Introduction
The neck contains numerous neurovascular structures organized into defined anatomic compartments. The anterior and posterior triangles represent the principal subdivisions, delineated by consistent surface landmarks (see Image. Superficial Neck Anatomy). Each triangle contains muscles, nerves, arteries, veins, and lymphatics arranged within fascial planes that facilitate surgical orientation and clinical localization. Vascular supply to this region arises primarily from branches of the carotid and subclavian arteries, while innervation derives largely from cranial nerves and the cervical plexus. Documented anatomic variants involve vascular branching patterns, muscular attachments, and nerve courses.
The cervical triangles serve as important clinical landmarks for localizing neurovascular structures, evaluating cervical lymphadenopathy, and identifying the source or spread of head and neck infections and malignancies. Surgical procedures in the neck, including carotid endarterectomy, thyroidectomy, and cervical lymph node dissection, rely on these anatomic divisions to guide safe exposure and avoid injury to critical nerves and vessels. Knowledge of the anatomy and functional relationships within the neck triangles enables clinicians to perform accurate physical examinations, interpret imaging findings, and plan diagnostic or therapeutic interventions with greater precision.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Anterior Triangle
The anterior triangle represents a bilateral anatomic subdivision of the neck located deep to the superficial cervical fascia and the platysma muscle. Laterally, the anterior triangle is bounded by the anterior border of the sternocleidomastoid (SCM) muscle. The superior boundary is the inferior border of the mandible. The medial boundary is the midline of the neck.
The anterior triangle is further divided into 4 subtriangles. The submandibular and submental triangles form the superior divisions, whereas the muscular and carotid triangles constitute the inferior divisions of the anterior neck.[1] The submandibular triangle is delineated by the inferior border of the mandible and the anterior and posterior bellies of the digastric muscle. The submental triangle, located medial to the submandibular triangle, is bounded by the hyoid bone, the anterior belly of the digastric, and the midline of the neck.[2]
The muscular triangle is outlined by the anterior border of the SCM, the superior belly of the omohyoid muscle, the midline of the neck, and the hyoid. The carotid triangle lies between the anterior border of the SCM, the superior belly of the omohyoid, and the posterior belly of the digastric, with the stylohyoid muscle running along its superior margin.[3]
The investing layer of the deep cervical fascia encases the infrahyoid strap muscles and forms the superficial boundary of the entire anterior triangle (see Image. Deep Cervical Fascia of the Neck). The pretracheal layer of the deep cervical fascia forms the deep boundary of the carotid and muscular triangles, whereas the mylohyoid muscle forms the deep boundary of the submandibular and submental triangles.[4]
The submandibular gland is a major salivary gland that emerges from the lateral surface of the mylohyoid. The submandibular gland occupies most of the submandibular triangle.[5]
Posterior Triangle
The posterior triangle of the neck lies posterior to the anterior triangle. Boundaries include the posterior border of the SCM, the anterior border of the trapezius muscle, and the middle 1/3 of the clavicle. The SCM and trapezius meet at the superior nuchal line, forming the apex of the triangle. The investing layer of the deep cervical fascia forms the superficial boundary of the posterior triangle, whereas the prevertebral fascia forms the floor. The inferior belly of the omohyoid passes deep to the SCM and crosses the posterior triangle, dividing the region into the occipital and subclavian triangles.[6]
Function of the Neck Triangles
The anterior and posterior triangles of the neck provide an anatomic framework for organizing the numerous structures of the cervical region into defined compartments. Muscles, bones, and cervical fascial layers establish boundaries that enclose important structures, including nerves, arteries, veins, lymphatics, and other muscles.
Embryology
The anatomic structures of the head and neck derive from the pharyngeal apparatus, an embryologic structure comprising 6 distinct arches arranged in a craniocaudal sequence. Each arch contains a central layer of mesoderm and neural crest cells surrounded internally by endoderm and externally by ectoderm. The mesodermal core of each arch gives rise to the corresponding arteries, nerves, muscles, and skeletal structures.[7]
Many anatomic relationships among head and neck structures reflect origins within the pharyngeal apparatus. The anterior belly of the digastric receives innervation from the mandibular division of the trigeminal nerve (cranial nerve V), whereas the posterior belly receives innervation from the facial nerve (cranial nerve VII). The anterior belly of the digastric and the mandibular division of the trigeminal nerve arise from mesoderm of the 1st pharyngeal arch. The posterior belly of the digastric and the facial nerve arise from mesoderm of the 2nd pharyngeal arch.[8]
Blood Supply and Lymphatics
Anterior Triangle
The carotid sheath is a dense layer of fascia that encases the superior portion of the common carotid artery, the proximal portions of the internal and external carotid arteries, the internal jugular vein, and the vagus nerve (cranial nerve X).[9] The sheath lies deep to the posterior border of the SCM. The carotid sheath ascends through the carotid triangle, and its contents pass deep to the posterior belly of the digastric while continuing along the lateral aspect of the neck.
The common carotid artery courses anteromedially to the internal jugular vein within the sheath and bifurcates between the 3rd and 4th cervical vertebrae, corresponding to the superior border of the thyroid cartilage. The internal carotid artery gives off no branches in the neck and ascends posterior to the external carotid artery to enter the cranial cavity. The external carotid artery branches immediately after the bifurcation and supplies most structures of the head and neck (see Image. Arterial and Venous Anatomy of the Head and Neck).[10]
The external carotid artery gives rise to 8 branches. However, only the 4 most proximal branches lie within the boundaries of the anterior triangle.[11]
The superior thyroid artery originates from the anterior aspect of the carotid artery and descends to supply the superior pole of the thyroid gland, the thyrohyoid and cricothyroid muscles, and the internal larynx via the superior laryngeal artery. The ascending pharyngeal artery arises from the posterior aspect of the external carotid just superior to the superior thyroid artery. The artery pierces the pretracheal fascia and supplies the pharyngeal constrictor muscles.
