 Anatomy, Bony Pelvis and Lower Limb, Hamstring Muscle
Anatomy, Bony Pelvis and Lower Limb, Hamstring Muscle
Introduction
The hamstring muscle complex occupies the posterior compartment of the thigh and comprises 3 individual muscles: the biceps femoris (including the long and short heads), semitendinosus, and semimembranosus (see Image. Hamstring Muscles). This muscle group plays a critical role in activities, ranging from upright posture to high-velocity movements such as sprinting and jumping. The region demonstrates a characteristic fusiform-to-elongated contour with a prominent proximal muscular bulk and tapering distal tendinous components. The structural organization of the hamstrings reflects the long muscle bellies arising from the ischial tuberosity, the parallel fiber orientation optimized for force generation and hip extension, and the convergence into cord-like tendons crossing the knee joint.
Hamstring injuries are common in both elite and amateur athletic populations, with management strategies ranging from conservative therapy to operative fixation. Intact hamstring tendons exhibit substantial tensile strength and are frequently harvested as autografts in knee ligament reconstruction procedures.
Knowledge of hamstring anatomy and function enables accurate injury localization, appropriate grading of musculotendinous pathology, and informed selection of management strategies. An understanding of origin, insertion, innervation, and biomechanical role facilitates distinction between muscle strain, tendon avulsion, and apophyseal injury on clinical examination and imaging. Functional insight into hip extension and knee flexion during high-speed activities supports risk assessment, surgical planning, graft selection, and rehabilitation design, thereby reducing complications and recurrence rates while optimizing return-to-activity outcomes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The hamstring complex consists of the biceps femoris (long and short heads), semitendinosus, and semimembranosus muscles.[1][2] Key structural and functional properties are outlined in the table below.
|
Muscle |
Origin |
Insertion |
Primary Function |
Innervation |
Vascular Supply |
|
Biceps femoris (short head) |
Lateral lip of the linea aspera |
Fibular head and lateral condyle of the tibia |
Knee flexion; lateral rotation of the tibia |
Common fibular (peroneal) nerve |
Perforating branches of the deep femoral artery |
|
Biceps femoris (long head) |
Ischial tuberosity |
Fibular head and lateral condyle of the tibia |
Knee flexion; lateral rotation of the tibia; hip extension |
Tibial nerve |
Perforating branches of the deep femoral artery |
|
Semitendinosus |
Lower medial surface of the ischial tuberosity |
Medial tibia (pes anserinus) |
Knee flexion; hip extension; medial rotation of the tibia (with knee flexion) |
Tibial nerve |
Perforating branches of the deep femoral artery |
|
Semimembranosus |
Ischial tuberosity |
Medial tibial condyle |
Knee flexion; hip extension; medial rotation of the tibia (with knee flexion) |
Tibial nerve |
Perforating branches of the deep femoral artery |
Originating at the pelvis and running posteriorly along the femur, most muscles of the hamstring complex cross both the femoroacetabular and tibiofemoral joints. The short head of the biceps femoris is an exception, arising from the lateral lip of the femoral linea aspera, distal to the femoroacetabular joint. The proximal long head of the biceps femoris and the semitendinosus are connected by an aponeurosis extending approximately 7 cm from the ischial tuberosity. The distal hamstrings define the upper boundaries of the popliteal fossa, with the biceps femoris positioned superolaterally and the semimembranosus and semitendinosus located superomedially. The gastrocnemius forms the lower boundary.[3]
Hamstrings facilitate hip extension by extending the femur posteriorly and knee flexion by flexing the tibia and fibula backward. During the gait cycle, activation occurs in the final 25% of the swing phase, generating hip extension force and resisting knee extension. The hamstrings also serve as dynamic stabilizers of the knee joint. In conjunction with the anterior cruciate ligament (ACL), these muscles resist anterior tibial translation during heel strike.[4]
The longest muscle within the group is the semitendinosus, averaging 44.3 cm, followed by the long head of the biceps femoris at 42.0 cm. The semimembranosus and the short head of the biceps femoris measure an average of 38.7 cm and 29.7 cm, respectively (see Image. Muscles of the Hip and Thigh).[5]
Embryology
The 3 hamstring muscles, like all skeletal muscle tissue, develop from the embryonic mesoderm, specifically from hypaxial muscle progenitor cells originating in the dermomyotome. The initial limb bud arises from the lateral plate mesoderm.[6] Between weeks 5 and 7 of embryogenesis, these migrating cells accumulate in the posterior compartment of the thigh, where mesodermal cells differentiate into myoblasts, which proliferate and fuse to form functional muscle tissue.[7] By week 8, individual hamstring muscles are distinguishable, and anatomic relationships to the femur and sciatic nerve are established.
