 Anatomy, Bony Pelvis and Lower Limb: Leg Anterior Compartment
Anatomy, Bony Pelvis and Lower Limb: Leg Anterior Compartment
Introduction
The lower leg is subdivided into 4 compartments: anterior, lateral, superficial posterior, and deep posterior (see Image. Transverse Section of the Leg).[1] The anterior compartment houses the tibialis anterior, extensor hallucis longus (EHL), extensor digitorum longus (EDL), and fibularis (peroneus) tertius muscles, innervated by the deep fibular (peroneal) nerve and supplied by the anterior tibial artery.[2] Muscles of the anterior compartment function as the primary extensors of the ankle (dorsiflexion) and toes.
The anterior compartment is the most common site of acute compartment syndrome, which constitutes a medical emergency requiring fasciotomy.[3] Other pathologies that may involve this region include neuromuscular conditions that lead to foot drop, atherosclerotic plaque buildup in the arteries, and deep vein thrombosis (DVT). Understanding both the anatomy and function of the anterior leg compartment enables clinicians to diagnose pathology, guide surgical planning, and prevent neurovascular complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The muscles of the anterior leg compartment include the tibialis anterior, EHL, EDL, and fibularis tertius. The origins and insertion points of these muscles are summarized below.
The tibialis anterior takes origin from the lateral condyle and proximal lateral surface of the tibia, as well as the interosseous membrane (IOM) between the tibia and fibula. The muscle is a thick, fusiform structure that forms the most medial component of the anterior compartment, with a prominent tendon visible on the anterior aspect of the ankle. The tendon inserts on the medial cuneiform and the base of the 1st metatarsal.
The EHL originates from the middle anterior surface of the fibula and the IOM. The muscle is a slender, deep structure positioned between the tibialis anterior and EDL. The tendon inserts on the dorsal aspect of the distal phalanx of the hallux.
The EDL originates from the lateral condyle of the tibia, the anterior surface of the fibula, and the IOM. The muscle is a broad, pennate structure forming the central superficial component of the anterior compartment and divides distally into 4 tendons. These tendons insert into the dorsal expansions of digits 2 through 5, extending to the middle and distal phalanges.
The fibularis tertius originates from the distal anterior fibula and the IOM, often as a distal extension of the EDL. The muscle is small and may be absent in some individuals. The tendon inserts on the dorsal base of the 5th metatarsal.
The anterior compartment of the leg primarily produces dorsiflexion at the ankle and extension of the toes. The tibialis anterior is the strongest dorsiflexor and contributes to inversion of the foot. The EHL extends the hallux and assists in ankle dorsiflexion. The EDL extends digits 2 through 5 and assists in dorsiflexion. The fibularis tertius weakly assists in dorsiflexion and contributes to eversion of the foot. Collectively, these muscles coordinate foot clearance during the swing phase of gait and stabilize foot positioning during heel strike and stance.
Embryology
The limb buds of the embryo begin to form approximately 4 to 5 weeks after fertilization. The lateral plate mesoderm migrates into the limb bud region. Condensation along the central axis gives rise to the vasculature and skeletal components of the lower limb.[4]
Several factors regulate limb bud development, including retinoic acid, sonic hedgehog (Shh), HOX genes, the apical ectodermal ridge (AER), and the zone of polarizing activity (ZPA). Retinoic acid functions as a global organizing gradient that initiates transcription factor expression responsible for regional differentiation and limb polarization.
The AER secretes fibroblast growth factors (FGFs) that promote limb bud outgrowth by stimulating mitosis in the underlying mesenchyme.[5] Hindlimb development specifically involves FGF10, which is regulated by T-box transcription factor 4 (Tbx4). The ZPA produces Shh, which organizes the limb bud along the anterior-posterior axis. Shh signaling activates HOX genes, including HOXD9, HOXD10, HOXD11, HOXD12, and HOXD13, which are essential for limb polarization and regional specification.[6] These genes regulate patterning and determine limb morphology during embryonic development. Errors in HOX gene expression may result in limb malformations.[7]
Blood Supply and Lymphatics
The anterior compartment of the lower limb receives its blood supply from the anterior tibial artery, a branch of the popliteal artery. The arterial supply of the lower limb originates from the popliteal artery, which divides into the anterior and posterior tibial arteries (see Image. Arteries of the Lower Limb, Anterior and Posterior Views).