The lingual artery originates from the anterior surface of the external carotid and passes deep to the mylohyoid to supply the muscles of the tongue and the sublingual salivary gland. The facial artery branches from the anterior surface of the external carotid just superior to the lingual artery. The blood vessel courses deep to the posterior belly of the digastric and the stylohyoid, continues superficial to the mylohyoid, and hooks over the inferior edge of the mandible just anterior to the masseter. The facial artery supplies the submandibular salivary gland, the soft palate, and multiple other facial structures via its numerous branches.[12]
The anterior triangle contains the submandibular and submental lymph node basins (see Image. Lymph Nodes of the Head and Neck). The submandibular nodes lie deep to the submandibular gland within the submandibular triangle and drain the oral cavity along with soft tissue structures of the lower face. The submental lymph nodes are located within the submental triangle and drain the lower lip, floor of the mouth, and apex of the tongue. Both lymph node groups hold clinical significance in infections of the lower face and deep neck spaces, as well as in head and neck malignancies.[13]
Posterior Triangle
The subclavian artery is the most prominent vascular structure of the posterior triangle. The artery traverses the subclavian triangle and becomes ensheathed in prevertebral fascia while crossing deep to the anterior scalene muscle. Medial to the anterior scalene, the subclavian artery gives rise to the thyrocervical trunk, which further branches into the suprascapular, transverse cervical, ascending cervical, and inferior thyroid arteries. The suprascapular and transverse cervical arteries course laterally over the anterior surface of the anterior scalene to supply the scapular muscles and trapezius, respectively. The ascending cervical artery ascends within the prevertebral fascia to supply the deep muscles of the neck. The inferior thyroid artery courses superomedially to the inferior lobe of the thyroid.[14]
Numerous lymph nodes associate with the posterior triangle and drain local structures. The posterior auricular and occipital nodes lie near the apex of the triangle on the superficial surfaces of the tendons of the SCM and trapezius. Superficial cervical nodes are located on the anterior surface of the SCM, whereas deep cervical nodes lie on the deep surface of the SCM. Posterior cervical nodes accompany the jugular vein as it pierces the investing fascia to enter the posterior triangle. Supraclavicular lymph nodes are located on the superior surface of the middle 1/3 of the clavicle.[15]
Nerves
Anterior Triangle
The anterior triangle of the neck contains several nerves that supply local structures and traverse the region en route to other destinations. The vagus nerve courses within the carotid sheath between the carotid artery and the internal jugular vein. Pharyngeal branches arise at the superior margin of the anterior triangle and provide motor innervation to the internal pharyngeal muscles. The superior laryngeal nerve branches from the vagus nerve just inferior to the pharyngeal branches and divides into the external and internal laryngeal nerves. The internal laryngeal nerve pierces the thyrohyoid membrane to supply sensory innervation to the larynx above the vocal cords. The external laryngeal nerve innervates the cricothyroid muscle.[16]
The hypoglossal nerve (cranial nerve XII) descends posterior to the internal carotid artery and enters the carotid triangle as it crosses the lateral surfaces of the internal and external carotid arteries (see Image. Schematic of Hypoglossal Nerve Distribution). The nerve courses anteriorly around the occipital artery, passes superficial to the lingual artery, and travels deep to the posterior belly of the digastric and the stylohyoid. The hypoglossal nerve then courses deep to the mylohyoid along its deep surface to innervate both the extrinsic and intrinsic muscles of the tongue.
The ansa cervicalis is a component of the cervical plexus that forms a loop of nerves within the anterior triangle and provides motor innervation to 3 of the 4 strap muscles.[17] The loop consists of a superior and an inferior root.
The superior root arises from the anterior ramus of the 1st cervical spinal nerve. This nerve root travels briefly with the hypoglossal nerve before descending along the anterior surface of the carotid sheath. The nerve to the thyrohyoid, derived from the 1st cervical spinal nerve but not considered a branch of the ansa cervicalis, courses with the hypoglossal nerve for an extended distance before separating to innervate the thyrohyoid muscle.
The inferior root originates from the anterior rami of the 2nd and 3rd cervical spinal nerves and descends along the lateral surface of the carotid sheath. The superior and inferior roots converge near the level of the 5th cervical vertebra to form the ansa loop, which gives off branches to innervate the omohyoid, sternohyoid, and sternothyroid.[18]
Branches of both the glossopharyngeal and vagus nerves innervate the carotid body and carotid sinus. The carotid body functions as a chemoreceptor to monitor blood oxygen content, while the carotid sinus acts as a baroreceptor to regulate blood pressure.[19]
Posterior Triangle
The spinal accessory nerve (cranial nerve XI) is located within the occipital division of the posterior triangle, providing motor innervation to the SCM and trapezius. After exiting the skull through the jugular foramen, the nerve descends along the deep surface of the SCM, giving off motor branches to the muscle. The nerve then emerges posterior to the SCM and traverses the posterior triangle in an inferior and posterior direction before passing deep to the trapezius.[20]
Several nerves associated with the posterior triangle provide cutaneous sensation to most of the cervical region. In addition to the ansa cervicalis, 4 nerves arise from the cervical plexus, originating from the anterior rami of the 2nd, 3rd, and 4th cervical spinal nerves.[21] These nerves emerge from the investing fascia near the posterior border of the SCM at its midpoint and course between the investing and superficial fascial layers toward their target regions.
The greater auricular and lesser occipital nerves ascend to innervate the skin of the parotid, mastoid, and lesser occipital regions. The transverse cervical nerve crosses medially over the SCM and supplies most of the skin of the anterior neck. The supraclavicular nerve courses inferiorly and branches broadly to provide cutaneous sensation over the clavicle and the first 2 ribs.[22]
Muscles
Anterior Triangle
The infrahyoid, or strap, muscles are a group of bilateral muscles located between the sternum and the hyoid. Innervation of the strap muscles is provided by the ansa cervicalis, except for the thyrohyoid, which is innervated by the 1st cervical spinal nerve.
