Introduction
Repair of medium- to large tissue defects can be accomplished through a variety of methods. Still, whether bone, soft tissue, or a combination of both is needed, axial flaps provide surgeons with a reliable, workhorse reconstructive option in most cases.[1] The term "axial" is used to refer to these flaps because of the presence of a primary feeding artery that runs from the flap's base through its long axis and its pedicle (the bridge of tissue that connects the flap to its donor site).[2][3] In contrast, "random" patterned flaps, which are used for reconstruction of small to medium-sized soft tissue defects, do not contain named blood vessels and rely solely on perfusion via the subdermal vascular plexus.[4]
Random-pattern flaps are therefore potentially less reliable than axial flaps. Still, they are typically more convenient to use because their design and placement are not constrained by vascular anatomy to the same extent as axial flaps.[5] For more information about random-patterned flaps, please see Basic Flap Design.[6]
Axial flaps may be categorized in several different ways, depending upon the manner in which the flap is transferred into its recipient site, the type of perfusion, and the sort of tissue involved. Flaps may be moved using advancement, rotation, transposition, interpolation (positioning the flap's pedicle either over or under intact intervening skin), or free microvascular transfer, in which the flap is entirely detached from the donor site, and then connected to an arterial supply and venous drainage (with or without motor or sensory nerve coaptation) at the recipient site (see Images. Posterior Scalp Advancement Flap, Reverse Sural Artery Flap, Anterolateral Thigh Flap Before Inset, and Anterolateral Thigh Flap After Inset).
Rotation and interpolation are the most common means of transferring axial flaps, with some interpolated flaps, such as the inferior turbinate flap when used for repair of a nasal septal perforation, requiring a second operation to divide the vascular pedicle several weeks after inset and others, such as a pericranial flap used for the same purpose, tunneling the pedicle under the surrounding tissue to obviate that requirement and maintain reliable, long-term perfusion of the flap (see Image. Inferior Turbinate Flap Reconstruction for Nasal Septal Perforation). Interpolated flaps whose pedicles contain no skin and pass underneath the tissue between the flap donor site and the recipient site are also known as "island" flaps (see Image. Supraclavicular Artery Island Flap for Facial Reconstruction). Microvascular free tissue transfer, on the other hand, is typically performed as a single-stage procedure.
Still, the surgeries are generally lengthy and challenging due to the technical demands of anastomosing small blood vessels and maintaining uninterrupted perfusion. The position of the blood supply is another important factor to consider, as the distance between the axial artery and the tissue paddle being relocated into the defect can affect the flap's reliability. "Direct cutaneous" flaps, in which the vessel runs immediately below the skin, such as the paramedian forehead flap, are very reliable.
In contrast, "perforator" flaps, such as the deep inferior epigastric perforator flap, may be more tenuous, as they rely upon small branches from the vascular pedicle, often located within or below a layer of underlying muscle, to supply blood to the skin. "Fasciocutaneous" flaps, including the radial forearm flap, have more tissue intervening between the primary artery and the tissue being perfused than direct cutaneous flaps, but do not rely on the long, easily disrupted arterial branches of perforator flaps (see Image. Fasciocutaneous Flap Perfusion). Of note, the term "fasciocutaneous" can be used to describe both the blood supply of a flap and its soft tissue components; conveniently, the 2 descriptions typically align anatomically.
In most cases, arterial flow into the flap will proceed in the physiological, antegrade direction of flow; however, there are some regions, particularly in the face, in which robust collateral circulation permits the pedicle to be placed distal to the flap, with respect to the normal direction of blood flow, and still maintain perfusion. This phenomenon may, in certain cases, significantly improve the surgeon's ability to maneuver the desired tissue into the defect; classic examples include the "retrograde" facial artery musculomucosal flap, the reverse sural artery flap, and the distally based radial forearm flap. While many flaps incorporate the distal end of the axial artery, some are based on an artery that traverses the flap and exits the other side, thus requiring ligation of the vessel both distally and proximally.
When one of these flaps is transferred, typically using a free microvascular technique, another free flap can be connected to the distal aspect of the first. The second flap will receive perfusion and drain its venous output via the first in a "flow-through" fashion. These are complex reconstructions with a relatively high risk of failure because they require serial vascular microanastomoses.
Still, they provide the surgeon with options for repairing even very large composite defects. Composite defects are best addressed with axial flaps, as the subdermal plexus by itself is insufficient to support inclusion of tissue elements beyond skin alone. Typical axial flaps are referred to as "fasciocutaneous," due to the presence of nothing more than skin and the underlying fascia within the flap, but "osteocutaneous" flaps, such as the free fibula flap, "myocutaneous," and even solid organ, hand, larynx, and face transplants are considered axial flaps as well (see Image. Fibula Free Flap Harvest and Closing Ostectomy).
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
The reliability of axial reconstruction techniques stems from the use of a specific vessel to perfuse a flap that typically contains a single angiosome, which is the region of tissue that can be supplied sufficiently by a single artery.[7] By limiting the amount of tissue transferred to 1 angiosome and ensuring that the vascular pedicle is neither compressed nor kinked when the flap is inset into the defect, the chance of axial flap survival is expected to exceed 95%.[8] In some cases, more than 1 angiosome needs to be included in a flap, and this is possible if the collateral circulation between the angiosomes, the "choke vessels," is patent.
These small-caliber arteries normally help maintain circulation when an angiosome's primary blood supply is injured or obstructed, and they can therefore be used to expand a flap artery's vascular territory via the "delay" phenomenon. By incising and elevating an axial flap, but then replacing it into its original location rather than transferring it into a defect, the choke vessels are allowed to dilate and perfuse tissue beyond the angiosome of the flap's primary artery before that vessel's blood flow is stressed by reorientation, stretching, and twisting during flap transfer. Choke vessel dilation may occur as soon as 48 to 72 hours after the delay procedure. Still, flaps are often delayed for 2 to 3 weeks to achieve maximum perfusion before the actual transfer operation.[9]
Depending upon the flap in question, the choke vessels are most likely to be located either within the skin or the muscle of the tissue paddle. Within the skin, blood flows through the superficial and deep subdermal plexi, low-pressure microvascular systems that support random-pattern local flaps by providing nutritional support, removing waste products, and regulating temperature.[10][11] For this reason, when flaps are delayed, the portion of the soft tissue that extends beyond the axial vessel's primary angiosome essentially behaves like a random pattern flap, which makes its survival less reliable than the portion within the primary angiosome.[12]
An example of a flap that is frequently delayed is the deltopectoral flap, which is based on the second and third perforators of the internal mammary artery, and whose primary angiosome reaches transversely from the lateral border of the sternum to the deltopectoral groove. Because a longer flap is frequently required for head and neck reconstruction, however, fasciocutaneous tissue located lateral to the distal tip of the flap may be needed. The region immediately beyond the primary angiosome is normally perfused primarily by a cutaneous branch of the thoracoacromial artery, and the region distal to that by the deltoid musculocutaneous branch of the thoracoacromial artery.
If a delayed procedure is successful, the flap can provide a substantial amount of skin and soft tissue, with all 3 angiosomes perfused by the internal mammary artery perforators. That said, the more distal portions have progressively more tenuous vascularity. In cases of vasculopathy or careless surgical technique, even the delay procedure itself may place the flap at risk and cause tissue necrosis before the reconstruction has begun in earnest.
Indications
Axial flap transfer is indicated for the repair of medium to large defects when there is insufficient tissue available adjacent to the wound to reconstruct it or when the geometry of an axial flap is preferable to that of a random flap. Axial flaps are indicated as well when skin grafts would be incapable of healing in the wound, for example, if there is bare bone or bare cartilage in the base of the defect. An axial flap's slim vascular pedicle often provides more mobility and inset flexibility than the broad swath of skin required to support a flap with a random pattern blood supply, given that the latter type of flap cannot usually have a length greater than 2 to 3 times its width.[6]
Axial flaps are also preferred when local flap reconstruction or skin grafting has failed, or the perfusion surrounding the wound is so compromised due to prior surgery, trauma, radiation, or vasculopathy that any attempt at repair will need to bring a fresh blood supply with the new tissue to reduce the risk of ischemia and necrosis of the flap. Additionally, any reconstruction that requires significant volume or vascularized composite tissue, such as skin with fascia and bone, or skin and muscle, will require transfer of an arterial blood supply along with the flap, thus necessitating an axial design. The axial flap selected for a given defect should ideally have a close match in terms of skin color, texture, thickness, and hair growth, and should be situated such that the inset into the defect will not compromise the transferred tissue's perfusion. The most common clinical situations in which axial flaps are employed include oncologic resections, diabetic nonhealing wounds, traumatic tissue avulsion or destruction, and organ transplantation.
Contraindications
The use of axial flaps is relatively contraindicated when there is an infection at the recipient site or oncologic margins at the wound are positive. When used in cases of trauma, the wound must be cleaned thoroughly and all foreign body debris removed prior to flap transfer; otherwise, the risk of infection may be unacceptably high. Patients who smoke or use nicotine-containing products should be counseled to discontinue these at least 1 to 2 weeks before any potential flap surgery because of their adverse impact on microvascular perfusion.[13] If necessary and feasible, surgery may be postponed to allow the remaining nicotine to be metabolized. Harvest of flaps from areas that will require excessive tension at closure, due to limitations of the vascular pedicle's length, or whose tissue is either unhealthy (due to radiation, infection, ischemia, or scarring) or a poor match to the recipient site, should be avoided.
Equipment
The equipment required for axial flap transfer will vary somewhat depending on the flap's location and size; larger flaps require larger retractors and other instruments, while smaller flaps may need finer forceps, scissors, and needle drivers, among other tools. If the flap is to be placed in the mouth, nose, or throat, specialized specula or retractors may be needed. Flaps containing bone will need a saw and likely a drill as well.
In many cases, a Doppler ultrasound probe will help identify the primary blood supply to the planned flap, and real-time fluorescence imaging at the end of the procedure may be useful to confirm adequate perfusion. If microvascular anastomosis is necessary, microvascular instruments and sutures, along with an operating microscope, will be required. In this case, an implantable Doppler probe may be useful for postoperative monitoring of the flap's arterial and venous flow.
Examples of necessary equipment include:
- Doppler probe
- Skin marker
- #15 blade scalpel and #3 Bard-Parker knife handle
- Scissors: Metzenbaum, Mayo, Reynolds tenotomy, iris
- McCabe dissector
- Clamps: Crile, Kelly, Schnidt (tonsil), Hartmann
- Forceps: DeBakey, Gerald, Adson-Brown, Castroviejo
- Needle drivers: Olsen-Hegar, Halsey, Castroviejo
- Retractors: Richardson, Green, Army-Navy, Senn, Ragnell
- Saw: Gigli or reciprocating
- High-speed power drill
- Bipolar and monopolar electrocautery
- Vessel loops
- Sutures
- Suction drain: Blake or Jackson-Pratt
- Microvascular instruments, including scissors, forceps, vessel dilators, needle drivers, Acland vessel clamps, and a microscope
- Weck sponges, heparinized saline, venous couplers
- Fluorescence perfusion imaging system
Personnel
Some small axial flaps, such as Abbé or paramedian forehead flaps, can be elevated and transferred under local anesthesia. Still, most are large enough to require regional or general anesthesia and an operating room (see Image. Abbé-Estlander Flap). In addition to the surgeon, an anesthesia provider, a circulating nurse, and a surgical technician would be required. For more complicated cases, such as microvascular free tissue transfer, the surgical team needs specific training or experience with the nuances of the procedure, including which anesthetic modalities are most appropriate and how to support the surgeon most efficiently and safely during flap ischemia, particularly while operating under the microscope.
Preparation
Selection of an appropriate flap donor site ensures that the tissue types required for reconstruction are present and viable, ideally with skin color, texture, thickness, and hair growth that match those of the recipient site. The flap should also be able to reach the recipient site without stressing its pedicle. In some cases, several different flap options may be considered, and the patient may need to be counseled that the final decision will be made intraoperatively, especially if an oncologic resection and reconstruction are to be performed under the same anesthetic. Means of closing the donor site (the "secondary" defect) should also be anticipated, using a manual pinch test to determine whether primary closure will suffice or whether the patient should be informed that a skin graft might be necessary. Counseling regarding scarring is also helpful, taking care to consider the patient's prior history of any unsightly, hypertrophic, or keloid scars.
When possible, the location and sufficiency of the flap's axial blood supply should be evaluated preoperatively, typically with a Doppler probe. The vessels are marked before any local anesthetic injections, which may temporarily affect blood flow. If a Doppler probe is unavailable, the physical examination should include evaluation of pulses and capillary refill in the proposed flap area, if applicable. Additionally, the viability of any tissue distal to the planned flap should be determined if a large artery is to be harvested. Angiography is commonly employed for this purpose, especially in the lower extremity, whether fluoroscopic, tomographic, or via magnetic resonance.
