 Anatomy, Shoulder and Upper Limb, Hand Extensor Pollicis Longus Muscle
Anatomy, Shoulder and Upper Limb, Hand Extensor Pollicis Longus Muscle
Introduction
An important contributor to thumb function, the extensor pollicis longus (EPL) muscle is an extrinsic thumb muscle that extends and adducts the thumb metacarpophalangeal (MCP) and interphalangeal joints (see Image. Extensor Pollicis Longus). The EPL is innervated by the posterior interosseous nerve (PIN) and receives arterial supply from the anterior interosseous artery (AIA), posterior interosseous artery (PIA), radial artery, and ulnar artery.
EPL variants are rare, with a prevalence of approximately 1%. The EPL tendon is associated with pathologies ranging from stenosing tenosynovitis to spontaneous tendon rupture.[1] These pathologies are often associated with medical comorbidities (eg, rheumatoid arthritis) or occur as sequelae of trauma (eg, distal radius fractures).[2][3] In the latter context, spontaneous rupture of the EPL may occur in up to 5% of adults following a nondisplaced distal radius fracture or in pediatric patients after dorsal plating for a displaced distal radius fracture. Overall, a thorough understanding of the EPL is essential for accurate characterization of relevant anatomy and associated pathologies, particularly those affecting dynamic thumb function.[4][5]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The EPL is an extrinsic thumb muscle within the deep dorsal forearm muscle group. The EPL originates from the middle 1/3 of the posterior ulnar diaphysis, traverses laterally along the forearm, passes over the Lister tubercle, courses through the 3rd osteofibrous tunnel, and travels superior to the extensor carpi radialis longus (ECRL) and brevis (ECRB) before inserting on the base of the distal phalanx of the pollex (see Image. Dorsal View of Hand Skeletal Anatomy and Surface Markings). An osteofibrous tunnel is a passageway located at synovial joints, characterized by a bony floor and a fascial roof, with transversely oriented fascia that stabilizes neurovascular structures and tendons. These tunnels are also termed "extensor compartments." The EPL is the sole occupant of the 3rd extensor compartment. A total of 6 extensor compartments are present at the wrist.[6][7]
At the wrist, the muscle belly transitions into a tendon surrounded by a synovial sheath, forming the medial border of the anatomical snuffbox (see Image. Anatomical Snuff Box and Ulnar Styloid Process). The tendon divides into proximal and distal tendinous segments separated by a fenestra. The total tendon length ranges from 6.7 to 9.7 cm, and the fenestra measures 3.1 to 3.5 cm in length. The anatomical snuffbox is formed by 3 tendons, arranged from medial (ulnar) to lateral (radial), as follows:
- EPL tendon
- Extensor pollicis brevis (EPB) tendon
- Abductor pollicis longus (APL) tendon
The floor of the anatomical snuffbox is formed by the scaphoid and trapezium bones and the ECRL and ECRB tendons.[8][9][10] The anatomical snuffbox contains the radial artery, radial nerve, and cephalic vein. The sagittal band provides stabilization of the EPL tendon as it crosses the 1st MCP joint dorsally. The sagittal band is U-shaped and consists of radial and ulnar components. The radial component originates from the palmar aspect of the MCP joint via the abductor pollicis brevis (APB) tendon, and the ulnar component originates from the palmar aspect of the MCP joint via the adductor pollicis tendon.[11] Although both components attach directly to the EPL, the radial component of the sagittal band is more critical for EPL stabilization, and injury to this component correlates with EPL instability.[12][13]
The EPL extends the interphalangeal joint of the thumb, along with the MCP joint of the thumb. The muscle also contributes to thumb adduction as it courses within the 3rd wrist extensor compartment. Studies evaluating thumb extension force generation have demonstrated greater force production in a functional position (wrist extension 30°) compared with the neutral wrist position. Male patients generate greater thumb extension force than female patients, and greater force is produced in the dominant hand compared with the nondominant hand. Peak EPL-related thumb extension force occurs during the 3rd decade of life, followed by a progressive decline thereafter.[14]
Embryology
The precursor extensor muscle mass gives rise to the musculature of the forearm through differentiation into 3 portions. The radial portion gives rise to the ECRL, ECRB, and brachioradialis. The superficial portion gives rise to the extensor digitorum communis (EDC), extensor carpi ulnaris (ECU), and extensor digiti minimi (EDM). The deep portion gives rise to the APL, EPB, EPL, and extensor indicis. The radial and superficial portions of the extensor muscle mass are well conserved among different primate species. In contrast, significant variation exists within the deep portion, accounting for the frequent anatomic variations of muscles and tendons in this compartment. EPL variations are rare, with a reported prevalence of approximately 1%.[15]
Blood Supply and Lymphatics
The EPL receives its vascular supply from multiple arterial branches proximodistally. The AIA and its muscular branches perfuse the muscle belly proximal to the musculotendinous junction, prior to encasement by a synovial tendon sheath (see Image. Forearm Arteries). The posterior ramus of the AIA provides arterial supply distal to the musculotendinous junction within the proximal tendon at the level of initial synovial tendon sheath formation, giving rise to branches that penetrate the sheath and supply the tendon. Two to three branches of the posterior ramus course along the tendon margins, while a single branch may supply the central portion.