The sternothyroid and thyrohyoid are relatively short muscles and lie deep to the longer omohyoid and sternohyoid. The sternothyroid originates from the posterior surface of the manubrium and the costal cartilage of the 1st rib. The muscle inserts on the oblique line of the thyroid cartilage and depresses the thyroid cartilage and larynx. The thyrohyoid is the superior continuation of the sternothyroid. This muscle originates from the oblique line of the thyroid cartilage and inserts on the greater horn and body of the hyoid. With the hyoid fixed, the thyrohyoid elevates the thyroid cartilage. With the thyroid cartilage fixed, the muscle depresses the hyoid.
The sternohyoid lies just lateral to the midline and superficial to both the sternothyroid and thyrohyoid. The sternohyoid originates from the sternoclavicular joint and neighboring manubrium and inserts on the body of the hyoid. The sternohyoid depresses the hyoid during swallowing.
The omohyoid lies lateral to the sternohyoid and superficial to the sternothyroid and thyrohyoid. The omohyoid consists of 2 bellies joined by an intermediate tendon. The superior belly separates the muscular and carotid triangles, originating from the intermediate tendon posterior to the SCM and inserting on the body of the hyoid lateral to the sternohyoid. The posterior belly passes through the posterior triangle and attaches to the superior aspect of the scapula. The omohyoid functions to depress the hyoid.[23]
Additional muscles relevant to the anterior triangle of the neck include the digastric, stylohyoid, and mylohyoid. The digastric consists of anterior and posterior bellies joined by a common tendon that attaches to the body of the hyoid. The anterior belly originates from the digastric fossa on the internal surface of the mandible and is innervated by the mandibular division of the trigeminal nerve. The posterior belly originates from the medial surface of the mastoid process and is innervated by the facial nerve. The digastric elevates the hyoid and depresses the mandible.
The stylohyoid follows a course similar to the posterior belly of the digastric and, together, these muscles separate the carotid and submandibular triangles. The stylohyoid originates from the styloid process at the base of the skull and inserts on the body of the hyoid and the digastric tendon. Innervation is from the facial nerve. The muscle retracts the hyoid during swallowing.
The mylohyoid forms the deep surface of the submandibular and submental triangles and constitutes the floor of the oral cavity. Originating from the mylohyoid line of the internal mandible, the mylohyoid inserts on the body of the hyoid and the contralateral mylohyoid at the midline. Innervation is from the nerve to mylohyoid, a branch of the inferior alveolar nerve of the mandibular division of the trigeminal nerve. The mylohyoid elevates and supports the floor of the oral cavity.[24]
Posterior Triangle
The SCM and trapezius contribute to the boundaries of the posterior triangle. Both muscles are wrapped in investing fascia and are innervated by the spinal accessory nerve.
The SCM originates from the manubrium and the medial end of the clavicle and inserts on the mastoid process and the superior nuchal line of the occipital bone. The actions of this muscle include ipsilateral flexion of the neck and contralateral rotation of the head.
The trapezius originates broadly from the superior nuchal line and the spinous processes of C2 through T2 and inserts on the spine of the scapula, the acromion process, and the lateral end of the clavicle. This muscle functions in multiple scapular movements, including elevation, lateral rotation, retraction, and depression.[25]
The superior belly of the omohyoid lies within the anterior triangle, whereas the inferior belly bisects the posterior triangle. The inferior belly originates from the superior border of the scapula near the suprascapular notch and inserts on the intermediate tendon deep to the SCM. Both bellies share innervation and function.
Physiologic Variants
Although the anatomy of the neck triangles is well-defined, numerous naturally occurring variants have been described. One variation involves the course of the spinal accessory nerve, which relates to both the anterior and posterior triangles. The nerve exits the cranial cavity via the jugular foramen and descends alongside the internal jugular vein, passing briefly through the carotid triangle. The accessory nerve typically crosses lateral to the internal jugular vein at the level of the 3rd cervical vertebra en route to the SCM and trapezius. A study of 207 neck dissections found the nerve crossed medial to the vein in 6 cases. Some cadaveric studies report an incidence of up to 1/3 of individuals having the nerve pass medial to the vein.[26]
The omohyoid exhibits additional anatomic variation, with alternate insertions on the clavicle rather than the scapula, and fusion of the superior belly to the sternohyoid.[27] The superior thyroid artery, usually the first branch of the external carotid artery, originates from the common carotid artery or the carotid bifurcation in over half of cases.
Surgical Considerations
Anterior Triangle
A thorough understanding of neck anatomy is essential to avoid injury during surgical procedures. Carotid endarterectomy, performed to relieve significant internal carotid artery stenosis, exposes multiple critical nerves and vascular structures.[28] The roots of the ansa cervicalis course along the anterior and lateral surfaces of the carotid sheath. The carotid sinus and the carotid branch of the glossopharyngeal nerve remain vulnerable during the procedure. Excessive or inadvertent stimulation of these structures can cause profound intraoperative bradycardia and hypotension, while direct injury may abolish the baroreceptor reflex. Damage to the vagus nerve within the carotid sheath can produce dysphagia, hoarseness, and aspiration.[29]
Thyroid and parathyroid surgery requires careful dissection of the anterior triangle, as these glands lie within the pretracheal layer of the deep cervical fascia. The strap muscles must be delicately retracted or divided using electrocautery to provide adequate visualization of the thyroid gland. The neurovascular structures of the thyroid and parathyroid glands lie deep to the strap muscles. Particular attention is required for the superior laryngeal artery and nerve near the superior pole of the thyroid. The superior thyroid artery must be ligated distal to the branch of the superior laryngeal artery to avoid injury to both the artery and nerve. Unilateral injury to the superior laryngeal nerve typically causes mild voice changes, such as reduced projection or voice fatigue, while bilateral injury abolishes the laryngeal cough reflex, increasing the risk of aspiration and airway compromise.[30]
The recurrent laryngeal nerve is also vulnerable during thyroid and parathyroid surgery as it ascends in the tracheoesophageal groove. The most common site of injury occurs near the ligament of Berry, a fascial structure derived from pretracheal fascia that anchors the thyroid capsule to the cricoid cartilage.[31] Unilateral recurrent laryngeal nerve injury presents as hoarseness, whereas bilateral injury results in complete vocal cord paralysis, leading to aspiration risk and airway compromise. Preoperative flexible laryngoscopy is recommended for patients with prior neck surgery to evaluate for occult unilateral vocal cord paralysis, as reoperation carries a risk of bilateral injury.[32]
Posterior Triangle
Operations involving the dissection of the posterior triangle require careful attention to the spinal accessory nerve. Intraoperative nerve mapping using direct stimulation is often necessary to prevent permanent nerve injury. Damage to the spinal accessory nerve within the posterior triangle can result in weakness of shoulder elevation or arm abduction and chronic pain due to disruption of trapezius innervation.[33] The SCM is generally spared, as the spinal accessory nerve supplies it at a more proximal location.[34]
Cutaneous branches of the cervical plexus are important for anesthetic management. A bilateral superficial cervical plexus block provides analgesia for procedures such as thyroidectomy, parathyroidectomy, and carotid endarterectomy. The block is performed by inserting a needle at the “nerve point of the neck,” located along the posterior border of the SCM just deep to the investing fascia. Local anesthetic is deposited to surround the emerging nerves. Head rotation to the contralateral side facilitates visualization of the SCM. Ultrasound guidance may be used but is not required.[35]
Clinical Significance
Anterior Triangle
The internal jugular vein holds considerable clinical significance as it courses through the anterior triangle of the neck. Jugular venous pressure serves as a key measure of right heart function. Conditions such as inferior wall myocardial infarction and congestive heart failure impede forward blood flow, causing pressure within the internal jugular vein to rise. This increased pressure leads to gross engorgement of the vein, and the resulting waveform can be assessed via jugular venous pulse tracing.