A frequently used means of assessing the future viability of the hand after radial artery transfer is the modified Allen test, which is performed by asking the patient to clench a fist on the side of the planned flap, typically the nondominant hand, taking care to exsanguinate the thenar eminence in particular. The examiner then applies digital pressure to the ulnar and radial arteries, and the patient opens the hand and extends the fingers. The examiner then releases pressure on the ulnar artery, keeping the radial artery occluded.
If the pallor in the hand resolves rapidly, collateral circulation from the ulnar artery via the palmar arch is considered adequate to support the hand in the absence of a radial artery (see Video. Modified Allen Test). Special attention is paid to the thenar eminence because it is most distal to the ulnar artery's entry point into the hand and therefore most susceptible to ischemia in the event of ulnar artery insufficiency.[14] If there is no obvious visual change with either arterial occlusion or release, the test may be repeated with a Doppler probe placed over the thenar eminence, ensuring that the pulse is lost when pressure is applied to the arteries and returns when blood flow through the ulnar artery resumes. For longer surgeries, the patient should be optimized medically beforehand, especially if there are major comorbidities, extensive malignancy, or advanced age, any of which can have both physiological and anatomical effects.[11]
Technique or Treatment
The steps of axial flap harvest and inset vary greatly depending upon the specific flap selected and the defect it will be used to reconstruct. General principles include ensuring adequate flap vascularity preoperatively. That of any distal anatomy, incorporating the salient vessels into the flap and avoiding harvesting tissue outside of that vessel's angiosome, preventing injury to the flap's vessels during harvest or kinking during transfer, and minimizing the use of cautery on the flap or the undersurface of the overlying skin, which can compromise flap perfusion or cause a burn. If possible, thrombin should be used for hemostasis, and vasoconstrictors should be avoided. The following are examples of some commonly used axial flaps.
Paramedian Forehead Flap
The paramedian forehead flap is classically transferred as an interpolated, axial flap that has the supratrochlear vessels running within it (see Image. Paramedian Forehead Flap for Nasal Reconstruction). This flap is used most often for repair of nasal defects, up to and including total nasal reconstruction, and may be employed in a 2-stage or multi-stage procedure, with the pedicle exposed until it is divided during the last phase of the operation.[15][16] The flap's skin texture and color match those of the nasal tip quite well. If more than 50% of the nasal tip (or whichever nasal subunit has been violated) is missing, the remainder of the skin in the tip is generally removed so that the flap can resurface the entire area and thereby produce a less conspicuous reconstruction.
The supratrochlear vessels may also be used to perfuse the pericranium that underlies the paramedian forehead flap, either in conjunction with the skin or instead of it; even split calvarial bone may be included in the flap, if necessary. If skin is not required for the reconstruction, a pericranial flap may be elevated as a narrow vertical strip centered on the supratrochlear vessels, like the paramedian forehead flap, or it may be elevated as a broad sheet of tissue supplied by the supratrochlear and supraorbital vessels bilaterally (see Image. Pericranial Flap Elevation). The pericranial flap is often applied to several different reconstructive needs, including obliteration of the frontal sinus, resurfacing a skull base defect, and obturating a nasal septal perforation (see Image. Pericranial Flap Elevation).[17][18][19] The pericranium can be transferred as a buried or tunneled flap that does not require a subsequent surgical procedure to divide the pedicle, because the pedicle is not left exposed, as with the paramedian forehead flap.
In its most basic form, the paramedian forehead flap is transferred in 2 stages, as follows: The defect is measured or a template is made using a foil suture packet, and then this is traced onto the forehead, but rotated 180° (although not a mirror image), typically at the hairline and directly above the medial brow to capture the supratrochlear vessels. These are located between 1.7 cm and 2.2 cm lateral to the glabellar midline, but their presence can be confirmed with a Doppler ultrasound probe.[20] Surgeon preference will determine on which side to base the flap, but consideration should be given to minimizing tension and kinking of the pedicle during transfer; when reconstructing a unilateral defect, elevating the flap contralaterally may be best.
The length required for the pedicle may be approximated using a piece of gauze held against the medial brow and then rotated down to the defect. If the forehead is too short to permit a pedicle of sufficient length, the flap may be elevated from the hair-bearing scalp and laser hair removal planned for the future, or the pedicle may be curved in its upper third, and the flap placed more laterally to provide additional pedicle length. The width of the pedicle is usually roughly 1.5 cm, which is wide enough to incorporate the blood vessels and prevent them from kinking during flap transfer, but narrow enough not to limit the flap's mobility.
Flap elevation begins with an incision around the markings, followed by development of a subcutaneous plane under the flap itself, such that its thickness will roughly approximate the depth of the defect or be slightly thicker to ensure adequate perfusion. The majority of the pedicle will then be elevated in the subgaleal/subfrontalis glide plane, which is comparatively avascular, although small, deep branches to the pericranium will be encountered. The proximal 1 to 2 cm above the brow will be elevated in a subperiosteal plane to ensure vessel capture at its origin.
Because the vessels within the pedicle are comparatively small, dissection that exposes them directly is liable to cause them injury; a layer of fat or fascia should be left covering them. The flap can then be rotated gently into the defect and inset around its distal 270 degrees, leaving the junction of the flap and pedicle unsutured. The pedicle is left exposed with either petrolatum gauze or a skin graft applied to the raw surface to decrease bleeding.
The pedicle portion of the donor site is usually closed primarily, although the flap portion may require healing by secondary intention, which generally provides an acceptable cosmetic result. The flap is then allowed to heal in the defect for 3 weeks before the next stage of the surgery is performed. The second stage of the procedure may involve elevating the flap and thinning it to improve its contour and cosmesis at the recipient site, followed by another 3 weeks of healing, or it may simply involve dividing the pedicle and completing the inset of the proximal portion of the flap. When the pedicle is divided, the base is typically placed back into the glabella as a small, vertical triangle, which helps to correct any malposition of the medial brow that occurred after the first phase of the operation.
Numerous variations of the paramedian forehead flap technique exist as well, particularly for total or subtotal nasal reconstruction. These include the use of bilateral flaps for internal and external nasal reconstruction, lamination of a single flap at a preliminary stage before transfer using a skin graft on its undersurface to substitute the vestibular lining, or even the addition of bone and cartilage components to restore the nasal skeleton during the intermediate stage, after flap transfer but before pedicle division.[21][22] For more information about this procedure, please see Paramedian Forehead Flaps.
Temporoparietal Fascia Flap
Unlike the paramedian forehead flap, the temporoparietal fascia flap is not typically elevated with attached skin. However, skin, muscle, and split calvarial bone can all be transferred together based on the superficial temporal vessels that supply this flap.[23][24] As a terminal branch of the external carotid artery, the superficial temporal artery is substantially larger than the supratrochlear artery (~2 mm vs 0.8–1 mm), making the temporoparietal fascia flap suitable for free microvascular tissue transfer, if necessary.[25][26]
The temporoparietal fascia flap is most often employed for reconstruction of the external ear, periorbital region, and anterolateral skull base, although it has been reported as a reconstructive option for defects as distant as the foot.[27][28] Because the skin overlying the temporoparietal fascia is thick and hair-bearing, the flap is often transferred without any skin, even if skin is required for the reconstruction; a full-thickness skin graft can be applied on top of the flap, which provides an excellent vascular supply to support its healing (see Images. Temporoparietal Fascia Flap, and Auricular Reconstruction with Temporoparietal Fascia Flap and Supraclavicular Full-Thickness Graft).
The superficial temporal artery crosses over the zygomatic arch immediately anterior to the tragus and, 3 to 5 cm more superiorly, divides into anterior and posterior branches under the hair-bearing scalp.[29] Typically, the anterior branch is used to perfuse the temporoparietal fascia flap; its course can be traced preoperatively with a Doppler ultrasound probe, and the flap is designed such that the vessel occupies a central position within it. Harvest of the temporoparietal fascia should ideally exclude tissue anterior to the temporal hairline, as dissection in this area may place the frontal branch of the facial nerve at risk. While the line described by Pitanguy and Ramos in 1966 approximates the course of this nerve, limiting the fascial elevation to the region beneath hair-bearing skin (or what may have been hair-bearing previously in some patients) reliably prevents nerve injury (see Image. Pitanguy Line).
Access to the temporoparietal fascia flap is classically approached via a temporal scalp incision that may either take a straight line course over the anterior branch of the superficial temporal artery or may zigzag for improved scar camouflage. The desired flap length determines the incision length; it may be slightly shorter, but it typically ends in a bifurcation to improve exposure. A technique similar to that described above for paramedian forehead flaps uses a gauze sponge to estimate the required flap length, accounting for loss of effective length during transposition into the defect.
Once the incision is made, subdermal flaps are raised to expose the tissue that will be transferred. The subdermal flaps are elevated just below the level of the hair follicles, taking care to avoid injury that could cause alopecia. A thin layer of fat may be left on the temporoparietal fascia, if desired, to provide additional thickness to the flap and protect its vasculature.
Next, the distal aspect of the superficial temporal vascular pedicle is located and ligated so that the flap can be elevated from superior to inferior. The incision is made at the distal margin of the flap, and a plane is developed on top of the fascia of the temporalis muscle. This plane is then followed inferiorly, towards the base of the incision, cutting along the edges of the flap and ensuring hemostasis as the dissection proceeds. The inferior limit of dissection is the zygomatic arch. However, elevation does not typically proceed that far proximally, as the incision for access would then become visible inferior to the hairline.
However, techniques have been described that aim to minimize scarring, albeit at the expense of exposure. One such variant, applied predominantly to auricular reconstruction, uses an abbreviated transverse supraauricular incision to provide access to the subdermal plane, through which the flap can be elevated. This is a technically challenging approach, but it greatly diminishes visible postoperative scarring.[30] For more information about this procedure, please see Temporoparietal Fascia Flaps.
Radial Forearm Flap
The radial forearm flap is a workhorse flap frequently employed as both a regional reconstruction option for the hand and a free tissue transfer option for head and neck defects, especially involving the tongue and pharynx. This flap is very reliable with a robust blood supply, and it can be harvested with skin and fascia, fascia only, fascia and bone, or skin, fascia, and bone altogether.[31] Additionally, the radial forearm flap can be oriented with antegrade blow flood, retrograde blood flow, or as a flow-through flap. The diameter of the radial artery is roughly 2.5 mm, making it suitable for microvascular anastomosis. The venous drainage is very robust, as it typically flows through 2 small venae comitantes that run along the radial artery as well as through the cephalic vein, all of which join together in the antecubital fossa, an arrangement that keeps the venous microanastomosis comparatively simple if the flap is harvested for free tissue transfer.[32]
Ensuring adequate flow through the radial artery preoperatively is a critical part of the evaluation, as the radial forearm flap's location along the course of, but not at the end of, the radial artery's path requires that perfusion of tissue distal to the flap's donor site, namely, the hand, be assured before harvest. Because the ulnar and radial arteries anastomose through the deep and superficial palmar arches, loss of radial artery continuity in the forearm is not usually hemodynamically significant unless there is an obstruction in the ulnar artery. Use of a simple preoperative modified Allen test or vascular imaging will help to confirm ulnar artery flow.
The flap is marked out on the volar forearm, roughly centered over the radial artery, but ideally oriented to include the cephalic vein (see Image. Radial Forearm Flap Harvest). The flap's dimensions are dictated by the size of the defect, with essentially the entirety of the forearm's skin able to be perfused by the radial artery. Case reports have, in fact, described the use of radial forearm free flaps, including all of the forearm's skin, taken from the amputated arm of a polytrauma patient, to repair a wound on another limb in the same patient.[33][34]
For smaller deficits, the flap can extend as far distally as the wrist crease if maximal vascular pedicle length is required, or it can be placed more proximally on the forearm if shorter vessels are desired. While the artery can be shortened after a free radial forearm flap is harvested, shortening the veins requires removing their distal confluence, which necessitates either ligation of 1 or more draining veins or multiple, time-consuming venous anastomoses. Once the flap has been planned, an incision is made from its proximal margin up to the antecubital fossa; many surgeons use a "lazy S" shape to minimize later scar contracture. Subdermal flaps are then elevated on either side of this incision, which will later permit exposure of the vascular pedicle as it courses between and underneath the flexor carpi radialis and brachioradialis muscles.
The radial forearm flap itself can then be circumcised with a scalpel, down to the level of the paratenons. Elevation typically begins on the ulnar side of the flap, a technically straightforward step. Dissection proceeds just superficial to the paratenons of the flexor tendons, to prevent tendon exposure and postoperative tethering, and continues until the radial artery is encountered between the tendons of the flexor carpi radialis medially and the brachioradialis laterally.
