Introduction
The esophagus is a tubular, elongated organ of the digestive system that connects the pharynx to the stomach (see Images. Digestive and Respiratory Structures Anatomically Related to the Esophagus; Muscles of the Cheek and Pharynx; Posterior View of the Pharynx, Esophagus, and Thoracic Structures). Food passes through the esophagus to reach the stomach for further digestion. This tubular organ follows a course posterior to the trachea and heart, anterior to the spinal column, and traverses the diaphragm before entering the stomach.[1][2]
The esophagus is divided into 3 anatomical segments: cervical, thoracic, and abdominal. The cervical segment begins at the cricopharyngeus and terminates at the suprasternal notch. This section lies just posterior to the trachea and is joined to it via loose connective tissue. Posteriorly, the prevertebral fascia connects the esophagus to the bodies of the 6th through 8th cervical vertebrae. The thoracic duct courses along the left side of the cervical esophagus near the 6th and 7th cervical vertebrae.[3] Laterally, the carotid sheath and the lower poles of the lateral thyroid gland are adjacent to the esophagus in the lower neck.
The thoracic segment extends from the suprasternal notch to the diaphragm, occupying the space between the vertebral column and the trachea in the superior mediastinum. Distally, the esophagus passes posterior to the aortic arch at the level of the T4–T5 intervertebral discs and enters the posterior mediastinum.
The abdominal segment of the esophagus extends from the diaphragm to the cardia of the stomach.[4] This portion passes through the esophageal hiatus, formed by the right crus of the diaphragm at approximately the T10 vertebral level, and terminates at the cardia, typically at the level of T11.
The organ is typically 9 to 10 in (23–25 cm) long in fully grown adults. Sphincters are present at both proximal and distal extremities. The lumen is lined with mucosa and supported by connective tissue, with an outer layer of smooth muscle. The upper esophageal sphincter (UES), located proximally, permits unidirectional passage of food into the organ, whereas the lower esophageal sphincter (LES), located distally, allows unidirectional passage of food into the stomach.[5][6][3]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The primary function of the esophagus is the transport of food from the pharynx into the stomach. This process begins at the UES, located at the junction of the pharynx and proximal esophagus, immediately inferior to the posterior portion of the tongue and oropharynx. The UES, also called the "pharyngoesophageal sphincter," consists of a circular bundle of muscle tissue that is normally contracted and closed. During swallowing, the muscles relax temporarily, permitting the passage of a bolus—composed of food, drink, mucus, and saliva—into the esophagus.
The bolus then enters the esophageal body. Peristaltic movement propels the bolus downward via primary and secondary peristalsis. During the pharyngeal stage of swallowing, contraction of the pharyngeal muscular walls generates an initial peristaltic motion, imparting kinetic energy to the bolus and propelling it through the UES. This wave continues into the esophagus as primary peristalsis. If primary peristalsis fails to transport the bolus to the stomach, continued esophageal distention triggers secondary peristalsis, which persists until the bolus reaches the stomach.
The LES, also termed the "cardiac sphincter" or "cardioesophageal sphincter," lies approximately 1 in (3 cm) proximal to the junction with the stomach. Like the UES, the LES remains normally contracted, preventing retrograde movement of gastric contents into the esophageal body. The LES opens involuntarily during esophageal peristalsis, allowing the bolus to enter the stomach and completing the organ’s primary function.
Although the main role of the esophagus is unidirectional transport from the pharynx to the stomach, the organ also enables retrograde expulsion of material from the stomach through vomiting, eructation, or gag reflex activation. This function is generally undesirable, as refluxed food may cause malnutrition and damage the esophageal lining due to exposure to gastric acid.
Embryology
During the 4th week of human development, the embryo elongates, and the yolk sac separates into intraembryonic and extraembryonic regions. The digestive tube forms within the intraembryonic region, while the extraembryonic portion regresses and disappears by approximately week 12. At this stage, the digestive system subdivides into the foregut, midgut, and hindgut. Continued development of the foregut gives rise to the esophagus.
