 Anatomy, Head and Neck: Auriculotemporal Nerve
Anatomy, Head and Neck: Auriculotemporal Nerve
Introduction
The auriculotemporal nerve is a branch of the mandibular division of the trigeminal nerve (cranial nerve V). The nerve contains sensory, vasomotor, and parasympathetic fibers. The auriculotemporal nerve usually arises as 2 roots from the posterior division of the mandibular nerve (cranial nerve V3), encircles the middle meningeal artery, and then ascends between the temporomandibular joint (TMJ) and the external acoustic meatus (EAM) to the temporal region, providing sensory innervation to portions of the ear, TMJ, scalp, and dura mater, as well as secretomotor and vasomotor innervation to the parotid gland (see Image. Scalp Nerves and Arteries). Vascular supply to the nerve is derived primarily from branches of the superficial temporal and middle meningeal arteries. Anatomic variation most commonly involves the number and configuration of roots arising from the mandibular nerve.
The auriculotemporal nerve is clinically significant in conditions such as TMJ disease, auriculotemporal neuralgia, Frey syndrome following parotid pathology or intervention, and perineural tumor spread involving the infratemporal fossa and skull base. TMJ procedures and parotidectomy place the auriculotemporal nerve at risk of injury, which may result in pain, paresthesia, or aberrant reinnervation of cutaneous sweat glands and blood vessels. Knowledge of the anatomy and function of this nerve enables accurate diagnosis of regional pain syndromes, guides targeted nerve blockade, and supports operative planning to reduce complications and preserve neural function.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The auriculotemporal nerve contains secretomotor, somatosensory, and vasomotor fibers. Sensory fibers of this peripheral branch of the mandibular nerve have 1st-order neuron cell bodies located in the trigeminal ganglion. After the mandibular nerve exits the skull through the foramen ovale, the auriculotemporal nerve usually arises from the posterior division by 2 roots, commonly described as "superior" and "inferior," which encircle the middle meningeal artery before uniting to form a single trunk. After fusion of both roots at approximately 1 to 2 cm posterior to the mandibular nerve, the auriculotemporal nerve courses posterior to the lateral pterygoid muscle and passes between the sphenomandibular ligament and the neck of the mandible.
The auriculotemporal nerve ascends through the parotid region in close relation to the neck of the mandible and the TMJ. Close association with the superficial temporal vessels is maintained as the nerve continues superiorly into the temporal region. Communication with branches of the facial nerve (cranial nerve VII) may occur along the course of the auriculotemporal nerve.
The superior root of the auriculotemporal nerve contains general somatic afferent fibers that provide sensation to portions of the auricle, the EAM, the TMJ, and the temporal scalp. Sensory fibers have cell bodies located in the trigeminal ganglion and project centrally to the trigeminal sensory nuclei in the brainstem.
The inferior root carries postganglionic parasympathetic secretomotor fibers from the otic ganglion to the parotid gland. Preganglionic parasympathetic fibers originate from the inferior salivatory nucleus in the brainstem, travel with the glossopharyngeal nerve (cranial nerve IX) via the tympanic branch to the tympanic plexus, continue as the lesser petrosal nerve, and synapse in the otic ganglion. Postganglionic fibers then accompany the auriculotemporal nerve en route to the parotid gland.
Embryology
The auriculotemporal nerve is a branch of the mandibular division of the trigeminal nerve and is associated with the 1st pharyngeal arch. The auriculotemporal nerve also carries postganglionic parasympathetic fibers to the parotid gland. These fibers arise from the glossopharyngeal nerve, associated with the 3rd pharyngeal arch, synapse in the otic ganglion, and then join the auriculotemporal nerve (see Image. Mandibular Development in a Human Embryo).
Nerves
The 5 main branches of the auriculotemporal nerve are the anterior auricular, articular, parotid, superficial temporal, and EAM branches. The anterior auricular branch provides somatosensory innervation to the skin of the ear, including the tragus and part of the helix. The articular branch provides somatosensory innervation to the posterior aspect of the TMJ.