Arterial supply arises from the dorsal carpal arch at the level of the proximal EPL tendon prior to crossing the 1st metacarpal. The dorsal carpal arch is formed by dorsal carpal branches of the ulnar and radial arteries, with contributions from anastomoses involving the AIA and PIA. The dorsal carpal arch gives rise to 2 arterial branches, 1 supplying the peripheral tendon and 1 extending toward the distal extent of the synovial tendon sheath. Upon reaching the tendon, these branches form a T-shaped configuration, with descending branches directed toward the palmar tendon surface and ascending branches directed dorsally. Anastomosis occurs between the proximal and distal tendon arterial branches.
The radial artery provides direct vascular supply to the distal EPL tendon segment over the 1st metacarpal, where synovial sheath coverage is absent. At the distal tendon segment along the phalanges, perfusion originates from the digital branch of the 1st dorsal metacarpal artery, which branches from the radial artery.[16]
Nerves
The EPL is innervated by a motor branch of the PIN, derived from the nerve's deep branch group (see Image. Nerves of the Posterior Upper Limb). The PIN originates from the radial nerve, which arises from the posterior cord of the brachial plexus (C5–T1). The radial nerve divides into the PIN and the superficial radial nerve near the lateral epicondyle. The PIN supplies the ECRB and supinator muscles, then traverses the supinator for an average length of 4.45 cm before dividing into superficial and deep branches. The superficial branch group innervates the EDC, EDM, and ECU. The deep branch group innervates the APL, EPB, EPL, and extensor indicis.[17][18]
Muscles
Intrinsic thumb muscles include the APB, opponens pollicis, adductor pollicis, and flexor pollicis brevis (FPB). The APB abducts the thumb. The opponens pollicis flexes and abducts the thumb. The adductor pollicis flexes and adducts the thumb. The FPB flexes and adducts the thumb.
Extrinsic thumb muscles include the EPL, EPB, APL, and flexor pollicis longus (FPL). The EPL extends and adducts the thumb. The EPB extends and slightly abducts the thumb. The APL extends and abducts the thumb. The FPL flexes the thumb.[19]
The deep muscle group of the dorsal forearm consists of the EPL, EPB, APL, extensor indicis, and supinator. The EPL extends and adducts the thumb. The EPB extends the thumb. The APL abducts the thumb. The extensor indicis extends the 2nd digit. The supinator produces forearm supination.[20]
The superficial muscle group of the dorsal forearm includes the EDC, EDM, ECU, and anconeus (see Image. Forearm Extensor Muscles and Tendons). The EDC extends the 2nd, 3rd, 4th, and 5th digits. The EDM extends the 5th digit. The ECU extends and adducts the wrist. The anconeus extends the forearm and stabilizes the elbow joint.[21] The table below summarizes the classification and primary actions of the intrinsic and extrinsic thumb muscles.
Table. Muscles Moving the Thumb and Other Parts of the Hand
| Muscle Group | Muscle | Primary Action |
| Intrinsic thumb muscles | APB | Abducts the thumb |
| Opponens pollicis | Flexes and abducts the thumb | |
| Adductor pollicis | Flexes and adducts the thumb | |
| FPB | Flexes and adducts the thumb | |
| Extrinsic thumb muscles | EPL | Extends and adducts the thumb |
| EPB | Extends and slightly abducts the thumb | |
| APL | Extends and abducts the thumb | |
| FPL | Flexes the thumb | |
| Deep dorsal forearm muscles | EPL | Extends and adducts the thumb |
| EPB | Extends the thumb | |
| APL | Abducts the thumb | |
| Extensor indicis | Extends the index finger | |
| Supinator | Produces forearm supination | |
| Superficial dorsal forearm muscles | EDC | Extends the 2nd, 3rd, 4th, and 5th digits |
| EDM | Extends the 5th digit | |
| ECU | Extends and adducts the wrist | |
| Anconeus | Extends the forearm and stabilizes the elbow joint |
Physiologic Variants
Anomalies of the EPL may be organized by utilizing the Türker classification. This system categorizes rare variations in the EPL tendon to help surgeons predict and manage atypical anatomical presentations during hand procedures.[22]
Type 1 anomalies of the EPL represent supernumerary variations characterized by duplication or aberrant tendon course and insertion patterns. Type 1A, designated double EPL tendons with separate compartments, is characterized by an additional EPL tendon traversing the 4th dorsal compartment, distinct from the EPL within the 3rd dorsal compartment. The accessory tendon courses parallel to the EPL at the level of the 1st metacarpal midshaft and inserts separately at the base of the distal phalanx of the thumb. Type 1B, defined as double EPL tendons within the same compartment, demonstrates an accessory EPL tendon running parallel to the EPL within the 3rd dorsal compartment. Separate insertion of the accessory tendon occurs at the base of the distal phalanx of the thumb, independent of the primary EPL insertion.