Blood Supply and Lymphatics
The esophagus has a rich arterial supply and segmental venous drainage. The cervical esophagus and UES receive arterial blood from branches of the inferior thyroid artery. The thoracic esophagus is supplied primarily by esophageal branches of the thoracic aorta, with additional contributions from the bronchial and intercostal arteries. The abdominal segment and LES receive blood from the left gastric artery and a branch of the left phrenic artery. These arteries form a dense network within the submucosa of the esophagus. Venous drainage of the esophagus is segmental. The cervical esophagus drains via the inferior thyroid veins into the brachiocephalic veins. The thoracic esophagus drains into the azygos and hemiazygos veins. The distal esophagus drains via tributaries of the left gastric vein into the portal venous system.[7]
Lymph channels and lymph nodes facilitate lymphatic drainage along the tubular structure (see Image. Lymphatics and Neurovascular Relations of the Trachea). The channels originate as endothelial tubes or blind sacculations, which are also endothelial. These structures converge into larger vessels running longitudinally along the esophagus, orthogonal to the transverse plane. Paired semilunar valves dictate the direction of lymph flow. The channels combine in different areas before entering the respective regional lymph nodes. Drainage occurs in 3 sections of the esophagus, divided into proximal, middle, and distal 3rds, with significant interconnections between segments. Lymph from the proximal 3rd drains via the thoracic duct from deep cervical lymph nodes. The middle 3rd drains into the superior and posterior mediastinal nodes. Lymph from the distal 3rd ultimately enters the gastric and celiac lymph nodes.
Nerves
Innervation of the esophagus involves both the sympathetic and parasympathetic nervous systems. Primary innervation arises from the vagus nerve and spinal nerves T1 to T10 via the thoracic and cervical sympathetic trunks. The vagus nerve mediates parasympathetic motor functions of the esophageal muscles and glands. The thoracic and cervical sympathetic chains provide sympathetic input, contributing to vasoconstriction and maintenance of UES and LES tone, while generally inhibiting esophageal peristalsis and glandular secretion.[8] Both systems convey sensation—the vagus nerve detects pressure, which may be perceived as pain, whereas the sympathetic trunk transmits nociceptive signals more directly.
Muscles
The proximal 3rd of the esophagus consists primarily of skeletal muscle, whereas the distal 2/3 is composed of smooth muscle. Esophageal muscle fibers are arranged bidirectionally. The external layer runs longitudinally, and the internal layer comprises circular fibers. The internal layer facilitates peristaltic contractions that propel boluses through the esophagus and is thicker than the external layer. Thickening and overlapping of the internal fibers at the distal portion of the esophagus, just above the stomach, form the LES, contributing to its function. Proximally, the cricopharyngeus, thyropharyngeus, and craniocervical muscles constitute the UES, with opposing orientations of their respective fibers.
Physiologic Variants
Natural physiological variations of the esophagus are uncommon, with the most frequent differences involving size and length. Congenital abnormalities, although rare, include tracheoesophageal fistula and atresia, esophageal stenosis, esophageal duplication and duplication cysts, esophageal rings, and esophageal webs.
Surgical Considerations
Certain esophageal conditions may require surgical intervention, including esophageal cancer, achalasia, tearing, and esophageal varices. When feasible, laparoscopic surgery is preferred to provide a minimally invasive approach and facilitate faster patient recovery.[9][10]
Clinical Significance
Understanding the anatomy and physiology of the esophagus is critical to the management of diseases affecting this organ. Early detection of most esophageal disorders allows for treatment that can prevent further tissue damage and reduce mortality. The esophagus serves as the primary conduit for food delivery to the stomach, and impairment of this pathway may compromise nutritional intake by limiting access to essential nutrients.