The internal jugular vein is frequently used for central venous access, including parenteral nutrition, dialysis, and administration of vasopressors or chemotherapy medications. Central access via the internal jugular vein generally carries fewer complications than the subclavian vein and may be localized using surface landmarks or ultrasound guidance. However, proximity to the carotid artery introduces the risk of accidental puncture or hematoma.[36]
The carotid sinus and the carotid body are located at the bifurcation of the common carotid artery and perform essential physiologic functions with clinical relevance. The carotid sinus acts as a baroreceptor that regulates blood pressure and receives innervation from the carotid branch of the glossopharyngeal nerve. Increased blood pressure stretches the sinus, triggering autonomic adjustments that decrease blood pressure, slow the heart rate, and reduce respiratory rate. Clinicians may perform gentle compression of the carotid sinus, known as carotid sinus massage, to terminate cardiac arrhythmias, such as supraventricular tachycardia.
The carotid body functions as a chemoreceptor that senses blood oxygen content, complementing the carotid sinus in cardiovascular regulation. Innervation of this structure arises from branches of both the glossopharyngeal and vagus nerves. Chronic hypoxic conditions, such as high-altitude exposure or chronic obstructive pulmonary disease, can overstimulate the carotid bodies, resulting in hypertrophy, hyperplasia, and, in rare cases, neoplastic transformation.[37]
Posterior Triangle
Lymphadenopathy is a relatively common pathology in the cervical region and may occur in both the anterior and posterior triangles of the neck. Physical examination and knowledge of lymphatic drainage patterns are essential for identifying the underlying cause. Soft, tender lymph nodes generally indicate infectious etiologies, such as pharyngitis or mononucleosis. Firm, rubbery lymph nodes are more suggestive of a neoplastic process.
Cervical lymphadenopathy often represents the initial manifestation of head and neck cancers in adults, warranting further evaluation to locate the primary tumor.[38] Nasopharyngeal carcinoma is classically associated with level V lymph node involvement in the posterior neck. Cutaneous malignancies and infections of the posterior scalp can also result in lymphadenopathy within the posterior triangle.[39]
Media
(Click Image to Enlarge)
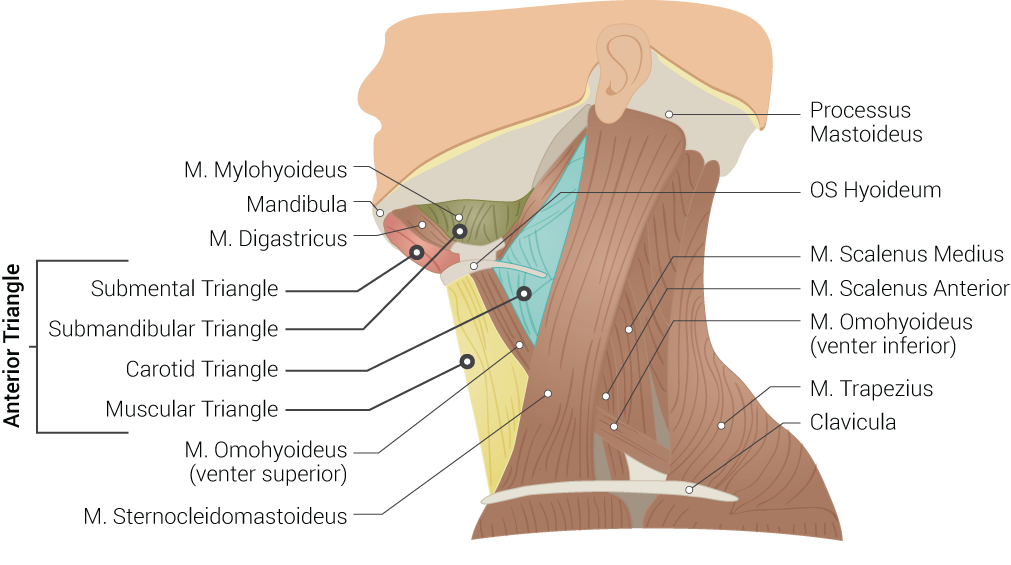
Superficial Neck Anatomy. This left lateral-view illustration shows the anterior and posterior triangles. The anterior triangle is further divided into the submental, submandibular, carotid, and muscular triangles. The muscles in this illustration include the mylohyoideus, digastricus, omohyoideus (venter superior and inferior), sternocleidomastoideus, scalenus medius and anterior, and trapezius. Bony structures include the mandible, mastoid process, left hyoid, and clavicle.
