Introduction
The dental pulp is a specialized, nonmineralized, highly vascularized connective tissue occupying the central compartment of the tooth, distinct from surrounding mineralized tissues, including enamel, dentin, and cementum.[1] The pulp contains connective tissue, blood vessels, and nerves. This structure communicates with the periodontium through the apical and, in some teeth, accessory foramina. Completely enclosed by dentin, the pulp provides nutritive support, participates in dentinogenesis, and mediates immunologic defense, underscoring its essential role in maintaining tooth vitality and function.
Detailed knowledge of pulp anatomy and physiology is critical for accurate diagnosis and treatment planning. Familiarity with this structure's vascular and neural architecture guides clinicians during pulpotomy, root canal treatment (RCT), and apical surgery, minimizing iatrogenic injury and preserving pulp vitality whenever possible. This insight also informs pain control, hemostasis, and prognosis assessment, ultimately improving tooth survival and patient outcomes.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Structure
The pulp mass is a highly vascularized, richly innervated connective tissue occupying the pulp chamber. This tissue contains diverse cell populations, including fibroblasts, odontoblasts, histiocytes, macrophages, mast cells, and plasma cells. The extracellular matrix consists of collagen fibers and ground substance. The pulp deposits dentin concentrically. Thus, the resulting shape mirrors the external contour of the enamel.[2][3]
Pulpal architecture consists of 2 principal regions: peripheral and central. The peripheral zone contains several structural layers adjacent to the calcified dentin. At the dentin-pulp interface lies a layer of columnar odontoblasts responsible for dentin formation. Numerous dentinal tubules, created by odontoblast activity, traverse the dentin from the pulp toward the enamel border.[4] Each tubule contains an odontoblast process, a cellular extension involved in dentinogenesis, as well as dentinal fluid. Since dentin is avascular, these tubules provide a pathway for nutrients carried in interstitial fluid derived from pulpal capillaries.
Beneath the odontoblastic layer lies the cell-free zone, or zone of Weil, a layer rich in capillaries and nerve plexuses. Deeper still is the cell-rich zone, located closest to the central pulp. This layer contains abundant fibroblasts and undifferentiated mesenchymal cells that support the odontoblast population through proliferation and differentiation. These cells can also give rise to fibroblasts and macrophages (see Image. Dental Pulp Histology).[5]
The inner margin of the cell-rich layer demarcates the central pulp zone. This region provides structural and metabolic support to the peripheral pulp and contains large blood vessels and nerve trunks that branch toward the periphery. Numerous fibroblasts are also present within this zone.
Pulp classification depends on its location, either within the crown (coronal pulp) or the root, which extends from the cervical region to the apex (radicular pulp). The coronal pulp contains pulp horns, which are projections housing abundant nerve fibers. These projections correspond to the incisal edges of anterior teeth and the major cusps of posterior teeth. Pulp horns are typically more prominent in younger than older individuals.[6] Despite the limitations of 2-dimensional imaging, periapical radiographs can reveal critical morphological relationships, including the proximity of pulp horns to the external tooth surface. Such information guides the placement and interpretation of pulp sensibility tests, including thermal and electric methods, because teeth with calcified or reduced pulp chambers often display delayed responses compared with teeth with normal pulp dimensions.
Function
The dental pulp performs 4 primary functions: dentin formation, dentin nutrition, tooth innervation, and tooth defense. Dentinogenesis is the most critical function, carried out by odontoblasts located at the dentin-pulp interface. The pulp also provides nutritive support by supplying dentin with moisture and macromolecules, including albumin, transferrin, and proteoglycans like tenascin.
Pulpal defense is mediated through the deposition of tertiary dentin, which forms a protective barrier against irritants and slows the progression of carious lesions. This process is initiated by the stimulation of existing odontoblasts or the differentiation of new odontoblasts from progenitor cells. The quality and amount of dentin formed are determined by the type of insult (eg, infectious, thermal, chemical), the depth and severity of tissue involvement, and the extent of the affected surface area. Additional dentin formation requires recruitment of undifferentiated mesenchymal cells from the cell-rich zone to replace depleted odontoblasts.[7]
Embryology
Understanding dental pulp development requires consideration of overall tooth formation. Initiation and progression of tooth and pulpal morphogenesis depend on bidirectional cell signaling between the oral epithelium and surrounding mesenchyme. Two primary cell populations contribute to tooth formation: oral epithelial cells, which give rise to the enamel organ, and mesenchymal cells, which differentiate into the dental papilla.