Heartburn and gastroesophageal reflux disease are among the most common esophageal disorders, affecting people across diverse demographics, though prevalence varies by factors like age, higher weight, and geography.[11] A thorough understanding of the LES function in these conditions is critical. Although these disorders are frequently considered minor, they may progress to more severe complications, including esophagitis, ulcers, strictures, Barrett esophagus, and esophageal adenocarcinoma.[12]
Media
(Click Image to Enlarge)
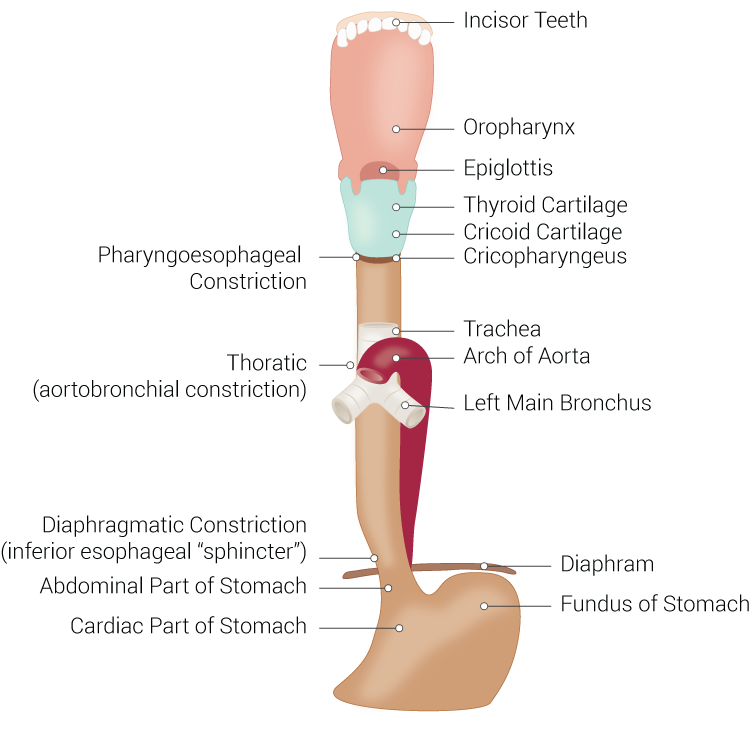
Digestive and Respiratory Structures Anatomically Related to the Esophagus. This illustration shows the esophagus and adjacent digestive and respiratory structures, including the incisors, oropharynx, laryngeal cartilages, trachea, aortic arch, bronchi, diaphragm, stomach, and esophageal constrictions.
Illustrated by B Palmer
(Click Image to Enlarge)
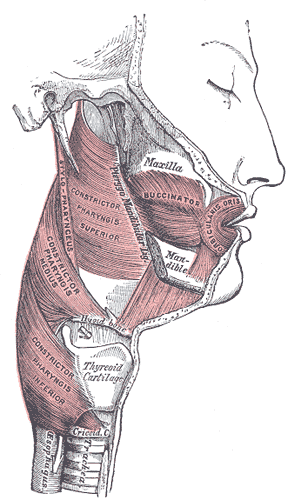
Muscles of the Cheek and Pharynx. This lateral view shows the buccinator, orbicularis oris, and the superior, middle, and inferior pharyngeal constrictor muscles, as well as the thyroid cartilage, trachea, upper esophagus, stylopharyngeus, maxilla, and mandible.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
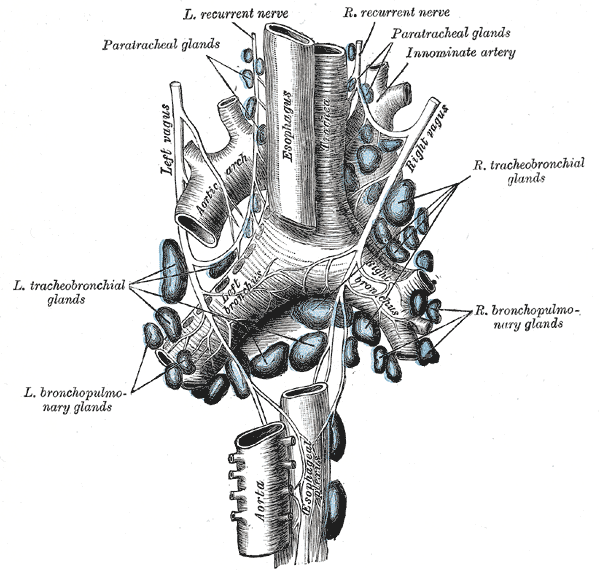
Lymphatics and Neurovascular Relations of the Trachea. This illustration details the extensive lymphatic network of the airway, including the paratracheal, tracheobronchial, and bronchopulmonary glands. The image also identifies the spatial relationship between these nodes and major structures such as the aortic arch, innominate artery, esophagus, and the left and right vagus and recurrent nerves. Other labeled structures include the descending aorta and the branching of the trachea into the left and right primary bronchi.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
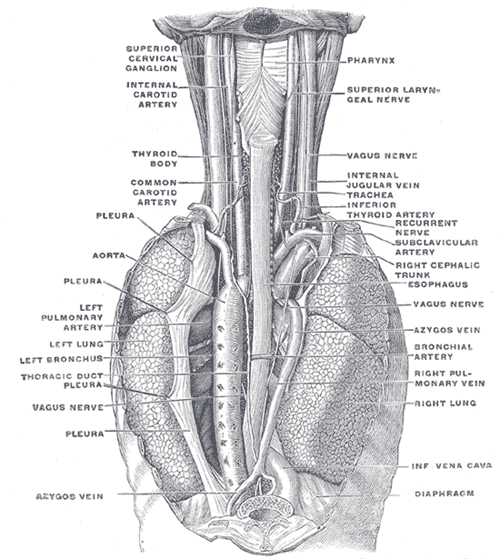
Posterior View of the Pharynx, Esophagus, and Thoracic Structures. This posterior-view illustration shows the pharynx, superior cervical ganglion, internal carotid artery, superior laryngeal nerve, thyroid body, common carotid artery, internal jugular vein, trachea, inferior thyroid artery, recurrent nerve, subclavian artery, right cephalic trunk, esophagus, pleura, aorta, left pulmonary artery, left lung, left bronchus, thoracic duct, azygos vein, right lung, bronchial artery, right pulmonary vein, inferior vena cava, diaphragm, and the vagus nerve along its cervical and thoracic course.