Introduction
The heart is the first functional organ to develop in the human embryo. By the end of the fourth week of development, the heart can beat spontaneously. Development of the atrioventricular septum begins during the third week. Improper development of the atrioventricular septum can result in abnormalities that affect the heart's normal physiology. These defects can range in severity.[1][2][3]
Development
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Development
The developing heart undergoes many processes as it transforms from a primitive tube into a functional organ. During embryonic development, the heart progresses through several stages before becoming functional. Around day 18 after fertilization, the primitive heart begins to develop from 2 bilateral tubes within the immature, disk-shaped embryo. As the embryo folds, the 2 tubes fuse in the midline, forming a single heart tube. The primitive atria and ventricles are positioned between the sinus venosus and the bulbus cordis. During the fourth week of development, the heart tube begins to loop, forming a shape that more closely resembles the adult heart.
The major septa of the heart form between days 27 and 37 of development. Around this time, endocardial cushions form through extracellular matrix deposition and cellular proliferation and migration. The cellular composition of the cushions depends on their location in the heart. For example, the atrioventricular cushions are derived from adjacent endocardial cells, whereas the conotruncal cushions are derived from neural crest cells. The atrioventricular endocardial cushions form along the ventral and dorsal borders of the atrioventricular canal. The primitive atrioventricular canal initially communicates only with the primitive left ventricle, and a bulboventricular flange separates it from the bulbus cordis. Over time, the posterior flange shrinks and becomes less prominent. The atrioventricular canal enlarges to the right, allowing blood flow to both primitive right and left ventricles. The dorsal and ventral endocardial cushions, along with 2 lateral atrioventricular cushions, grow and eventually fuse to form a septum that divides the right and left atrioventricular canals.
Endocardial cushions involved in the development of the atrioventricular canal also contribute to the development of the interventricular septum and the closure of the ostium primum. The resulting anatomy has a cross-like appearance. Visualization of this cross-like appearance on ultrasonography is crucial for confirming cardiac integrity during pregnancy. Endocardial cushion development is also crucial for the formation of the atrial and ventricular septa, atrioventricular canals and valves, and the aortic and pulmonary outflow tracts. Failure of fusion can result in several congenital cardiac anomalies.
The septum primum forms within the primitive atrium and separates the right atrium from the left atrium. This septum extends inferiorly toward the endocardial cushions. A space in this septum, known as the foramen primum, maintains blood flow within the heart. As the foramen primum decreases in size, the foramen secundum forms. The septum secundum forms to the right of the septum primum and eventually expands to cover most of the foramen secundum. The remaining opening persists as the foramen ovale in the fetus to maintain a right-to-left shunt. The atrial septum then forms through fusion of the septum primum and septum secundum. A flap covering the foramen ovale develops from the septum primum. Shortly after birth, increased left atrial pressure causes the flap to close. A patent foramen ovale can persist if the septa fail to fuse.By the end of the fourth week, the ventricular septum also begins to form. The 2 primitive ventricles begin to expand through continuous growth of the myocardium externally and formation of trabeculae internally. Over time, the medial walls of the ventricles fuse, forming a muscular interventricular septum. The interventricular foramen remains superior to this septum. Next, the aorticopulmonary septum rotates and fuses with the muscular interventricular septum, together forming the membranous portion of the interventricular septum.[4][5][6]
Clinical Significance
Atrioventricular septal defects (AVSDs) account for 4% to 5% of all congenital heart defects and approximately 0.5% of live births. AVSDs are strongly associated with trisomy 21. Nonsyndromic atrioventricular canal defects appear to be associated with maternal diabetes and obesity.[7][8][9]
AVSDs occur when the endocardial cushions fail to fuse adequately with the central portion of the atrial septum and the muscular portion of the ventricular septum. Two common types of AVSDs exist: complete and partial. Approximately half of these atrioventricular canal defects are complete defects involving both atrial and ventricular septal defects with a common atrioventricular valve.