Type 1C, classified as dual origin of the EPL converging into a single insertion, is characterized by an additional EPL tendon traversing the 4th dorsal compartment, distinct from the EPL in the 3rd dorsal compartment. The accessory tendon courses obliquely, becomes parallel to the EPL, and ultimately merges with the distal EPL tendon, resulting in a single insertion site at the distal phalanx of the thumb. Type 1D, designated extensor pollicis tertius, consists of an accessory tendon arising from the 4th dorsal compartment, separate from the EPL in the 3rd dorsal compartment. The tendon courses obliquely, crosses over the extensor carpi radialis tendons and EPL, and inserts at the proximal phalanx of the thumb rather than the distal phalanx.
Type 1E, identified as extensor pollicis et indicis communis, is characterized by an accessory muscle arising from the ulna between the EPL and extensor indicis. The muscle passes through the 4th dorsal compartment, courses parallel to the EPL within the 1st webspace, and bifurcates distally into 2 slips, 1 inserting at the distal phalanx of the thumb and the other into the dorsal extensor hood of the index finger. Type 1F, defined as extracompartimental 2-slip EPL, involves a single EPL muscle belly giving rise to 2 distinct tendinous slips, radial and ulnar. The radial slip courses between the 1st and 2nd dorsal compartments, while the ulnar slip passes superficial to the extensor retinaculum without entering the 3rd dorsal compartment. Both slips run parallel and insert on the distal phalanx of the thumb.
Type 2 anomalies of the EPL represent interconnection variations involving tendinous communication between the EPL and the extensor apparatus of the index finger. Type 2A, classified as an interconnection between the EPL and extensor indicis proprius (EIP), is characterized by a tendinous connection between the EPL and the EIP to the index finger, located proximal to the 1st webspace. Type 2B, identified as an interconnection between the EPL and EDC to the index finger, demonstrates a tendinous connection between the EPL and the EDC to the index finger, proximal to the 1st webspace.
Type 2C, designated interconnection between the EPL and index finger extensor apparatus with an intracompartmental accessory slip, is characterized by an accessory slip of the EPL that accompanies the EPL as both structures emerge from the 3rd dorsal compartment. The accessory slip inserts into the index finger extensor hood, while the EPL inserts on the distal phalanx of the thumb. Type 2D, defined as an interconnection between the EPL and index finger extensor apparatus with an extracompartmental connection, involves the EPL coursing through the 3rd dorsal compartment, followed by emergence from the compartment. A tendinous connection is then established between the EPL and the extensor hood of the index finger, while the EPL maintains its insertion at the distal phalanx of the thumb.
Munn and Gillis reported additional cases of supernumerary EPL tendons and proposed a modification to the existing Türker classification. Type 3 anomalies, classified as multiple accessory tendons, encompass variations involving additional EPL and EIP tendons with distinct or shared compartmental patterns. Type 3A, classified as double EPL tendons with an accessory tendon to the index finger within the same compartment, is characterized by an accessory EPL tendon and accessory EIP tendon coursing together within the 4th dorsal compartment. The accessory EPL tendon inserts at the distal phalanx of the thumb, while the accessory EIP tendon inserts into the extensor hood of the index finger. The native EPL and EIP tendons remain present within their respective 3rd and 4th dorsal compartments.
Type 3B, identified as double EPL tendons with accessory tendons to the index finger in different compartments, demonstrates an accessory EPL tendon located within the 3rd dorsal compartment and an accessory EIP tendon located within the 4th dorsal compartment. The accessory EPL tendon inserts at the distal phalanx of the thumb, while the accessory EIP tendon inserts into the extensor hood of the index finger. The native EPL and EIP tendons remain present within their standard 3rd and 4th dorsal compartments.[23]
Multiple other anatomic variations of the EPL have been described in the literature. The muscle has been reported to course through the 3rd extensor compartment and insert onto the radial aspect of the proximal phalanx of the thumb in an asymptomatic patient with hypoplasia of the thumb musculature. This configuration has been interpreted as a possible adaptive response to absent APL and EPB musculature, with preservation of thumb extension and abduction.
A separate case report has described fusion of the APL and EPB muscle bellies with subsequent separation into distinct tendons. In this variation, the EPL passes beneath the extensor retinaculum into the 1st compartment and attaches to the EPB.[24]
Another reported variation describes the EPL coursing through the 2nd extensor compartment, with the absence of tendinous structures within the 3rd extensor compartment. The exact insertion site of the EPL within the 2nd compartment was not identified. Overall, awareness of rare but clinically significant EPL variations is important for accurate surgical planning and management of wrist and hand pathologies.
Surgical Considerations
Extensor Pollicis Longus Tenosynovitis
EPL stenosing tenosynovitis, a rare condition, typically requires surgical management due to the absence of documented successful nonoperative treatment. Surgical treatment is supported in the literature, with particular emphasis on the prevention of EPL tendon rupture secondary to chronic attritional changes. Complete release of the EPL tendon is necessary during surgical correction, followed by transposition into the subcutaneous tissue on the radial aspect of the Lister tubercle. Transposition of the EPL tendon reduces the recurrence of tenosynovitis, prevents tendon bowstringing, and preserves tendon function.