The posterior tibial artery descends along the posterior aspect of the leg, supplying the posterior compartment muscles and giving rise to the fibular artery. The anterior tibial artery courses anteriorly between the tibia and fibula, traversing the IOM to supply the anterior compartment muscles.
The anterior tibial artery continues inferiorly into the foot, where it becomes the dorsalis pedis artery. The dorsalis pedis artery supplies the tarsal bones and the dorsal aspect of the metatarsals. Distally, the dorsalis pedis artery anastomoses with the lateral plantar artery to form the deep plantar arch.
Venous drainage of the anterior compartment accompanies the anterior tibial artery via the anterior tibial veins, which drain into the popliteal vein.[8] Lymphatic drainage follows the deep lymphatic system of the lower limb, converging primarily toward the popliteal lymph nodes before continuing to the deep inguinal nodes.
Nerves
The deep fibular nerve provides innervation to the anterior compartment of the leg (see Image. Deep Fibular Nerve and Related Structures). This nerve is a branch of the common fibular nerve, itself a branch of the sciatic nerve. The sciatic nerve bifurcates at the apex of the popliteal fossa into the tibial and common fibular nerves.
The tibial nerve descends along the posterior aspect of the leg, posterior to the tibia, and supplies the deep muscles of the posterior compartment. The terminal division of the tibial nerve forms the medial and lateral plantar nerves of the foot.
The common fibular nerve courses around the neck of the fibula, where it divides into the superficial and deep fibular nerves. The superficial fibular nerve supplies the lateral compartment of the leg and provides sensory innervation to the dorsum of the foot. The deep fibular nerve supplies motor innervation to the anterior compartment of the leg and sensory innervation to the 1st dorsal webspace.
Physiologic Variants
Variants involving the anterior leg compartment may affect muscles, vessels, and nerves. These findings reflect both congenital and acquired anatomic variability described in recent anatomical literature.
Muscular variants most commonly involve the fibularis tertius, which may be absent or poorly developed in some individuals. Accessory extensor slips and variant connections between EDL and adjacent tendons have also been reported. Such variations may alter tendon routing at the ankle and influence surgical exposure or reconstructive planning.[9][10]
Vascular variation most frequently involves the anterior tibial artery, including hypoplasia, segmental absence, or compensatory enlargement of the fibular artery.[11][12] High-origin or variant branching patterns at the popliteal bifurcation have been documented and may modify perfusion to the anterior compartment and dorsum of the foot. These variants are clinically relevant in bypass grafting and endovascular procedures. [Source: Lamprecht, et al Popliteal artery anatomy: An angiographic description of variants. 2021]
Variations in innervation most commonly involve the deep fibular nerve and include differences in its course, branching pattern, and level of emergence within the anterior compartment.[13] Such variation may influence susceptibility to entrapment neuropathy and modify the clinical presentation of foot drop or sensory deficits in the 1st dorsal webspace.
Surgical Considerations
The anterior compartment of the lower leg is the most common site of acute compartment syndrome. Increased pressure within the anterior compartment can compromise tissue perfusion, resulting in irreversible muscle and nerve damage, including muscle necrosis. Common causes of anterior compartment syndrome include trauma, such as fractures, crush injuries, contusions, and gunshot wounds; tight casts or dressings; extravasation of intravenous infusions; burns; postischemic swelling; bleeding disorders; and arterial injury.[14] Fractures are the most frequent cause of anterior compartment syndrome, accounting for over 65% of cases.[15]
Recognition of compartment syndrome is essential for treatment and prevention of ischemia and necrosis involving neurovascular structures and muscle. Physical examination findings are often described as the “5 P’s”: pain with passive stretch of the toes or ankle, paresthesias, paralysis, palpable swelling, and pulselessness. Pain with passive stretch is widely regarded as the most sensitive clinical finding, whereas paralysis and pulselessness are late manifestations and are often irreversible.
