 Anatomy, Shoulder and Upper Limb: Supraclavicular Fossa
Anatomy, Shoulder and Upper Limb: Supraclavicular Fossa
Introduction
The supraclavicular fossa is a surface depression of the lower lateral neck overlying the supraclavicular triangle of the posterior cervical region (see Image. Surface Landmarks of the Lower Neck and Upper Thorax). This anatomically complex space contains major neurovascular and lymphatic structures, including the subclavian vessels, brachial plexus, and terminal lymphatic ducts. The region serves as a passage for innervation, blood flow, and lymphatic drainage of the upper extremity. The subclavian artery and its branches provide the principal arterial supply, while the jugular and subclavian veins facilitate venous return. The cervical and brachial plexuses constitute the principal neural structures within the region. Physiologic variation is common, particularly in lymphatic architecture and soft tissue composition.
The supraclavicular fossa has substantial clinical significance due to its complex anatomy and involvement in various conditions, encompassing neoplastic, congenital, and infectious etiologies. The area is also important in the evaluation of supraclavicular lymphadenopathy and metastatic disease. Critical neurovascular and lymphatic structures in the region make surgical intervention high-risk. Careful operative technique and a structured diagnostic approach are essential to minimize complications. In-depth understanding of the anatomy and function of the supraclavicular fossa enables accurate diagnosis, appropriate imaging and procedural selection, and safe surgical planning.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The neck is classically divided into 2 primary anatomic triangles: anterior and posterior. The anterior triangle may be subdivided into 4 smaller triangles: submental, submandibular, superior carotid, and inferior carotid. These anterior regions fall outside the scope of this discussion. The posterior triangle is defined by the posterior border of the sternocleidomastoid (SCM), the clavicle, and the anterior border of the trapezius. The inferior belly of the omohyoid muscle divides the posterior triangle into the occipital and supraclavicular triangles. The supraclavicular triangle is the focus of this activity. The supraclavicular triangle is also called the "subclavian triangle" in some sources.[1] The term “fossa” denotes the shallow depression overlying the triangle. Some authors propose subdividing the supraclavicular fossa into 2 regions, including the costoclavicular space and the scalene triangle.[2]
Embryology
The supraclavicular fossa is a surface anatomical depression that develops from the complex embryologic organization of the lateral neck, primarily shaped by mesodermal and neural crest–mediated patterning of the pharyngeal apparatus and surrounding musculoskeletal structures. During the 4th to 8th weeks of gestation, segmentation of paraxial mesoderm into somites forms the scalene musculature and connective tissue framework, ultimately defining the posterior cervical triangle and its inferior component, the supraclavicular fossa.[3]
Neural crest cells contribute to the formation of cervical fascial planes and vascular structures, while the lymphatic system arises from venous endothelial outpouchings that form primitive lymph sacs. These sacs later differentiate into cervical lymph node chains, including the supraclavicular nodes. The close spatial relationship between the developing thoracic duct on the left and the right lymphatic duct on the right explains the asymmetric lymphatic drainage observed in adulthood, with the left supraclavicular region (Virchow node) receiving lymph from the thoracoabdominal cavity. The supraclavicular fossa thus represents a convergence zone in which musculoskeletal boundaries, vascular structures, and lymphatic pathways established during embryogenesis create a clinically significant anatomic space.
Blood Supply and Lymphatics
The vasculature of the supraclavicular triangle is complex and critical for generating a differential diagnosis of regional pathology. The largest artery within the fossa is the subclavian artery, divided into 3 segments by the anterior scalene muscle. The 3rd segment, distal to the anterior scalene, traverses the supraclavicular fossa. The transverse cervical and suprascapular arteries, branches of the subclavian, course through the fossa after originating from its 1st segment. Venous structures include the external and internal jugular veins, as well as the corresponding subclavian, suprascapular, and transverse cervical veins. The fascia of the omohyoid muscle separates the superficial suprascapular vein from the deep suprascapular artery.
The supraclavicular fossa contains lymphatic structures that differ according to laterality. The thoracic duct on the left collects lymph from the majority of the body and empties into the origin of the brachiocephalic vein.[4] The right lymphatic duct drains lymph from the right thorax, right upper extremity, and right portion of the head and neck into the subclavian vein or right internal jugular vein (see Image. Lymphatic System). Numerous lymph nodes occupy the supraclavicular fossa, with precise locations highly variable and beyond the scope of this activity. Classification by neck levels designates these nodes as Level V, while regional classification identifies them as inferior deep cervical lymph nodes.
Nerves
Primary neural structures in the supraclavicular fossa are organized into superficial and deep components by the fascial carpet of the neck. The vagus nerve (cranial nerve X) courses superficially within the carotid sheath. Deep to the fascial carpet, the phrenic nerve (C3–C5) innervates the diaphragm and runs along the anterior scalene muscles within the supraclavicular triangle toward its thoracic insertion.[5] The brachial plexus (C5–T1) also traverses the fossa, forming a complex network that innervates portions of the upper extremities and thorax. Detailed anatomy and the distal course of the brachial plexus are beyond the scope of this activity.
Muscles
The musculature of the supraclavicular fossa is critical for understanding regional anatomy, as muscles often serve as anatomic landmarks. The platysma, a thin superficial muscle, extends from the pectoralis and deltoid to the base of the mandible. The platysma overlies the fascial carpet and receives innervation from the cervical branch of the facial nerve (cranial nerve VII).