The radial side of the flap is then elevated in the same plane, but care is taken to ensure the cephalic vein is ligated distally and elevated into the flap. In contrast, the superficial branch of the radial nerve, which exits the distal aspect of the brachioradialis muscle, is not incorporated into the flap. If desired, however, the medial and/or lateral antebrachial cutaneous nerves may be included in the flap to render it sensate.[35]
The palmaris longus tendon, if present, may also be included if needed for structural support, for example, if reconstructing a lip or an eyelid.[36][37] Once the radial artery is visualized, it can be ligated distally, along with its venae comitantes. The flap is then gently retracted, and the undersurface of the radial artery dissected out from between the aforementioned tendons, taking care to ligate any perforating branches that come off it unless bone is to be harvested as well.
The amount of radius bone that can be harvested is limited to roughly 40% of the bone's circumference, and the remaining bone is often plated prophylactically to reinforce it against future pathological fractures.[38] The vascular pedicle proximal to the flap is then dissected up to the antecubital fossa. Some surgeons prefer to leave the vessels bare, while others include a "beaver tail" of fatty tissue with them, which provides additional bulk and protects the vessels from kinking or inadvertent injury. The proximal extent of arterial dissection is the branch point of the recurrent radial artery, and the proximal extent of venous dissection is just proximal to the confluence of the venae comitantes and the cephalic vein (see Video. Radial Forearm Flap Before Transfer). Typically, accessing the venous confluence will require ligating 1 or more other branches within the antecubital venous plexus, also known as the "rat's nest."
Closure of the forearm incision is performed in layers, over a suction drain. The flap donor site can be covered with a skin graft, although if a fascia-only flap was harvested (such as for a mucosal reconstruction), the skin from the flap itself can be used to cover the donor site with the "hinged flap" technique. This variant involves harvesting a split-thickness skin graft from the radial forearm flap before flap harvest, but leaving the skin graft attached at the wrist crease so that it can "hinge" back into place once flap harvest is complete.[39] After skin grafting, the arm is dressed, with the hand often splinted in extension to prevent wrist contracture during healing. For more information about this procedure, please see Radial Forearm Tissue Transfer.
Gracilis Flap
The gracilis flap, like the radial forearm flap, can be transferred as a regional flap or used for free tissue transfer. When used regionally, lower extremity and pelvic reconstruction are common indications. As a free flap, the gracilis has been the gold-standard option for facial reanimation for many years, and it is also used for upper-extremity functional restoration after brachial plexus injuries or Volkmann's contracture, among others.
What makes the gracilis flap unusual is that, in addition to bringing fat and skin with the muscle tissue, the muscle itself can be transferred with its motor nerve, thereby rendering it functional and capable of voluntary contraction.[40][41][42][41][42] The gracilis is a long, comparatively slim muscle within the adductor compartment of the medial thigh, innervated by a branch of the obturator nerve and perfused by the anterior branch of the adductor artery. Removal of the gracilis typically causes only transient gate abnormalities, unless the obturator nerve is divided too proximally and inadvertently denervates the adductor longus as well.
The incision used to approach the gracilis flap harvest runs parallel and roughly 1 to 2 cm posterior to a line drawn between the medial condyle of the tibia and the insertion of the adductor muscle tendons on the medial pubis; the length of the incision will depend on the desired length of the gracilis muscle (see Image. Gracilis Free Flap for Facial Reanimation). Dissection proceeds through the subcutaneous fat, taking care to avoid injury to the great saphenous vein, which will be encountered within it. The vein may be harvested for grafting, if needed.
The gracilis muscle is located between the adductor longus muscle anteriorly and the adductor magnus posteriorly, and can be identified by visualizing the neurovascular pedicle that enters its deep surface approximately 8 cm inferior to the pubic tubercle. There may be more than 1 pedicle, but the one at this location is typically the largest and contains the vessels most appropriate for microsurgical anastomosis. The artery measures 1 to 1.5 mm in diameter, and its venae comitantes, through which the flap will drain, measure 2 to 3 mm. The vessels enter the muscle perpendicularly, whereas the nerve approaches at an oblique angle, originating superolateral but entering the muscle at the same location as the vessels.
After identification of the neurovascular pedicle, the gracilis can be circumferentially liberated from its fascial attachments, remaining anchored superiorly and inferiorly, as well as at the pedicle. The muscle may then be incised and the appropriate amount harvested, incorporating the neurovascular pedicle as close to the center of the flap as is practical. For facial reanimation, a portion roughly 14 cm in length and half the width of the muscle belly is taken.
The vascular pedicle is not long, only 5 to 6 cm at most, and it originates from the femoral vessels or the deep femoral vessels. Care should be taken during ligation to ensure that a large, bleeding vessel does not retract deep into the thigh. Due to the risk of major hemorrhage going undetected for a prolonged period, the harvest site should be closed in layers over a suction drain, allowing the care team to monitor any postoperative fluid accumulation in the wound.
If used as a functional free muscle, the gracilis must be inset under tension to produce effective contraction with motor nerve stimulation. After the muscle has been inset, the blood vessels are anastomosed to the recipient-site vessels, and the motor nerve is then coapted to the donor nerve (see Image. Vascular Anastomoses). While verification of flap perfusion through the vascular anastomoses should be immediate and repeated frequently throughout the early postoperative course, the effectiveness of the neurorrhaphy will not be evident until 6 to 9 months postoperatively, and optimizing motor function will typically require a course of physical therapy (see Video. Gracilis Transfer for Facial Reanimation). For more information about this procedure, please see Gracilis Tissue Transfer.
Complications
The complication that typically worries surgeons most when performing axial flap transfers is flap necrosis, which usually occurs at the distal tip, farthest from the vascular pedicle, but may involve the entire transferred tissue, particularly with a microvascular free flap. Tissue necrosis is caused by vascular insufficiency, which may result from excessive tension or kinking of the pedicle vessels, pressure on the pedicle vessels (generally due to a hematoma or infection), or thrombosis of the vessels.[43] In all of these cases, the venous drainage is 3 times more likely to be affected than the arterial supply because it is a lower-pressure system with lower velocity flow and thinner walls that are less resilient to external compression.[44]
A flap that appears edematous, firm, and dusky or ecchymotic, particularly with dark blood oozing from the incision lines, is liable to be experiencing venous outflow insufficiency. With sufficient time, venous obstruction within the flap may also lead to arterial inflow obstruction, making flap salvage even more challenging. If the artery is affected in isolation, the flap will be pale, with minimal or absent capillary refill, supple, and cool (unless it is located within a body cavity).
A mnemonic developed by Dr Scott Bevans to guide monitoring of axial flaps via physical examination is "Check with The Chief, Big Dog," which directs the clinician to assess color, temperature, capillary refill, bleeding, and Doppler signal. Doppler examination of a flap with arterial insufficiency will reveal a lack of any pulses, while a flap with venous obstruction may still have an arterial pulse, albeit a sharper "hammer" pulse due to altered hemodynamics. Using a 21-gauge needle to prick a flap without arterial inflow will cause no bleeding, whereas a flap with venous obstruction only will bleed dark blood faster than blood would normally issue from a pinprick.
In some cases, venous obstruction can be addressed by applying leeches to the flap, which will remove venous blood as well as infuse a potentially helpful anticoagulant, but this should always be accompanied by administration of a fluoroquinolone antibiotic to prevent soft tissue infection with Aeromonas hydrophila that is often present in the gut of the leech.[45][46] Alternatively, thrombolytics or anticoagulants may be injected directly into the flap instead.[47][48] Ideally, however, the underlying vascular problem should be addressed, generally in the operating room.
This may require evacuating a hematoma and securing hemostasis, releasing tension on the pedicle or reorienting it to reduce kinking, or, in the case of free tissue transfer, disconnecting the flap from its blood supply to clear thrombus from the vein and/or artery before restoring the vascular anastomoses. Whatever intervention is required should be performed as soon as possible to limit the extent of tissue necrosis and reduce the likelihood of a "no-reflow" phenomenon, in which disseminated clotting within the flap's microvasculature prevents tissue reperfusion even if all of the other insults have been corrected. Irreversible ischemic damage occurs after approximately 6 hours without blood flow, but perfusion can be restored in over 90% of cases if the problem is recognized and corrected promptly.[49][43] If a flap's blood supply is irreversibly compromised and tissue death occurs, areas of limited necrosis may be managed with local wound care, including conservative debridement and wet-to-dry dressings or antibiotic ointment, with or without hyperbaric oxygen.[50] Complete flap loss, on the other hand, may require debridement and replacement with another flap, a skin graft, or allowing the wound to heal by secondary intention.
Other complications of flap transfer include infection, scarring, contracture, cosmetic dissatisfaction, and damage to surrounding anatomy during flap harvest. Among the more likely potential iatrogenic injuries are sensory and motor nerve trauma, such as damage to the superficial branch of the radial nerve, the frontal branch of the facial nerve, and the proximal obturator nerve, which can cause loss of sensation or adjacent muscle weakness. Cosmetic complaints may arise from poor color, texture, or hair match between the flap and the recipient area, or contour irregularities due to inappropriate sizing of the flap, typically with too much thickness or surface area in too small a defect, which results in a heaped-up or "pincushion" appearance. In some cases, the flap may be debulked without risking damage to its blood supply, but not in all. Differences in skin quality and hair growth are often satisfactorily addressed with laser resurfacing or hair removal.
Ultimately, each flap has a unique risk profile due to its harvest site. Harvest of extremity flaps, like fibula and radial forearm flaps, can compromise the perfusion of distal anatomy, such as the foot or hand, if an appropriate preoperative vascular evaluation is not performed. Similarly, bone removal can cause pathological fractures or mobility decrements, such as shoulder or ankle instability after incautious harvest of a scapula or fibula flap. Flaps, like the temporoparietal fascia flap, that are harvested under the scalp may cause alopecia if excessive cautery is used. The examples are nearly endless, and it is the surgeon's responsibility to identify, mitigate, and counsel the patient about these risks appropriately.
Clinical Significance
Axial flaps provide versatile, highly reliable options for reconstructing medium- to large skin or composite tissue defects arising from oncologic resection, traumatic injury, or other causes. They can be employed to replace missing skin, mucosa, fascia, muscle, and bone, and can be used in areas with poor vascularity because they bring their own blood supply to the defect. Axial flaps are also useful for closing wounds that cannot heal spontaneously or that have undergone prior reconstruction with skin grafts or local flaps that subsequently failed. More complex axial flap transfers, however, may be challenging to perform or may require multiple surgical stages to complete (eg, the interpolated paramedian forehead flap and the delayed deltopectoral flap) and should be performed only by trained reconstructive surgeons. Similarly, effective management of flap complications requires an experienced eye to identify them and provide the appropriate treatment in a timely fashion.
Enhancing Healthcare Team Outcomes
Optimal outcomes with axial flaps depend on precise surgical judgment, disciplined perioperative strategy, and clear role delineation across the team. Surgeons and advanced clinicians must integrate detailed knowledge of angiosomes and vascular anatomy into preoperative planning, which may include handheld Doppler assessment, computed tomography angiographic mapping in complex cases, and thoughtful flap selection tailored to defect size, location, and patient comorbidities. Intraoperatively, meticulous technique to preserve the vascular pedicle, minimize tension, and ensure adequate inset is critical.
At the same time, the anesthesia team supports hemodynamic stability and avoids vasoconstrictive states that could compromise perfusion. Postoperatively, nurses and advanced practitioners play a central role in standardized flap monitoring protocols, serial clinical exams (color, turgor, capillary refill, temperature), adjunctive monitoring when indicated, and early escalation pathways for suspected vascular compromise, facilitating timely return to the operating room when salvage is possible.
Interprofessional communication and coordinated care are essential for reducing complications and improving patient-centered outcomes. Pharmacists contribute by optimizing anticoagulation or antiplatelet strategies when appropriate, guiding antibiotic stewardship, and avoiding medications that may impair microvascular flow. Nursing teams ensure adherence to positioning protocols, pressure offloading, and wound care, while also providing patient education on activity restrictions and warning signs.
Physical and occupational therapists assist with early, protected mobilization that preserves flap integrity and function. Structured handoffs, shared checklists, and multidisciplinary rounds enhance situational awareness, align goals of care, and reduce variability. This coordinated approach improves flap survival, minimizes infection and thrombotic events, and supports functional recovery and patient satisfaction.