Although compartment syndrome is primarily a clinical diagnosis, definitive confirmation may be obtained by measuring compartment pressures. A diagnosis of compartment syndrome is confirmed when the resting compartment pressure exceeds 30 mm Hg or when the perfusion pressure gradient (ΔP) is less than 30 mm Hg, where ΔP is calculated as diastolic blood pressure minus compartment pressure. Time remains critical in acute compartment syndrome. Treatment within 6 hours of ischemia is associated with complete recovery, whereas ischemia beyond 6 hours typically results in necrosis.[16]
The definitive management of acute anterior compartment syndrome involves fasciotomy. Treatment of chronic anterior compartment syndrome may be conservative and includes activity modification, nonsteroidal anti-inflammatory drug administration, stretching, orthotics, and physical therapy. Tendon transfer procedures may be considered in patients with persistent foot drop following missed or inadequately treated compartment syndrome.
Another surgical intervention involving the anterior compartment of the leg includes bypass surgery for peripheral arterial disease. The arteries of the lower extremities are particularly prone to atherosclerotic plaque formation and peripheral arterial disease, in which progressive luminal narrowing reduces arterial perfusion of the lower limbs.[17][18] Initial management of peripheral arterial disease includes lifestyle modification and pharmacologic therapy. However, failure of conservative treatment may necessitate surgical intervention.[19][20] Common procedures for peripheral arterial disease include angioplasty, thrombus removal, and bypass surgery.[21][22]
Clinical Significance
The anterior compartment of the leg is essential for dorsiflexion of the foot and extension of the toes, with additional contributions to inversion and eversion of the foot. The region is routinely assessed during physical examination to evaluate the range of motion and motor strength of the ankle and toes. Reduced or absent motor strength may indicate muscle or nerve injury involving the anterior compartment of the leg.
As mentioned, the anterior leg compartment is the most common site of compartment syndrome. This condition may occur acutely, following blunt force injury or trauma, or chronically, developing from repeated exertion often seen in athletes. Compartment syndrome constitutes a medical emergency requiring fasciotomy of the involved compartment.[23] Foot drop may arise as a complication of anterior compartment syndrome due to ischemic injury of the deep fibular nerve and associated extensor musculature.
The anterior compartment of the leg may also be involved in DVT, a frequent complication following major orthopedic surgery. Most cases of DVT in the lower limb involve the muscular, posterior tibial, and fibular veins, while involvement of the anterior tibial vein is least common. Thrombosis of the anterior tibial vein is an extremely rare form of lower extremity thrombosis, with isolated anterior tibial vein thrombosis being even rarer, with a reported incidence of 0% to 0.3%. Interventions for DVT include anticoagulation, thrombolysis, vena cava filter placement, and compression stocking use.[24]
Other Issues
Stasis dermatitis most commonly arises from chronic venous insufficiency, in which venous valve incompetence, venous obstruction, or calf muscle pump dysfunction produces sustained venous hypertension and impaired venous return. Venous hypertension promotes capillary leakage, erythrocyte extravasation, inflammation, and hemosiderin deposition, resulting in brown skin discoloration. Risk factors include older age, obesity, pregnancy, prolonged standing, prior DVT, varicose veins, and reduced mobility. The pretibial (anterior shin) region is particularly vulnerable because of dependent venous pressure, limited soft tissue coverage, and frequent microtrauma.[25] Although not immediately dangerous, pretibial hyperpigmentation may indicate progressive chronic venous insufficiency and risk of ulceration.[26][27] Management includes compression therapy, leg elevation, exercise, weight reduction, and treatment of underlying venous reflux.