Pulp formation proceeds through 3 morphologic stages: bud, cap, and bell. During the bud stage, epithelial cells of the dental lamina, an epithelial band projecting from the oral epithelium, undergo proliferation and produce a bud-like projection into the adjacent ectomesenchyme. This epithelial bud enlarges and acquires a concave surface, marking the onset of the cap stage. At this point, the enamel organ and dental papilla are fully established. The bell stage follows, characterized by morphodifferentiation and histodifferentiation of the pulp. Peripheral cells differentiate into odontoblasts, acquire a columnar morphology, and secrete predentin, a collagenous matrix that subsequently mineralizes into dentin.[8]
The dental papilla, the precursor of the dental pulp, contains a dense population of cells even during the early bud stage, composed primarily of fibroblasts. Blood vessels and associated nerve fibers are established early within the papilla, providing nutrition to the developing organ. Initially located in the central zone, these vessels give rise to smaller capillaries that extend toward the periphery and supply nutrients to elongating odontoblasts. Dentin deposition by odontoblasts in the central region signifies the transition of the dental papilla into the dental pulp.[9]
Blood Supply and Lymphatics
The blood supply of the dental pulp is derived from arterioles that enter through the apical foramen and traverse the radicular pulp. Each pulp chamber typically contains 1 to 2 arterioles and a single large venule, which branch into an extensive capillary network within the coronal pulp. This network occupies the region beneath the odontoblastic layer and, in some areas, penetrates the layer. Although pulpal tissue pressure exceeds that of most other tissues, capillary blood flow remains comparatively high, producing bulk fluid movement across the capillary walls into the interstitial space. Lymphatic drainage removes this fluid at a rate sufficient to maintain constant tissue volume. Elevated tissue pressure also promotes outward fluid movement through the dentinal tubules, a mechanism that helps clear toxins and bacteria from the dentin-pulp interface.[10]
Nerves
Two principal nerve types innervate the dental pulp: autonomic and afferent sensory fibers. Sympathetic autonomic fibers arise from the superior cervical ganglion, located superior to the carotid artery. Axonal projections of these unmyelinated neurons innervate arteriolar smooth muscle within the pulp, regulating vascular tone and pulpal blood flow. Afferent sensory fibers originate from the maxillary and mandibular branches of the trigeminal nerve. Unlike the autonomic fibers, these sensory neurons are predominantly myelinated except at their free terminals and mediate thermal and mechanical nociception. The myelinated segments branch extensively beneath the cell-rich zone to form the plexus of Raschkow, while the unmyelinated terminals traverse the cell-free zone and terminate near odontoblasts, with some projecting into the dentinal tubules.[11][12]
Physiologic Variants
Pulp physiology undergoes significant changes with aging, resulting in distinct phenotypic alterations. Progressive deposition of secondary dentin at the apical root gradually constricts the apical foramen, compromising circulation and innervation. Blood vessels, lymphatic vessels, and nerves entering aged pulp exhibit arteriosclerotic changes, degenerative alterations, and progressive mineralization of the nerve sheath, respectively. Loss of neural elements contributes to the frequent absence of pain in aged teeth.
Odontoblasts that remain in aged pulp are reduced in size and display a flattened morphology. Cellular density decreases markedly, falling by approximately 50% between ages 20 and 70. Aged pulp also demonstrates increased fibrosis and accumulation of collagen fibers. This apparent rise in collagen content does not reflect increased synthesis; rather, it represents residual connective tissue sheaths left behind following the degeneration of nerves and blood vessels, which subsequently integrate into the fibrous matrix.[13][14]
Surgical Considerations
Recent studies demonstrate the potential for dental pulp regeneration using transplantation of dental pulp stem cells in human models of pulpitis. These findings suggest a pathway toward biologically based endodontic therapies that could replace or complement conventional RCT.
