Introduction
The anatomy of the head and neck is complex due to the sheer number of fine structures in this region, many of which have variable depth and course. From a clinical standpoint, the head and neck maintain several critical neurovascular structures that have essential functions and potentially disastrous consequences if injured during surgery or a traumatic event. The neck is subdivided into smaller regions, zones, and compartments to help maintain the organization of this highly complex area. The 2 primary regions of the neck are the anterior and posterior triangles, the borders of which are defined by readily identifiable anatomic structures. These triangles are found deep to the skin, subcutaneous tissue, superficial cervical fascia, and platysma muscle and span the entire length of the neck. Muscles, nerves, blood vessels, lymphatics, and adipose tissue are present within these triangles.
The posterior cervical region contains major neurovascular structures and lymphatic pathways that are frequently involved in cervical lymphadenopathy, traumatic injuries, and peripheral nerve dysfunction. This region also serves as a key surgical landmark for procedures, such as cervical plexus and interscalene nerve blocks and neck dissections, in which precise anatomic knowledge helps minimize iatrogenic injury. A strong grasp of the anatomy and function of the posterior cervical region enables clinicians to accurately localize pathology, perform procedures safely, and interpret clinical findings involving the neck and upper extremity.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Anatomic Boundaries
The posterior triangle occupies the posterolateral aspect of the posterior cervical region on each side of the neck. (see Image. Surface Anatomy of the Anterolateral Cervical Region). Distinct anatomic borders define this area. The anterior border is bounded by the posterior aspect of the sternocleidomastoid (SCM) muscle. The posterior border is delineated by the anterior border of the trapezius muscle. The union of the SCM and the trapezius at the superior nuchal line of the occipital bone forms the apex of the posterior triangle. The superior aspect of the middle 1/3 of the clavicle defines the inferior boundary, which forms the base of the posterior triangle (see Image. Anatomical Structures of the Lateral Neck).
The inferior belly of the omohyoid muscle further subdivides the posterior triangle of the neck into 2 smaller triangles. The omohyoid consists of superior and inferior bellies joined by an intermediate tendon, which lies just posterior to the inferior attachment of the SCM. The superior belly extends from the body of the hyoid bone to the intermediate tendon and lies within the anterior triangle of the neck. The inferior belly originates from the lateral end of the superior border of the scapula and inserts on the intermediate tendon. The inferior belly traverses the posterior triangle of the neck. The area superior to the omohyoid is the occipital triangle, whereas the area inferior to the muscle is the subclavian triangle.[1]
The superficial border, or "roof," of the posterior triangle of the neck consists of the investing layer of the deep cervical fascia. The deep cervical fascia subdivides into several distinct layers that further organize the structures of the neck. The investing layer of the deep cervical fascia lies just deep to the superficial fascia, a sheet of loose connective tissue containing the platysma. The investing layer of the deep cervical fascia forms a single layer over the roof of the posterior triangle. However, the investing layer splits into 2 layers to enclose the SCM and infrahyoid muscles anteriorly and the trapezius posteriorly, thereby "investing" these muscles. Several structures originating deeper in the neck pierce the investing layer of the deep cervical fascia within the posterior triangle to reach more superficial structures, including the external jugular vein and the transverse cervical, supraclavicular, lesser occipital, and greater auricular nerves.[2]
The deep border, or "floor," of the posterior triangle of the neck consists of the prevertebral layer of the deep cervical fascia. The prevertebral layer surrounds the cervical vertebrae and the deep prevertebral muscles of the neck. The space between the investing and prevertebral layers of the deep cervical fascia contains the contents of the posterior triangle of the neck (see Image. Cross-Section of the Human Neck).[3]
Function
The posterior cervical region contains the posterior triangle of the neck, one of the major anatomic subdivisions of the cervical area. Muscles and fascial layers of the posterior cervical region form natural boundaries that organize the neck and its contents (see Image. Musculature of the Posterior Neck). The posterior cervical region also contains muscles, nerves, blood vessels, and lymphatics.