Muscle separation and maturation progress from superficial to deep layers, representing the adult configuration during early fetal development.[8][9] Local signaling factors and myogenic regulatory genes regulate this complex migration and formation of embryonic components.[10]
Blood Supply and Lymphatics
The hamstring muscle complex receives its primary vascular supply from branches of the profunda femoris artery, a branch of the deep femoral artery, with additional contributions from the inferior gluteal artery.[11][12] The inguinal ligament demarcates the transition between the external iliac and femoral arteries (see Image. Branches of the Femoral Artery). These blood vessels supply the semitendinosus, semimembranosus, and long head of the biceps femoris as they course through the posterior compartment of the thigh. The short head of the biceps femoris receives blood from the profunda femoris artery and the popliteal artery in its distal distribution.[13]
The deep veins of the thigh correspond to the major arteries with which they course. The femoral vein provides primary venous drainage of the thigh, accompanies the femoral artery, and receives additional drainage from the profunda femoris vein. At the level of the inguinal ligament, the femoral vein transitions into the external iliac vein.
Lymphatic drainage of the hamstring complex occurs through both superficial and deep pathways. Superficial lymphatic vessels in the posterior thigh drain toward the superficial inguinal lymph nodes, with some flow passing through the popliteal nodes before reaching the inguinal region.[14] Deep lymphatic vessels accompany the profunda femoris and popliteal vessels, draining the muscle compartment and reaching the deep inguinal lymph nodes.[15]
Nerves
The hamstring muscle complex is supplied by nerves originating from the lumbar and sacral plexuses. These plexuses give rise to the sciatic nerve, formed by the ventral rami of spinal nerved from L4 to S3. The sciatic nerve exits the pelvis via the greater sciatic foramen, typically inferior to the piriformis muscle, and descends through the posterior thigh. At the level of the tibiofemoral joint, the sciatic nerve bifurcates into the tibial and common fibular (peroneal) nerves.[16]
The tibial nerve supplies the semimembranosus, semitendinosus, and long head of the biceps femoris, while the common fibular nerve innervates the short head of the biceps femoris (see Image. Posterior Thigh Musculature Dissection in a Newborn). Semitendinosus and the long head of the biceps femoris receive 2 branches, whereas the semimembranosus and the short head of the biceps femoris typically receive a single branch, although anatomical variations are observed.[17]
Physiologic Variants
Although uncommon, anatomical variations of the hamstring musculature require clinical recognition, particularly for surgical planning. The hamstring group, excluding the short head of the biceps femoris, typically originates from a conjoint tendon at the ischial tuberosity. Variations have been reported in which the semitendinosus and long head of the biceps femoris arise from distinct tendinous origins. Additional anomalies include a 3rd head of the biceps femoris and an accessory muscle inserting into the semimembranosus.[18]
A rare variant involves bilateral absence of the semimembranosus, identified incidentally on magnetic resonance imaging in a patient evaluated for knee pain following a fall.[19] Although the report did not attribute prior symptoms to this anomaly, such findings may be clinically significant in the context of ACL reconstruction, where hamstring autografts are commonly employed.
Anatomical variations of the hamstring complex may predispose to neuropathic complications. Common fibular nerve entrapment most frequently occurs near the fibular head and neck. A 2018 case report described fibular neuropathy associated with an anomalous short head of the biceps femoris, in which the nerve traversed a 4.4-cm tunnel between the gastrocnemius and the short head of the biceps femoris.[20]
Innervation patterns also demonstrate variability, including differing muscle entry points, variable branching, and shared branches between muscles. Muscle vascular supply is generally consistent, although the number and course of perforating branches from the profunda femoris artery vary, with multiple degrees of anastomosis observed between vessels. These anatomical variations hold clinical relevance for injury risk assessment, surgical planning, and rehabilitation strategies.[21]
Surgical Considerations
The majority of hamstring injuries are managed nonoperatively. Hamstring tendon avulsions frequently require surgical repair, typically performed using endoscopic fixation of the avulsed tendon to the ischial tuberosity.[22] Chronic proximal hamstring ruptures may necessitate augmentation with an Achilles tendon autograft during surgical reconstruction.[23]