Distal Radius Fractures
Displaced distal radius fractures requiring open reduction and internal fixation may be managed with either dorsal or volar plating techniques. Dorsal plating is associated with an increased risk of iatrogenic extensor tendon injury within the wrist and hand due to mechanical irritation, with potential progression to EPL tendon rupture. This risk remains clinically relevant despite continued advancement in low-profile dorsal plating systems aimed at reducing extensor tendon complications.[25][26] Anatomic variations of the EPL tendon may also be encountered during dorsal plating of distal radius fractures, necessitating careful surgical dissection to avoid iatrogenic injury.[27]
Tendon Transfers
Patients requiring surgical reconstruction of a ruptured EPL tendon may be candidates for tendon transfer or free tendon grafting. The extensor indicis is commonly used for tendon transfer, while additional options include the palmaris longus, ECRL, ECRB, and APL. Although the palmaris longus tendon is avascular, its use for tendon transfer may help preserve index finger extension strength, which may otherwise decrease following procedures involving the extensor indicis.
Appropriate tensioning of the reconstructed tendon is essential. Excessive tension results in thumb hyperextension with impaired flexion, whereas insufficient tension leads to extension deficit. A described method for estimating appropriate tension involves positioning the hand flat on a table with the forearm pronated and the wrist in neutral alignment, then measuring the vertical distance from the center of the thumbnail edge to the table. A target distance of 2 cm is recommended. If deviation from this measurement is present, the reconstruction should be adjusted or revised to achieve appropriate tension, ensuring maintenance of the intended 2 cm clearance between the thumbnail edge and the table.[28][29]
The sagittal band of the thumb is critical for stabilizing the EPL tendon, with the radial component playing a primary role. Lacerations near the thumb MCP joint may involve disruption of both radial and ulnar components of the sagittal band, as well as injury to adjacent tendinous structures, including the EPL and EPB. Surgical repair of injured structures is essential, particularly when the radial sagittal band is affected, given the structure's key role in EPL stabilization. Failure to repair the radial sagittal band may result in EPL tendon subluxation.
In patients with rheumatoid arthritis, ulnar sagittal band contracture may occur in association with radial sagittal band weakness. This imbalance may result in the development of a boutonnière deformity of the thumb. In early rheumatoid arthritis, surgical release of the contracted ulnar sagittal band combined with augmentation of the radial sagittal band may be performed to address deformity and restore balance across the extensor mechanism.
EPL tendon anomalies are typically asymptomatic and are not associated with deficits in thumb extension or wrist and hand pain. Such anomalies are often identified incidentally during surgical procedures performed for other wrist or hand pathologies. Surgical intervention is not indicated in asymptomatic cases. In symptomatic cases, surgical management may include extensor retinaculum release and excision of the Lister tubercle to reduce EPL tendon compression within the extensor compartment.
Clinical Significance
"Tenosynovitis" refers to inflammation of the synovial tendon sheath surrounding tendons and most commonly involves structures within the 1st extensor compartment of the wrist, including the APL and EPB tendons. Involvement of the remaining extensor compartments is uncommon in patients without rheumatoid arthritis. However, cases of EPL tenosynovitis involving the synovial sheath within the 3rd extensor compartment have been reported.
Patients typically present with nonspecific wrist pain following repetitive wrist or thumb motion, with tenderness along the Lister tubercle and the EPL tendon. Pain may also be elicited with passive motion of the thumb interphalangeal joint. Localization of symptoms to the 3rd extensor compartment may be delayed for several months, making diagnosis challenging.
In reported cases, all patients demonstrated an EPL musculotendinous junction terminating within the 3rd extensor compartment. This anatomic configuration has been suggested to increase susceptibility to tenosynovitis due to a relatively confined compartmental space.
EPL tendon instability may occur secondary to pathologies affecting the extensor hood or the MCP joint. Patients with EPL instability may experience tendon subluxation, resulting in significant discomfort and pain. Treatment of the underlying cause is necessary to alleviate symptoms.[30]
Distal radius fractures account for approximately 1 out of 6 of all fractures treated in the emergency department. An uncommon but well-documented complication of nondisplaced distal radius fractures in adults is EPL rupture occurring several weeks after injury. Proposed mechanisms include hematoma and callus formation at the fracture site, resulting in compression of the 3rd extensor compartment, leading to ischemia, irritation, and degeneration of the EPL tendon and subsequent rupture.
The development of impaired active thumb extension at the MCP and interphalangeal joints with preserved passive range of motion should prompt evaluation of EPL integrity following diagnosis of a distal radius fracture. Limited active extension of the thumb at the MCP and interphalangeal joints with preserved passive motion should include EPL tendon rupture in the differential diagnosis. Patients may report a popping sensation at the time of rupture and may demonstrate tenderness over the Lister tubercle.[31]
Risk factors for EPL rupture in nondisplaced distal radius fractures include fracture lines located distal to the Lister tubercle and variations in Lister tubercle morphology. A higher radial peak relative to the ulnar peak of the Lister tubercle is associated with an increased risk of EPL rupture.[32]
Evaluation for associated congenital syndromes is essential in patients with thumb muscle hypoplasia, which may present with EPL tendon insertion on the radial aspect of the proximal phalanx of the thumb. Reported associations include Fanconi anemia, which presents with pancytopenic anemia; Holt–Oram syndrome, associated with congenital heart defects; Cornelia de Lange syndrome, associated with dwarfism; Okihiro syndrome, associated with impaired eye movement and deafness; VACTERL (vertebral anomalies, anal atresia, cardiac anomalies, tracheoesophageal fistula with or without esophageal atresia, renal anomalies, and limb anomalies) association; and thrombocytopenia with absent radius.