Embryology
The pharyngeal apparatus gives rise to the structures of the head and neck. The pharyngeal apparatus consists of 6 branchial arches that develop in a cranial-to-caudal direction. Each arch contains mesoderm and neural crest cells that form cartilage, nerves, fascia, and muscles. Branchial clefts of ectodermal origin line the superficial surface of the arches. Endodermal branchial pouches line the deep surface of the arches.[4]
The SCM and the trapezius, which occupy a large portion of the posterior cervical region and form the borders of the posterior triangle, develop from somites and neural crest cells located just caudal to the 6th branchial arch. A case study describes a congenital absence of the posterior triangle resulting from fusion of the SCM and the trapezius. Embryologically, this anomaly results from failure of the mesoderm of the 6th branchial arch to separate and subsequently degenerate.[5]
Blood Supply and Lymphatics
Blood Vessels
Posterior triangle vessels are located within the subclavian triangle, inferior to the omohyoid. The subclavian artery divides anatomically into 3 parts. The 1st part is the most proximal segment. The 2nd part passes posterior to the anterior scalene muscle. The 3rd part is the most distal segment and enters the posterior triangle after emerging from behind the anterior scalene. The subclavian artery becomes the axillary artery after passing over the 1st rib.
The transverse cervical and suprascapular arteries also course through the subclavian triangle anterior to the anterior scalene. Both arteries arise from the thyrocervical trunk, a major branch of the 1st part of the subclavian artery that originates immediately medial to the anterior scalene.
The subclavian, transverse cervical, and suprascapular veins accompany their corresponding arteries through the posterior triangle. However, the subclavian vein passes anterior to the anterior scalene, unlike the subclavian artery. The external jugular vein courses superficial to the posterior triangle before piercing the investing layer of the deep cervical fascia to enter the posterior triangle and drain into the subclavian vein.[6]
Lymphatics
Several lymph node groups are located within the posterior cervical region. The supraclavicular lymph nodes lie along the superior border of the clavicle within the posterior triangle. The posterior cervical lymph nodes course along the external jugular vein within the posterior triangle. The superficial cervical lymph nodes lie along the anterior surface of the SCM, whereas the deep cervical lymph nodes follow the posterior surface of the same muscle. The posterior auricular and occipital lymph node groups are situated near the apex of the posterior triangle, superficial to the superior portions of the SCM and the trapezius, respectively (see Image. Lymph Nodes of the Head and Neck).[7]
The lymphatic and circulatory systems converge near the posterior cervical region. On the right side of the body, the right lymphatic duct empties into the junction of the right internal jugular and right subclavian veins. The right lymphatic duct drains lymph from the right side of the head and neck, the right upper extremity, and the right hemithorax. The thoracic duct drains lymph from the remainder of the body. The thoracic duct empties into the junction of the left internal jugular and left subclavian veins.[8]
Nerves
The spinal accessory nerve (cranial nerve XI) provides motor innervation to the SCM and the trapezius.[9] After exiting the skull through the jugular foramen, the spinal accessory nerve courses along the deep surface of the SCM. The nerve descends obliquely through the posterior triangle. Investing fascia encloses the spinal accessory nerve as it crosses the posterior triangle and continues to the deep surface of the trapezius.[10]
The superficial branches of the cervical plexus supplying cutaneous sensation to the cervical region emerge from the posterior aspect of the SCM near its midpoint at the nerve point of the neck, or the Erb point.[11] The anterior rami of the cervical spinal nerves pierce the investing fascia and divide into 4 cutaneous nerves that course deep to the platysma.