Two of the 3 borders of the supraclavicular fossa are muscular. The SCM forms the anteromedial border, extending from the sternum to the mastoid process and lying superficial to the fascial carpet. The omohyoid forms the superolateral border, extending from the scapula to the hyoid bone while passing behind the SCM. The omohyoid consists of 2 bellies connected by a tendon invested in the deep cervical fascia (see Image. Anterior Neck Muscles and Related Structures).
Deep to the cervical fascia lie the scalene muscles, a group of 3 accessory muscles originating on the cervical vertebrae and inserting on the 1st and 2nd ribs. The scalenes receive innervation from C4 to C6 and function as accessory muscles of respiration.
A rare anatomical variant, the supraclavicularis proprius muscle, can cause clavicular motion dysfunction and compression of nerves within the supraclavicular fossa. This muscle originates posteriorly from the clavicle near the sternoclavicular joint and may insert along the clavicle near the acromion, extending toward the acromion and trapezius.[6]
Physiologic Variants
Physiologic variants of the supraclavicular fossa reflect inherent anatomic and functional variability of lymphatic, vascular, and soft tissue components, and recognition of these differences is essential to avoid misinterpretation as pathology. The fossa contains a variable number of lymph nodes, typically ranging from 4 to 12, with considerable interindividual differences in size, morphology, and location along the transverse cervical vessels and adjacent scalene musculature.[7] Small, mobile, nontender lymph nodes may be palpable in otherwise healthy individuals, particularly in thin patients, representing normal physiologic prominence rather than disease. Lymph node size may also fluctuate in response to transient immune stimulation, including minor infections or inflammatory processes, without indicating malignancy.
Laterality is an important physiologic variant within the supraclavicular region. The right and left supraclavicular fossae exhibit distinct lymphatic drainage patterns resulting from asymmetric embryologic development of the lymphatic ducts. The right fossa drains via the right lymphatic duct, receiving lymph from the right thorax, upper extremity, and head and neck. The left fossa is associated with the thoracic duct, which drains lymph from the majority of the body. This asymmetry contributes to differences in lymph node prominence and functional load between sides and may explain subtle baseline size discrepancies that are physiologic rather than pathologic.[8]
Anatomic variation in the composition of the supraclavicular fossa also affects clinical appearance. Differences in adipose tissue volume, platysma and deep cervical fascia thickness, and development of adjacent musculature, including the SCM and omohyoid muscles, alter fossa depth and contour. The fossa may appear more pronounced in individuals with low body fat or well-developed musculature but look shallow or less distinct in others. Vascular structures, including the subclavian and transverse cervical vessels, may vary in caliber and course, occasionally producing visible or palpable pulsations that can be mistaken for masses.
Lymphatic architecture within the supraclavicular fossa exhibits physiologic heterogeneity. Lymph nodes may differ in internal composition, including the relative proportion of cortical and fatty hilar elements, which can affect imaging appearance. On ultrasound or cross-sectional imaging, normal nodes may appear slightly enlarged while retaining benign features, such as an oval shape and preserved fatty hilum. Distinguishing these variants from malignant characteristics is essential, particularly given the historical clinical significance of supraclavicular lymphadenopathy. Node number and clustering also vary, with some individuals exhibiting accessory nodal groups or densely aggregated chains, reflecting normal developmental variation rather than pathology.
Dynamic physiologic changes occur within the supraclavicular fossa. Lymph node size and visibility may transiently increase during immune activation, such as after vaccination or localized inflammation, and subsequently regress. Positional changes of the neck and upper extremity can also modify the palpability of fossa structures due to shifting relationships among the clavicle, scalene muscles, and overlying soft tissues.
The supraclavicular fossa exhibits a wide spectrum of physiologic variation in lymph node number, size, laterality, and surrounding soft tissue anatomy. Recognition of these normal variants, particularly asymmetry in lymphatic drainage, nodal morphology variability, and effects of body habitus, is essential in clinical and radiologic evaluation to prevent overdiagnosis and distinguish benign findings from clinically significant pathology.
Surgical Considerations
Supraclavicular Cystic Masses
Evaluation of a supraclavicular fossa cystic mass begins with ultrasound, followed by computed tomography (CT) to assess lesion vascularity. Core needle biopsy may be performed under ultrasound guidance when indicated. Lesions without appreciable vascularity on imaging are typically assessed with fine needle aspiration (FNA), with fluid characteristics and cytologic analysis guiding subsequent surgical management.
Surgical evaluation and management of a cystic mass in the supraclavicular fossa require a structured, stepwise approach to minimize complications and ensure accurate diagnosis. High-resolution ultrasound typically serves as the 1st-line imaging modality, providing real-time assessment of cystic versus solid components, internal septations, and vascularity through Doppler interrogation. Ultrasound also delineates relationships between the lesion and adjacent structures, including the internal jugular vein, subclavian vessels, and brachial plexus. Contrast-enhanced CT or magnetic resonance imaging (MRI) is often performed subsequently to define lesion extent, evaluate deep thoracic inlet involvement, and detect subtle enhancement indicative of a solid or malignant component. This imaging is critical due to the proximity of vital neurovascular structures and potential inferior extension into the mediastinum.