Ischial apophyseal avulsion fractures are uncommon, representing 1.4% to 4% of all hamstring injuries.[24] Fractures with displacement of less than 1 cm are generally treated conservatively, with avoidance of hamstring stretching to prevent further displacement of the apophyseal fragment.[25] Surgical intervention is indicated in cases of fractures displaced by over 1 cm or symptomatic malunion, with early fixation recommended to reduce the risk of ischiofemoral impingement.[26]
Hamstring tendons are frequently harvested as autografts for ACL reconstruction. A quadruple hamstring autograft, incorporating the semitendinosus and gracilis tendons, is considered among the strongest graft options.[27] Compared with patellar tendon autografts, hamstring autografts are associated with lower rates of donor-site morbidity, including patellofemoral crepitation, kneeling pain, and extension loss exceeding 5°. These autografts carry an increased risk of graft laxity and postoperative hamstring weakness.[28] Long-term comparative outcomes remain inconclusive. Kocher et al reported no significant difference in patient satisfaction between hamstring and patellar tendon grafts for ACL reconstruction.[29]
Clinical Significance
Hamstring strains are among the most common injuries in both elite and recreational athletes, with a high recurrence rate. Approximately 1/3 of athletes sustain reinjury within a year of return to play.[30] Most injuries occur during high-risk activities such as sprinting, where rapid acceleration or deceleration causes excessive muscle elongation. The biceps femoris is the most frequently injured hamstring muscle, followed by the semimembranosus and semitendinosus.[31][32]
Clinically, hamstring injuries present with posterior thigh pain, often exacerbated by knee flexion or hip extension. Severe injuries may produce an audible pop. Differential diagnoses include lumbosacral radiculopathy, adductor strain, and femoral stress fracture.[33]
Hamstring strains are graded according to severity. Grade I injuries involve minimal pain and functional limitation with minor myofibrillar disruption. Grade II injuries consist of partial-thickness musculotendinous tears with pronounced pain and measurable strength loss. Grade III injuries comprise complete tears with severe pain, hematoma, and marked strength deficits. Orthopedic consultation is recommended for Grade III injuries and high-grade partial tears, particularly those affecting the distal tendon.[34]
Initial management in the acute phase emphasizes protection, rest, ice, compression, and elevation (PRICE) to limit swelling and inflammation.[35] Range of motion should be guided by tolerance, as aggressive stretching may promote scar formation.[36] The use of nonsteroidal anti-inflammatory drugs remains controversial. Some studies demonstrate limited benefit or potential adverse effects, although short courses (5–7 days) are generally safe for analgesia.[37][38] Platelet-rich plasma has been investigated as an adjunctive therapy, but current evidence does not indicate a significant benefit in recovery.[39]
Rehabilitation programs should prioritize progressive eccentric strengthening to accelerate recovery and reduce recurrence risk.[40] Exercise protocols must be tailored to the stage of healing and may continue throughout late rehabilitation to maintain protection against reinjury.[41] Although hamstring stretching is commonly incorporated, flexibility training alone has not been shown to reduce recurrence.
Neuromuscular control of the lumbopelvic region is critical for long-term outcomes. A prospective randomized trial demonstrated that athletes completing a progressive agility and trunk stabilization program experienced lower reinjury rates compared with those following standard stretching and strengthening protocols.[42]
Other Issues
Functional Consequences of Below-Knee Amputation on Thigh Musculature
Thigh muscles exhibit significant atrophy and strength deficits after below-knee amputation, with hamstrings often relatively dominant over quadriceps, promoting knee flexion contracture from unopposed pull and altered activation patterns.[43] Increased energy expenditure during prosthetic gait, particularly 10% to 40% higher than nonamputee walking, results from altered mechanics and reliance on proximal musculature. (Source: Huston et al, 1998)
Reduced hamstring and quadriceps strength correlates with asymmetrical gait and compensatory loading of the intact limb, increasing the risk of low back pain and musculoskeletal strain. Early targeted rehabilitation, including hamstring–quadriceps strengthening and contracture-preventive positioning, combined with prosthetic training and core stabilization exercises, improves residual limb function and prosthetic mobility.
The Role of the Hamstrings in the Patellar Reflex
Hamstrings act as antagonists in the patellar reflex, undergoing inhibition to facilitate quadriceps contraction and knee extension (see Image. Patellar Tendon Reflex Arc). Tapping the patellar tendon stretches quadriceps muscle spindles, sending Ia afferents to the spinal cord (L3-L4), where they monosynaptically excite quadriceps motor neurons while polysynaptically activating inhibitory interneurons to suppress hamstring α motor neurons via reciprocal inhibition. This coordinated relaxation prevents opposition, enabling the characteristic kick.