The lesser occipital nerve arises from the 2nd cervical spinal nerve and ascends posterior to the SCM to innervate the scalp and neck posterior to the ear.[12] The greater auricular nerve arises from the 2nd and 3rd cervical spinal nerves and ascends along the anterior surface of the SCM to innervate the skin over the mastoid and parotid regions inferior to the ear.[13] The transverse cervical nerve arises from the 2nd and 3rd cervical spinal nerves and courses horizontally across the SCM to innervate the anterior neck. The supraclavicular nerve arises from the 3rd and 4th cervical spinal nerves and descends across the investing fascia over the posterior triangle before branching extensively to innervate the skin over the clavicle and first 2 ribs.[14]
The phrenic nerve lies deep to the posterior triangle within the prevertebral fascia as it courses along the anterior surface of the anterior scalene. The anterior rami of the 5th cervical through the 1st thoracic spinal nerves form the roots and trunks of the brachial plexus, which also lie within the prevertebral fascia between the anterior and middle scalenes.[15]
Muscles
The largest muscles of the posterior cervical region are the SCM and the trapezius. The margins of these muscles form the anterior and posterior borders of the posterior triangle, respectively. The SCM originates from the anterior surface of the manubrium and the medial 1/3 of the clavicle. This muscle inserts on the mastoid process and the lateral aspect of the superior nuchal line. The SCM rotates the head contralaterally and flexes the neck ipsilaterally. The trapezius is a broad muscle with an extensive origin from the superior nuchal line and the spinous processes of the C2 to T12 vertebrae. This muscle inserts on the posterior aspect of the lateral 1/3 of the clavicle, the acromion, and the spine of the scapula. The trapezius elevates, adducts, and depresses the scapula. The muscle also assists scapular rotation during arm abduction above the horizontal.[16][17]
The inferior belly of the omohyoid is the only muscle located within the true boundaries of the posterior triangle.[18][19] The inferior belly passes through the triangle in an anterior-to-posterior direction approximately 2.5 cm above the clavicle and further subdivides the posterior triangle into the occipital and subclavian triangles. The infrahyoid layer of the pretracheal fascia encloses the omohyoid. The infrahyoid layer is another component of the deep cervical fascia, along with the investing and prevertebral layers. Several posterior cervical muscles lie just deep to the posterior triangle and are enclosed by the prevertebral layer of the deep cervical fascia, collectively forming the prevertebral muscles. The prevertebral fascia forms the deep border of the posterior triangle, and the underlying prevertebral muscles constitute the floor. The prevertebral muscles include the anterior, middle, and posterior scalenes and the levator scapulae.
Physiologic Variants
Anatomic variation of the posterior cervical region occurs most commonly at the nerve point of the neck. The terminal distributions of the cutaneous branches of the cervical plexus are relatively consistent, but the origins of these branches vary considerably. After a cervical spinal nerve pierces the investing layer of the deep cervical fascia, the nerve divides into 4 cutaneous branches. However, the branching point is often variable. A cervical spinal nerve may divide before emerging from the investing fascia, allowing 1 to 4 cutaneous nerves to pierce the investing fascia individually. The transverse cervical and supraclavicular nerves may also travel together for a greater distance before dividing, and the same pattern may occur in the lesser occipital and greater auricular nerves.
Surgical Considerations
Various surgical procedures rely on detailed knowledge of posterior cervical anatomy. For instance, cutaneous branches of the cervical plexus may be anesthetized with a superficial cervical plexus block. When performing this procedure, the anesthesia provider inserts a needle along the posterior aspect of the SCM through the skin and platysma. Local anesthetic is injected near the site where the cutaneous branches emerge from the investing fascia. Deep or unintended spread of the local anesthetic can increase the risk of phrenic nerve involvement, so the technique is typically avoided in patients with respiratory comorbidities, such as chronic obstructive pulmonary disease. Superficial cervical plexus blocks are often performed bilaterally with or without ultrasound guidance and are used for analgesia in thyroidectomy, parathyroidectomy, and carotid endarterectomy (see Image. Area Covered by a Superficial Cervical Plexus Block).[20]
The interscalene block is another regional anesthetic technique involving the posterior cervical region.[21] This procedure targets the roots and trunks of the brachial plexus to provide anesthesia for orthopedic procedures involving the clavicle or humerus. When performing an interscalene block, the anesthesia provider typically inserts a needle posterior to the clavicular head of the SCM through the prevertebral fascia and into the interscalene groove. Ultrasound guidance identifies the superior, middle, and inferior trunks of the brachial plexus during the procedure. The trunks appear on ultrasound as hollow circles arranged in a "stoplight" pattern (see Image. Interscalene Block Regional Landmarks).
Several major structures within the posterior cervical region are susceptible to inadvertent injury during surgery, including the spinal accessory nerve.[22] Intraoperative stimulation of the spinal accessory nerve helps map its course and motor distribution, reducing the risk of iatrogenic injury.[23]
Clinical Significance
Cervical lymphadenopathy is a common manifestation of various disease processes. Lymph node enlargement has numerous causes, and physical examination is essential for determining the underlying etiology. Soft, tender lymph nodes typically result from acute inflammatory processes, such as infectious mononucleosis or streptococcal pharyngitis. In contrast, large, firm, rubbery lymph nodes often indicate chronic conditions, such as lymphoma.[24]
Nerve injury within the posterior triangle is another important clinical consideration. Spinal accessory nerve injury can impair shoulder shrugging and arm elevation above the horizontal because of trapezius dysfunction. Damage to the spinal accessory nerve within the posterior triangle spares the SCM because motor branches arise proximal to the triangle.[25] Trauma and iatrogenic injury can also affect the cutaneous branches of the cervical plexus, resulting in sensory deficits over the cervical region. Recognition of the sensory distribution of the cervical plexus helps localize the affected nerve.