Determining vascularity is a critical decision point. Vascular lesions, such as venous malformations or aneurysms, generally preclude percutaneous biopsy due to hemorrhage risk, prompting referral to vascular surgery or interventional radiology. Nonvascular, cystic lesions are typically assessed with FNA as a minimally invasive diagnostic step. FNA provides information on cyst contents, including serous fluid, chyle, purulence, or keratinaceous debris. Cytologic analysis may reveal malignant cells, particularly in cystic nodal metastases that are increasingly associated with head and neck squamous cell carcinoma, including human papillomavirus–related disease.
FNA results guide further management. Benign-appearing cysts with nonsuspicious cytology may still require surgical excision if symptomatic, enlarging, or cosmetically concerning, as definitive diagnosis often relies on histopathology. Detection of malignant cells necessitates comprehensive oncologic evaluation, including imaging of the primary site and interprofessional planning prior to surgical intervention. Open excisional biopsy without prior diagnostic workup is generally discouraged due to disruption of tissue planes, potential complications for subsequent oncologic surgery, and increased risk of tumor seeding.[9]
Surgical excision in the supraclavicular fossa demands meticulous planning due to the dense concentration of vital structures. The spinal accessory nerve (cranial nerve XI), phrenic nerve, brachial plexus trunks, thoracic duct (left side), and major vascular structures are all at risk during dissection. Preoperative imaging must be carefully reviewed to anticipate anatomic variations and define safe surgical planes. Intraoperative blunt and sharp dissection preserves these structures. Surgeons should pay special attention to identifying the left thoracic duct to prevent chyle leak—a postoperative complication that may require dietary changes, drainage, or reoperation if persistent.
The surgical approach to a supraclavicular cystic mass is guided by imaging findings and FNA results. Emphasis should be placed on accurate lesion evaluation, prevention of premature excision, and careful consideration of regional anatomy to maximize safety and outcomes.
Supraclavicular Surgical Approach
The supraclavicular fossa serves as a versatile surgical window into the thoracic inlet, upper limb, and lower neck, providing direct access to lymph nodes, brachial plexus trunks, subclavian vessels, and phrenic nerve. Advantages of this approach include minimized tissue disruption, clear visualization of critical neurovascular structures, and feasibility for procedures such as lymph node dissection, tumor excision, thoracic outlet syndrome (TOS) decompression, and subclavian-vessel repair. Limitations involve the high density of vital structures, narrow operative corridor, and risk of nerve or vascular injury, necessitating meticulous preoperative planning, imaging review, and surgical expertise to optimize outcomes.[10][11]
A supraclavicular corridor is created by a transverse incision approximately 1 fingerbreadth above the clavicle, extending from near the midline toward the posterior border of the SCM, entering the roof of the posterior cervical triangle. Dissection proceeds through the platysma and investing layer of deep cervical fascia, taking care to preserve the omohyoid, scalene muscles, and underlying neurovascular structures. This route provides direct access to the supraclavicular triangle, brachial plexus trunks, subclavian vessels, and adjacent Level V lymph nodes while minimizing tissue disruption.[12]
Supraclavicular Artery Island Flap
The supraclavicular fossa serves as a donor site for pedicled or free flaps based on the supraclavicular artery, a major branch of the transverse cervical artery. Indications include reconstruction of head, neck, and upper thoracic defects, especially after oncologic resection.[13] Advantages include thin, pliable tissue with a reliable vascular pedicle and minimal donor-site morbidity. Limitations involve flap size constraints, potential distal necrosis, and the need for careful planning to preserve shoulder and neck function while achieving adequate coverage.[14]
Clinical Significance
The complex anatomy of the supraclavicular fossa permits a broad differential diagnosis for regional pathology, encompassing neoplastic, congenital, and infectious etiologies. Neoplastic processes may cause supraclavicular lymph node enlargement from either a primary tumor, such as lymphoma, or metastatic growth from a distant site. Primary malignancies that metastasize to the region include, but are not limited to, tumors of the breast, lung, reproductive organs, gastrointestinal tract, and thyroid. FNA assists in identifying the primary neoplasm. Enlargement of the left supraclavicular node, or Virchow node, may indicate advanced gastrointestinal malignancy (see Image. Virchow Node and Troisier Sign).[15] A study reported that most supraclavicular masses biopsied via FNA represented malignant processes, with metastatic tumors far more common than lymphoma.[16][17]
Congenital anomalies producing supraclavicular masses may result from abnormal development of the upper respiratory or gastrointestinal tract. These masses are often cystic and include epidermoid cysts, cystic teratomas, and bronchogenic cysts, among others.[18][19][20] Lymphatic malformations, such as cystic hygromas, may also present as supraclavicular masses and warrant inclusion in the differential diagnosis.
Infectious processes can produce lymphadenopathy manifesting as cystic supraclavicular masses. Causative pathogens vary by location and include streptococcal, staphylococcal, fungal, and mycobacterial species. FNA and culture can help identify the causative pathogen.