Media
(Click Image to Enlarge)
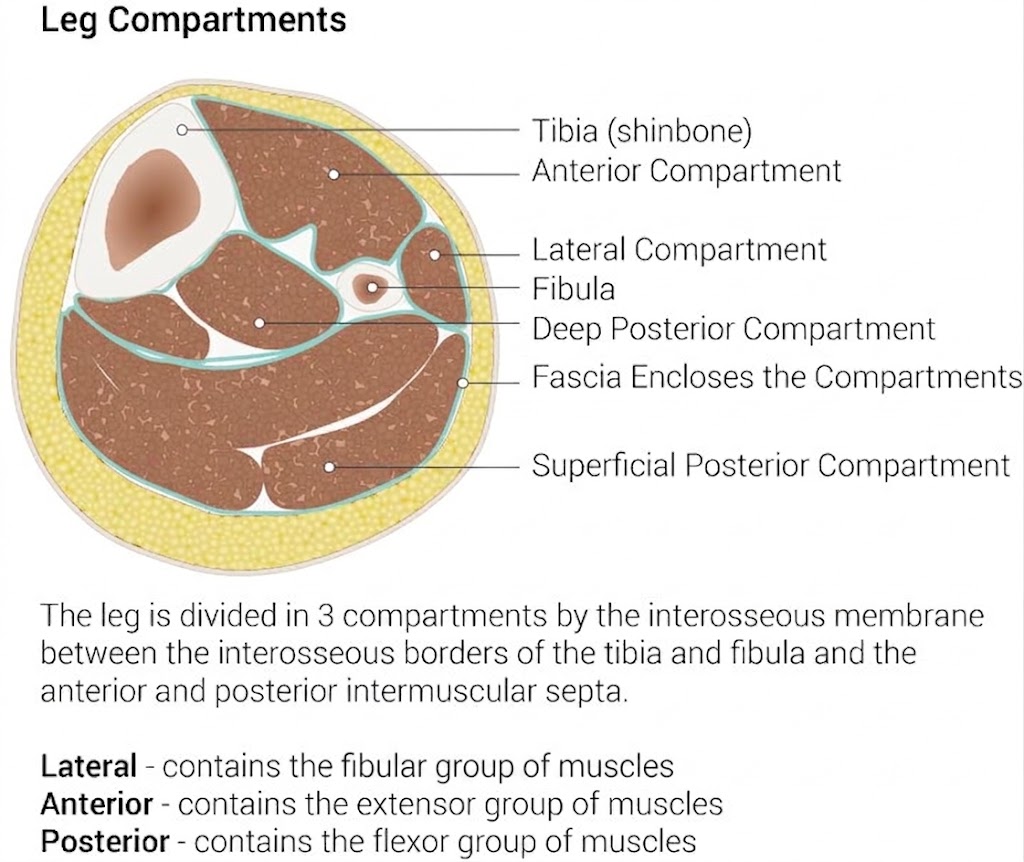
Transverse Section of the Leg. The illustration depicts the fascial boundaries that separate the leg into anterior, lateral, and posterior functional groups. Each compartment is defined by its relationship to the tibia and fibula, housing specific neurovascular bundles and synergistic muscle sets.
Illustrated by B Palmer
(Click Image to Enlarge)
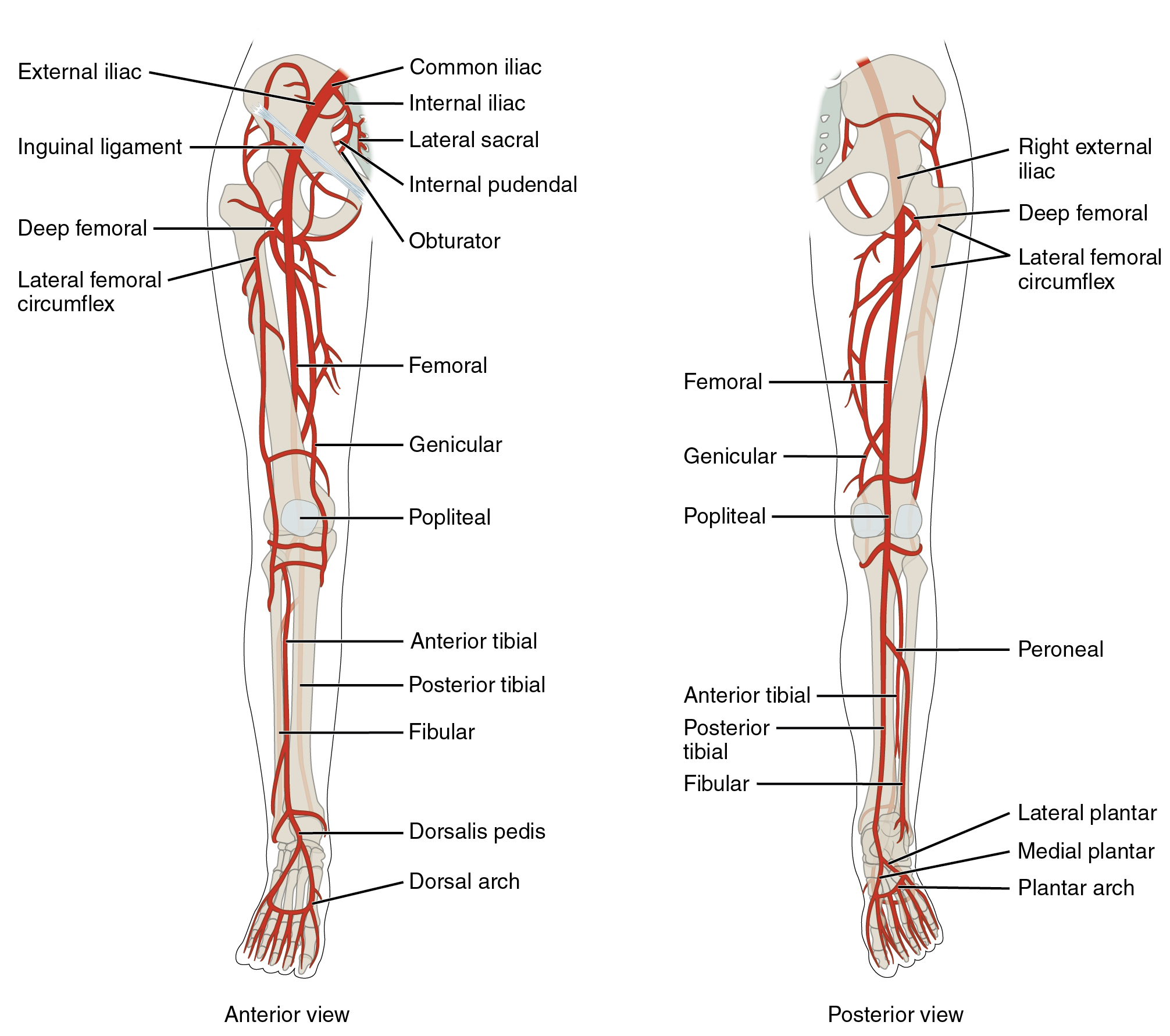
Arteries of the Lower Limb, Anterior and Posterior Views. This detailed illustration shows the arterial anatomy of the lower limb from both anterior and posterior perspectives. Labeled vessels include the common, external, and internal iliac arteries, femoral artery, profunda femoris (deep femoral) artery with its lateral and medial circumflex branches, genicular artery, popliteal artery, anterior and posterior tibial arteries, fibular (peroneal) artery, dorsalis pedis artery, medial and lateral plantar arteries, and the dorsal and plantar arches.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
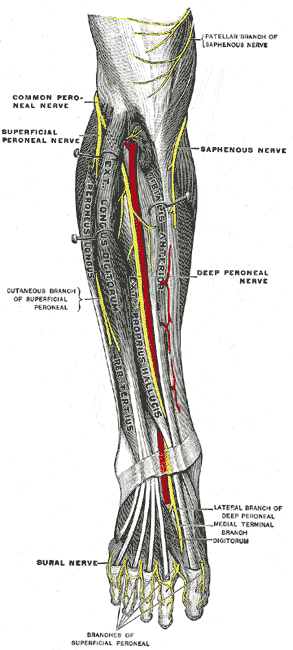
Deep Fibular Nerve and Related Structures. The deep fibular nerve courses through the anterior compartment of the leg in close association with the anterior tibial artery. Distal branching includes lateral and medial terminal branches on the dorsum of the foot. Adjacent nerves, such as the superficial fibular, saphenous, and sural nerves, are also illustrated.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Kaur G, Lalwani R, Khan MM, Athavale SA. Muscle Architecture of Leg Muscles: Functional and Clinical Significance. Acta medica Lituanica. 2023:30(2):194-205. doi: 10.15388/Amed.2023.30.2.12. Epub 2023 Jul 31 [PubMed PMID: 38516510]
Thakkar R, Tran S, Gillie M, Anderson J. Chronic Exertional Compartment Syndrome in a Fire Captain. Cureus. 2022 Jul:14(7):e27321. doi: 10.7759/cureus.27321. Epub 2022 Jul 27 [PubMed PMID: 36043013]
Taylor RM, Sullivan MP, Mehta S. Acute compartment syndrome: obtaining diagnosis, providing treatment, and minimizing medicolegal risk. Current reviews in musculoskeletal medicine. 2012 Sep:5(3):206-13. doi: 10.1007/s12178-012-9126-y. Epub [PubMed PMID: 22644598]