Media
(Click Image to Enlarge)
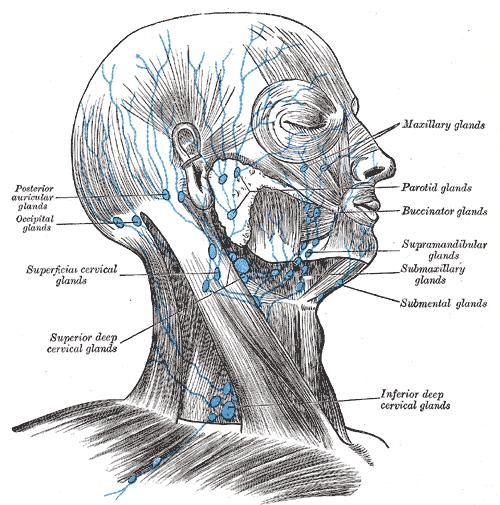
Lymph Nodes of the Head and Neck. This illustration shows the major lymph node groups of the head and neck, including the posterior auricular, occipital, superficial cervical, deep cervical, submental, submandibular, supramandibular, buccinator, parotid, and maxillary groups. The original labels reflect historical anatomic nomenclature.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
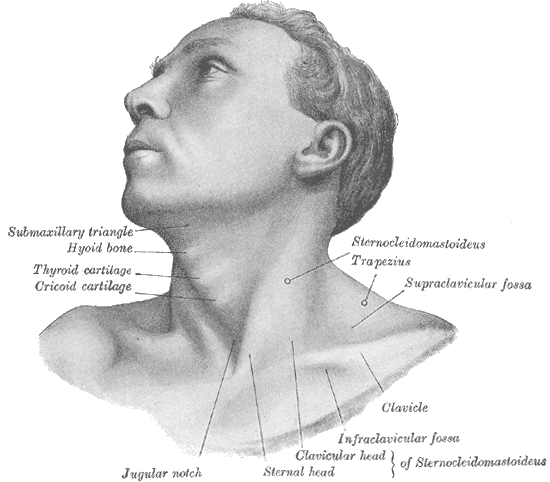
Surface Anatomy of the Anterolateral Cervical Region. This illustration features key landmarks and surface features on the human head and neck, including the submaxillary triangle, hyoid bone, thyroid cartilage, cricoid cartilage, jugular notch, sternal and clavicular heads of sternocleidomastoideus, infraclavicular fossa, clavicle, supraclavicular fossa, trapezius, and sternocleidomastoideus belly.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
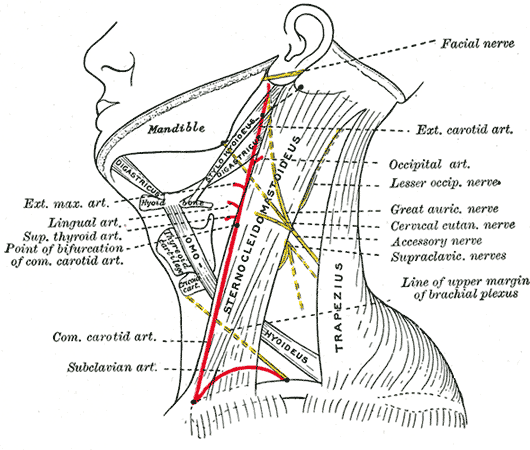
Anatomical Structures of the Lateral Neck. This diagram shows the anterior and posterior triangles of the neck separated by the sternocleidomastoid. The digastric and omohyoid muscles further subdivide these spaces, creating smaller anatomical regions. The red lines highlight the course and branching points of the common carotid artery, as well as the trajectory of the subclavian artery. The yellow lines show the locations of the spinal accessory and cervical nerves.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