Other Issues
The supraclavicular fossa ultrasound window has been recommended for real-time positioning of a central venous catheter tip within the cavoatrial junction. This approach also helps avoid arterial puncture.[21]
Brachial plexus blocks are typically performed via axillary, interscalene, or infraclavicular approaches. Ultrasound-guided supraclavicular blocks may reduce the risk of pneumothorax.[22]
Lymph nodes in the left supraclavicular area, known as Virchow nodes, may indicate the presence of tumors, such as adenocarcinoma or malignancies of the abdominal, lung, breast, thyroid, nasopharyngeal, and prostate regions. Enlargement and hardening of Virchow nodes constitute the Troisier sign, a clinical indicator of malignancy.[23]
No unanimous consensus has been established on whether supraclavicular lymph nodes serve as sites of metastases for tumors such as esophageal carcinoma, regardless of disease stage.[24] Lymph node metastases at this site do not directly predict survival or mortality.
Compression of the supraclavicular and infraclavicular fossae can lead to TOS, most commonly of neurogenic origin (see Image. Anatomical Relationships at the Right Thoracic Outlet). Increased tone and shortening of the anterior and medial scalene muscles, along with the subclavius, compress the brachial vasculonervous complex. Management of this syndrome is often nonsurgical.
Rarely, the supraclavicular fossa may contain a phrenic nerve schwannoma, which can present as an asymptomatic swelling. Confirmation with MRI or CT typically warrants surgical resection.[25]
TOS may also result from a cervical rib that further narrows the brachial vascular and nervous passage, producing neurogenic symptoms (see Image. Neurovascular Compression in Thoracic Outlet Syndrome). Surgical resection is indicated if conservative treatment fails.[26]
Media
(Click Image to Enlarge)
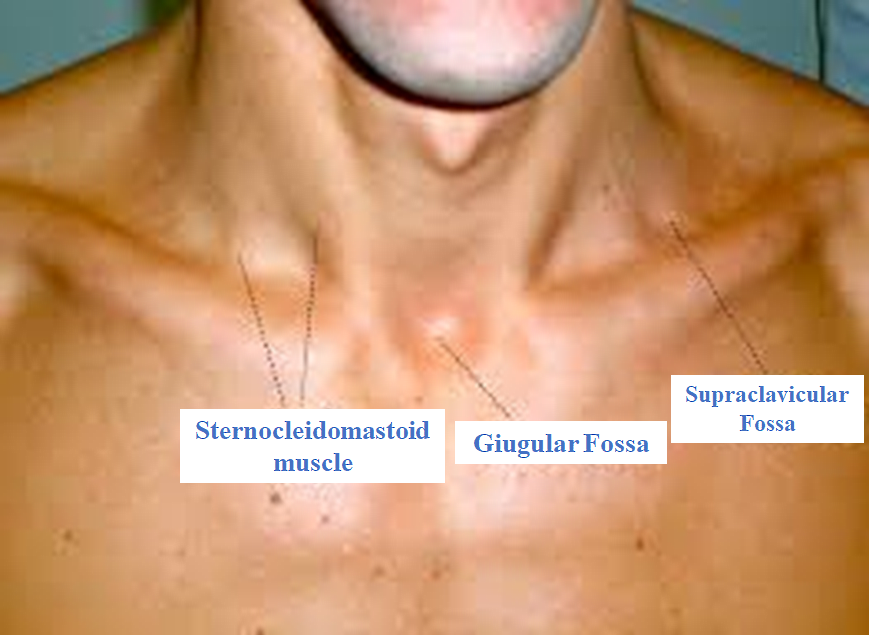
Surface Landmarks of the Lower Neck and Upper Thorax. This image highlights the visible anatomical features used to identify underlying structures. Key landmarks include the sternocleidomastoid muscle, the jugular (suprasternal) fossa, and the supraclavicular fossa.
Contributed by Bruno Bordoni, PhD.