Lower motor neuron lesions cause hyporeflexia or absent knee jerk (Westphal sign) due to quadriceps failure or hamstring disinhibition, producing flaccid weakness, whereas upper motor neuron lesions lead to hyperreflexia and clonus from lost supraspinal control. Hamstring injury or sciatic lesions involving the nerves of L5 to S2 may invert the patellar reflex, signaling focal myelopathy and gait instability.[44][45]
Media
(Click Image to Enlarge)
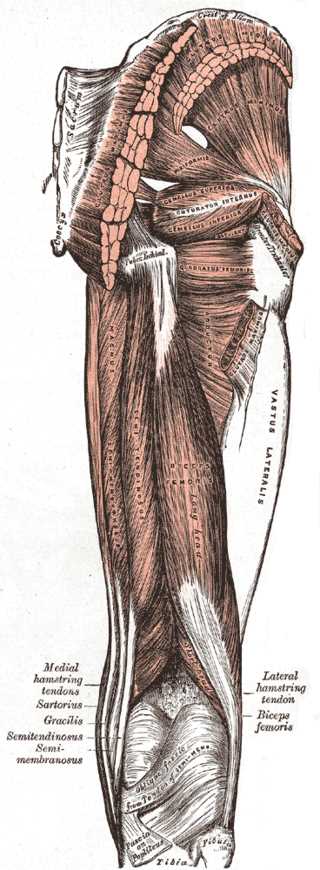
Muscles of the Hip and Thigh. The gluteal muscles include the gluteus maximus, gluteus medius, and gluteus minimus. Hip muscles include the piriformis, gemellus superior, gemellus inferior, and obturator internus. Thigh muscles include the adductor magnus, vastus lateralis, biceps femoris, semitendinosus, hamstring tendons, and gracilis.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
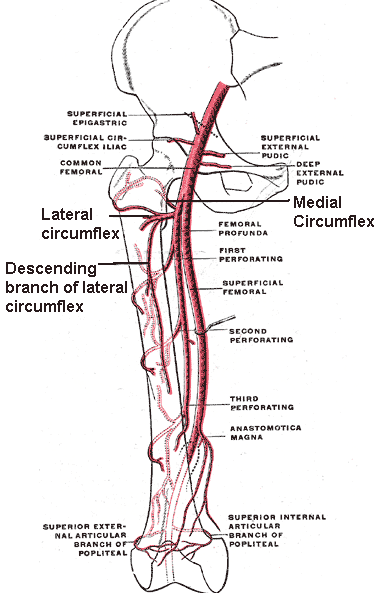
Branches of the Femoral Artery. The illustration depicts the common femoral artery, deep femoral (profunda femoris) artery, superficial femoral artery, perforating arteries, lateral and medial circumflex arteries, descending branch of the lateral circumflex artery, anastomotica magna, and the superior external and internal articular branches of the popliteal artery.
Mikael Häggström, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
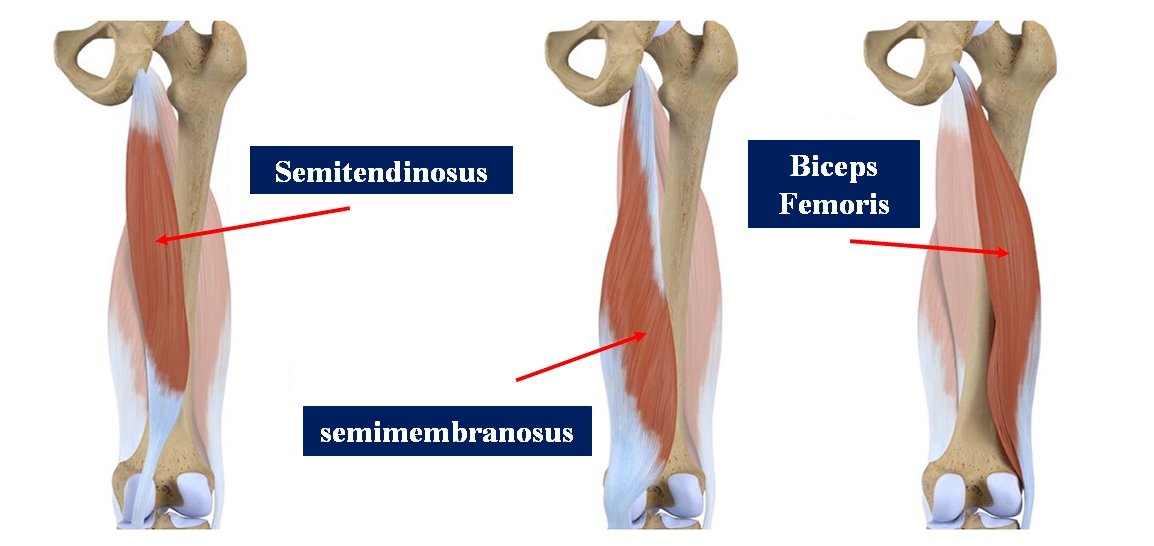
Hamstring Muscles. The image illustrates the individual muscles comprising the posterior compartment of the thigh, including the biceps femoris, semitendinosus, and semimembranosus.