Media
(Click Image to Enlarge)
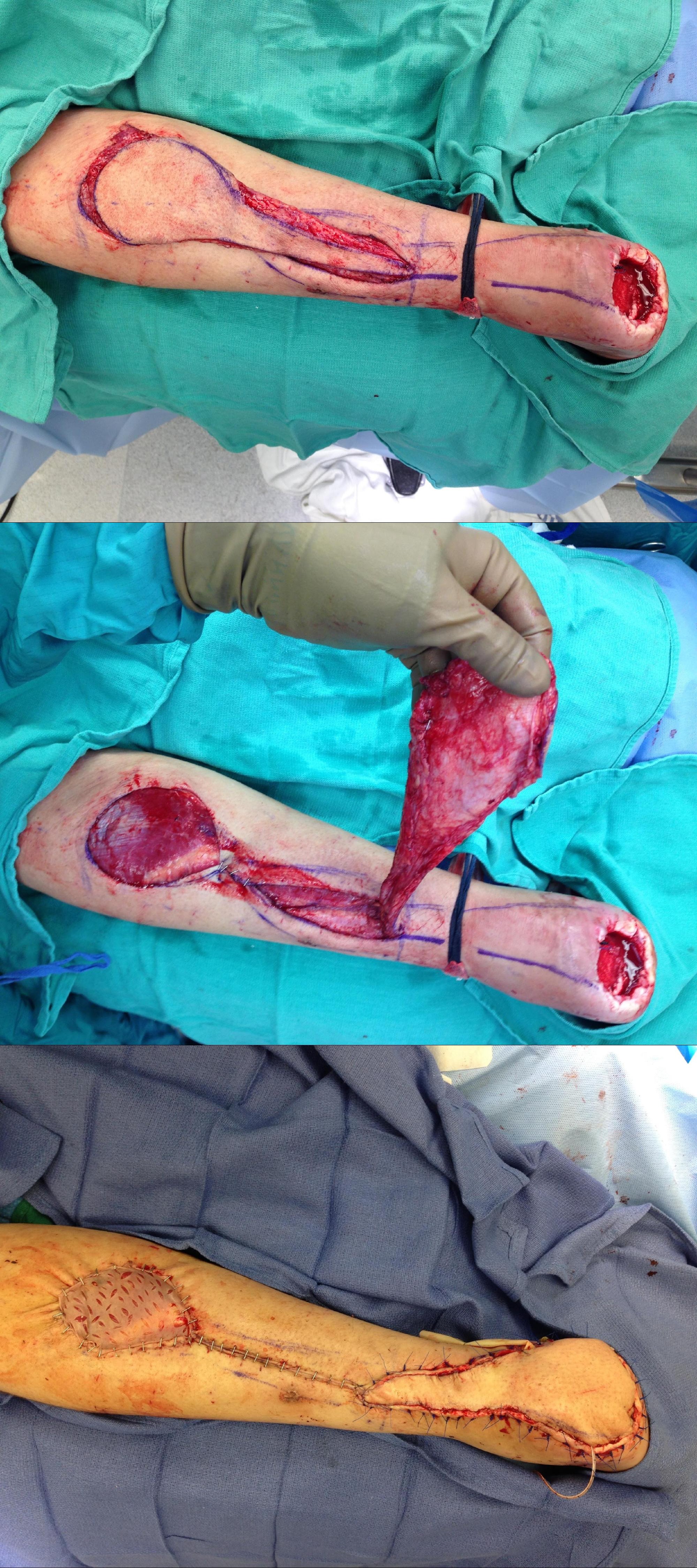
Reverse Sural Artery Flap. This rotation flap is being used to reconstruct a nonhealing heel ulcer.
Contributed by MA Dreyer, DPM, FACFAS
(Click Image to Enlarge)
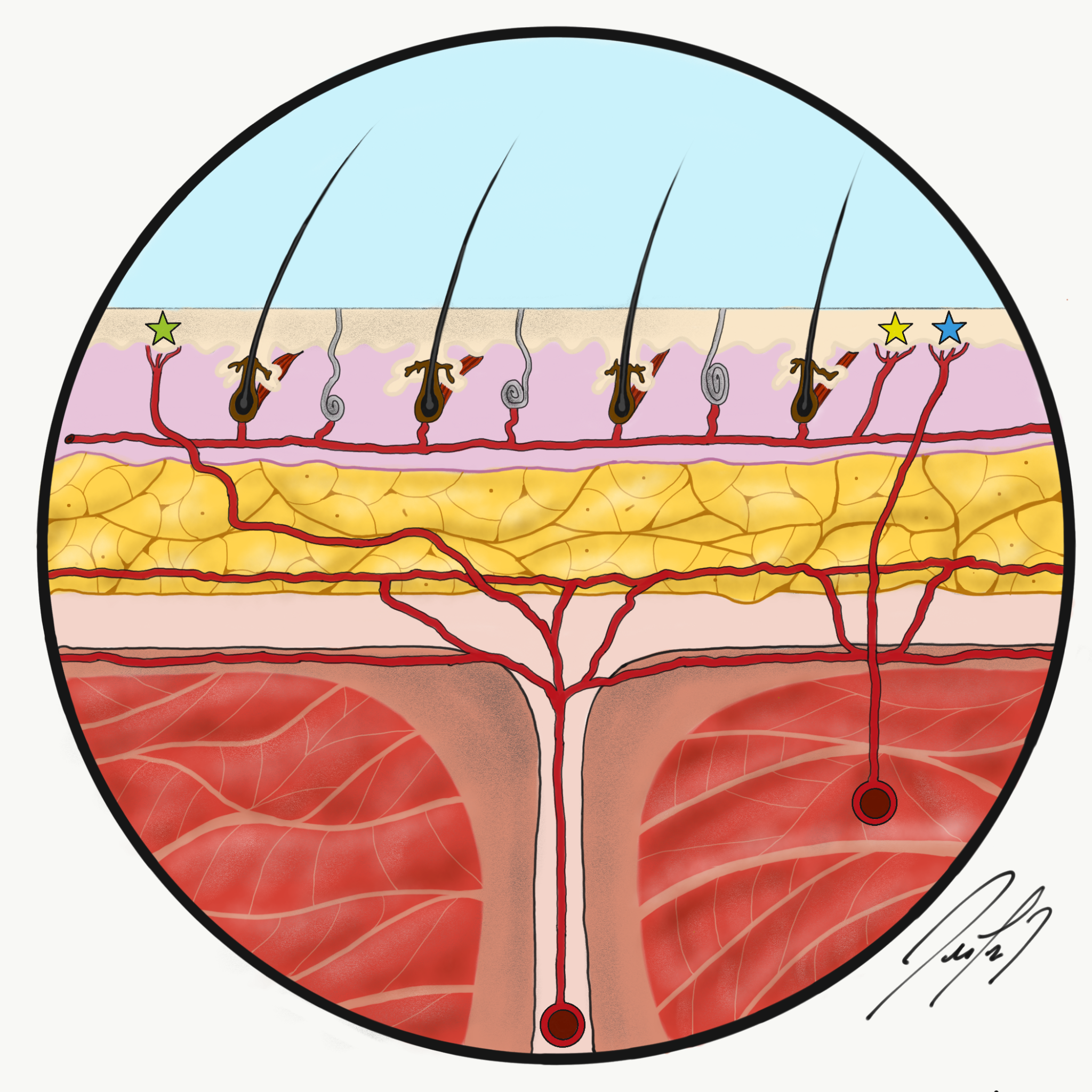
Fasciocutaneous Flap Perfusion. The green star indicates a septocutaneous perforator, the yellow star is a direct cutaneous perforator, and the blue star is a musculocutaneous perforator.
Contributed by FL De Cicco, MD
(Click Image to Enlarge)
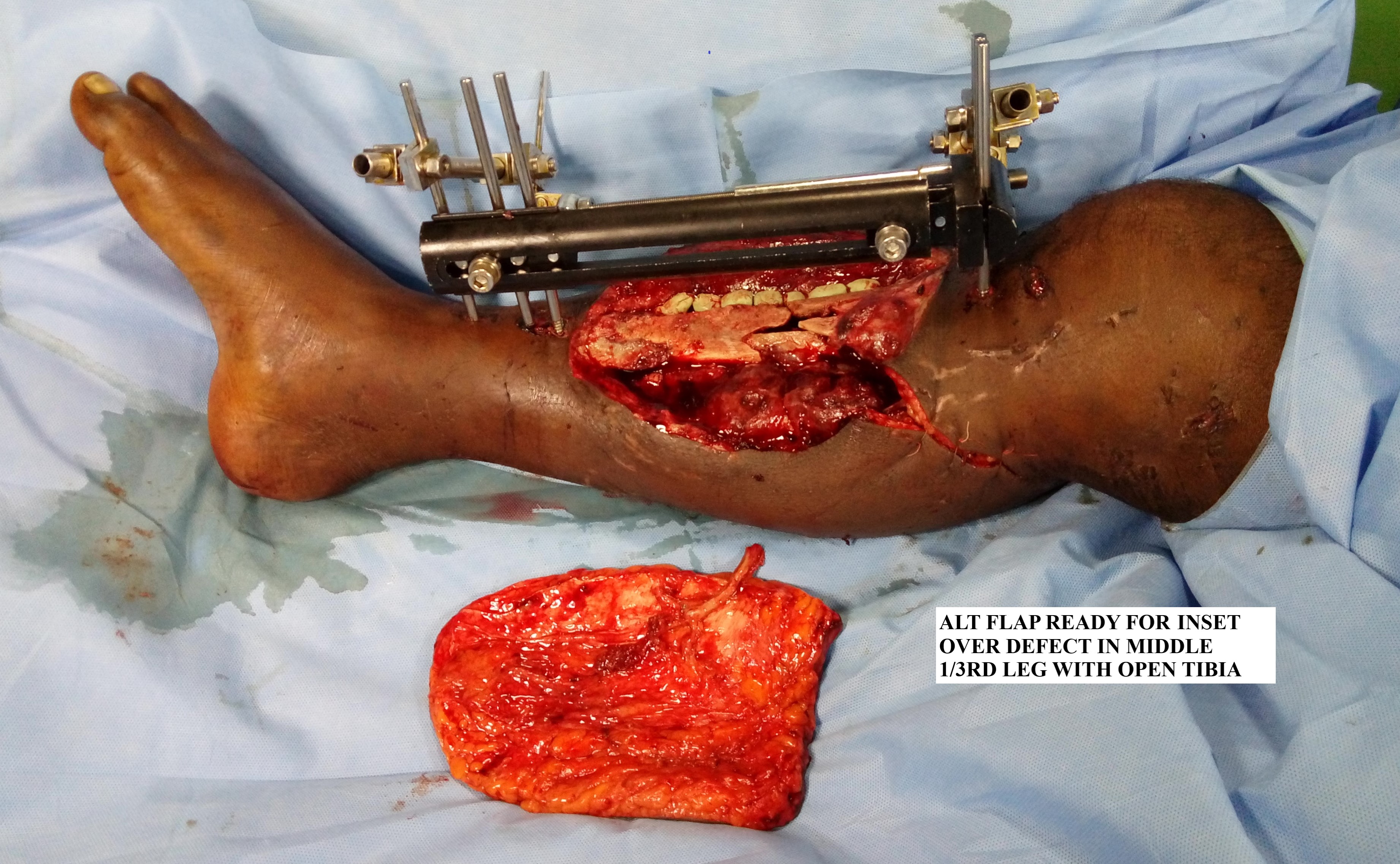
Anterolateral Thigh Flap Before Inset. The free flap is seen prior to being inset over the defect in the middle third of the leg.
Contributed by L Alexander, MD
(Click Image to Enlarge)

Anterolateral Thigh Flap After Inset. The free flap is seen after its inset over the defect in the middle third of the leg.
Contributed by L Alexander, MD
(Click Image to Enlarge)

Abbe-Estlander Flap.