(Click Image to Enlarge)
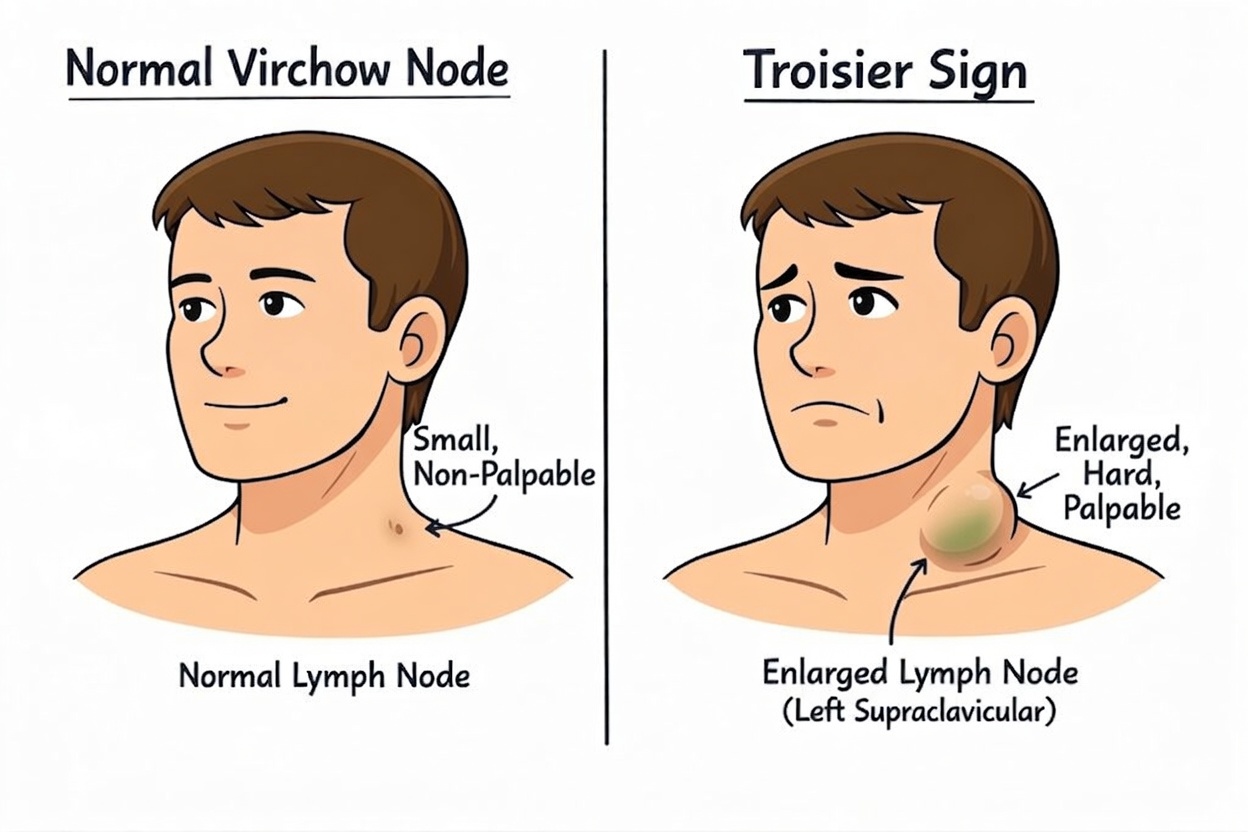
Virchow Node and Troisier Sign. This diagram contrasts a normal, nonpalpable left supraclavicular lymph node with the enlarged, firm, palpable Virchow node characteristic of Troisier sign, classically indicating gastric cancer metastasis via the thoracic duct.
Contributed by StatPearls
(Click Image to Enlarge)
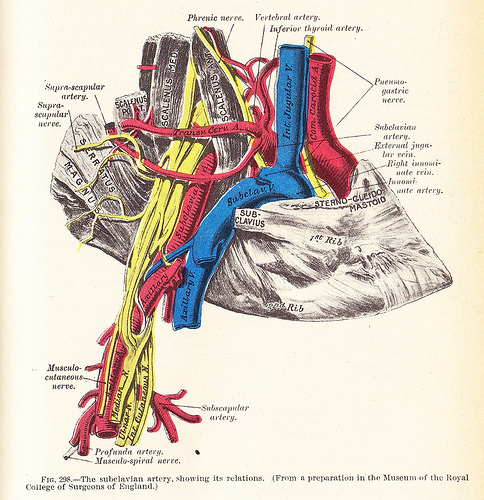
Anatomical Relationships at the Right Thoracic Outlet. The diagram depicts the right subclavian vein and artery, along with adjacent vessels, nerves, muscles, and bones involved in thoracic outlet compression.
Henry Van Dyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
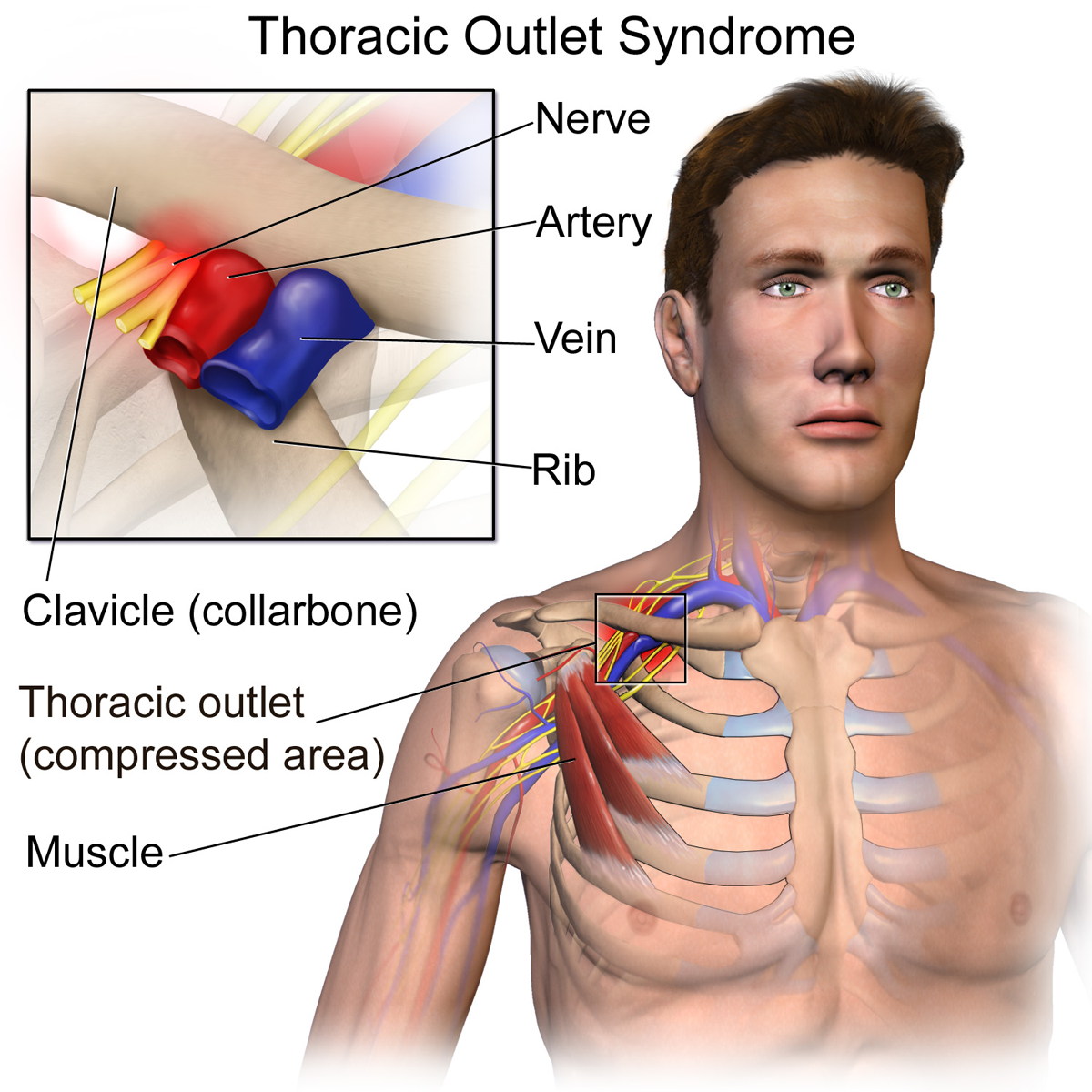
Neurovascular Compression in Thoracic Outlet Syndrome. This illustration shows the compression of the neurovascular bundle (the brachial plexus nerves and subclavian vessels) as they pass through the narrow space between the collarbone (clavicle) and the 1st rib.
BruceBlaus, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
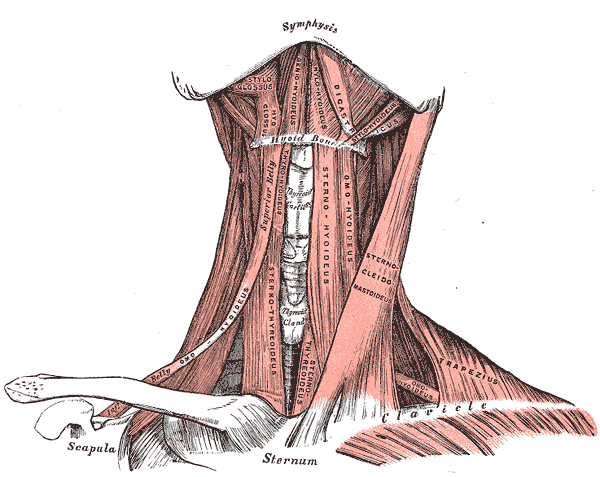
Anterior Neck Muscles and Related Structures. This illustration shows the suprahyoid, infrahyoid, styloglossus, hyoglossus, geniohyoideus, mylohyoideus, digastricus, stylohyoideus, omohyoideus, sternothyroideus, sternohyoideus, omohyoideus, sternocleidomastoideus, trapezius, and omohyoideus muscles. The mandibular symphysis, thyroid cartilage, thyroid gland, hyoid bone, clavicles, scapula, and sternum are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
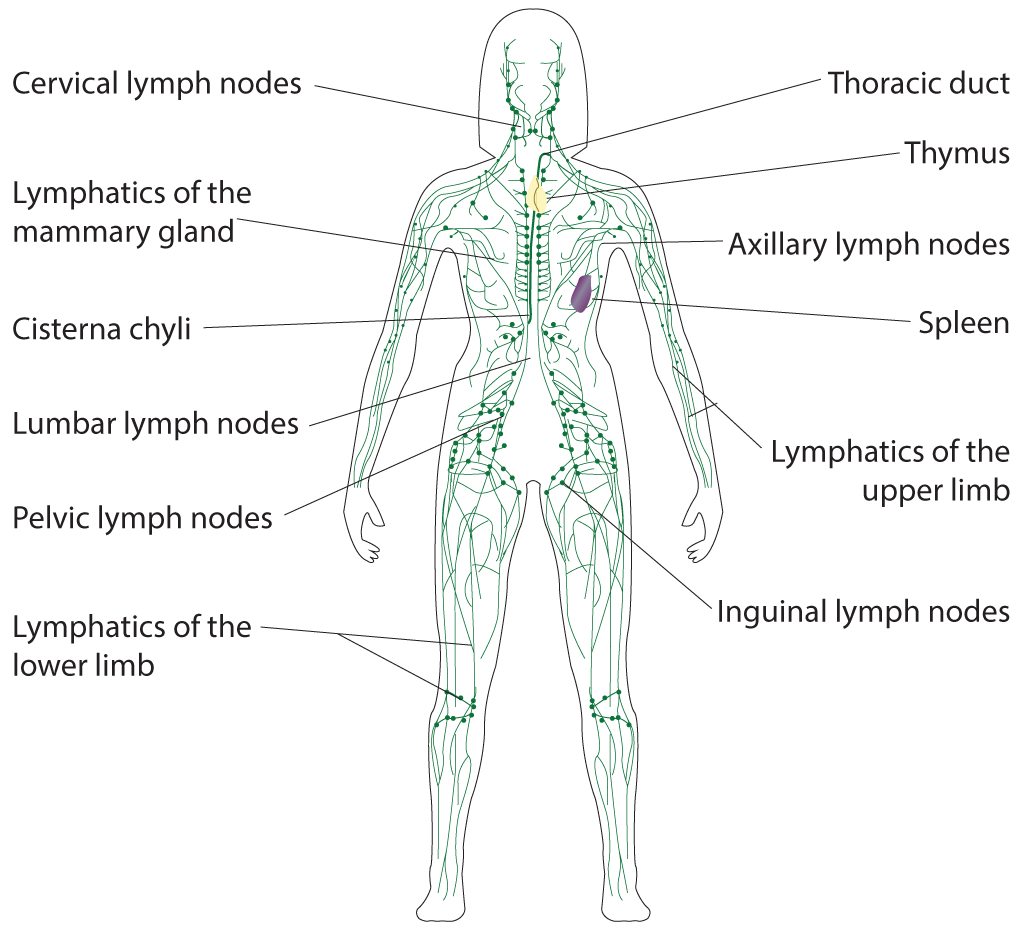
Lymphatic System. Illustrated anatomy includes the cervical lymph nodes, lymphatics of the mammary gland, cisterna chyli, lumbar lymph nodes, pelvic lymph nodes, lymphatics of the lower limb, thoracic duct, thymus, axillary lymph nodes, spleen, lymphatics of the upper limb, and inguinal lymph nodes.
Illustrated by B Parker
References
Kohan EJ, Wirth GA. Anatomy of the neck. Clinics in plastic surgery. 2014 Jan:41(1):1-6. doi: 10.1016/j.cps.2013.09.016. Epub [PubMed PMID: 24295343]