Clinical Significance
In exchange for producing dentin and supplying it with nutrients, the surrounding dentin encases the pulp in a barrier that protects against the microbially rich oral environment. Despite this protection, the pulp remains vulnerable to injury, and inflammation resulting from such injury is termed "pulpitis."
Pulpitis occurs in 2 forms: reversible and irreversible. Reversible pulpitis involves mild-to-moderate inflammation that resolves once the underlying cause is eliminated. Common etiologies include bacterial invasion from dental caries, acute trauma, repetitive occlusal trauma such as bruxism, thermal injury, excessive cavity desiccation during restorative procedures, and irritation of exposed dentin. In contrast, irreversible pulpitis results exclusively from bacterial invasion severe enough to render pulpal healing impossible.[15]
Several diagnostic methods help differentiate reversible from irreversible pulpitis. Sensibility testing evaluates pulpal innervation by measuring the sensory response of the tooth to external stimuli. A common example is the cold test, in which a chilled stimulus, often a cotton pellet cooled with dry ice, is applied to the tooth. A healthy pulp produces a brief, mild pain response that resolves within 1 to 2 seconds after the stimulus is removed.[16] In contrast, an irreversibly inflamed pulp produces a sharp, exaggerated pain that lingers for more than 30 seconds after stimulus removal. Additional sensibility evaluations include percussion, which involves tapping on the crown; bite assessments using hard objects; and electric pulp testing, which determines whether pulpal neurons can generate an action potential.[17]
Other Issues
Recent evidence supports the use of vital pulp therapy (VPT), including partial and full pulpotomy, for teeth with fully developed roots.[18][19] These procedures aim to preserve healthy pulp tissue by selectively removing the inflamed portion, thereby maintaining the tooth’s natural defense mechanisms and avoiding many of the technical challenges associated with conventional RCT.[20]
Successful outcomes require careful case selection, accurate diagnosis, and meticulous execution, including proper hemostasis, placement of bioactive capping materials such as hydraulic calcium silicate cements, and immediate coronal restoration to prevent microleakage. In mature teeth, pulpotomy represents a predictable and minimally invasive alternative to RCT, offering success rates comparable to traditional endodontic therapy while maintaining pulp vitality, immune function, and dentinogenesis.
Media