Contributed by R Winters, MD
(Click Image to Enlarge)
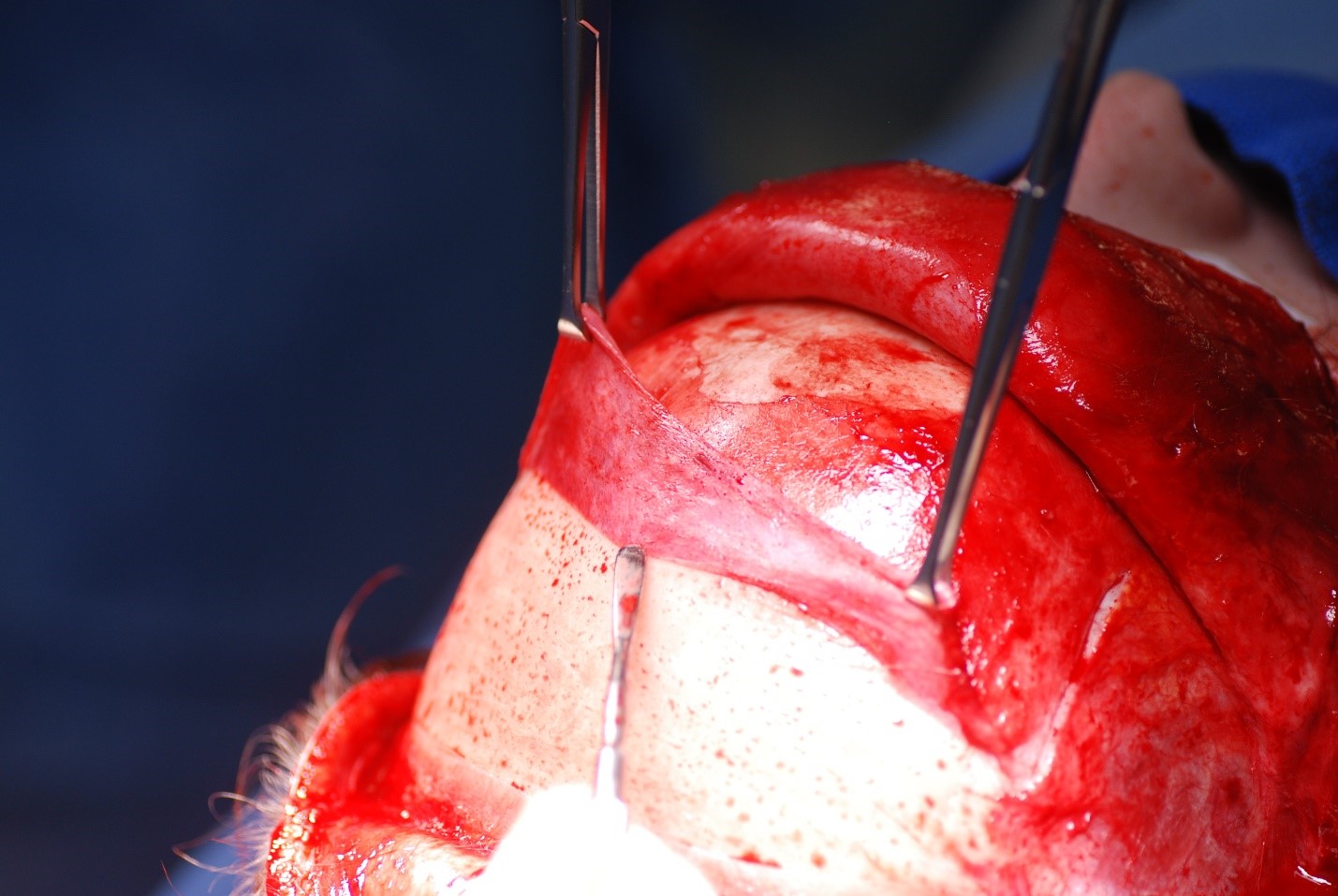
Pericranial Flap Elevation. The pericranial flap can be elevated separately from the forehead flap if necessary.
Contributed by MH Hohman, MD, FACS
(Click Video to Play)
Modified Allen Test. The modified Allen test assesses whether the ulnar artery can adequately supply the hand if the radial artery is ligated, as during radial forearm flap harvest.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
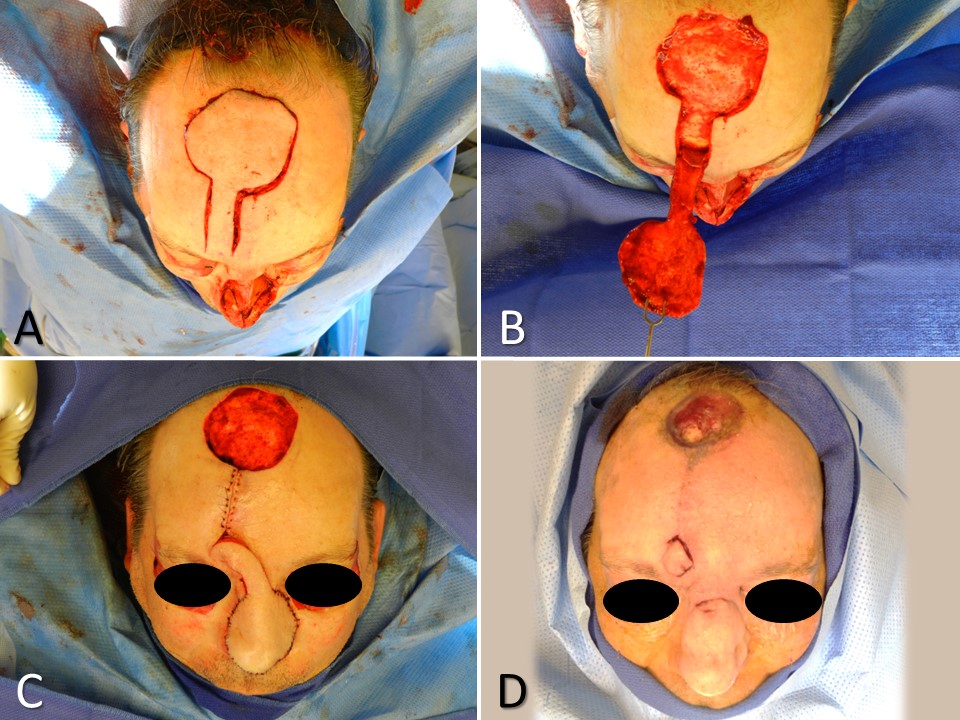
Paramedian Forehead Flap for Nasal Reconstruction. A subtotal nasal defect due to Mohs resection of basal cell carcinoma requires multilayer reconstruction, including a large paramedian forehead flap (A). The skin paddle is elevated in a subdermal plane, the pedicle in the supraperiosteal plane, and the base in the subperiosteal plane (B). The flap is transferred, and the secondary defect is left to heal by secondary intention due to its size (C). The pedicle is divided 3 weeks later as the secondary defect continues to heal (D).
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
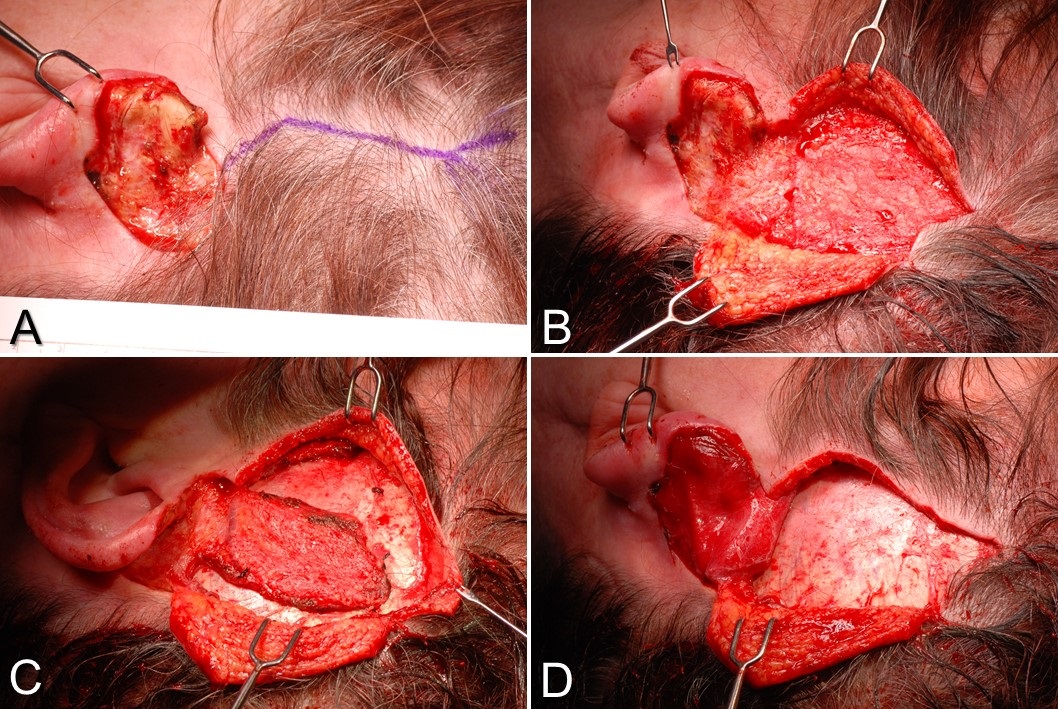
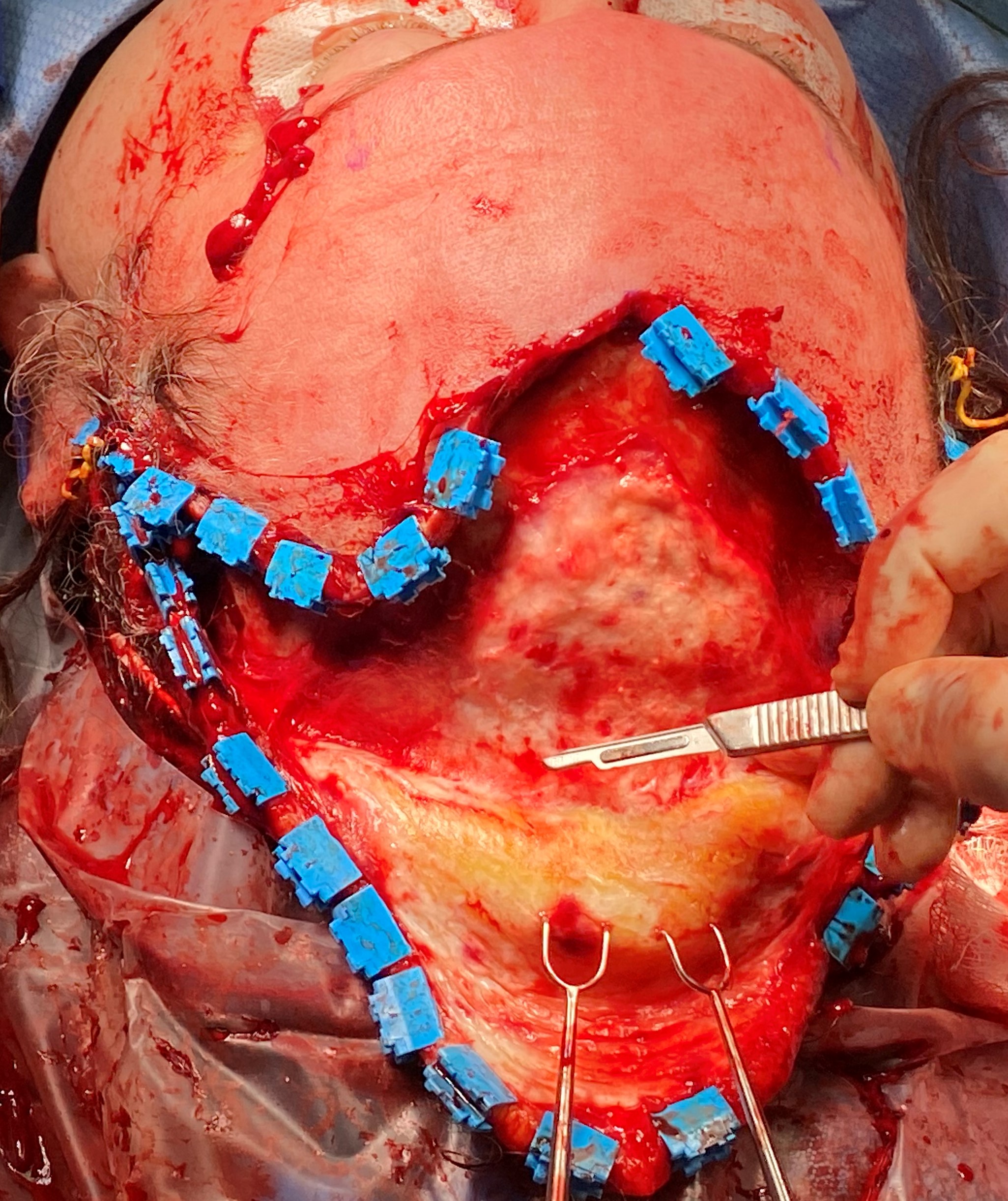
Temporoparietal Fascia Flap. A) This is a postauricular defect from Mohs surgery with too much bare cartilage for a skin graft alone to survive. A Y-shaped incision is planned, paralleling the course of the superficial temporal artery. B) The scalp flaps are elevated in a subdermal plane, exposing the temporoparietal fascia. C) The temporoparietal fascia flap is incised on 3 sides, with the pedicle intact inferiorly. D) The temporoparietal fascia flap is transferred into the defect, after which the scalp will be closed in layers, and a skin graft will be applied to the flap.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
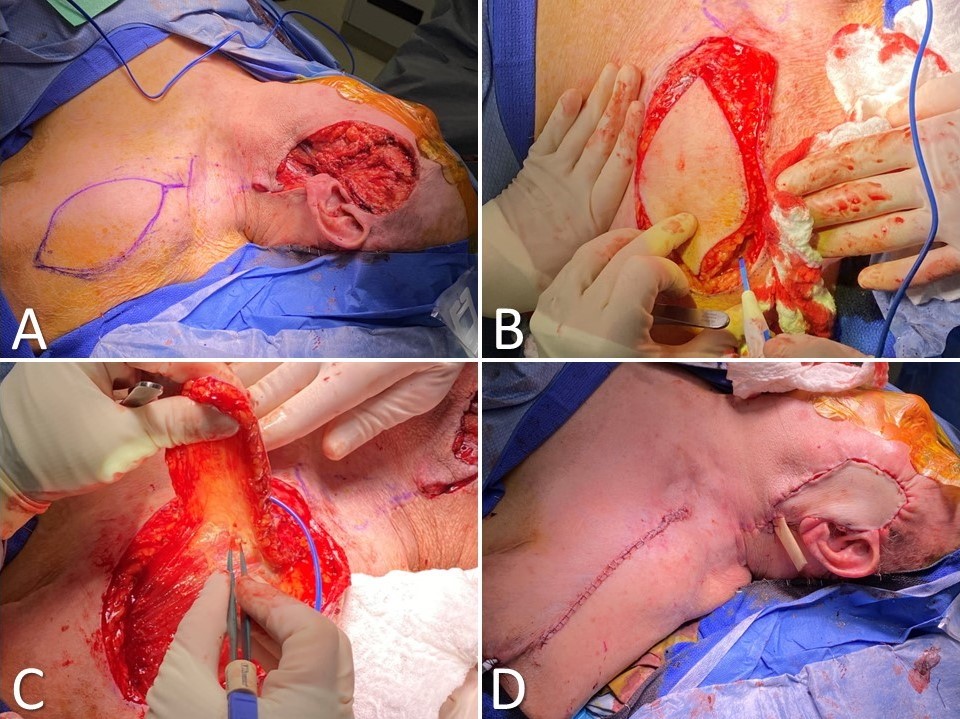
Supraclavicular Artery Island Flap for Facial Reconstruction. (A) Parotidectomy and skin defect due to dermatosarcoma with supraclavicular artery island flap (SCAIF) drawn out incorporating the supraclavicular artery; (B) the skin paddle is circumcised down to the level of the deltoid muscle; (C) the flap is elevated, ensuring the vascular pedicle remains intact medially; (D) the flap is tunneled into the defect and inset over a Penrose drain, whereas the donor site is closed primarily.