Illustrated by B Palmer
(Click Image to Enlarge)
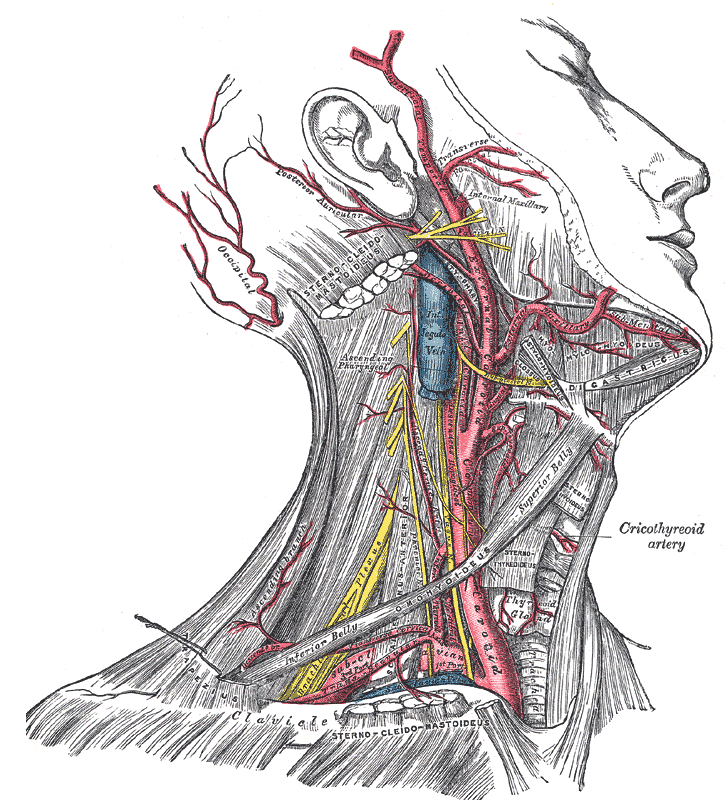
Arterial and Venous Anatomy of the Head and Neck. This illustration highlights the major vascular structures of the head and neck, including the external carotid artery, internal jugular vein, and maxillary artery. These vessels provide arterial perfusion to the facial and cranial regions and facilitate venous drainage to the heart.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
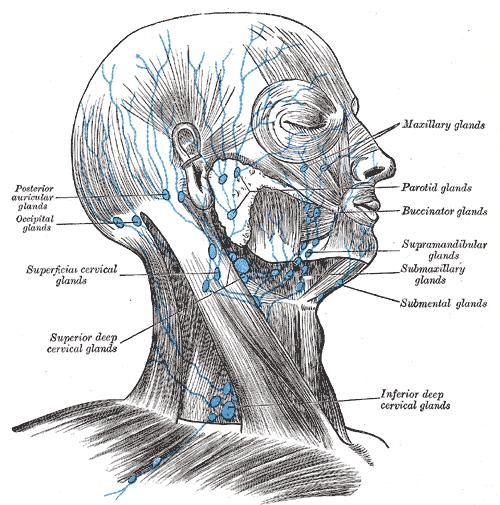
Lymph Nodes of the Head and Neck. This illustration shows the major lymph node groups of the head and neck, including the posterior auricular, occipital, superficial cervical, deep cervical, submental, submandibular, supramandibular, buccinator, parotid, and maxillary groups. The original labels reflect historical anatomic nomenclature.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
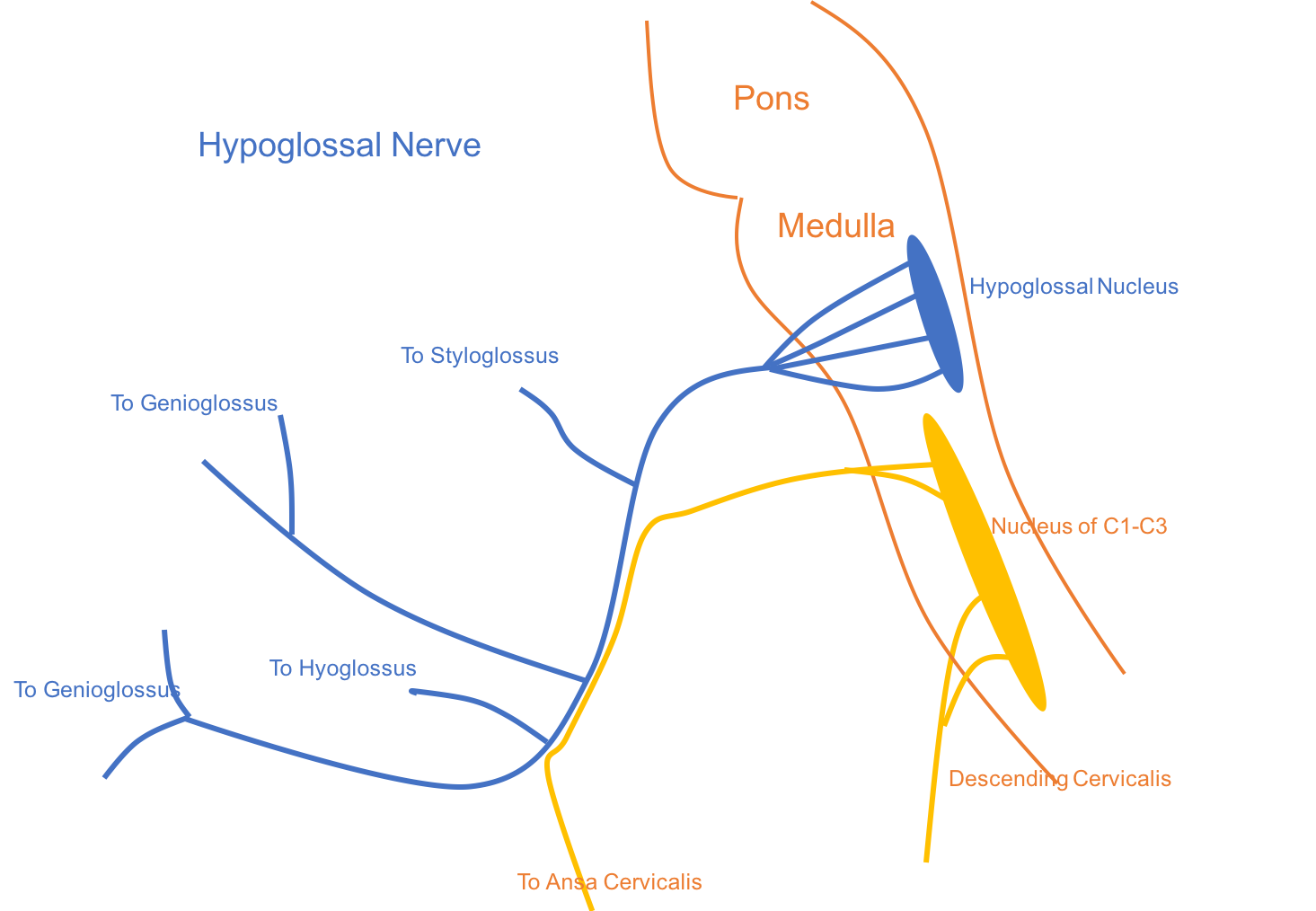
Schematic of Hypoglossal Nerve Distribution. The diagram illustrates cranial nerve XII originating from the hypoglossal nucleus in the medulla, with peripheral branches innervating tongue muscles (genioglossus, hyoglossus, styloglossus). Cervical contributions from C1 to C3 run with cranial nerve XII for a short distance to form the superior root of the ansa cervicalis and give off descending branches to infrahyoid muscles.