Ahmed AS, Lafosse T, Graf AR, Karzon AL, Gottschalk MB, Wagner ER. Modern Treatment of Neurogenic Thoracic Outlet Syndrome: Pathoanatomy, Diagnosis, and Arthroscopic Surgical Technique. Journal of hand surgery global online. 2023 Jul:5(4):561-576. doi: 10.1016/j.jhsg.2022.07.004. Epub 2023 Jan 18 [PubMed PMID: 37521545]
Borthakur D, Kusuma H, Ansari MA. Bilateral Accessory Clavicular Heads of Sternocleidomastoid Stenosing Supraclavicular Fossa in Human: Case Report. Prague medical report. 2025:126(4):246-250. doi: 10.14712/23362936.2025.39. Epub [PubMed PMID: 41480704]
Level 3 (low-level) evidenceJones AS, Paul N, Surendran S, Yacob M, Chandran S, Samarasam I. Thoracic duct visualisation with subcutaneous administration of indocyanine green dye during minimally invasive oesophagectomy. Journal of minimal access surgery. 2026 Mar 19:():. doi: 10.4103/jmas.jmas_243_25. Epub 2026 Mar 19 [PubMed PMID: 41860064]
Lin HW, Lister MT, Deschler DG. Cystic masses of the supraclavicular fossa: clinical features and diagnostic strategies. American journal of otolaryngology. 2010 Nov-Dec:31(6):435-41. doi: 10.1016/j.amjoto.2009.08.008. Epub 2009 Oct 31 [PubMed PMID: 20015800]
Level 3 (low-level) evidenceRaikos A, English T, Agnihotri A, Yousif OK, Sandhu M, Bennetto J, Stirling A. Supraclavicularis proprius muscle associated with supraclavicular nerve entrapment. Folia morphologica. 2014 Nov:73(4):527-30. doi: 10.5603/FM.2014.0081. Epub [PubMed PMID: 25448916]
Porter SB, Garner HW, Schoch BS, Murray PM, Robards CB, Franco MJ. Anomalous Course of the Brachial Plexus Identified During Ultrasound-Guided Brachial Plexus Nerve Block. Turkish journal of anaesthesiology and reanimation. 2022 Aug:50(4):312-314. doi: 10.5152/TJAR.2022.21064. Epub [PubMed PMID: 35979981]
Lee GM, Carroll M, Marquis KM, Walker CM. Lymphatic Drainage of Thoracic and Extrathoracic Malignancies. Radiologic clinics of North America. 2025 Jul:63(4):537-552. doi: 10.1016/j.rcl.2024.12.013. Epub 2025 Feb 13 [PubMed PMID: 40409934]
Nishi T, Hirata R, Tago M. Late Recurrence of Estrogen Receptor-Positive Breast Cancer Presenting as a Golf-Ball-Sized Mass in the Left Supraclavicular Fossa. Clinical case reports. 2025 Oct:13(10):e71088. doi: 10.1002/ccr3.71088. Epub 2025 Oct 8 [PubMed PMID: 41079837]