Contributed by MW Herr, MD; KG Anderson MD, FACS; and MH Hohman, MD, FACS
(Click Image to Enlarge)
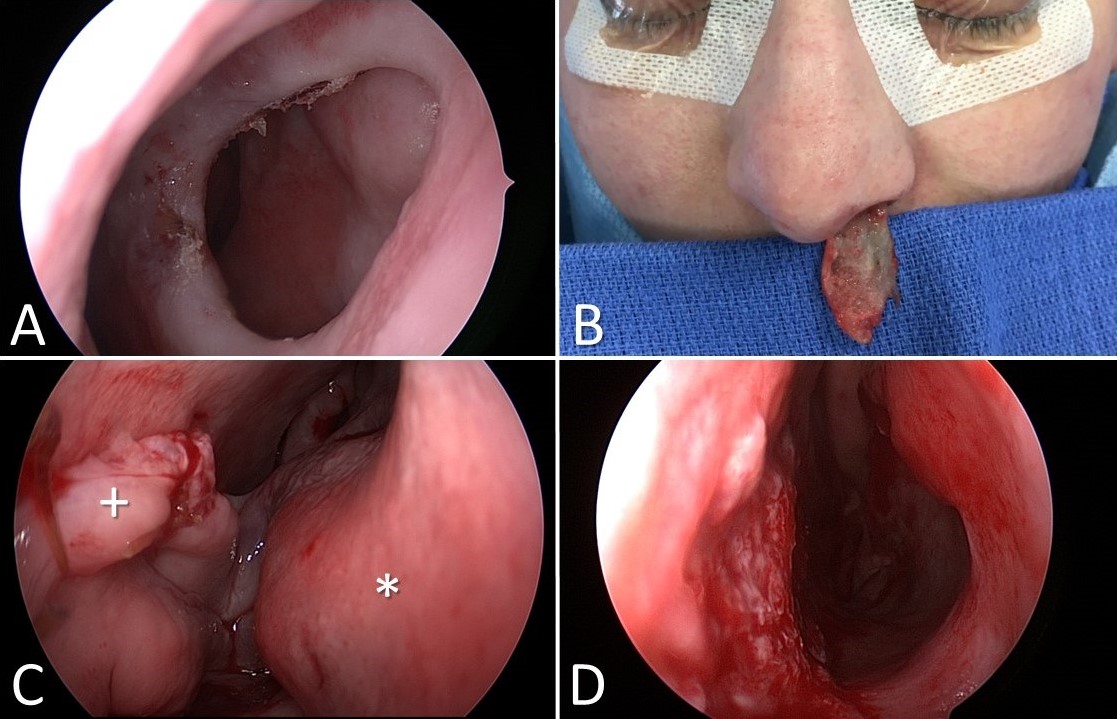
Inferior Turbinate Flap Reconstruction for Nasal Septal Perforation. Nasal septal perforation (A). The left inferior turbinate is separated from the lateral nasal wall and incised along its length to permit the removal of the conchal bone while remaining pedicled anteriorly (B). The flap is transferred and inset into the septal perforation. The plus sign indicates the flap, and the asterisk marks the remaining in situ anterior face of the inferior turbinate, with the pedicle running across the nasal cavity between them (C). The pedicle is divided 3 weeks later, leaving a patent nasal cavity and an intact nasal septum (D).
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
Posterior Scalp Advancement Flap. The flap is elevated in a subcutaneous plane using a #15 blade, which improves its ability to stretch and lower the frontal hairline.
Contributed by Marc H Hohman, MD, FACS
(Click Image to Enlarge)
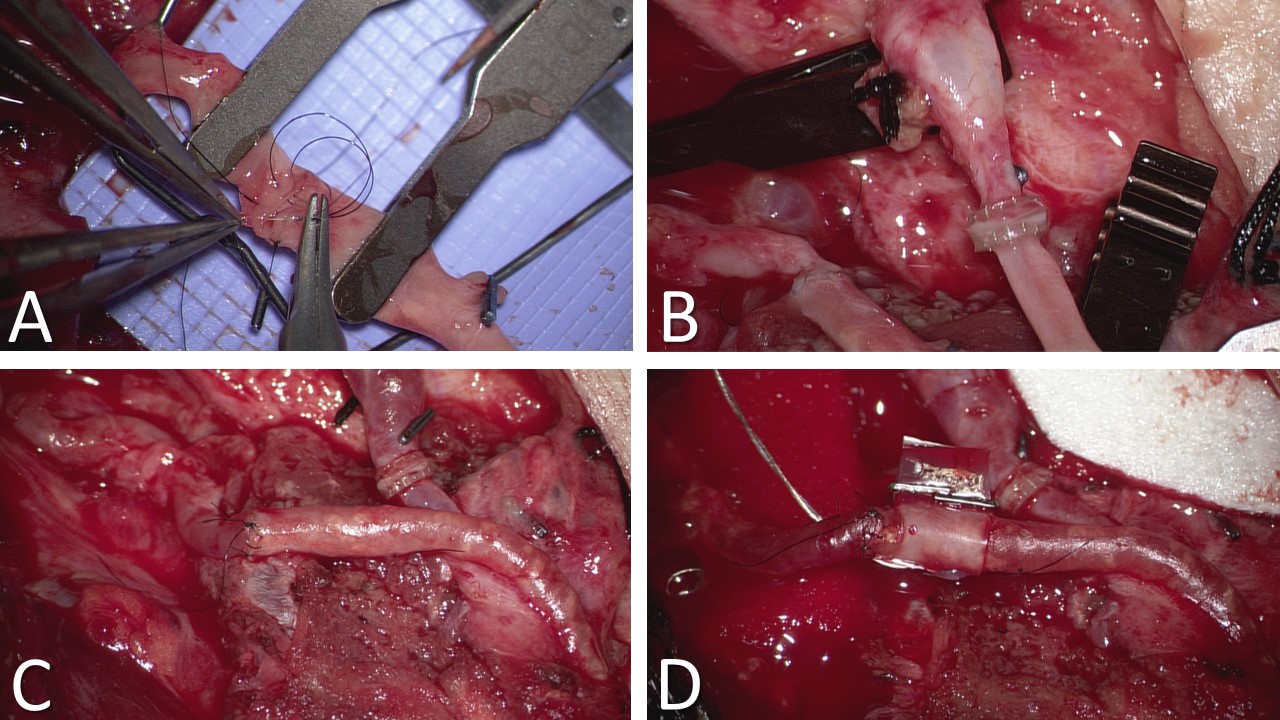
Vascular Anastomoses. (A) Arterial anastomosis between the facial artery and the peroneal artery was performed under microscopy using 8-0 nylon. (B) Venous anastomosis between the facial vein and a peroneal vena comitans using a 3 mm coupler. (C) Completed vascular anastomoses. (D) An implantable Doppler probe is wrapped around the arterial anastomosis to facilitate monitoring of flap perfusion. The implantable Doppler probe is particularly useful for buried flaps, such as bone-only fibula free flaps and gracilis flaps for facial reanimation. Once arterial monitoring is no longer required, the Doppler wire is gently withdrawn from the patient, and the probe wrapped around the arterial anastomosis is left in place.
Contributed by MH Hohman, MD, FACS, and WJ Harsha, MD
(Click Image to Enlarge)
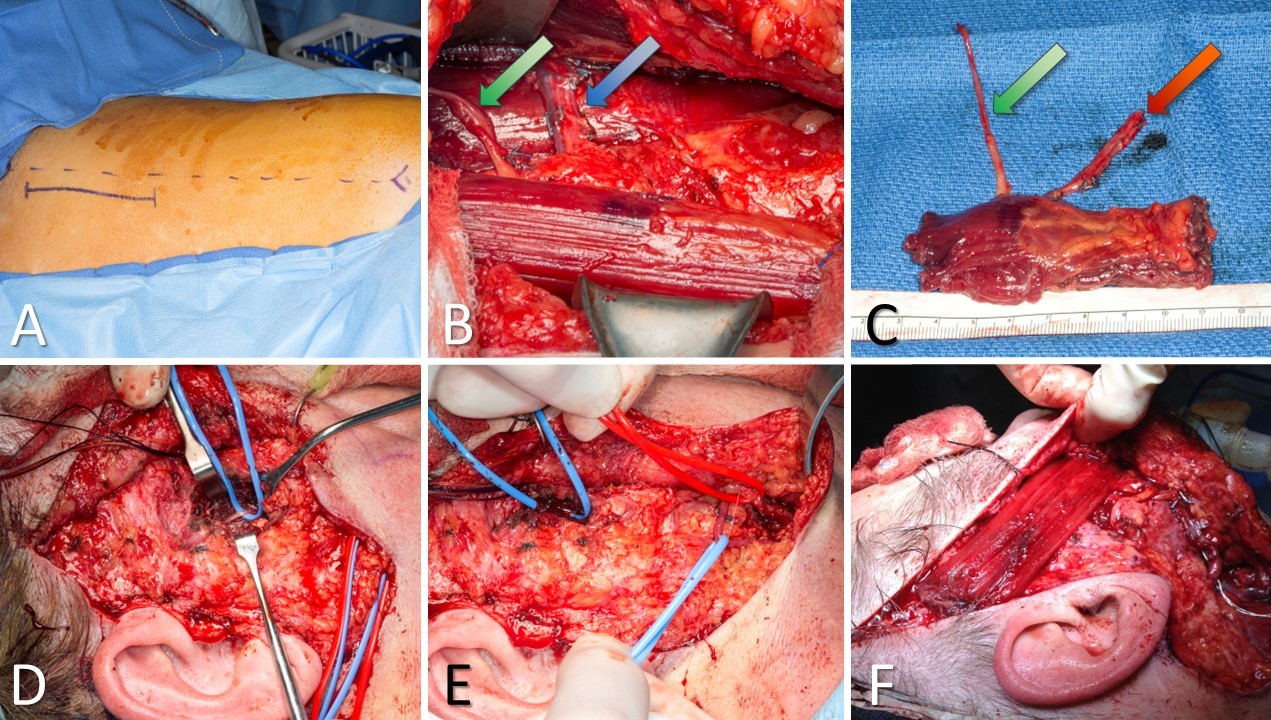
Gracilis Free Flap for Facial Reanimation. A) The incision is marked 2 cm posterior to a line drawn between the medial tibial epicondyle and the insertion of the adductor tendons on the pubis. B) The gracilis muscle is exposed, with the obturator nerve (green arrow) and the adductor artery with its 2 venae comitantes (blue arrow). C) The gracilis free flap harvested and thinned, with the obturator nerve (green arrow) and the adductor artery with its 2 venae comitantes (red arrow). D) Masseteric nerve isolated for coaptation to the obturator nerve on the gracilis flap. E) Facial artery (red loop) and facial vein (blue loop) isolated for anastomosis to the adductor artery and a vena comitans on the gracilis flap. F) Gracilis flap inset between the modiolus of the oral commissure and the temporalis fascia. An implantable Doppler probe has been placed to monitor the perfusion of this buried flap.