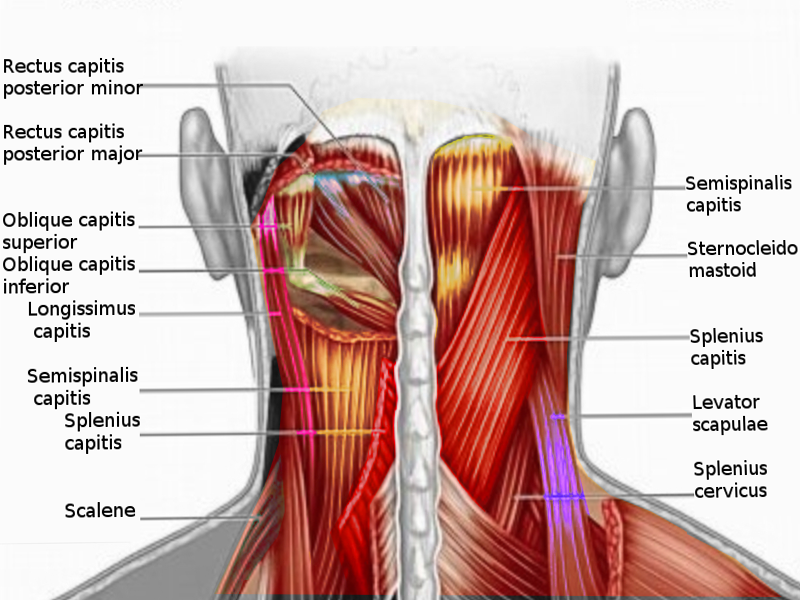
Musculature of the Posterior Neck. This anatomical diagram illustrates the deep and superficial muscle layers of the dorsal neck region, showing the rectus capitis posterior minor and major, oblique capitis superior and inferior, longissimus capitis, semispinalis capitis, splenius capitis, scalene, sternocleidomastoid, levator scapulae, and splenius cervicus.
Image courtesy S Bhimji MD
(Click Image to Enlarge)
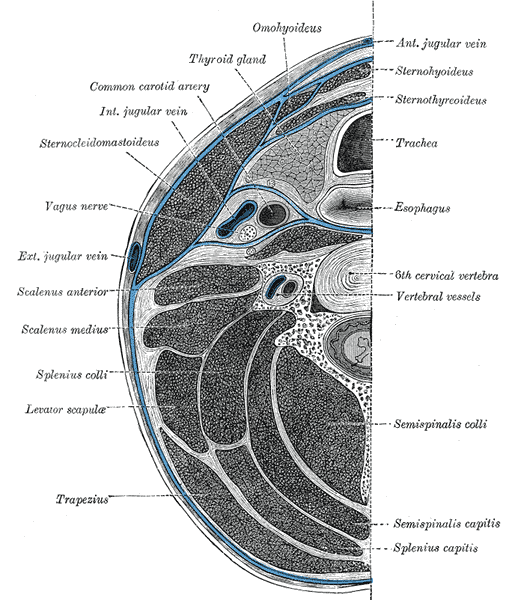
Cross-Section of the Human Neck. This diagram illustrates the anatomical relationships between the cervical fascia, major muscle groups, and visceral organs at the C6 level. Key neurovascular structures, including the carotid artery and vagus nerve, are shown within their respective compartments.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
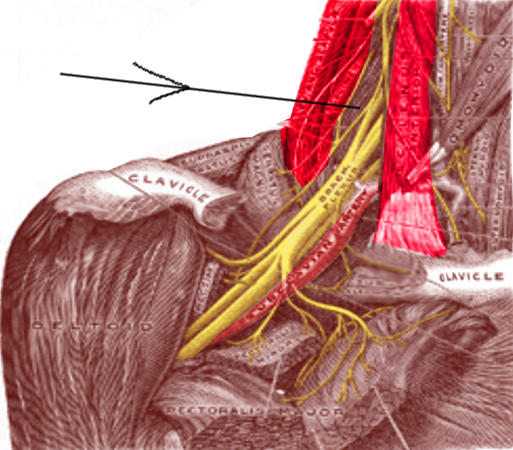
Interscalene Block Regional Landmarks. This illustration demonstrates the interscalene groove located between the scalenus anterior and medius muscles (dark red). The black arrow indicates the injection site for the nerve block, where the brachial plexus (yellow) sits adjacent to the subclavian artery (light red).