Contributed by Seung Yun Kim and Imama Naqvi, MD
(Click Image to Enlarge)
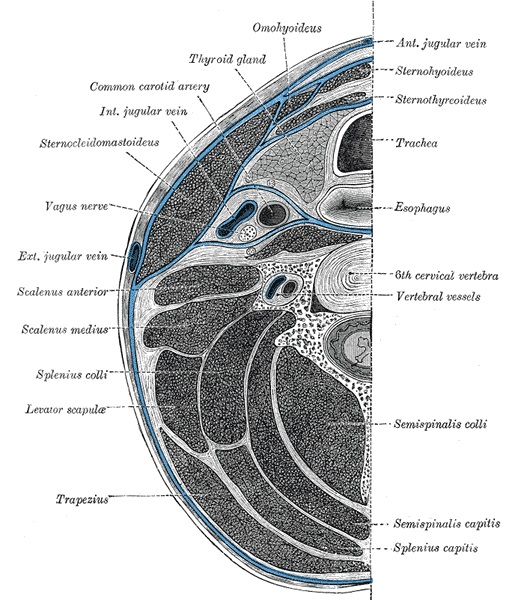
Deep Cervical Fascia of the Neck. The deep cervical fascia of the neck, which is located at the level of the 6th cervical vertebra, is highlighted in blue.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Mina V, Chrysikos D, Troupis T, Filippou D. Anatomical Variations of the Carotid Triangle: A Systematic Review. Cureus. 2025 Sep:17(9):e91547. doi: 10.7759/cureus.91547. Epub 2025 Sep 3 [PubMed PMID: 41049905]
Level 1 (high-level) evidenceBhat NP, Sumalatha S, Shetty A, Prabhath S. A clinical perspective on the anatomical study of digastric muscle. Anatomy & cell biology. 2023 Dec 31:56(4):441-447. doi: 10.5115/acb.23.043. Epub 2023 Oct 6 [PubMed PMID: 37798015]
Level 3 (low-level) evidenceWang M, Li G, Sui S, Cao S, Gai X, Zhu J, Chao Li CL. Complex carotid artery stenosis via enhanced anterior cervical triangle posterior vena jugularisinterna approach. Pakistan journal of pharmaceutical sciences. 2019 Jan:32(1(Special)):453-457 [PubMed PMID: 30852484]
Sutcliffe P, Lasrado S. Anatomy, Head and Neck, Deep Cervical Neck Fascia. StatPearls. 2026 Jan:(): [PubMed PMID: 31082135]
Ghosh S, Joseph B, Chakraborty P, Singh S, Das E. Harnessing the Forgotten Triangles of the Neck for Lingual Artery Ligation in Glossectomies: A Technical Report. Cureus. 2023 Aug:15(8):e43836. doi: 10.7759/cureus.43836. Epub 2023 Aug 21 [PubMed PMID: 37736471]
Ellis S, Brassett C, Glibbery N, Cheema J, Madenlidou S. The spinal accessory nerve and its entry point into the posterior triangle of the neck. Folia morphologica. 2023:82(2):256-260. doi: 10.5603/FM.a2022.0014. Epub 2022 Feb 21 [PubMed PMID: 35187635]
Toro-Tobon S, Manrique M, Paredes-Gutierrez J, Mantilla-Rivas E, Oh H, Ahmad L, Oh AK, Rogers GF. Pharyngeal Arches, Chapter 1: Normal Development and Derivatives. The Journal of craniofacial surgery. 2023 Oct 1:34(7):2237-2241. doi: 10.1097/SCS.0000000000009374. Epub 2023 Jun 2 [PubMed PMID: 37264513]
Natsis K, Piagkou M, Vrochidis P, Papadopoulou E, Lazaridis N. Unilateral asymmetrical anterior bellies of the digastric muscle in coexistence with accessory muscle bundles in the submental triangle: A rare case report. Morphologie : bulletin de l'Association des anatomistes. 2018 Jun:102(337):83-86. doi: 10.1016/j.morpho.2017.10.001. Epub 2018 Feb 26 [PubMed PMID: 29496384]
Level 3 (low-level) evidenceBond JD, Zheng F, Wang Q, Zhang M. The carotid sheath: Anatomy and clinical considerations. World neurosurgery: X. 2023 Apr:18():100158. doi: 10.1016/j.wnsx.2023.100158. Epub 2023 Jan 24 [PubMed PMID: 37081926]
Chengazi HU, Bhatt AA. Pathology of the carotid space. Insights into imaging. 2019 Feb 15:10(1):21. doi: 10.1186/s13244-019-0704-z. Epub 2019 Feb 15 [PubMed PMID: 30771026]
Sasikumar N, S V, Raghunath G, Karunakaran B, S N, Ks PD, M K, G SN, Gurusamy K, Maria Francis Y. Morphometric Study and Branching Patterns of External Carotid Artery Using Computed Tomography Angiography Among the South Indian Population: A Retrospective Study. Cureus. 2023 Feb:15(2):e35624. doi: 10.7759/cureus.35624. Epub 2023 Feb 28 [PubMed PMID: 37007303]
Level 2 (mid-level) evidencePadur AA, Kumar N. Unusual branching pattern and termination of facial artery and its clinical implications for facial operations. Jornal vascular brasileiro. 2019 Jul 12:18():e20190021. doi: 10.1590/1677-5449.190021. Epub 2019 Jul 12 [PubMed PMID: 31360158]
Janković I, Kovačević P, Janković D, Stevanović G, Momčilović S. Lymphatic drainage map of the head and neck skin squamous cell carcinoma detected by sentinel lymph node biopsy. European review for medical and pharmacological sciences. 2021 Aug:25(16):5228-5234. doi: 10.26355/eurrev_202108_26536. Epub [PubMed PMID: 34486697]
Weiglein AH, Moriggl B, Schalk C, Künzel KH, Müller U. Arteries in the posterior cervical triangle in man. Clinical anatomy (New York, N.Y.). 2005 Nov:18(8):553-7 [PubMed PMID: 16187318]