Avulsion fractures of the 2nd metacarpal at the insertion of the ECRL tendon may result in EPL tendon rupture due to displacement of the avulsed fragment if not appropriately stabilized. Surgical management may be required in 2nd metacarpal avulsion fractures involving the ECRL insertion to prevent this complication.[33]
Media
(Click Image to Enlarge)
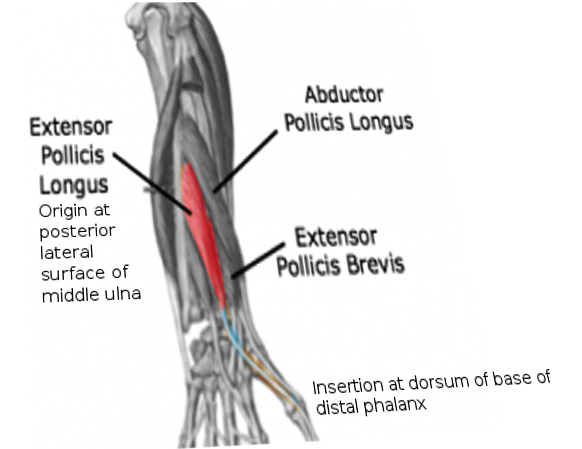
Extensor Pollicis Longus. This diagram illustrates the origin, course, and insertion of the extensor pollicis longus muscle. The image highlights the origin site at the posterolateral surface of the middle ulna and its distal insertion at the base of the distal phalanx of the thumb.
Contributed by O Chaigasame, MD
(Click Image to Enlarge)
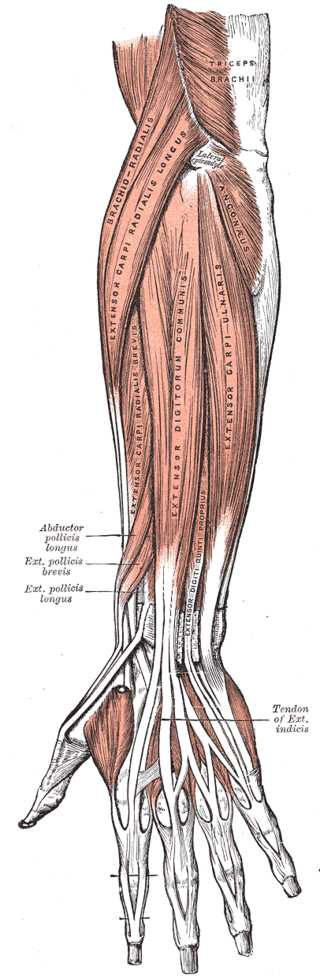
Forearm Extensor Muscles and Tendons. This illustration shows the anatomic relationships between the extensor pollicis longus, extensor indicis, extensor carpi ulnaris, extensor digitorum communis, extensor carpi radialis, extensor carppi radialis longus, extensor carpi radialis brevis, and extensor digiti quinti proprius muscles and tendons. Other upper limb structures in this image include the triceps brachii, lateral epicondyle, and anconeus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
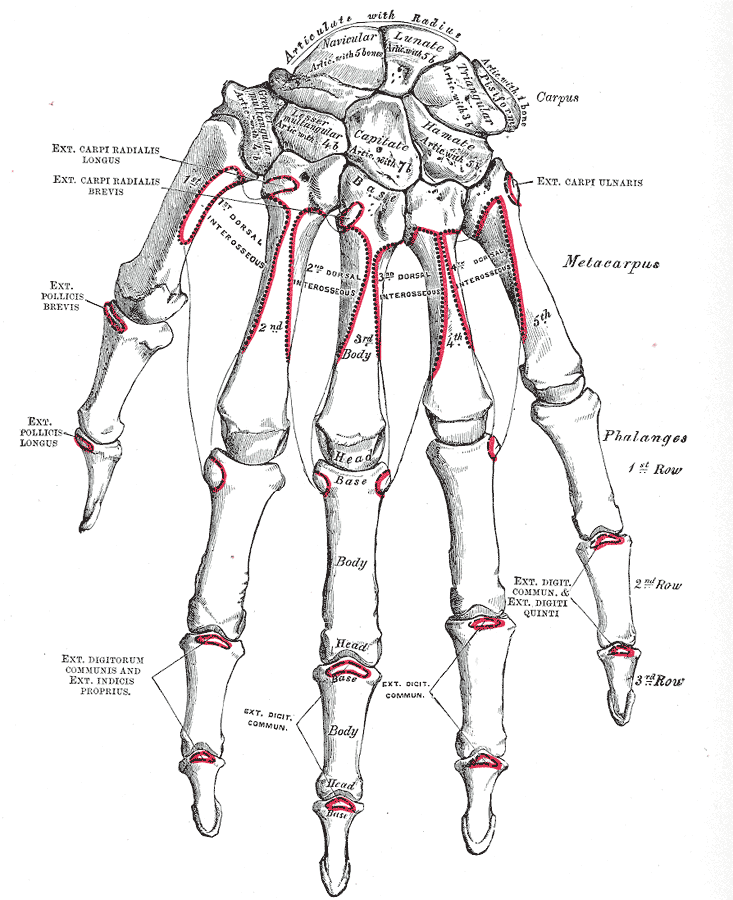
Dorsal View of Hand Skeletal Anatomy and Surface Markings. This anatomical plate illustrates the dorsal aspect of the right hand, including the carpus, metacarpus, and phalanges, with articulation to the radius and detailed visualization of the scaphoid, lunate, pisiform, triquetrum, hamate, capitate, trapezoid, and trapezium bones, as well as the extensor carpi radialis longus, extensor carpi radialis brevis, extensor pollicis brevis, extensor pollicis longus, extensor digitorum communis, extensor indicis proprius, and dorsal interosseous muscles.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
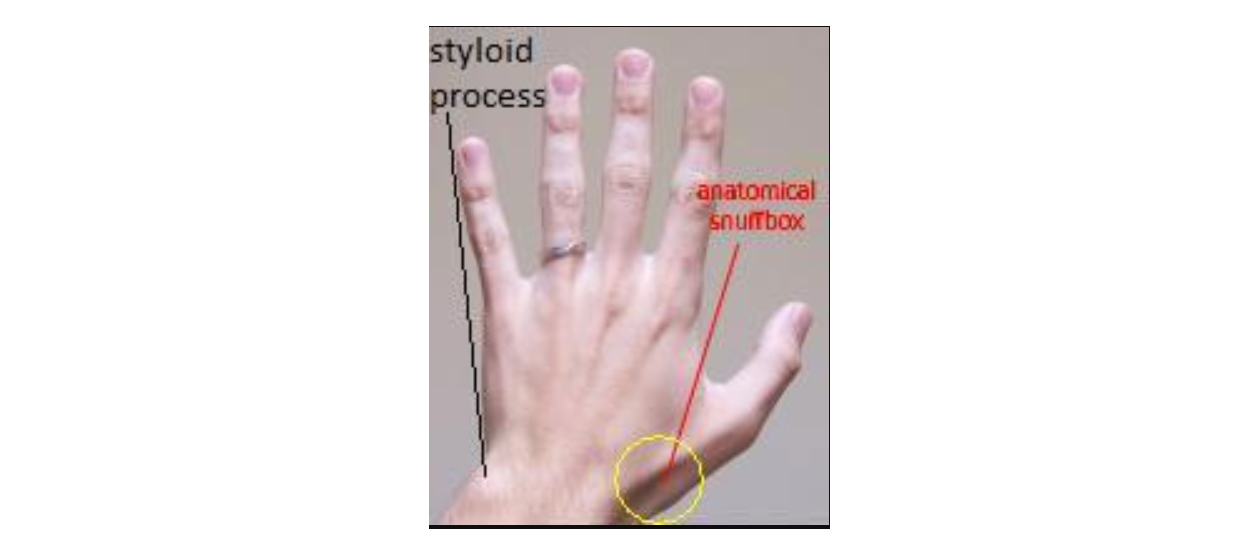
Anatomical Snuff Box and Ulnar Styloid Process. The anatomical snuff box and ulnar styloid process are shown in the image. The boundaries of the anatomical snuff box are the tendons of the abductor pollicis longus and extensor pollicis brevis laterally and the extensor pollicis longus medially.
Mcstrother, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
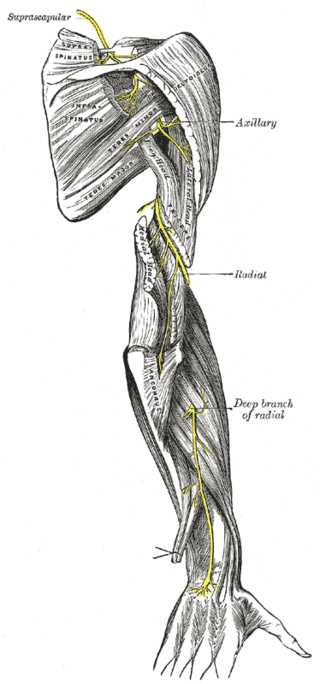
Nerves of the Posterior Upper Limb. This posterior view of the right upper extremity illustrates the distribution of the major nerves. The suprascapular nerve is shown innervating the rotator cuff muscles, while the axillary nerve supplies the deltoid and teres minor. The radial nerve is depicted descending the arm, providing branches to the 3 heads of the triceps brachii and the anconeus, before continuing as the deep branch to supply the posterior compartment of the forearm.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