Level 3 (low-level) evidenceSuzuki T, Kimura H, Matsumura N, Iwamoto T. Surgical Approaches for Thoracic Outlet Syndrome: A Review of the Literature. Journal of hand surgery global online. 2023 Jul:5(4):577-584. doi: 10.1016/j.jhsg.2022.04.007. Epub 2022 May 5 [PubMed PMID: 37521542]
Dawson SE, Gross JN, Berns JM, Weinzerl T, Adkinson JM, Borschel GH. Supraclavicular Approach to the Brachial Plexus. Plastic and reconstructive surgery. Global open. 2023 Jan:11(1):e4771. doi: 10.1097/GOX.0000000000004771. Epub 2023 Jan 23 [PubMed PMID: 36699229]
Al-Hashel JY, El Shorbgy AA, Ahmed SF, Elshereef RR. Early versus Late Surgical Treatment for Neurogenic Thoracic Outlet Syndrome. ISRN neurology. 2013:2013():673020. doi: 10.1155/2013/673020. Epub 2013 Sep 10 [PubMed PMID: 24109518]
Şahin B, Ulusan M, Başaran B, Güneş S, Oymak E, Genç S. Supraclavicular artery island flap for head and neck reconstruction. Acta chirurgiae plasticae. 2021 Summer:63(2):52-56. doi: 10.48095/ccachp202152. Epub [PubMed PMID: 34404217]
Kokot N, Mazhar K, Reder LS, Peng GL, Sinha UK. The supraclavicular artery island flap in head and neck reconstruction: applications and limitations. JAMA otolaryngology-- head & neck surgery. 2013 Nov:139(11):1247-55. doi: 10.1001/jamaoto.2013.5057. Epub [PubMed PMID: 24158458]
Level 2 (mid-level) evidenceSundriyal D, Kumar N, Dubey SK, Walia M. Virchow's node. BMJ case reports. 2013 Sep 12:2013():. doi: 10.1136/bcr-2013-200749. Epub 2013 Sep 12 [PubMed PMID: 24031077]
Level 3 (low-level) evidenceFranzen A, Günzel T, Buchali A, Coordes A. Etiologic and differential diagnostic significance of tumor location in the supraclavicular fossa. The Laryngoscope. 2018 Mar:128(3):646-650. doi: 10.1002/lary.26775. Epub 2017 Jul 20 [PubMed PMID: 28727141]
Ellison E, LaPuerta P, Martin SE. Supraclavicular masses: results of a series of 309 cases biopsied by fine needle aspiration. Head & neck. 1999 May:21(3):239-46 [PubMed PMID: 10208667]