Lezak B, Wehrle CJ, Summers S. Anatomy, Bony Pelvis and Lower Limb: Posterior Tibial Artery. StatPearls. 2026 Jan:(): [PubMed PMID: 30725666]
Mróz I, Kielczewski S, Pawlicki D, Kurzydło W, Bachul P, Konarska M, Bereza T, Walocha K, Kaythampillai LN, Depukat P, Pasternak A, Bonczar T, Chmielewski P, Mizia E, Skrzat J, Mazur M, Warchoł Ł, Tomaszewski K. Blood vessels of the shin - anterior tibial artery - anatomy and embryology - own studies and review of the literature. Folia medica Cracoviensia. 2016:56(1):33-47 [PubMed PMID: 27513837]
Gros J, Tabin CJ. Vertebrate limb bud formation is initiated by localized epithelial-to-mesenchymal transition. Science (New York, N.Y.). 2014 Mar 14:343(6176):1253-6. doi: 10.1126/science.1248228. Epub [PubMed PMID: 24626928]
Level 3 (low-level) evidenceBarham G, Clarke NM. Genetic regulation of embryological limb development with relation to congenital limb deformity in humans. Journal of children's orthopaedics. 2008 Feb:2(1):1-9. doi: 10.1007/s11832-008-0076-2. Epub 2008 Feb 7 [PubMed PMID: 19308596]
Lezak B, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Foot Veins. StatPearls. 2026 Jan:(): [PubMed PMID: 31194435]
Karauda P, Paulsen F, Polguj M, Diogo R, Olewnik Ł. Morphological variability of the fibularis tertius tendon in human foetuses. Folia morphologica. 2022:81(2):451-457. doi: 10.5603/FM.a2021.0039. Epub 2021 Apr 26 [PubMed PMID: 33899207]
Węgiel A, Zielinska N, Maślanka K, Gonera B, Kurtys K, Olewnik Ł. Accessory slip of fibularis tertius to extensor digitorum longus - an unreported variant. Folia morphologica. 2025:84(3):779-783. doi: 10.5603/fm.100239. Epub 2024 Dec 15 [PubMed PMID: 39674898]
Marin-Concha J, Rengifo P, Tapia P, Kaiser D, Siepmann T. Prevalence and characteristics of the aberrant anterior tibial artery: a single-center magnetic resonance imaging study and scoping review. BMC musculoskeletal disorders. 2021 Nov 2:22(1):922. doi: 10.1186/s12891-021-04801-9. Epub 2021 Nov 2 [PubMed PMID: 34727902]