The parotid branch carries postganglionic fibers arising from the glossopharyngeal nerve via the tympanic plexus and lesser petrosal nerve after synapsing in the otic ganglion. This branch provides secretomotor parasympathetic innervation and vasomotor sympathetic innervation to the parotid gland. The superficial temporal branches course posterior to the superficial temporal artery and provide somatosensory innervation to the skin over the temporal region. Communication with the facial nerve and the zygomaticotemporal nerve, a branch of the maxillary division of the trigeminal nerve (cranial nerve V2), may occur (see Image. Maxillary and Mandibular Nerve Distribution). The branch to the EAM provides somatosensory innervation to the skin of the meatus and part of the tympanic membrane.
Physiologic Variants
The most common variant of the auriculotemporal nerve is observed in its root pattern arising from the mandibular nerve. Although the auriculotemporal nerve most often has 2 roots, the literature describes variations in both the number and location of these roots. Two reports of cadaveric dissections described multiple branching patterns, with findings demonstrating as few as 1 and as many as 4 roots arising from the mandibular nerve.[1][2]
Surgical Considerations
Surgical consideration is required in multiple procedures due to the complex course of the auriculotemporal nerve (see Image. Superficial Neurovascular Structures of the Temporal Region). During TMJ surgery, the auriculotemporal nerve is vulnerable to injury as it courses 10 to 13 mm inferior to the superior edge of the mandibular condyle.[3][4] Injury during surgical intervention may result in pain or paresthesia affecting all terminal branches distal to the lesion (see Nerves). Parotidectomy is another procedure in which preservation of the auriculotemporal nerve is essential. Following this procedure, parasympathetic secretomotor fibers previously innervating the parotid gland may be damaged and undergo aberrant regeneration to sweat glands and cutaneous blood vessels in the overlying skin, resulting in Frey syndrome (see Clinical Significance).[5]
Clinical Significance
Various conditions can affect auriculotemporal nerve function.[6] Selected disorders are discussed below.
Neuralgia of the auriculotemporal nerve presents as throbbing unilateral pain in any of its terminal distribution areas, including the TMJ, scalp, EAM, auricle, and parotid region. Neuralgia may arise from compression of the nerve, particularly by the lateral pterygoid muscle during mastication. The condition is uncommon, with an incidence of approximately 0.4%. Diagnosis may be challenging due to nonspecific symptomatology and a broad differential diagnosis, including cervicalgia, TMJ disease, migraine, hemicrania continua, otitis, trigeminal neuralgia, atypical facial pain, temporal arteritis, and odontalgia. Diagnostic confirmation may be achieved by nerve blockade with complete resolution of symptoms.[7][8] Botulinum toxin injection may provide symptomatic relief.[9]
The auriculotemporal nerve is vulnerable during surgical procedures due to its close anatomic relationships with the parotid gland, TMJ, EAM, and middle meningeal artery. Injury may result in temporal pain, neuralgia, paresthesia, and reduced secretomotor function to the parotid gland.
Frey syndrome, also referred to as "auriculotemporal syndrome," "Baillarger syndrome," "Dupuy syndrome," or "gustatory hyperhidrosis," is named after Jules Baillarger, who first described the manifestations, and Lucia Frey, who systematized the condition. Frey syndrome presents as unilateral sweating of the cheek and external ear, accompanied by erythema following eating or drinking. Gustatory stimulation is not always required for symptom onset. Frey syndrome may also occur in response to olfactory or cognitive stimuli, including thinking about, seeing, or dreaming about food that induces salivation.
Frey syndrome results from injury to the auriculotemporal nerve, in which damaged parasympathetic fibers undergo aberrant regeneration to innervate sweat glands and cutaneous blood vessels in the overlying skin. Frey syndrome most commonly occurs secondary to parotid surgery, parotid gland infection, or facial trauma, and is the most frequent adverse effect following parotidectomy.[10][11]
Differentiation from primary or secondary hyperhidrosis, emotional sweating, pediatric food allergy, and Bogorad syndrome (crocodile tears syndrome) is required. Diagnosis relies primarily on clinical presentation and a history of prior trauma or surgery involving the parotid or auriculotemporal region. The Minor starch–iodine test may be performed when diagnostic confirmation is required. This test involves the application of iodine followed by starch to the skin, with sweating producing a characteristic blue discoloration. Treatment options include botulinum toxin injection and topical aluminum chloride. Intraoperative flaps and implants may reduce the risk of aberrant reinnervation and subsequent symptom development.