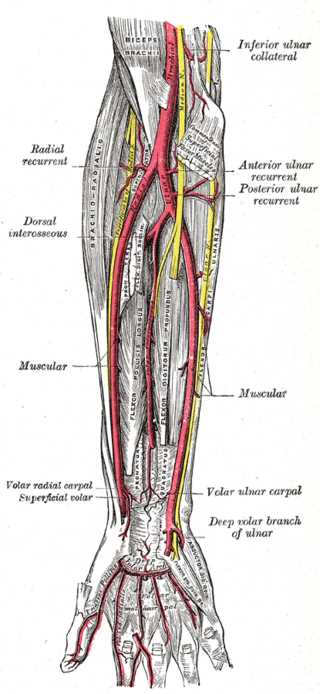
Forearm Arteries. This image highlights the ulnar artery's deep palmar branch and the radial, ulnar, anterior and posterior ulnar recurrent, dorsal interosseous, volar interosseous (termination), dorsal ulnar carpal, dorsal radial carpal arteries, muscular, radial recurrent, volar radial carpal, superficial volar, and volar ulnar carpal arteries. The arm's inferior ulnar collateral and profunda brachii arteries and the ulnar artery's deep volar branch in the hand are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Kardashian G, Vara AD, Miller SJ, Miki RA, Jose J. Stenosing synovitis of the extensor pollicis longus tendon. The Journal of hand surgery. 2011 Jun:36(6):1035-8. doi: 10.1016/j.jhsa.2011.02.004. Epub [PubMed PMID: 21636022]
Hong J, Kim DK, Kang SH, Seo KM. Anomalous course of the extensor pollicis longus with multiple absences of thumb muscles. Annals of rehabilitation medicine. 2013 Feb:37(1):151-5. doi: 10.5535/arm.2013.37.1.151. Epub 2013 Feb 28 [PubMed PMID: 23526731]
Horton TC. Isolated paralysis of the extensor pollicis longus muscle: a further variation of posterior interosseous nerve palsy. Journal of hand surgery (Edinburgh, Scotland). 2000 Apr:25(2):225-6 [PubMed PMID: 11062588]
Level 3 (low-level) evidenceHuang HW, Strauch RJ. Extensor pollicis longus tenosynovitis: a case report and review of the literature. The Journal of hand surgery. 2000 May:25(3):577-9 [PubMed PMID: 10811765]
Level 3 (low-level) evidenceBogart R, Vidlock K. Ruptured Extensor Pollicis Longus Tendon After a Nondisplaced Distal Radius Fracture in a Young Adult Soccer Player. Clinical journal of sport medicine : official journal of the Canadian Academy of Sport Medicine. 2020 Jan:30(1):e23-e24. doi: 10.1097/JSM.0000000000000708. Epub [PubMed PMID: 30550417]
Martinoli C, Bianchi S, Gandolfo N, Valle M, Simonetti S, Derchi LE. US of nerve entrapments in osteofibrous tunnels of the upper and lower limbs. Radiographics : a review publication of the Radiological Society of North America, Inc. 2000 Oct:20 Spec No():S199-213; discussion S213-7 [PubMed PMID: 11046171]
Kim YJ, Lee JH, Baek JH. Variant course of extensor pollicis longus tendon in the second wrist extensor compartment. Surgical and radiologic anatomy : SRA. 2016 May:38(4):497-9. doi: 10.1007/s00276-015-1541-5. Epub 2015 Aug 8 [PubMed PMID: 26253859]
Tang A, Varacallo MA. Anatomy, Shoulder and Upper Limb, Hand Carpal Bones. StatPearls. 2026 Jan:(): [PubMed PMID: 30571003]
Hayat Z, Varacallo MA. Scaphoid Wrist Fracture. StatPearls. 2026 Jan:(): [PubMed PMID: 30725592]
