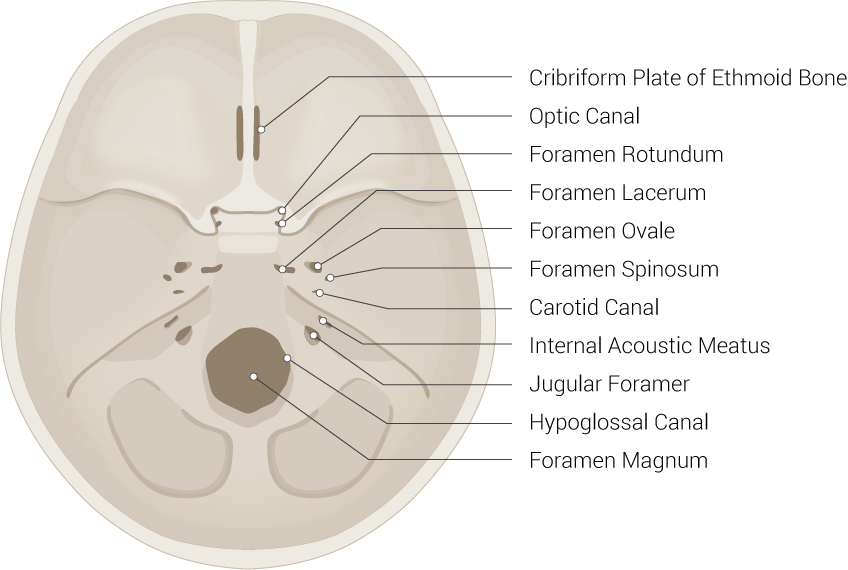
Skull Foramina. This illustration includes the cribriform plate of the ethmoid bone, optic canal, foramen rotundum, foramen lacerum, foramen ovale, foramen spinosum, carotid canal, internal acoustic meatus, jugular foramen, hypoglossal canal, and foramen magnum.
Illustrated by B Palmer
(Click Image to Enlarge)

Radiographic Identification of the Foramen Spinosum. The red arrow highlights the foramen spinosum, a small circular opening in the floor of the middle cranial fossa. This aperture is positioned lateral to the foramen ovale and anterior to the petrous portion of the temporal bone, serving as a critical landmark for the entry of the middle meningeal vasculature into the cranial vault.
Contributed by Sunil Munakomi, MD
(Click Image to Enlarge)
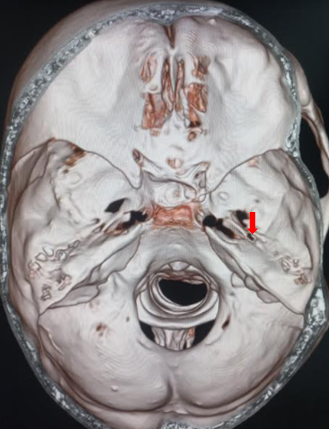
Three-Dimensional Computed Tomography Reconstruction of the Middle Cranial Fossa and Foramen Spinosum. This image identifies the foramen spinosum with a red arrow, located posterolateral to the foramen ovale in the greater wing of the sphenoid bone. This opening transmits the middle meningeal artery and the meningeal branch of the mandibular nerve into the cranial vault. Visible surrounding structures include the cribriform plate, lesser wings of the sphenoid, sella turcica, clivus, petrous temporal bone, and the foramen magnum.
Contributed by Sunil Munakomi, MD
References
Khairnar KB, Bhusari PA. An anatomical study on the foramen ovale and the foramen spinosum. Journal of clinical and diagnostic research : JCDR. 2013 Mar:7(3):427-9. doi: 10.7860/JCDR/2013/4894.2790. Epub 2013 Mar 1 [PubMed PMID: 23634389]
Yanagi S. [Developmental studies on the foramen rotundum, foramen ovale and foramen spinosum of the human sphenoid bone]. [Hokkaido igaku zasshi] The Hokkaido journal of medical science. 1987 May:62(3):485-96 [PubMed PMID: 3610040]
Nemzek WR, Brodie HA, Hecht ST, Chong BW, Babcook CJ, Seibert JA. MR, CT, and plain film imaging of the developing skull base in fetal specimens. AJNR. American journal of neuroradiology. 2000 Oct:21(9):1699-706 [PubMed PMID: 11039353]
Yamamoto M, Jin ZW, Hayashi S, Rodríguez-Vázquez JF, Murakami G, Abe S. Association between the developing sphenoid and adult morphology: A study using sagittal sections of the skull base from human embryos and fetuses. Journal of anatomy. 2021 Dec:239(6):1300-1317. doi: 10.1111/joa.13515. Epub 2021 Jul 15 [PubMed PMID: 34268732]
Lee SH, Hwang SJ, Koh KS, Song WC, Han SD. Macroscopic Innervation of the Dura Mater Covering the Middle Cranial Fossa in Humans Correlated to Neurovascular Headache. Frontiers in neuroanatomy. 2017:11():127. doi: 10.3389/fnana.2017.00127. Epub 2017 Dec 19 [PubMed PMID: 29311855]
Schueler M, Neuhuber WL, De Col R, Messlinger K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache. 2014 Jun:54(6):996-1009. doi: 10.1111/head.12371. Epub 2014 May 6 [PubMed PMID: 24673461]
Lang J, Maier R, Schafhauser O. [Postnatal enlargement of the foramina rotundum, ovale et spinosum and their topographical changes]. Anatomischer Anzeiger. 1984:156(5):351-87 [PubMed PMID: 6486466]
Ellwanger JH, Campos Dd. Abnormality of the Foramen Spinosum due to a Variation in the Trajectory of the Middle Meningeal Artery: A Case Report in Human. Journal of neurological surgery reports. 2013 Dec:74(2):73-6. doi: 10.1055/s-0033-1347901. Epub 2013 May 23 [PubMed PMID: 24294564]
Level 3 (low-level) evidenceKrayenbühl N, Isolan GR, Al-Mefty O. The foramen spinosum: a landmark in middle fossa surgery. Neurosurgical review. 2008 Oct:31(4):397-401; discussion 401-2. doi: 10.1007/s10143-008-0152-6. Epub 2008 Aug 2 [PubMed PMID: 18677523]
Zdilla MJ, Hatfield SA, McLean KA, Laslo JM, Cyrus LM, Lambert HW. Orientation of the Foramen Ovale: An Anatomic Study With Neurosurgical Considerations. The Journal of craniofacial surgery. 2016 Jan:27(1):234-7. doi: 10.1097/SCS.0000000000002332. Epub [PubMed PMID: 26703059]
Zdilla MJ, Hatfield SA, Mangus KR. Angular Relationship Between the Foramen Ovale and the Trigeminal Impression: Percutaneous Cannulation Trajectories for Trigeminal Neuralgia. The Journal of craniofacial surgery. 2016 Nov:27(8):2177-2180. doi: 10.1097/SCS.0000000000003138. Epub [PubMed PMID: 28005784]
Roski RA, Owen M, White RJ, Takaoka Y, Bellon EM. Middle meningeal artery trauma. Surgical neurology. 1982 Mar:17(3):200-3 [PubMed PMID: 7079938]
Level 3 (low-level) evidenceChmielewski P, Skrzat J, Walocha J. Clinical importance of the middle meningeal artery. Folia medica Cracoviensia. 2013:53(1):41-6 [PubMed PMID: 24858329]