Perineural tumor spread along the auriculotemporal nerve may extend cranially through the foramen ovale to the skull base. Extension to the skull base may produce trigeminal pain or palsy and involve adjacent infratemporal and vascular structures.
First bite syndrome is an important postoperative complication of deep parotid lobe surgery. The condition is characterized by severe cramping pain in the parotid region during the first bite of each meal, with symptoms typically diminishing as the meal progresses. First bite syndrome is thought to result primarily from damage to postganglionic sympathetic fibers, leading to relative parasympathetic overactivity and exaggerated myoepithelial contraction, rather than isolated auriculotemporal nerve injury.
Auriculotemporal nerve involvement in parotid malignancy is relatively uncommon but is likely underrecognized. Reported manifestations include periauricular pain, facial weakness, and local tumor recurrence.
Media
(Click Image to Enlarge)
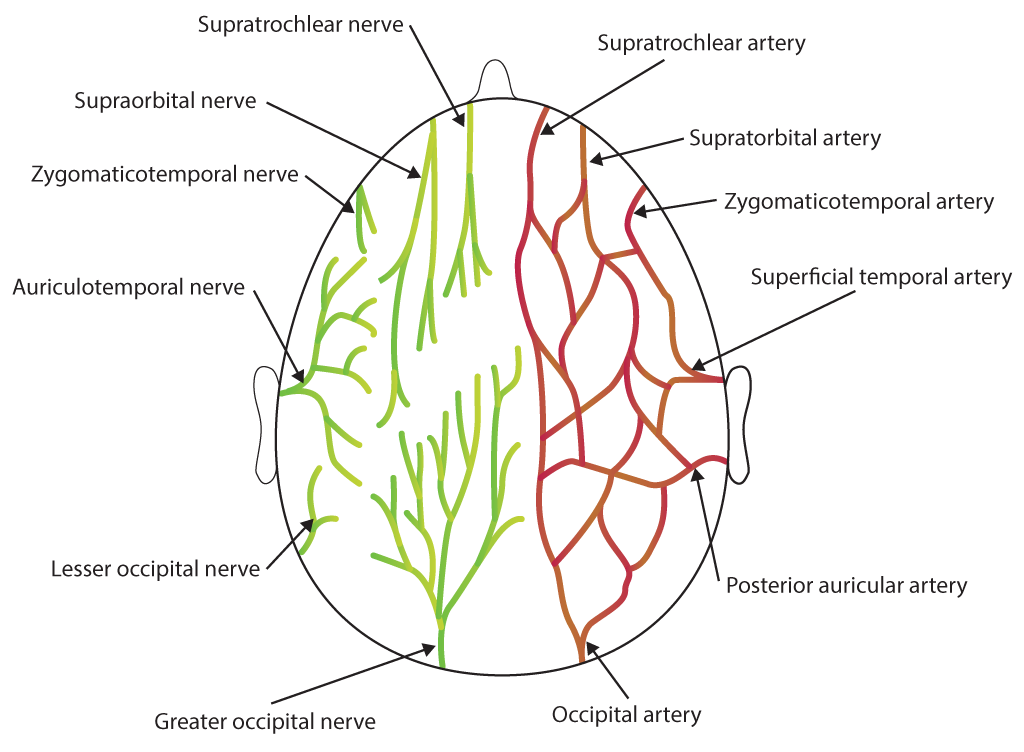
Scalp Nerves and Arteries. This illustration depicts the superior view of the scalp's neurovascular network. The image identifies the supratrochlear, supraorbital, zygomaticotemporal, auriculotemporal, lesser occipital, and greater occipital nerves alongside their corresponding arterial pathways.