Contributed by MH Hohman, MD; SE Bevans, MD; JM Robitschek, MD; and WJ Harsha, MD
(Click Video to Play)
Radial Forearm Flap Before Transfer. The radial artery is pulsating, and atop it lies the cephalic vein, which courses medially as it travels proximally. Situated lateral to the pedicle is the lateral antebrachial cutaneous nerve, which can be used to provide sensation to the flap.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
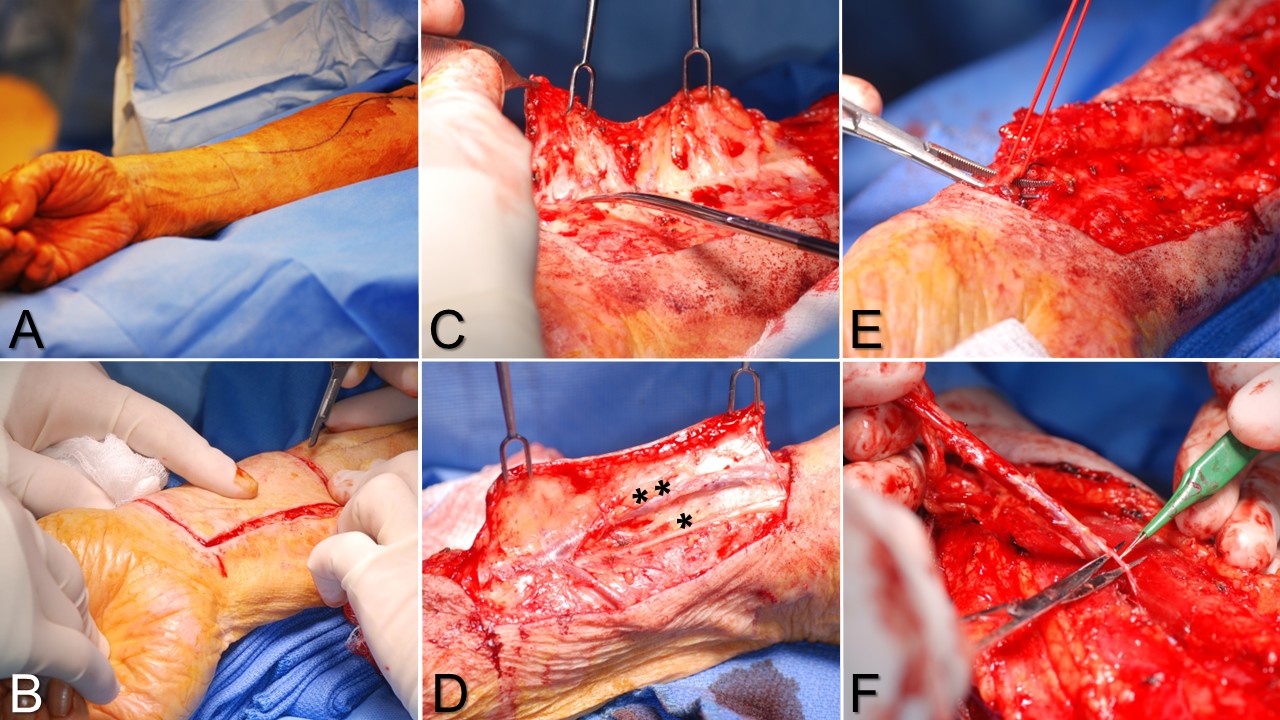
Radial Forearm Flap Harvest. A) The flap is designed centered over the radial artery, with a tissue paddle of the correct size and a curvilinear incision on the forearm to reduce scar contracture. B) The flap is circumcised down to the paratenons. C) Elevation begins on the ulnar side, proceeding superficial to the paratenons up to the radial artery. D) Elevation on the radial side keeps the cephalic vein** within the flap to improve venous drainage but leaves the superficial branch of the radial nerve* in the arm to preserve dorsal hand and thumb sensation. E) The radial artery and its venae comitantes are ligated before elevation of the vascular pedicle from distal to proximal. F) The pedicle is elevated from between the brachioradialis and the flexor carpi radialis muscles, ligating perforating until reaching the confluence of the venae comitantes with the cephalic vein in the antecubital fossa, which marks the proximal extent of the vascular pedicle.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)

Auricular Reconstruction with Temporoparietal Fascia Flap and Supraclavicular Full-Thickness Graft. The defect was caused by Mohs resection of a basal cell carcinoma, leaving a substantial area of bare cartilage exposed. The decision was made to interpose a thin temporoparietal fascia flap between the wound bed and the skin graft to improve the likelihood of graft healing. The Y-shaped incision, through which the temporoparietal fascia flap was elevated and transferred, can be seen at right.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
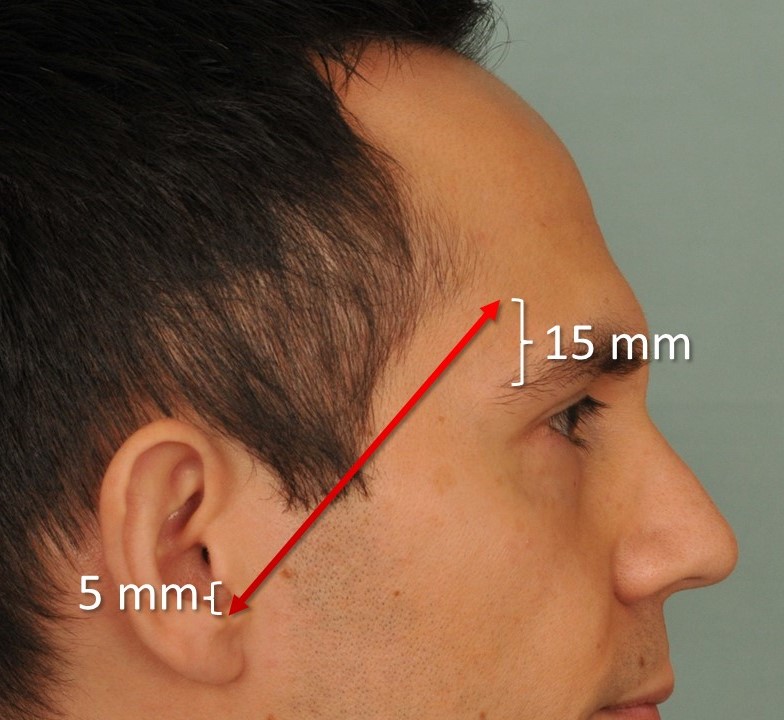
Pitanguy Line. This image illustrates the Pitanguy line, which runs from a point 5 mm inferior to the tragus to a point 15 mm superior to the lateral brow. This line approximates the course of the frontal branch of the facial nerve.
Contributed by MH Hohman, MD, FACS
(Click Video to Play)
Gracilis Transfer for Facial Reanimation. A 63-year-old male with left-sided congenital facial palsy underwent contralateral gracilis functional free muscle transfer, using the facial vessels and the masseteric nerve.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
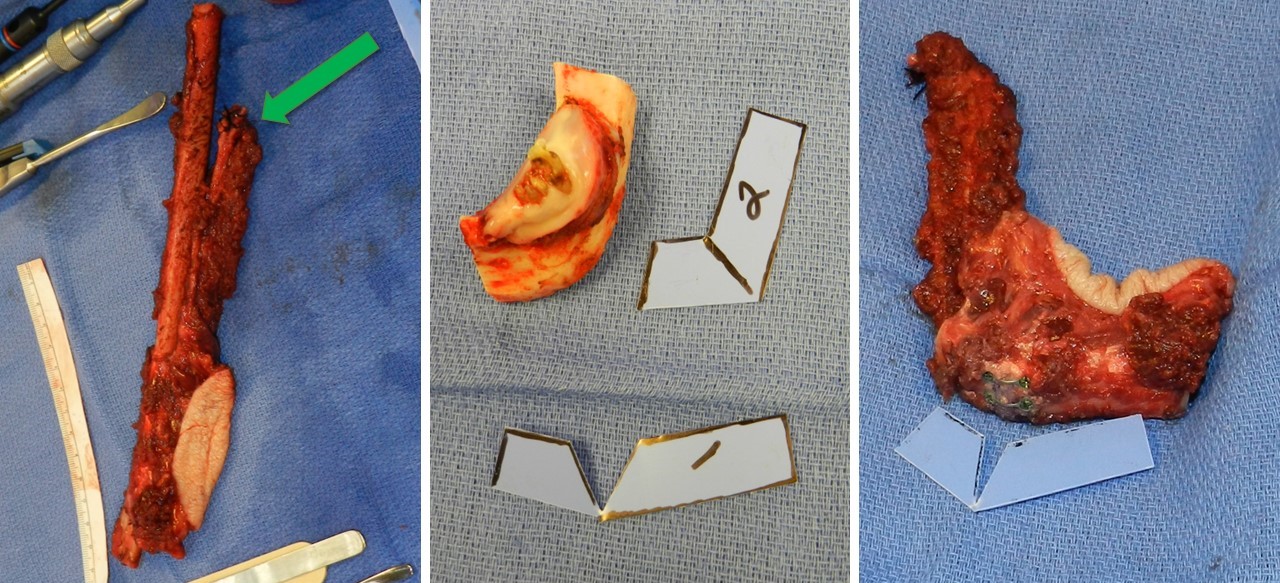
Fibula Free Flap Harvest and Closing Ostectomy. The fibula free flap is harvested (left), providing roughly 20 cm of bone in this patient and a skin paddle to fill an intraoral mucosa defect. The vascular pedicle is marked with a green arrow. The resected segment of the mandible is curved (center). A template is improvised to guide a closing ostectomy that conforms the harvested fibula to the contour of the resected segment of the mandible. After a closing ostectomy is performed, the fibula is bent and plated to follow the curve of the resected segment of the mandible (right).