Contributed by B Bordoni, PhD
(Click Image to Enlarge)
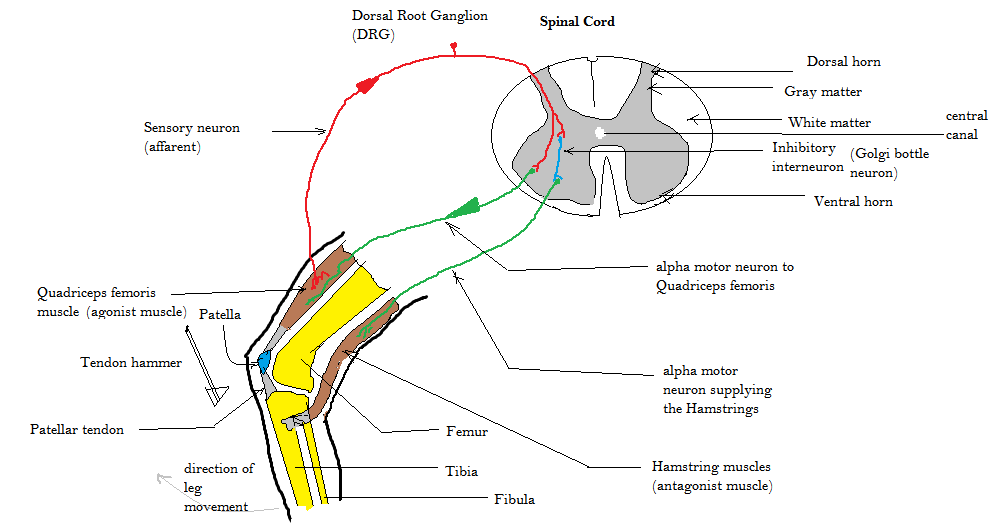
Patellar Tendon Reflex Arc. This diagram illustrates the knee-jerk reflex (red and green arrows) and reciprocal inhibition of the hamstring muscle via an interneuron (blue).
Amiya Sarkar, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
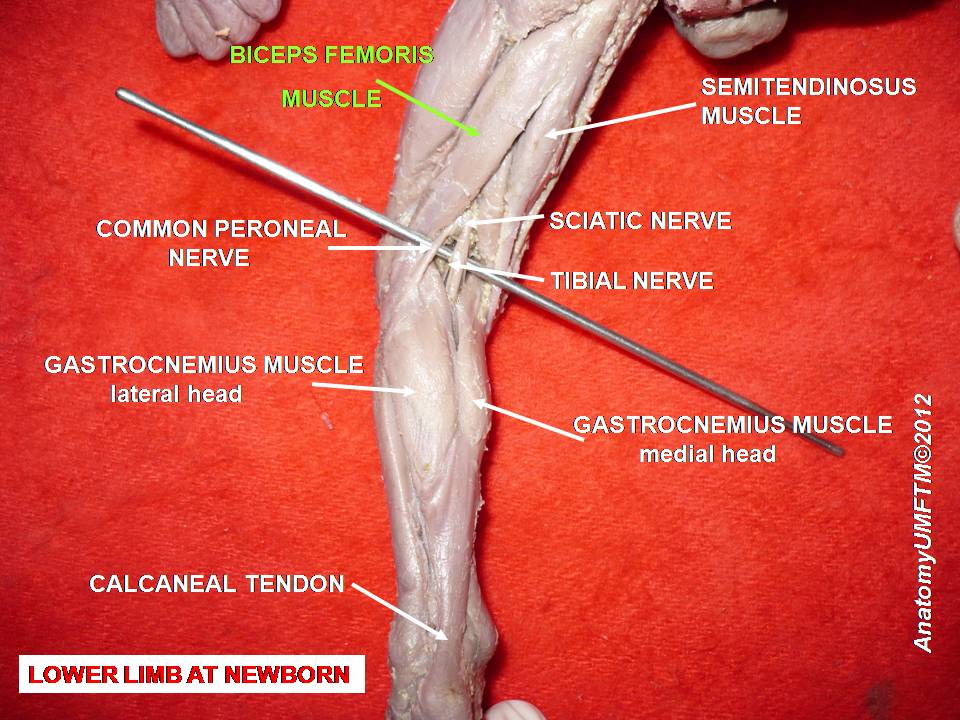
Posterior Thigh Musculature Dissection in a Newborn. Highlighted in this dissection are the primary hamstring muscles of a newborn, including the biceps femoris. Additional structures visible include the sciatic, tibial, and common peroneal nerves, surrounding semitendinosus and semimembranosus, the proximal portions of the gastrocnemius, and the calcaneal tendon.