Eguchi K, Muro S, Miwa K, Yamaguchi K, Akita K. Deep cervical fascia as an anatomical landmark of lingual lymph nodes: An anatomic and histologic study. Auris, nasus, larynx. 2020 Jun:47(3):464-471. doi: 10.1016/j.anl.2019.11.007. Epub 2019 Dec 18 [PubMed PMID: 31864835]
Cheruiyot I, Kipkorir V, Henry BM, Munguti J, Cirocchi R, Odula P, Wong LM, Olabu B, Walocha J. Surgical anatomy of the external branch of the superior laryngeal nerve: a systematic review and meta-analysis. Langenbeck's archives of surgery. 2018 Nov:403(7):811-823. doi: 10.1007/s00423-018-1723-9. Epub 2018 Nov 14 [PubMed PMID: 30430230]
Level 1 (high-level) evidencePereira Boog GH, Hojaij FC, Mazzaro Conchy MM, Bentes RDS, Akamatsu FE, Jácomo AL. Ansa cervicalis or ansa hypoglossi? A systematic review. Brazilian journal of otorhinolaryngology. 2025 Jul:91 Suppl 1(Suppl 1):101604. doi: 10.1016/j.bjorl.2025.101604. Epub 2025 May 29 [PubMed PMID: 40446387]
Level 1 (high-level) evidenceKikuta S, Jenkins S, Kusukawa J, Iwanaga J, Loukas M, Tubbs RS. Ansa cervicalis: a comprehensive review of its anatomy, variations, pathology, and surgical applications. Anatomy & cell biology. 2019 Sep:52(3):221-225. doi: 10.5115/acb.19.041. Epub 2019 Aug 26 [PubMed PMID: 31598349]
Ishii K, Izaki T, Asahara R, Komine H. Carotid sinus baroafferent signals contribute to cerebral blood flow regulation during acute hypotension in young males: A randomized crossover study. Physiological reports. 2024 Feb:12(3):e15937. doi: 10.14814/phy2.15937. Epub [PubMed PMID: 38325901]
Level 1 (high-level) evidenceKim DH, Cho YJ, Tiel RL, Kline DG. Surgical outcomes of 111 spinal accessory nerve injuries. Neurosurgery. 2003 Nov:53(5):1106-12; discussion 1102-3 [PubMed PMID: 14580277]
Level 2 (mid-level) evidenceSimon KS, Rout S, Lionel KR, Joel JJ, Daniel P. Anatomical considerations of cutaneous nerves of scalp for an effective anesthetic blockade for procedures on the scalp. Journal of neurosciences in rural practice. 2023 Jan-Mar:14(1):62-69. doi: 10.25259/JNRP-2022-2-4-R2-(2362). Epub 2023 Jan 2 [PubMed PMID: 36891119]
Lee JH, Cheng KL, Choi YJ, Baek JH. High-resolution Imaging of Neural Anatomy and Pathology of the Neck. Korean journal of radiology. 2017 Jan-Feb:18(1):180-193. doi: 10.3348/kjr.2017.18.1.180. Epub 2017 Jan 5 [PubMed PMID: 28096728]
Valentino WL, Alnouri G, Vance D, Paknezhad H, Tami A, Sataloff RT. The Utility of Strap Muscle in Complex Type I Thyroplasties. Journal of voice : official journal of the Voice Foundation. 2021 May:35(3):493-496. doi: 10.1016/j.jvoice.2019.08.025. Epub 2019 Sep 20 [PubMed PMID: 31543359]
Bell FE 3rd, Neuffer FH, Haddad TR, Epps JC, Kozik ME, Warren BC. Active Learning of the Floor of Mouth Anatomy with Ultrasound. Anatomical sciences education. 2019 May:12(3):310-316. doi: 10.1002/ase.1839. Epub 2018 Nov 9 [PubMed PMID: 30414266]
Ihnatsenka B, Boezaart AP. Applied sonoanatomy of the posterior triangle of the neck. International journal of shoulder surgery. 2010 Jul:4(3):63-74. doi: 10.4103/0973-6042.76963. Epub [PubMed PMID: 21472066]
Brennan PA, St J Blythe J, Alam P, Green B, Parry D. Division of the spinal accessory nerve in the anterior triangle: a prospective clinical study. The British journal of oral & maxillofacial surgery. 2015 Sep:53(7):633-6. doi: 10.1016/j.bjoms.2015.04.010. Epub 2015 May 13 [PubMed PMID: 25979155]
Rai R, Ranade A, Nayak S, Vadgaonkar R, Mangala P, Krishnamurthy A. A study of anatomical variability of the omohyoid muscle and its clinical relevance. Clinics (Sao Paulo, Brazil). 2008 Aug:63(4):521-4 [PubMed PMID: 18719765]
Reiff T, Eckstein HH, Mansmann U, Jansen O, Fraedrich G, Mudra H, Böckler D, Böhm M, Debus ES, Fiehler J, Mathias K, Ringelstein EB, Schmidli J, Stingele R, Zahn R, Zeller T, Niesen WD, Barlinn K, Binder A, Glahn J, Hacke W, Ringleb PA, SPACE-2 Investigators. Carotid endarterectomy or stenting or best medical treatment alone for moderate-to-severe asymptomatic carotid artery stenosis: 5-year results of a multicentre, randomised controlled trial. The Lancet. Neurology. 2022 Oct:21(10):877-888. doi: 10.1016/S1474-4422(22)00290-3. Epub [PubMed PMID: 36115360]