Lane R, Tafti D, Varacallo MA. Scapholunate Advanced Collapse. StatPearls. 2026 Jan:(): [PubMed PMID: 30725809]
Acosta JR, Graefe SB, Varacallo MA. Anatomy, Shoulder and Upper Limb, Hand Adductor Pollicis. StatPearls. 2026 Jan:(): [PubMed PMID: 30252315]
Hallett Reid S, Jozsa F, Ashurst JV. Anatomy, Shoulder and Upper Limb: Hand Anatomical Snuff Box. StatPearls. 2026 Jan:(): [PubMed PMID: 29489241]
Jaibaji M, Rayan GM, Chung KW. Functional anatomy of the thumb sagittal band. The Journal of hand surgery. 2008 Jul-Aug:33(6):879-84. doi: 10.1016/j.jhsa.2008.01.039. Epub [PubMed PMID: 18656759]
Sarigiannis CN, Andreasson I, Ekström L, Ullman M, Björkman A. Normative data on extensor pollicis longus force, lift-off height, and tendon gliding amplitude. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2026 Mar 3:():. pii: S0894-1130(25)00209-1. doi: 10.1016/j.jht.2025.12.010. Epub 2026 Mar 3 [PubMed PMID: 41781311]
Tordjman D, Pierrart J, Bellity J, Delgrande D, Masmejean E. Accessory extensor pollicis longus: A rare tendon anomaly. Hand surgery & rehabilitation. 2018 Feb:37(1):60-63. doi: 10.1016/j.hansur.2017.10.234. Epub 2017 Dec 14 [PubMed PMID: 29248395]
Zbrodowski A, Gajisin S, Grodecki J. Vascularization of the tendons of the extensor pollicis longus, extensor carpi radialis longus and extensor carpi radialis brevis muscles. Journal of anatomy. 1982 Sep:135(Pt 2):235-44 [PubMed PMID: 7174499]
Zhang L, Dong Z, Zhang CL, Gu YD. Surgical Anatomy of the Radial Nerve at the Elbow and in the Forearm: Anatomical Basis for Intraplexus Nerve Transfer to Reconstruct Thumb and Finger Extension in C7 - T1 Brachial Plexus Palsy. Journal of reconstructive microsurgery. 2016 Nov:32(9):670-674 [PubMed PMID: 27351936]
Gragossian A, Varacallo MA. Radial Nerve Injury. StatPearls. 2026 Jan:(): [PubMed PMID: 30725989]
Smutz WP, Kongsayreepong A, Hughes RE, Niebur G, Cooney WP, An KN. Mechanical advantage of the thumb muscles. Journal of biomechanics. 1998 Jun:31(6):565-70 [PubMed PMID: 9755041]
Precerutti M, Garioni E, Ferrozzi G. Dorsal forearm muscles: US anatomy Pictorial Essay. Journal of ultrasound. 2010 Jun:13(2):66-9. doi: 10.1016/j.jus.2010.07.007. Epub 2010 Jul 24 [PubMed PMID: 23396199]
Javed O, Maldonado KA, Ashmyan R. Anatomy, Shoulder and Upper Limb, Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 29494017]
Türker T, Robertson GA, Thirkannad SM. A classification system for anomalies of the extensor pollicis longus. Hand (New York, N.Y.). 2010 Dec:5(4):403-7. doi: 10.1007/s11552-010-9273-9. Epub 2010 May 21 [PubMed PMID: 22131923]
Munn A, Gillis J. Accessory Extensor Pollicis Longus Tendon Classification Modification. Journal of hand surgery global online. 2024 Jan:6(1):114-116. doi: 10.1016/j.jhsg.2023.10.005. Epub 2023 Nov 18 [PubMed PMID: 38313616]