Anatomist90, Public Domain, via Wikimedia Commons
{kind=link}
References
Woodley SJ, Mercer SR. Hamstring muscles: architecture and innervation. Cells, tissues, organs. 2005:179(3):125-41 [PubMed PMID: 15947463]
Miguel-Pérez M, Iglesias-Chamorro P, Ortiz-Miguel S, Ortiz-Sagristà JC, Möller I, Blasi J, Agullò J, Martinoli C, Pérez-Bellmunt A. Anatomical Relationships of the Proximal Attachment of the Hamstring Muscles with Neighboring Structures: From Ultrasound, Anatomical and Histological Findings to Clinical Implications. Diagnostics (Basel, Switzerland). 2024 Aug 8:14(16):. doi: 10.3390/diagnostics14161725. Epub 2024 Aug 8 [PubMed PMID: 39202213]
Greenwood K, Zyl RV, Keough N, Hohmann E. Defining the popliteal fossa by bony landmarks and mapping of the courses of the neurovascular structures for application in popliteal fossa surgery. Anatomy & cell biology. 2021 Mar 31:54(1):10-17. doi: 10.5115/acb.20.179. Epub [PubMed PMID: 33594009]
Koulouris G, Connell D. Hamstring muscle complex: an imaging review. Radiographics : a review publication of the Radiological Society of North America, Inc. 2005 May-Jun:25(3):571-86 [PubMed PMID: 15888610]
van der Made AD, Wieldraaijer T, Kerkhoffs GM, Kleipool RP, Engebretsen L, van Dijk CN, Golanó P. The hamstring muscle complex. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2015 Jul:23(7):2115-22. doi: 10.1007/s00167-013-2744-0. Epub 2013 Nov 5 [PubMed PMID: 24190369]
Buckingham M, Bajard L, Chang T, Daubas P, Hadchouel J, Meilhac S, Montarras D, Rocancourt D, Relaix F. The formation of skeletal muscle: from somite to limb. Journal of anatomy. 2003 Jan:202(1):59-68 [PubMed PMID: 12587921]
Level 3 (low-level) evidenceTickle C. How the embryo makes a limb: determination, polarity and identity. Journal of anatomy. 2015 Oct:227(4):418-30. doi: 10.1111/joa.12361. Epub 2015 Aug 7 [PubMed PMID: 26249743]
Christ B, Brand-Saberi B. Limb muscle development. The International journal of developmental biology. 2002:46(7):905-14 [PubMed PMID: 12455628]
Warmbrunn MV, de Bakker BS, Hagoort J, Alefs-de Bakker PB, Oostra RJ. Hitherto unknown detailed muscle anatomy in an 8-week-old embryo. Journal of anatomy. 2018 Aug:233(2):243-254. doi: 10.1111/joa.12819. Epub 2018 May 3 [PubMed PMID: 29726018]
Tickle C, Barker H. The Sonic hedgehog gradient in the developing limb. Wiley interdisciplinary reviews. Developmental biology. 2013 Mar-Apr:2(2):275-90. doi: 10.1002/wdev.70. Epub 2012 May 25 [PubMed PMID: 24009037]
Level 3 (low-level) evidenceTomaszewski KA, Henry BM, Vikse J, Pękala P, Roy J, Svensen M, Guay D, Hsieh WC, Loukas M, Walocha JA. Variations in the origin of the deep femoral artery: A meta-analysis. Clinical anatomy (New York, N.Y.). 2017 Jan:30(1):106-113. doi: 10.1002/ca.22691. Epub 2016 Feb 2 [PubMed PMID: 26780216]
Level 1 (high-level) evidenceChoy KW, Kogilavani S, Norshalizah M, Rani S, Aspalilah A, Hamzi H, Farihah HS, Das S. Topographical anatomy of the profunda femoris artery and the femoral nerve: normal and abnormal relationships. La Clinica terapeutica. 2013:164(1):17-9. doi: 10.7417/T.2013.1504. Epub [PubMed PMID: 23455736]
Miller SL, Gill J, Webb GR. The proximal origin of the hamstrings and surrounding anatomy encountered during repair. A cadaveric study. The Journal of bone and joint surgery. American volume. 2007 Jan:89(1):44-8 [PubMed PMID: 17200309]
Pan WR, Wang DG, Levy SM, Chen Y. Superficial lymphatic drainage of the lower extremity: anatomical study and clinical implications. Plastic and reconstructive surgery. 2013 Sep:132(3):696-707. doi: 10.1097/PRS.0b013e31829ad12e. Epub [PubMed PMID: 23985641]
Yamazaki S, Suami H, Imanishi N, Aiso S, Yamada M, Jinzaki M, Kuribayashi S, Chang DW, Kishi K. Three-dimensional demonstration of the lymphatic system in the lower extremities with multi-detector-row computed tomography: a study in a cadaver model. Clinical anatomy (New York, N.Y.). 2013 Mar:26(2):258-66. doi: 10.1002/ca.22179. Epub 2013 Jan 22 [PubMed PMID: 23339085]