Level 2 (mid-level) evidenceTarasiuk A, Tubbs RS, Zielinska N, Karauda P, Gonera B, Olewnik Ł. Variations of the popliteal artery: A review. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2023 Aug:249():152100. doi: 10.1016/j.aanat.2023.152100. Epub 2023 Apr 25 [PubMed PMID: 37105405]
Palmisano LL, Launico MV. Anatomy, Bony Pelvis and Lower Limb: Calf Deep Peroneal Nerve (Deep Fibular Nerve). StatPearls. 2026 Jan:(): [PubMed PMID: 30252289]
Khan IA, Mahabadi N, D'Abarno A, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Leg Lateral Compartment. StatPearls. 2026 Jan:(): [PubMed PMID: 30137811]
van Zantvoort APM, de Bruijn JA, Hundscheid HPH, Teijink JAW, Scheltinga MR. Lower Leg Lateral Chronic Exertional Compartment Syndrome: Prospective Surgical Treatment Outcomes for Isolated or Combined Lateral Fasciotomy. Foot & ankle international. 2023 Nov:44(11):1097-1104. doi: 10.1177/10711007231192076. Epub 2023 Sep 19 [PubMed PMID: 37724857]
raza F, Mabrouk A, Kaiser K. Tibial Anterior Compartment Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 30085512]
Day CP, Orme R. Popliteal artery branching patterns -- an angiographic study. Clinical radiology. 2006 Aug:61(8):696-9 [PubMed PMID: 16843754]
Level 2 (mid-level) evidenceOlin JW, Sealove BA. Peripheral artery disease: current insight into the disease and its diagnosis and management. Mayo Clinic proceedings. 2010 Jul:85(7):678-92. doi: 10.4065/mcp.2010.0133. Epub [PubMed PMID: 20592174]
Thangada ND, McDermott MM. Exercise Therapy for Peripheral Artery Disease. Current cardiology reports. 2024 May:26(5):405-412. doi: 10.1007/s11886-024-02043-4. Epub 2024 May 9 [PubMed PMID: 38722492]
McDermott MM. Peripheral Artery Disease in the Legs. The New England journal of medicine. 2026 Jan 29:394(5):486-496. doi: 10.1056/NEJMcp2501200. Epub [PubMed PMID: 41604641]
Ravilla A. Medical Management of Peripheral Arterial Disease. Techniques in vascular and interventional radiology. 2026 Mar:29(1):101100. doi: 10.1016/j.tvir.2026.101100. Epub 2026 Feb 6 [PubMed PMID: 41826022]