Rosa RC, de Oliveira KM, Léo JA, Elias BA, Dos Santos PR, de Santiago HA. Anomalous bilateral contribution of extensor pollicis longus and muscle fusion of the first compartment of the wrist. Revista brasileira de ortopedia. 2016 Mar-Apr:51(2):235-8. doi: 10.1016/j.rboe.2016.02.008. Epub 2016 Feb 26 [PubMed PMID: 27069895]
Yu YR, Makhni MC, Tabrizi S, Rozental TD, Mundanthanam G, Day CS. Complications of low-profile dorsal versus volar locking plates in the distal radius: a comparative study. The Journal of hand surgery. 2011 Jul:36(7):1135-41. doi: 10.1016/j.jhsa.2011.04.004. Epub [PubMed PMID: 21712136]
Level 2 (mid-level) evidenceDevaux N, Henning J, Haefeli M, Honigmann P. The Retinaculum Flap for Dorsal Fixation of Distal Radius Fractures. The Journal of hand surgery. 2018 Apr:43(4):391.e1-391.e7. doi: 10.1016/j.jhsa.2018.01.011. Epub [PubMed PMID: 29618418]
Le LT, Butcher B, Loewenstein SN. Accessory Extensor Pollicis Longus Tendon Incidentally Discovered During Dorsal Distal Radius Plating. Journal of hand surgery global online. 2024 Jan:6(1):126-129. doi: 10.1016/j.jhsg.2023.10.010. Epub 2023 Dec 3 [PubMed PMID: 38313623]
Kamoi F, Kondo M, Hayashi M, Uchiyama S, Kato H. A new technique to determine the tension in extensor pollicis longus reconstruction. The Journal of hand surgery, European volume. 2019 Oct:44(8):790-794. doi: 10.1177/1753193419845281. Epub 2019 May 2 [PubMed PMID: 31046534]
Jerome JTJ. Dual-Tendon Transfer for Chronic Extensor Pollicis Longus Ruptures: Augmented Extensor Indicis Proprius Transfer with Proximal EPL Stump Lengthening. JBJS essential surgical techniques. 2025 Jul-Sep:15(3):. doi: 10.2106/JBJS.ST.24.00044. Epub 2025 Sep 9 [PubMed PMID: 40917992]
Feltrin M, Dinh A. Nontraumatic Extensor Pollicis Longus Snapping: Report of 2 Cases. JBJS case connector. 2025 Oct 1:15(4):. doi: e25.00032. Epub 2025 Oct 31 [PubMed PMID: 41171949]
Level 3 (low-level) evidenceKitridis D, Bei G, Dogramatzis K, Givissis P. Death of an Extensor Pollicis Longus due to a Funeral. Journal of orthopaedic case reports. 2018 Sep-Oct:8(5):89-91. doi: 10.13107/jocr.2250-0685.1228. Epub [PubMed PMID: 30740386]
Level 3 (low-level) evidenceSaito T, Furutani T, Nakamichi R, Nakahara R, Kondo H, Shimamura Y, Imatani J, Ozaki T. Risk factors for extensor pollicis longus tendon rupture following non-displaced distal radius fractures. Injury. 2025 Aug:56(8):112454. doi: 10.1016/j.injury.2025.112454. Epub 2025 May 24 [PubMed PMID: 40449182]
Cassell OC, Vidal P. An unreported cause of rupture of the extensor pollicis longus tendon. Journal of hand surgery (Edinburgh, Scotland). 1996 Oct:21(5):640-1 [PubMed PMID: 9230951]
Level 3 (low-level) evidence