Level 3 (low-level) evidenceTomaszewski KA, Graves MJ, Henry BM, Popieluszko P, Roy J, Pękala PA, Hsieh WC, Vikse J, Walocha JA. Surgical anatomy of the sciatic nerve: A meta-analysis. Journal of orthopaedic research : official publication of the Orthopaedic Research Society. 2016 Oct:34(10):1820-1827. doi: 10.1002/jor.23186. Epub 2016 Feb 22 [PubMed PMID: 26856540]
Level 1 (high-level) evidenceFarfán E, Rojas S, Olivé-Vilás R, Rodríguez-Baeza A. Innervation patterns of hamstring muscles, including morphological descriptions and clinical implication. Surgical and radiologic anatomy : SRA. 2024 Jun:46(6):749-760. doi: 10.1007/s00276-024-03371-4. Epub 2024 Apr 23 [PubMed PMID: 38652253]
Chakravarthi K. Unusual unilateral multiple muscular variations of back of thigh. Annals of medical and health sciences research. 2013 Nov:3(Suppl 1):S1-2. doi: 10.4103/2141-9248.121206. Epub [PubMed PMID: 24349835]
Level 3 (low-level) evidenceSussmann AR. Congenital bilateral absence of the semimembranosus muscles. Skeletal radiology. 2019 Oct:48(10):1651-1655. doi: 10.1007/s00256-019-03210-3. Epub 2019 Apr 15 [PubMed PMID: 30982941]
Park JH, Park KR, Yang J, Park GH, Cho J. Unusual variant of distal biceps femoris muscle associated with common peroneal entrapment neuropathy: A cadaveric case report. Medicine. 2018 Sep:97(38):e12274. doi: 10.1097/MD.0000000000012274. Epub [PubMed PMID: 30235672]
Level 3 (low-level) evidenceKellis E. Intra- and Inter-Muscular Variations in Hamstring Architecture and Mechanics and Their Implications for Injury: A Narrative Review. Sports medicine (Auckland, N.Z.). 2018 Oct:48(10):2271-2283. doi: 10.1007/s40279-018-0975-4. Epub [PubMed PMID: 30117053]
Level 3 (low-level) evidenceLempainen L, Banke IJ, Johansson K, Brucker PU, Sarimo J, Orava S, Imhoff AB. Clinical principles in the management of hamstring injuries. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2015 Aug:23(8):2449-2456. doi: 10.1007/s00167-014-2912-x. Epub 2014 Feb 21 [PubMed PMID: 24556933]
Folsom GJ, Larson CM. Surgical treatment of acute versus chronic complete proximal hamstring ruptures: results of a new allograft technique for chronic reconstructions. The American journal of sports medicine. 2008 Jan:36(1):104-9 [PubMed PMID: 18055919]
Level 2 (mid-level) evidenceLiu H, Zhang Y, Rang M, Li Q, Jiang Z, Xia J, Zhang M, Gu X, Zhao C. Avulsion Fractures of the Ischial Tuberosity: Progress of Injury, Mechanism, Clinical Manifestations, Imaging Examination, Diagnosis and Differential Diagnosis and Treatment. Medical science monitor : international medical journal of experimental and clinical research. 2018 Dec 27:24():9406-9412. doi: 10.12659/MSM.913799. Epub 2018 Dec 27 [PubMed PMID: 30589058]
Sherry M. Examination and treatment of hamstring related injuries. Sports health. 2012 Mar:4(2):107-14 [PubMed PMID: 23016076]
Gidwani S, Jagiello J, Bircher M. Avulsion fracture of the ischial tuberosity in adolescents--an easily missed diagnosis. BMJ (Clinical research ed.). 2004 Jul 10:329(7457):99-100 [PubMed PMID: 15242916]
Level 3 (low-level) evidenceFrank RM, Hamamoto JT, Bernardoni E, Cvetanovich G, Bach BR Jr, Verma NN, Bush-Joseph CA. ACL Reconstruction Basics: Quadruple (4-Strand) Hamstring Autograft Harvest. Arthroscopy techniques. 2017 Aug:6(4):e1309-e1313. doi: 10.1016/j.eats.2017.05.024. Epub 2017 Aug 14 [PubMed PMID: 29354434]
Goldblatt JP, Fitzsimmons SE, Balk E, Richmond JC. Reconstruction of the anterior cruciate ligament: meta-analysis of patellar tendon versus hamstring tendon autograft. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2005 Jul:21(7):791-803 [PubMed PMID: 16012491]
Level 1 (high-level) evidenceKocher MS, Steadman JR, Briggs K, Zurakowski D, Sterett WI, Hawkins RJ. Determinants of patient satisfaction with outcome after anterior cruciate ligament reconstruction. The Journal of bone and joint surgery. American volume. 2002 Sep:84(9):1560-72 [PubMed PMID: 12208912]