Level 1 (high-level) evidenceWest CT, Brassett C, Gaunt ME. Variations in carotid sinus anatomy and their relevance to carotid interventions. Folia morphologica. 2018:77(4):693-697. doi: 10.5603/FM.a2018.0017. Epub 2018 Mar 3 [PubMed PMID: 29500893]
Shin DU, Sung JK, Nam KH, Cho DC. Bilateral internal superior laryngeal nerve palsy of traumatic cervical injury patient who presented as loss of cough reflex after anterior cervical discectomy with fusion. Journal of Korean Neurosurgical Society. 2012 Sep:52(3):264-6. doi: 10.3340/jkns.2012.52.3.264. Epub 2012 Sep 30 [PubMed PMID: 23115675]
Level 3 (low-level) evidencePatra A, Asghar A, Chaudhary P, Ravi KS. Identification of valid anatomical landmarks to locate and protect recurrent laryngeal nerve during thyroid surgery: a cadaveric study. Surgical and radiologic anatomy : SRA. 2023 Jan:45(1):73-80. doi: 10.1007/s00276-022-03054-y. Epub 2022 Dec 2 [PubMed PMID: 36459179]
Ringel MD, Sosa JA, Baloch Z, Bischoff L, Bloom G, Brent GA, Brock PL, Chou R, Flavell RR, Goldner W, Grubbs EG, Haymart M, Larson SM, Leung AM, Osborne JR, Ridge JA, Robinson B, Steward DL, Tufano RP, Wirth LJ. 2025 American Thyroid Association Management Guidelines for Adult Patients with Differentiated Thyroid Cancer. Thyroid : official journal of the American Thyroid Association. 2025 Aug:35(8):841-985. doi: 10.1177/10507256251363120. Epub [PubMed PMID: 40844370]
Kopacz KS, Mauermann ML, Laughlin RS, Sellon JL, Shin AY, Pulos NA, Bishop AT, Maldonado AA, Spinner RJ, Meiling JB. Diagnostic Neuromuscular Ultrasonography of Spinal Accessory Nerve Injury After Cosmetic Rhytidectomy. Journal of clinical ultrasound : JCU. 2025 Nov-Dec:53(9):2210-2214. doi: 10.1002/jcu.70015. Epub 2025 Jul 21 [PubMed PMID: 40689442]
Brînzeu A, Sindou M. Functional anatomy of the accessory nerve studied through intraoperative electrophysiological mapping. Journal of neurosurgery. 2017 Mar:126(3):913-921. doi: 10.3171/2015.11.JNS15817. Epub 2016 Apr 8 [PubMed PMID: 27058194]
Senapathi TGA, Widnyana IMG, Aribawa IGNM, Wiryana M, Sinardja IK, Nada IKW, Jaya AGPS, Putra IGKS. Ultrasound-guided bilateral superficial cervical plexus block is more effective than landmark technique for reducing pain from thyroidectomy. Journal of pain research. 2017:10():1619-1622. doi: 10.2147/JPR.S138222. Epub 2017 Jul 14 [PubMed PMID: 28761368]
Saugel B, Scheeren TWL, Teboul JL. Ultrasound-guided central venous catheter placement: a structured review and recommendations for clinical practice. Critical care (London, England). 2017 Aug 28:21(1):225. doi: 10.1186/s13054-017-1814-y. Epub 2017 Aug 28 [PubMed PMID: 28844205]
Amato B, Compagna R, Florio A, Calemma F, Rocca A, Salzano F, Brongo S, Gasbarro V, Aprea G. Surgical Versus Sequential Hybrid Treatment of Carotid Body Tumors. Open medicine (Warsaw, Poland). 2019:14():968-976. doi: 10.1515/med-2019-0115. Epub 2019 Dec 26 [PubMed PMID: 31934642]
Fernández Aceñero MJ, Caso Viesca A, Díaz Del Arco C. Role of fine needle aspiration cytology in the management of supraclavicular lymph node metastasis: Review of our experience. Diagnostic cytopathology. 2019 Mar:47(3):181-186. doi: 10.1002/dc.24064. Epub 2018 Nov 23 [PubMed PMID: 30468321]
Pynnonen MA, Gillespie MB, Roman B, Rosenfeld RM, Tunkel DE, Bontempo L, Brook I, Chick DA, Colandrea M, Finestone SA, Fowler JC, Griffith CC, Henson Z, Levine C, Mehta V, Salama A, Scharpf J, Shatzkes DR, Stern WB, Youngerman JS, Corrigan MD. Clinical Practice Guideline: Evaluation of the Neck Mass in Adults Executive Summary. Otolaryngology--head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery. 2017 Sep:157(3):355-371. doi: 10.1177/0194599817723609. Epub [PubMed PMID: 28891424]
Level 1 (high-level) evidence