Contributed by S Bhimji, MD
(Click Image to Enlarge)

Area Covered by a Superficial Cervical Plexus Block. This clinical image highlights the sensory distribution of a superficial cervical plexus block. Local anesthetic deposited near the superficial branches of the cervical plexus (C2 to C4) provides anesthesia of the earlobe, neck, and clavicular regions.
Contributed by J Hipskind, MD
References
Ihnatsenka B, Boezaart AP. Applied sonoanatomy of the posterior triangle of the neck. International journal of shoulder surgery. 2010 Jul:4(3):63-74. doi: 10.4103/0973-6042.76963. Epub [PubMed PMID: 21472066]
Sutcliffe P, Lasrado S. Anatomy, Head and Neck, Deep Cervical Neck Fascia. StatPearls. 2026 Jan:(): [PubMed PMID: 31082135]
Miyake N, Takeuchi H, Cho BH, Murakami G, Fujimiya M, Kitano H. Fetal anatomy of the lower cervical and upper thoracic fasciae with special reference to the prevertebral fascial structures including the suprapleural membrane. Clinical anatomy (New York, N.Y.). 2011 Jul:24(5):607-18. doi: 10.1002/ca.21125. Epub 2011 Jan 13 [PubMed PMID: 21647961]
Mnatsakanian A, Minutello K, Black AC, Bordoni B. Anatomy, Head and Neck, Retropharyngeal Space. StatPearls. 2026 Jan:(): [PubMed PMID: 30725729]
Singh S, Chauhan P, Loh HK, Mehta V, Suri RK. Absence of Posterior Triangle: Clinical and Embryological Perspective. Journal of clinical and diagnostic research : JCDR. 2017 Feb:11(2):AD01-AD02. doi: 10.7860/JCDR/2017/23896.9176. Epub 2017 Feb 1 [PubMed PMID: 28384846]
Level 3 (low-level) evidenceWeiglein AH, Moriggl B, Schalk C, Künzel KH, Müller U. Arteries in the posterior cervical triangle in man. Clinical anatomy (New York, N.Y.). 2005 Nov:18(8):553-7 [PubMed PMID: 16187318]
Guidera AK, Dawes PJ, Fong A, Stringer MD. Head and neck fascia and compartments: no space for spaces. Head & neck. 2014 Jul:36(7):1058-68. doi: 10.1002/hed.23442. Epub 2014 Jan 29 [PubMed PMID: 23913739]
Johnson OW, Chick JF, Chauhan NR, Fairchild AH, Fan CM, Stecker MS, Killoran TP, Suzuki-Han A. The thoracic duct: clinical importance, anatomic variation, imaging, and embolization. European radiology. 2016 Aug:26(8):2482-93. doi: 10.1007/s00330-015-4112-6. Epub 2015 Dec 1 [PubMed PMID: 26628065]
Abakay MA, Güneş S, Küçük C, Yazıcı ZM, Gülüstan F, Arslan MN, Sayın İ. Accessory Nerve Anatomy in Anterior and Posterior Cervical Triangle: A Fresh Cadaveric Study. Turkish archives of otorhinolaryngology. 2020 Sep:58(3):149-154. doi: 10.5152/tao.2020.5263. Epub 2020 Sep 1 [PubMed PMID: 33145498]
Kim DH, Cho YJ, Tiel RL, Kline DG. Surgical outcomes of 111 spinal accessory nerve injuries. Neurosurgery. 2003 Nov:53(5):1106-12; discussion 1102-3 [PubMed PMID: 14580277]
Level 2 (mid-level) evidenceSchoenbrunner A, Konschake M, Zwierzina M, Egro FM, Moriggl B, Janis JE. The Great Auricular Nerve Trigger Site: Anatomy, Compression Point Topography, and Treatment Options for Headache Pain. Plastic and reconstructive surgery. 2022 Jan 1:149(1):203-211. doi: 10.1097/PRS.0000000000008673. Epub [PubMed PMID: 34807011]
Saglam L, Coskun O, Gayretli O. Morphological and morphometric anatomy of the lesser occipital nerve and its possible clinical relevance. Scientific reports. 2024 Mar 10:14(1):5844. doi: 10.1038/s41598-024-55648-8. Epub 2024 Mar 10 [PubMed PMID: 38462647]