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Rizvi S, Wehrle CJ, Law MA. Anatomy, Thorax, Mediastinum Superior and Great Vessels. StatPearls. 2025 Jan:(): [PubMed PMID: 30137860]
Bains KNS, Kashyap S, Lappin SL. Anatomy, Thorax: Diaphragm. StatPearls. 2025 Jan:(): [PubMed PMID: 30137842]
Ilahi M, St Lucia K, Ilahi TB. Anatomy, Thorax, Thoracic Duct. StatPearls. 2025 Jan:(): [PubMed PMID: 30020599]
Hudgi A, Parthasarathy S, Mirza A, Woodcock A, Goosenberg E. Esophagogastroduodenoscopy (EGD). StatPearls. 2026 Jan:(): [PubMed PMID: 30335301]
Mahabadi N, Goizueta AA, Bordoni B. Anatomy, Thorax, Lung Pleura And Mediastinum. StatPearls. 2025 Jan:(): [PubMed PMID: 30085590]
Bardo DME, Biyyam DR, Patel MC, Wong K, van Tassel D, Robison RK. Magnetic resonance imaging of the pediatric mediastinum. Pediatric radiology. 2018 Aug:48(9):1209-1222. doi: 10.1007/s00247-018-4112-1. Epub 2018 Aug 4 [PubMed PMID: 30078043]
Fischer NJ, Morreau J, Sugunesegran R, Taghavi K, Mirjalili SA. A reappraisal of pediatric thoracic surface anatomy. Clinical anatomy (New York, N.Y.). 2017 Sep:30(6):788-794. doi: 10.1002/ca.22913. Epub 2017 Jun 19 [PubMed PMID: 28514496]
Bajwa SA, Toro F, Kasi A. Physiology, Esophagus. StatPearls. 2026 Jan:(): [PubMed PMID: 30085553]
Bradley PJ. Symptoms and Signs, Staging and Co-Morbidity of Hypopharyngeal Cancer. Advances in oto-rhino-laryngology. 2019:83():15-26. doi: 10.1159/000492304. Epub 2019 Feb 12 [PubMed PMID: 30943511]
Level 3 (low-level) evidenceSanghi V, Thota PN. Barrett's esophagus: novel strategies for screening and surveillance. Therapeutic advances in chronic disease. 2019:10():2040622319837851. doi: 10.1177/2040622319837851. Epub 2019 Mar 26 [PubMed PMID: 30937155]
Level 3 (low-level) evidenceGoosenberg E, Vadakekut ES. Gastroesophageal Reflux Disease (GERD). StatPearls. 2026 Jan:(): [PubMed PMID: 32119349]
Gonzalez Ayerbe JI, Hauser B, Salvatore S, Vandenplas Y. Diagnosis and Management of Gastroesophageal Reflux Disease in Infants and Children: from Guidelines to Clinical Practice. Pediatric gastroenterology, hepatology & nutrition. 2019 Mar:22(2):107-121. doi: 10.5223/pghn.2019.22.2.107. Epub 2019 Mar 8 [PubMed PMID: 30899687]