Gornik HL, Aronow HD, Goodney PP, Arya S, Brewster LP, Byrd L, Chandra V, Drachman DE, Eaves JM, Ehrman JK, Evans JN, Getchius TSD, Gutiérrez JA, Hawkins BM, Hess CN, Ho KJ, Jones WS, Kim ESH, Kinlay S, Kirksey L, Kohlman-Trigoboff D, Long CA, Pollak AW, Sabri SS, Sadwin LB, Secemsky EA, Serhal M, Shishehbor MH, Treat-Jacobson D, Wilkins LR, Peer Review Committee Members. 2024 ACC/AHA/AACVPR/APMA/ABC/SCAI/SVM/SVN/SVS/SIR/VESS Guideline for the Management of Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2024 Jun 11:149(24):e1313-e1410. doi: 10.1161/CIR.0000000000001251. Epub 2024 May 14 [PubMed PMID: 38743805]
Level 1 (high-level) evidenceMabvuure NT, Malahias M, Hindocha S, Khan W, Juma A. Acute compartment syndrome of the limbs: current concepts and management. The open orthopaedics journal. 2012:6():535-43. doi: 10.2174/1874325001206010535. Epub 2012 Nov 30 [PubMed PMID: 23248724]
Wang H, Qi X, Luo H, Zhang Q, Chen Y, Sun J. Catheter-directed thrombolysis through anterior tibial vein for treating acute extensive deep venous thrombosis. Journal of vascular surgery. Venous and lymphatic disorders. 2018 Nov:6(6):681-688. doi: 10.1016/j.jvsv.2018.04.013. Epub 2018 Aug 17 [PubMed PMID: 30126796]
Level 2 (mid-level) evidenceYosipovitch G, Nedorost ST, Silverberg JI, Friedman AJ, Canosa JM, Cha A. Stasis Dermatitis: An Overview of Its Clinical Presentation, Pathogenesis, and Management. American journal of clinical dermatology. 2023 Mar:24(2):275-286. doi: 10.1007/s40257-022-00753-5. Epub 2023 Feb 17 [PubMed PMID: 36800152]
Level 3 (low-level) evidenceJanßen S, Schmölders J, Jansen TM, Ertas N, Rembe JD, Homey B, Hoff NP. Intermittent Pneumatic Impulse Compression in the Treatment of Stasis Dermatitis-A Monocenter Randomized Controlled Trial. Journal of clinical medicine. 2025 May 9:14(10):. doi: 10.3390/jcm14103321. Epub 2025 May 9 [PubMed PMID: 40429319]
Level 1 (high-level) evidenceVasudevan B. Venous leg ulcers: Pathophysiology and Classification. Indian dermatology online journal. 2014 Jul:5(3):366-70. doi: 10.4103/2229-5178.137819. Epub [PubMed PMID: 25165676]