Level 2 (mid-level) evidenceHeiderscheit BC, Sherry MA, Silder A, Chumanov ES, Thelen DG. Hamstring strain injuries: recommendations for diagnosis, rehabilitation, and injury prevention. The Journal of orthopaedic and sports physical therapy. 2010 Feb:40(2):67-81. doi: 10.2519/jospt.2010.3047. Epub [PubMed PMID: 20118524]
Askling CM, Tengvar M, Saartok T, Thorstensson A. Acute first-time hamstring strains during high-speed running: a longitudinal study including clinical and magnetic resonance imaging findings. The American journal of sports medicine. 2007 Feb:35(2):197-206 [PubMed PMID: 17170160]
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports medicine (Auckland, N.Z.). 2012 Mar 1:42(3):209-26. doi: 10.2165/11594800-000000000-00000. Epub [PubMed PMID: 22239734]
Allahabadi S, Salazar LM, Obioha OA, Fenn TW, Chahla J, Nho SJ. Hamstring Injuries: A Current Concepts Review: Evaluation, Nonoperative Treatment, and Surgical Decision Making. The American journal of sports medicine. 2024 Mar:52(3):832-844. doi: 10.1177/03635465231164931. Epub 2023 Apr 24 [PubMed PMID: 37092718]
Hamilton B, Valle X, Rodas G, Til L, Grive RP, Rincon JA, Tol JL. Classification and grading of muscle injuries: a narrative review. British journal of sports medicine. 2015 Mar:49(5):306. doi: 10.1136/bjsports-2014-093551. Epub 2014 Nov 13 [PubMed PMID: 25394420]
Level 3 (low-level) evidenceBrukner P. Hamstring injuries: prevention and treatment-an update. British journal of sports medicine. 2015 Oct:49(19):1241-4. doi: 10.1136/bjsports-2014-094427. Epub 2015 Jun 23 [PubMed PMID: 26105015]
Järvinen MJ, Lehto MU. The effects of early mobilisation and immobilisation on the healing process following muscle injuries. Sports medicine (Auckland, N.Z.). 1993 Feb:15(2):78-89 [PubMed PMID: 8446826]
Level 3 (low-level) evidenceReynolds JF, Noakes TD, Schwellnus MP, Windt A, Bowerbank P. Non-steroidal anti-inflammatory drugs fail to enhance healing of acute hamstring injuries treated with physiotherapy. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde. 1995 Jun:85(6):517-22 [PubMed PMID: 7652633]
Level 1 (high-level) evidenceMishra DK, Fridén J, Schmitz MC, Lieber RL. Anti-inflammatory medication after muscle injury. A treatment resulting in short-term improvement but subsequent loss of muscle function. The Journal of bone and joint surgery. American volume. 1995 Oct:77(10):1510-9 [PubMed PMID: 7593059]
Level 3 (low-level) evidenceEngebretsen L, Steffen K, Alsousou J, Anitua E, Bachl N, Devilee R, Everts P, Hamilton B, Huard J, Jenoure P, Kelberine F, Kon E, Maffulli N, Matheson G, Mei-Dan O, Menetrey J, Philippon M, Randelli P, Schamasch P, Schwellnus M, Vernec A, Verrall G. IOC consensus paper on the use of platelet-rich plasma in sports medicine. British journal of sports medicine. 2010 Dec:44(15):1072-81. doi: 10.1136/bjsm.2010.079822. Epub [PubMed PMID: 21106774]
Level 3 (low-level) evidenceHickey JT, Opar DA, Weiss LJ, Heiderscheit BC. Hamstring Strain Injury Rehabilitation. Journal of athletic training. 2022 Feb 1:57(2):125-135. doi: 10.4085/1062-6050-0707.20. Epub [PubMed PMID: 35201301]
Brooks JH, Fuller CW, Kemp SP, Reddin DB. Incidence, risk, and prevention of hamstring muscle injuries in professional rugby union. The American journal of sports medicine. 2006 Aug:34(8):1297-306 [PubMed PMID: 16493170]
Level 2 (mid-level) evidenceSherry MA, Best TM. A comparison of 2 rehabilitation programs in the treatment of acute hamstring strains. The Journal of orthopaedic and sports physical therapy. 2004 Mar:34(3):116-25 [PubMed PMID: 15089024]
Level 1 (high-level) evidenceDemir Y, Aydemir K. Gülhane lower extremity amputee rehabilitation protocol: A nationwide, 123-year experience. Turkish journal of physical medicine and rehabilitation. 2020 Dec:66(4):373-382. doi: 10.5606/tftrd.2020.7637. Epub 2020 Nov 9 [PubMed PMID: 33364556]
Rodriguez-Beato FY, De Jesus O. Physiology, Deep Tendon Reflexes. StatPearls. 2026 Jan:(): [PubMed PMID: 32965909]
Falkson SR, Hinson JW. Westphal Sign. StatPearls. 2025 Jan:(): [PubMed PMID: 31985995]