Fenech M, Gallagher J, Berry C. Sonographic anatomy and imaging of the great auricular nerve. Surgical and radiologic anatomy : SRA. 2025 Nov 13:48(1):3. doi: 10.1007/s00276-025-03765-y. Epub 2025 Nov 13 [PubMed PMID: 41233613]
Lee JH, Cheng KL, Choi YJ, Baek JH. High-resolution Imaging of Neural Anatomy and Pathology of the Neck. Korean journal of radiology. 2017 Jan-Feb:18(1):180-193. doi: 10.3348/kjr.2017.18.1.180. Epub 2017 Jan 5 [PubMed PMID: 28096728]
Falyar CR, Shaffer KM, Perera RA. Localization of the brachial plexus: Sonography versus anatomic landmarks. Journal of clinical ultrasound : JCU. 2016 Sep:44(7):411-5. doi: 10.1002/jcu.22354. Epub 2016 Mar 29 [PubMed PMID: 27028598]
Mnatsakanian A, Al Khalili Y. Anatomy, Head and Neck, Thyroid Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 31082107]
Henson B, Kadiyala B, Edens MA. Anatomy, Back, Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 30725759]
Riju J, Verma P. Posterior Belly of Digastric Muscle is not Always an Intern's Friend, During Neck Dissection. Indian journal of otolaryngology and head and neck surgery : official publication of the Association of Otolaryngologists of India. 2024 Apr:76(2):2149-2150. doi: 10.1007/s12070-023-04359-z. Epub 2023 Dec 7 [PubMed PMID: 38566629]
Toledano N, Dar G. Ultrasonographic measurements of the omohyoid muscle during shoulder muscles contraction. Journal of ultrasound. 2023 Sep:26(3):711-716. doi: 10.1007/s40477-022-00754-4. Epub 2022 Nov 28 [PubMed PMID: 36437441]
Senapathi TGA, Widnyana IMG, Aribawa IGNM, Wiryana M, Sinardja IK, Nada IKW, Jaya AGPS, Putra IGKS. Ultrasound-guided bilateral superficial cervical plexus block is more effective than landmark technique for reducing pain from thyroidectomy. Journal of pain research. 2017:10():1619-1622. doi: 10.2147/JPR.S138222. Epub 2017 Jul 14 [PubMed PMID: 28761368]
Kaye AD, Upshaw WC, Holley C, Bailey PD, Tassin JP, Frolov MV, Sudini S, Miller BC, Palowsky ZR, Kataria S, Ahmadzadeh S, Shekoohi S, Robinson CL. Overview and Comparison of Interscalene Block Techniques for Brachial Plexus Pain Management. Current pain and headache reports. 2024 Dec 30:29(1):1. doi: 10.1007/s11916-024-01346-z. Epub 2024 Dec 30 [PubMed PMID: 39739068]
Level 3 (low-level) evidenceFabiano AS, Pernik MN, MacAllister M, Payne R. Accessory Nerve Disruption Following Core-Needle Biopsy: A Review of Iatrogenic Accessory Nerve Injuries and an Illustrative Case. World neurosurgery. 2022 May:161():156-161. doi: 10.1016/j.wneu.2022.02.091. Epub 2022 Feb 25 [PubMed PMID: 35219915]
Level 3 (low-level) evidenceBrînzeu A, Sindou M. Functional anatomy of the accessory nerve studied through intraoperative electrophysiological mapping. Journal of neurosurgery. 2017 Mar:126(3):913-921. doi: 10.3171/2015.11.JNS15817. Epub 2016 Apr 8 [PubMed PMID: 27058194]
Fernández Aceñero MJ, Caso Viesca A, Díaz Del Arco C. Role of fine needle aspiration cytology in the management of supraclavicular lymph node metastasis: Review of our experience. Diagnostic cytopathology. 2019 Mar:47(3):181-186. doi: 10.1002/dc.24064. Epub 2018 Nov 23 [PubMed PMID: 30468321]
Gordon SL, Graham WP 3rd, Black JT, Miller SH. Acessory nerve function after surgical procedures in the posterior triangle. Archives of surgery (Chicago, Ill. : 1960). 1977 Mar:112(3):264-8 [PubMed PMID: 843216]
Level 3 (low-level) evidence