Contributed by B Parker
(Click Image to Enlarge)
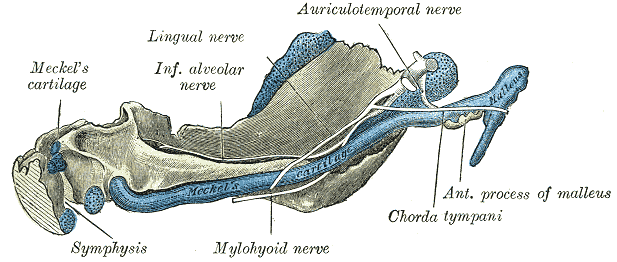
Mandibular Development in a Human Embryo. This anatomical drawing illustrates the inner aspect of a 95-mm human embryo mandible. The image highlights the prominence of the Meckel cartilage and the distribution of the lingual, inferior alveolar, mylohyoid, and auriculotemporal nerves, as well as the chorda tympani and the malleus.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
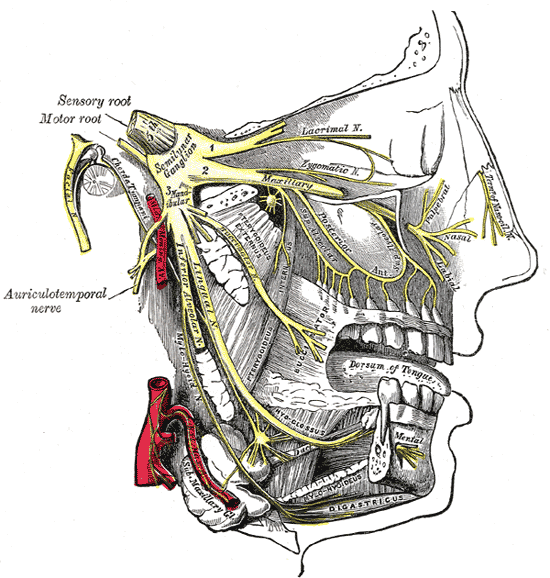
Maxillary and Mandibular Nerve Distribution. This image illustrates the trigeminal nerve and its 3 divisions, originating from the semilunar ganglion. The ophthalmic division gives rise to the lacrimal nerve and nasal branches of the nasociliary nerve. The maxillary division branches into the zygomatic nerves and terminates as the infraorbital nerve, with the associated pterygopalatine (sphenopalatine) ganglion. The mandibular division gives rise to the auriculotemporal, lingual, and inferior alveolar nerves, with the latter continuing as the mental nerve. The otic ganglion near the medial pterygoid and the submandibular ganglion hanging from the lingual nerve are also shown. The image additionally identifies the nerve to the mylohyoid and the digastric muscles.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
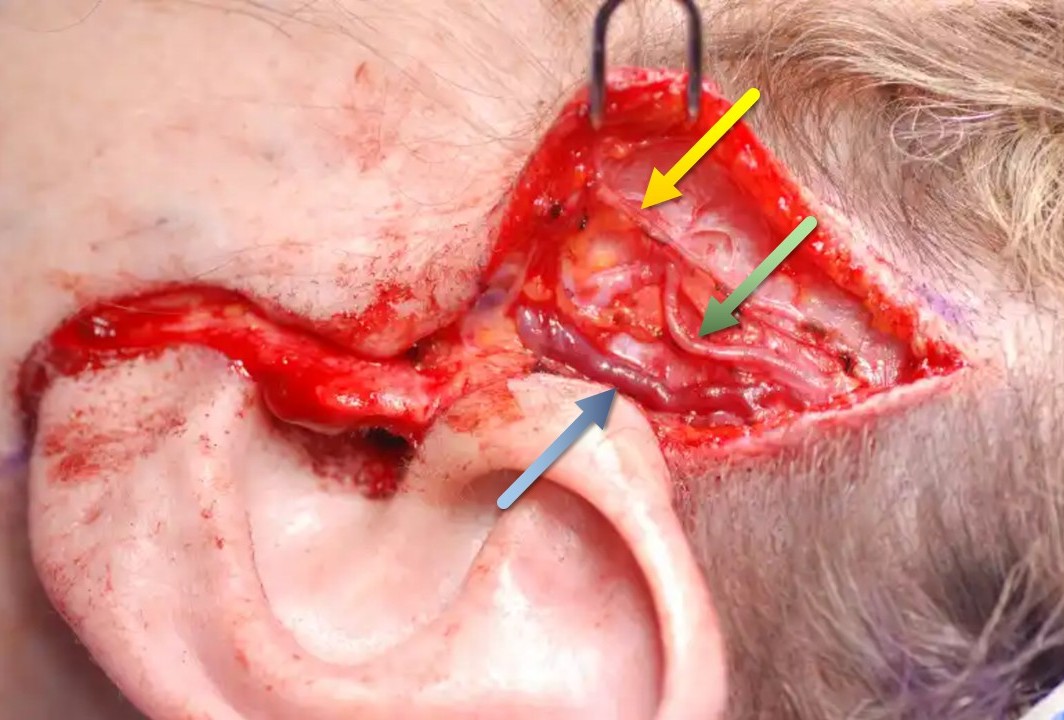
Superficial Neurovascular Structures of the Temporal Region. This intraoperative photograph displays the anatomical landmarks of the temple during surgical exposure. The green arrow indicates the superficial temporal artery, the blue arrow points to the superficial temporal vein, and the yellow arrow identifies the auriculotemporal nerve.