(Click Image to Enlarge)
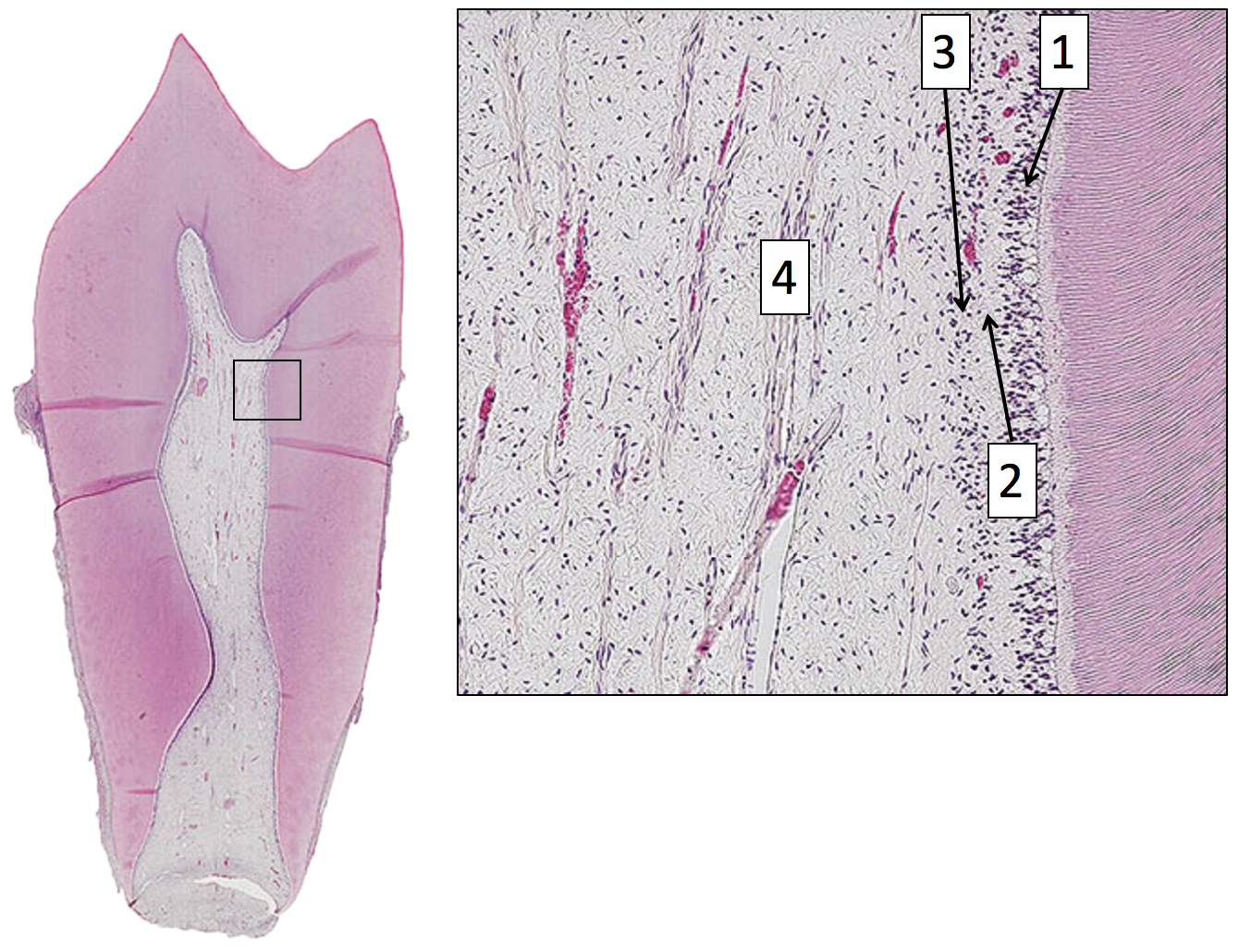
Dental Pulp Histology. This image is a histological slide of a tooth's dental pulp. A close-up view identifies several key structures. The odontoblast layer (1) is visible at the periphery, followed by the cell-free zone of Weil (2). The cell-rich zone (3) and the central pulp core (4) are also clearly shown.
Image in the Public Domain Wikimedia Commons https://commons.wikimedia.org/w/index.php?curid=87411232
References
Ahmed HMA. A critical analysis of laboratory and clinical research methods to study root and canal anatomy. International endodontic journal. 2022 Apr:55 Suppl 2():229-280. doi: 10.1111/iej.13702. Epub 2022 Mar 31 [PubMed PMID: 35124829]
Yu C, Abbott PV. An overview of the dental pulp: its functions and responses to injury. Australian dental journal. 2007 Mar:52(1 Suppl):S4-16 [PubMed PMID: 17546858]
Level 3 (low-level) evidenceGREEN D. Morphology of the pulp cavity of the permanent teeth. Oral surgery, oral medicine, and oral pathology. 1955 Jul:8(7):743-59 [PubMed PMID: 14394660]
Yoshida S, Ohshima H. Distribution and organization of peripheral capillaries in dental pulp and their relationship to odontoblasts. The Anatomical record. 1996 Jun:245(2):313-26 [PubMed PMID: 8769670]
Level 3 (low-level) evidenceShi S, Gronthos S. Perivascular niche of postnatal mesenchymal stem cells in human bone marrow and dental pulp. Journal of bone and mineral research : the official journal of the American Society for Bone and Mineral Research. 2003 Apr:18(4):696-704 [PubMed PMID: 12674330]
Ahmed HMA, Wolf TG, Rossi-Fedele G, Dummer PMH. The Study and Relevance of Pulp Chamber Anatomy in Endodontics - A Comprehensive Review. European endodontic journal. 2024 Jan 1:9(1):18-34. doi: 10.14744/eej.2023.76598. Epub 2023 Nov 22 [PubMed PMID: 37990569]
Slavkin HC. The nature and nurture of epithelial-mesenchymal interactions during tooth morphogenesis. Journal de biologie buccale. 1978 Sep:6(3):189-204 [PubMed PMID: 282288]
Level 3 (low-level) evidenceMacNeil RL, Thomas HF. Development of the murine periodontium. I. Role of basement membrane in formation of a mineralized tissue on the developing root dentin surface. Journal of periodontology. 1993 Feb:64(2):95-102 [PubMed PMID: 8433258]
Level 3 (low-level) evidenceFanali S, Rametta D, Di Vincenzo F. [The embryological development of the nerve fibers of the tooth. An analysis of their formation and development correlated with the different evolutionary stages of the dental structures]. Minerva stomatologica. 1991 May:40(5):309-18 [PubMed PMID: 1944042]