Level 2 (mid-level) evidenceKoeller KK, Alamo L, Adair CF, Smirniotopoulos JG. Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics : a review publication of the Radiological Society of North America, Inc. 1999 Jan-Feb:19(1):121-46; quiz 152-3 [PubMed PMID: 9925396]
Woods RD 2nd, Pearson BW, Weiland LH. Benign cervical cystic teratoma. Otolaryngology. 1978 May-Jun:86(3 Pt 1):ORL468-72 [PubMed PMID: 112538]
Level 3 (low-level) evidenceJain A, Anand K, Singla S, Kumar A. Congenital cystic lung diseases. Journal of clinical imaging science. 2013:3():5. doi: 10.4103/2156-7514.106620. Epub 2013 Jan 30 [PubMed PMID: 23607074]
Kim SC, Gräff I, Weber S. A Supraclavicular Fossa Ultrasound Window for Central Venous Catheter Positioning. Anesthesia and analgesia. 2017 Apr:124(4):1374-1375. doi: 10.1213/ANE.0000000000001920. Epub [PubMed PMID: 28319555]
Vermeylen K, Engelen S, Sermeus L, Soetens F, Van de Velde M. Supraclavicular brachial plexus blocks: review and current practice. Acta anaesthesiologica Belgica. 2012:63(1):15-21 [PubMed PMID: 22783706]
Kao YJ, Hsu WL, Chen YC, Lo WC, Cheng PC, Liao LJ. Clinical Characteristics and Survival Analysis of Patients with Supraclavicular Fossa Lymphadenopathy. Diagnostics (Basel, Switzerland). 2025 Jun 11:15(12):. doi: 10.3390/diagnostics15121480. Epub 2025 Jun 11 [PubMed PMID: 40564800]
Zhang B, Zhang H, Chen Y, Xia W, Wang Y. Supraclavicular lymph node metastasis in esophageal carcinoma: a topic of ongoing controversy. Frontiers in oncology. 2025:15():1527625. doi: 10.3389/fonc.2025.1527625. Epub 2025 Jan 27 [PubMed PMID: 39931082]
Level 3 (low-level) evidenceGarcía RLB, Jimenez J, Vargas N, Granados Á. Phrenic nerve schwannoma as an incidental intraoperative finding. Case report. International journal of surgery case reports. 2022 Feb:91():106783. doi: 10.1016/j.ijscr.2022.106783. Epub 2022 Jan 24 [PubMed PMID: 35101715]
Level 3 (low-level) evidenceTung-Chen Y, Marín-Baselga R, Tejada-Sorados R, Enfedaque-Castilla I. The use of ultrasound in the emergency department for the detection of thoracic outlet syndrome: A single case study. Ultrasound (Leeds, England). 2021 Feb:29(1):64-66. doi: 10.1177/1742271X20941174. Epub 2020 Jul 14 [PubMed PMID: 33552230]
Level 3 (low-level) evidence