Contributed by Marc H Hohman, MD, FACS
References
Gülekon N, Anil A, Poyraz A, Peker T, Turgut HB, Karaköse M. Variations in the anatomy of the auriculotemporal nerve. Clinical anatomy (New York, N.Y.). 2005 Jan:18(1):15-22 [PubMed PMID: 15597375]
Dias GJ, Koh JM, Cornwall J. The origin of the auriculotemporal nerve and its relationship to the middle meningeal artery. Anatomical science international. 2015 Sep:90(4):216-21. doi: 10.1007/s12565-014-0247-9. Epub 2014 Jun 28 [PubMed PMID: 24973088]
Fernandes PR, de Vasconsellos HA, Okeson JP, Bastos RL, Maia ML. The anatomical relationship between the position of the auriculotemporal nerve and mandibular condyle. Cranio : the journal of craniomandibular practice. 2003 Jul:21(3):165-71 [PubMed PMID: 12889671]
Rodriguez-Lopez MJ, Fernandez-Baena M, Aldaya-Valverde C. Management of pain secondary to temporomandibular joint syndrome with peripheral nerve stimulation. Pain physician. 2015 Mar-Apr:18(2):E229-36 [PubMed PMID: 25794224]
Henry N, Baker BG, Iyer S. Frey's syndrome following a facial burn treated with botulinum toxin. Annals of burns and fire disasters. 2018 Mar 31:31(1):47-48 [PubMed PMID: 30174572]
Kadrie A, Toomey P, Callaway J, Gillespie MB, Boughter JD Jr. The Auriculotemporal Nerve: A Comprehensive Review of Its Anatomical Variation and Clinical Manifestations. Laryngoscope investigative otolaryngology. 2025 Aug:10(4):e70238. doi: 10.1002/lio2.70238. Epub 2025 Aug 15 [PubMed PMID: 40822616]
Stuginski-Barbosa J, Murayama RA, Conti PC, Speciali JG. Refractory facial pain attributed to auriculotemporal neuralgia. The journal of headache and pain. 2012 Jul:13(5):415-7. doi: 10.1007/s10194-012-0439-4. Epub 2012 Mar 30 [PubMed PMID: 22460942]
Level 3 (low-level) evidenceKravchik L, Ng M, Hsu NM, VanHoy TB. Peripheral Nerve Block of the External Ear. StatPearls. 2026 Jan:(): [PubMed PMID: 30860741]
Wilhour D, Nahas SJ. The Neuralgias. Current neurology and neuroscience reports. 2018 Aug 16:18(10):69. doi: 10.1007/s11910-018-0880-0. Epub 2018 Aug 16 [PubMed PMID: 30116913]
Freni F, Gazia F, Stagno d'Alcontres F, Galletti B, Galletti F. Use of botulinum toxin in Frey's syndrome. Clinical case reports. 2019 Mar:7(3):482-485. doi: 10.1002/ccr3.2019. Epub 2019 Jan 31 [PubMed PMID: 30899477]
Level 3 (low-level) evidenceDulguerov P, Quinodoz D, Cosendai G, Piletta P, Marchal F, Lehmann W. Prevention of Frey syndrome during parotidectomy. Archives of otolaryngology--head & neck surgery. 1999 Aug:125(8):833-9 [PubMed PMID: 10448728]
Level 1 (high-level) evidence