Tønder KJ. Blood flow and vascular pressure in the dental pulp. Summary. Acta odontologica Scandinavica. 1980:38(3):135-44 [PubMed PMID: 6998253]
Level 3 (low-level) evidenceByers MR, Närhi MV, Mecifi KB. Acute and chronic reactions of dental sensory nerve fibers to cavities and desiccation in rat molars. The Anatomical record. 1988 Aug:221(4):872-83 [PubMed PMID: 3189878]
Level 3 (low-level) evidenceDahl E, Mjör IA. The structure and distribution of nerves in the pulp-dentin organ. Acta odontologica Scandinavica. 1973 Dec:31(6):349-56 [PubMed PMID: 4520984]
Carvalho TS, Lussi A. Age-related morphological, histological and functional changes in teeth. Journal of oral rehabilitation. 2017 Apr:44(4):291-298. doi: 10.1111/joor.12474. Epub 2017 Jan 28 [PubMed PMID: 28032898]
Morse DR. Age-related changes of the dental pulp complex and their relationship to systemic aging. Oral surgery, oral medicine, and oral pathology. 1991 Dec:72(6):721-45 [PubMed PMID: 1812456]
Peng C, Zhao Y, Wang W, Yang Y, Qin M, Ge L. Histologic Findings of a Human Immature Revascularized/Regenerated Tooth with Symptomatic Irreversible Pulpitis. Journal of endodontics. 2017 Jun:43(6):905-909. doi: 10.1016/j.joen.2017.01.031. Epub 2017 Apr 14 [PubMed PMID: 28416306]
Level 2 (mid-level) evidenceMainkar A, Kim SG. Diagnostic Accuracy of 5 Dental Pulp Tests: A Systematic Review and Meta-analysis. Journal of endodontics. 2018 May:44(5):694-702. doi: 10.1016/j.joen.2018.01.021. Epub 2018 Mar 20 [PubMed PMID: 29571914]
Level 1 (high-level) evidenceNissan R, Trope M, Zhang CD, Chance B. Dual wavelength spectrophotometry as a diagnostic test of the pulp chamber contents. Oral surgery, oral medicine, and oral pathology. 1992 Oct:74(4):508-14 [PubMed PMID: 1408029]
Level 3 (low-level) evidenceAhmed HMA, El-Karim I, Duncan HF, Krastl G, Galler K. Implications of root, pulp chamber, and canal anatomy on pulpotomy and revitalization procedures. Clinical oral investigations. 2023 Nov:27(11):6357-6369. doi: 10.1007/s00784-023-05284-9. Epub 2023 Oct 23 [PubMed PMID: 37870593]
Careddu R, Duncan HF. A prospective clinical study investigating the effectiveness of partial pulpotomy after relating preoperative symptoms to a new and established classification of pulpitis. International endodontic journal. 2021 Dec:54(12):2156-2172. doi: 10.1111/iej.13629. Epub 2021 Sep 26 [PubMed PMID: 34490637]
Duncan HF. Present status and future directions-Vital pulp treatment and pulp preservation strategies. International endodontic journal. 2022 May:55 Suppl 3(Suppl 3):497-511. doi: 10.1111/iej.13688. Epub 2022 Feb 3 [PubMed PMID: 35080024]
Level 3 (low-level) evidence