Contributed by MH Hohman, MD, FACS, and WJ Harsha, MD
References
Mankin KT. Axial Pattern Flaps. The Veterinary clinics of North America. Small animal practice. 2017 Nov:47(6):1237-1247. doi: 10.1016/j.cvsm.2017.06.008. Epub 2017 Aug 7 [PubMed PMID: 28797554]
Level 3 (low-level) evidenceMcGregor IA, Morgan G. Axial and random pattern flaps. British journal of plastic surgery. 1973 Jul:26(3):202-13 [PubMed PMID: 4580012]
Zito PM, Hohman MH, Mazzoni T. Paramedian Forehead Flaps. StatPearls. 2026 Jan:(): [PubMed PMID: 29763107]
Kunert P. [A simple classification system for all skin flaps]. Handchirurgie, Mikrochirurgie, plastische Chirurgie : Organ der Deutschsprachigen Arbeitsgemeinschaft fur Handchirurgie : Organ der Deutschsprachigen Arbeitsgemeinschaft fur Mikrochirurgie der Peripheren Nerven und Gefasse : Organ der V.... 1995 May:27(3):124-31 [PubMed PMID: 7622125]
Pavletic MM. Canine axial pattern flaps, using the omocervical, thoracodorsal, and deep circumflex iliac direct cutaneous arteries. American journal of veterinary research. 1981 Mar:42(3):391-406 [PubMed PMID: 7271004]
Level 3 (low-level) evidenceSaber AY, Hohman MH, Dreyer MA. Basic Flap Design. StatPearls. 2026 Jan:(): [PubMed PMID: 33085399]
Taylor GI, Corlett RJ, Ashton MW. The Functional Angiosome: Clinical Implications of the Anatomical Concept. Plastic and reconstructive surgery. 2017 Oct:140(4):721-733. doi: 10.1097/PRS.0000000000003694. Epub [PubMed PMID: 28953725]
Demir A, Kucuker I, Keles MK, Demirtas Y. The effect of learning curve on flap selection, re-exploration, and salvage rates in free flaps; A retrospective analysis of 155 cases. Microsurgery. 2013 Oct:33(7):519-26. doi: 10.1002/micr.22153. Epub 2013 Aug 14 [PubMed PMID: 23946161]
Level 2 (mid-level) evidenceDhar SC, Taylor GI. The delay phenomenon: the story unfolds. Plastic and reconstructive surgery. 1999 Dec:104(7):2079-91 [PubMed PMID: 11149772]
Etzkorn JR, Zito PM, Hohman MH, Council M. Advancement Flaps. StatPearls. 2026 Jan:(): [PubMed PMID: 28613735]
Gaboriau HP, Murakami CS. Skin anatomy and flap physiology. Otolaryngologic clinics of North America. 2001 Jun:34(3):555-69 [PubMed PMID: 11447002]
Pavletic MM. New techniques in small animal reconstructive surgery. The veterinary quarterly. 1997 Apr:19(sup1):25-27 [PubMed PMID: 22047419]
Level 3 (low-level) evidenceHwang K, Son JS, Ryu WK. Smoking and Flap Survival. Plastic surgery (Oakville, Ont.). 2018 Nov:26(4):280-285. doi: 10.1177/2292550317749509. Epub 2018 Jan 9 [PubMed PMID: 30450347]
Allen EV. Thrombo-Angiitis Obliterans. Bulletin of the New York Academy of Medicine. 1942 Mar:18(3):165-89 [PubMed PMID: 19312256]
Menick FJ. A 10-year experience in nasal reconstruction with the three-stage forehead flap. Plastic and reconstructive surgery. 2002 May:109(6):1839-55; discussion 1856-61 [PubMed PMID: 11994582]
Correa BJ, Weathers WM, Wolfswinkel EM, Thornton JF. The forehead flap: the gold standard of nasal soft tissue reconstruction. Seminars in plastic surgery. 2013 May:27(2):96-103. doi: 10.1055/s-0033-1351231. Epub [PubMed PMID: 24872749]
Tallal RE, Estawrow MA. Obliteration and Contouring of Comminuted Anterior Wall Frontal Sinus Fracture Using Pericranial Flaps. Plastic and reconstructive surgery. Global open. 2021 Aug:9(8):e3670. doi: 10.1097/GOX.0000000000003670. Epub 2021 Aug 9 [PubMed PMID: 34386309]
Giurintano J, McDermott MW, El-Sayed IH. Vascularized Pericranial Flap for Endonasal Anterior Skull Base Reconstruction. Journal of neurological surgery. Part B, Skull base. 2022 Apr:83(2):133-136. doi: 10.1055/s-0040-1721816. Epub 2021 Feb 18 [PubMed PMID: 35433180]
Waters CM, Zanation AM, Thorp BD, Shockley WW, Clark JM. Repair of Septal Perforation with Endoscopic-Assisted Pericranial Flap Harvest and Open Rhinoplasty Approach. Facial plastic surgery & aesthetic medicine. 2020 May/Jun:22(3):225-226. doi: 10.1089/fpsam.2020.0008. Epub 2020 Mar 26 [PubMed PMID: 32212970]
Shumrick KA, Smith TL. The anatomic basis for the design of forehead flaps in nasal reconstruction. Archives of otolaryngology--head & neck surgery. 1992 Apr:118(4):373-9 [PubMed PMID: 1554465]
Prasanna NS. Nasal reconstruction with pre-laminated forehead flap. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2017 Sep-Dec:50(3):306-309. doi: 10.4103/ijps.IJPS_165_17. Epub [PubMed PMID: 29618867]
Ziegler JP, Oyer SL. Prelaminated paramedian forehead flap for subtotal nasal reconstruction using three-dimensional printing. BMJ case reports. 2021 Jan 26:14(1):. doi: 10.1136/bcr-2020-238146. Epub 2021 Jan 26 [PubMed PMID: 33500305]
Level 3 (low-level) evidenceJose A, Nagori SA, Arya S, Roy ID. Chimeric temporopareital osteofascial and temporalis muscle flap; a novel method for the reconstruction of composite orbito-maxillary defects. Journal of stomatology, oral and maxillofacial surgery. 2019 Jun:120(3):250-254. doi: 10.1016/j.jormas.2019.02.002. Epub 2019 Feb 11 [PubMed PMID: 30763779]
Denadai R, Raposo-Amaral CE, Marques FF, Raposo-Amaral CA. Posttraumatic eyebrow reconstruction with hair-bearing temporoparietal fascia flap. Einstein (Sao Paulo, Brazil). 2015 Jan-Mar:13(1):106-9. doi: 10.1590/S1679-45082015RC2834. Epub 2015 Mar 3 [PubMed PMID: 25993077]
Marano SR, Fischer DW, Gaines C, Sonntag VK. Anatomical study of the superficial temporal artery. Neurosurgery. 1985 Jun:16(6):786-90 [PubMed PMID: 4010900]
Edizer M, Beden U, Icten N. Morphological parameters of the periorbital arterial arcades and potential clinical significance based on anatomical identification. The Journal of craniofacial surgery. 2009 Jan:20(1):209-14. doi: 10.1097/SCS.0b013e318191cf9f. Epub [PubMed PMID: 19165029]
Jawad BA, Hohman MH, Raggio BS. Temporoparietal Fascia Flaps. StatPearls. 2026 Jan:(): [PubMed PMID: 32310365]
Schreiber M, Dragu A. Free temporal fascia flap to cover soft tissue defects of the foot: a case report. GMS Interdisciplinary plastic and reconstructive surgery DGPW. 2015:4():Doc01. doi: 10.3205/iprs000060. Epub 2015 Jan 13 [PubMed PMID: 26504730]
Level 3 (low-level) evidenceDaskalopoulou D, Matsas A, Chrysikos D, Troupis T. The Superficial Temporal Artery: Anatomy and Clinical Significance in the Era of Facial Surgery and Aesthetic Medicine. Acta medica academica. 2022 Dec:51(3):232-242. doi: 10.5644/ama2006-124.393. Epub 2022 Dec 20 [PubMed PMID: 36799316]
Reinisch JF, Lewin S. Ear reconstruction using a porous polyethylene framework and temporoparietal fascia flap. Facial plastic surgery : FPS. 2009 Aug:25(3):181-9. doi: 10.1055/s-0029-1239448. Epub 2009 Oct 6 [PubMed PMID: 19809950]
Bigcas JLM, Bond J. Osteocutaneous Radial Forearm Flap(Archived). StatPearls. 2026 Jan:(): [PubMed PMID: 33232054]
Wahood W, Ghozy S, Al-Abdulghani A, Kallmes DF. Radial artery diameter: a comprehensive systematic review of anatomy. Journal of neurointerventional surgery. 2022 Dec:14(12):1274-1278. doi: 10.1136/neurintsurg-2021-018534. Epub 2022 Feb 15 [PubMed PMID: 35169033]
Level 1 (high-level) evidenceWaterhouse N, Moss AL, Townsend PL. Lower limb salvage using an extended free radial forearm flap. British journal of plastic surgery. 1984 Jul:37(3):394-7 [PubMed PMID: 6743906]
Jones NF, Hardesty RA, Goldstein SA, Ward WT. Upper limb salvage using a free radial forearm flap. Plastic and reconstructive surgery. 1987 Mar:79(3):468-71 [PubMed PMID: 3823222]
Hentz VR, Pearl RM, Grossman JA, Wood MB, Cooney WP. The radial forearm flap: a versatile source of composite tissue. Annals of plastic surgery. 1987 Dec:19(6):485-98 [PubMed PMID: 3439761]
Level 3 (low-level) evidenceJeng SF, Kuo YR, Wei FC, Su CY, Chien CY. Total lower lip reconstruction with a composite radial forearm-palmaris longus tendon flap: a clinical series. Plastic and reconstructive surgery. 2004 Jan:113(1):19-23 [PubMed PMID: 14707618]
Ueda K, Oba S, Okada M, Hara M, Zen N. Eyelid reconstruction with a composite radial forearm palmaris longus tendon flap. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2007:60(3):256-9 [PubMed PMID: 17293282]
Militsakh ON, Werle A, Mohyuddin N, Toby EB, Kriet JD, Wallace DI, Girod DA, Tsue TT. Comparison of radial forearm with fibula and scapula osteocutaneous free flaps for oromandibular reconstruction. Archives of otolaryngology--head & neck surgery. 2005 Jul:131(7):571-5 [PubMed PMID: 16027278]
Level 2 (mid-level) evidenceBoahene K, Richmon J, Byrne P, Ishii L. Hinged forearm split-thickness skin graft for radial artery fasciocutaneous flap donor site repair. Archives of facial plastic surgery. 2011 Nov-Dec:13(6):392-4. doi: 10.1001/archfacial.2011.65. Epub [PubMed PMID: 22106183]
Bhama PK, Weinberg JS, Lindsay RW, Hohman MH, Cheney ML, Hadlock TA. Objective outcomes analysis following microvascular gracilis transfer for facial reanimation: a review of 10 years' experience. JAMA facial plastic surgery. 2014 Mar-Apr:16(2):85-92. doi: 10.1001/jamafacial.2013.2463. Epub [PubMed PMID: 24481538]
Level 2 (mid-level) evidenceHarii K, Ohmori K, Torii S. Free gracilis muscle transplantation, with microneurovascular anastomoses for the treatment of facial paralysis. A preliminary report. Plastic and reconstructive surgery. 1976 Feb:57(2):133-43 [PubMed PMID: 1250883]
Level 3 (low-level) evidenceKay S, Pinder R, Wiper J, Hart A, Jones F, Yates A. Microvascular free functioning gracilis transfer with nerve transfer to establish elbow flexion. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2010 Jul:63(7):1142-9. doi: 10.1016/j.bjps.2009.05.021. Epub 2009 Jun 13 [PubMed PMID: 19525160]
Novakovic D, Patel RS, Goldstein DP, Gullane PJ. Salvage of failed free flaps used in head and neck reconstruction. Head & neck oncology. 2009 Aug 21:1():33. doi: 10.1186/1758-3284-1-33. Epub 2009 Aug 21 [PubMed PMID: 19698095]
Miyasaka M, Ichikawa K, Nishimura M, Yamazaki A, Taira H, Imagawa K, Tanino R. Salvage operations of free tissue transfer following internal jugular venous thrombosis: a review of 4 cases. Microsurgery. 2005:25(3):191-5 [PubMed PMID: 15744722]
Level 3 (low-level) evidenceJunren C, Xiaofang X, Huiqiong Z, Gangmin L, Yanpeng Y, Xiaoyu C, Yuqing G, Yanan L, Yue Z, Fu P, Cheng P. Pharmacological Activities and Mechanisms of Hirudin and Its Derivatives - A Review. Frontiers in pharmacology. 2021:12():660757. doi: 10.3389/fphar.2021.660757. Epub 2021 Apr 16 [PubMed PMID: 33935784]
Level 2 (mid-level) evidenceLineaweaver WC, Hill MK, Buncke GM, Follansbee S, Buncke HJ, Wong RK, Manders EK, Grotting JC, Anthony J, Mathes SJ. Aeromonas hydrophila infections following use of medicinal leeches in replantation and flap surgery. Annals of plastic surgery. 1992 Sep:29(3):238-44 [PubMed PMID: 1524373]
Level 3 (low-level) evidencePérez M, Sancho J, Ferrer C, García O, Barret JP. Management of flap venous congestion: the role of heparin local subcutaneous injection. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2014 Jan:67(1):48-55. doi: 10.1016/j.bjps.2013.09.003. Epub 2013 Sep 12 [PubMed PMID: 24094618]
Brouwers K, Kruit AS, Hummelink S, Ulrich DJO. Management of free flap salvage using thrombolytic drugs: A systematic review. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2020 Oct:73(10):1806-1814. doi: 10.1016/j.bjps.2020.05.057. Epub 2020 May 25 [PubMed PMID: 32591263]
Level 1 (high-level) evidenceWolff KD, Stiller D. Ischemia tolerance of free-muscle flaps: an NMR-spectroscopic study in the rat. Plastic and reconstructive surgery. 1993 Mar:91(3):485-91 [PubMed PMID: 8438020]
Level 3 (low-level) evidenceGampper TJ, Zhang F, Mofakhami NF, Morgan RF, Amiss R, Hoard MA, Angel MF. Beneficial effect of hyperbaric oxygen on island flaps subjected to secondary venous ischemia. Microsurgery. 2002:22(2):49-52 [PubMed PMID: 11921070]