Atrial septal defects, which occur in approximately 6.5 per 10,000 births, are congenital heart abnormalities that may result from an ostium secundum defect. This defect results in an abnormal opening between the left and right atria. Proposed mechanisms include insufficient formation of the septum secundum and excessive cell death and resorption of the septum primum. Other rare and serious abnormalities include cor triloculare biventriculare (common atrium) and cor triloculare biatrium. Cor triloculare biventriculare is defined as a complete absence of the atrial septum and is the more common of the 2. Cor triloculare biatrium is the complete absence of the ventricular septum.
Failure of the atrioventricular septum to fuse with the septum primum of the atria causes the foramen primum to remain open, resulting in a foramen primum defect. Generally, this defect occurs with a malformation of the mitral valve. When the ventral and dorsal endocardial cushions fail to fuse, a large opening develops in the center of the heart. This defect is called a persistent common atrioventricular canal. This malformation results in the tricuspid and mitral valves forming a single common atrioventricular valve. The defect causes left-to-right shunting at the atrial level, resulting in enlargement of the right atrium and right ventricle.Ebstein anomaly occurs when the posterior and septal leaflets of the tricuspid valve fail to attach normally, displacing the leaflets into the right ventricle. This displacement causes atrialization of a portion of the right ventricle.
Media
(Click Image to Enlarge)
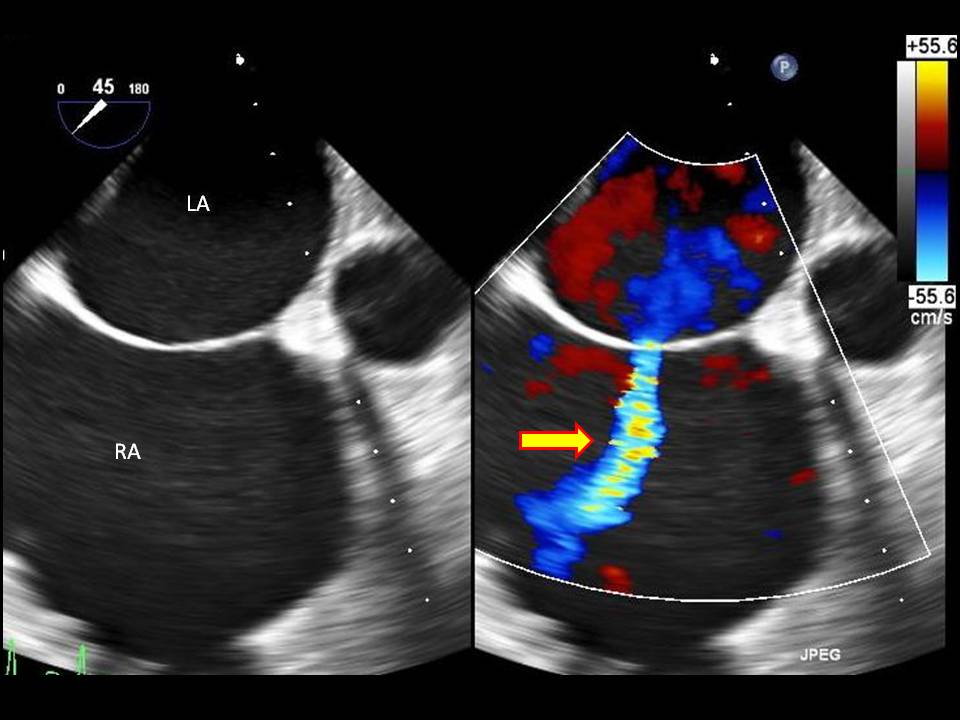
Atrial Septal Defect on Ultrasound with Doppler Study. This transesophageal echocardiography image shows a secundum atrial septal defect, with color Doppler indicating a left-to-right shunt flow (arrow) across the interatrial septum.
Contributed by Amgad Makaryus, M.D.
References
Anderson RH, Spicer DE, Mohun TJ, Hikspoors JPJM, Lamers WH. Remodeling of the Embryonic Interventricular Communication in Regard to the Description and Classification of Ventricular Septal Defects. Anatomical record (Hoboken, N.J. : 2007). 2019 Jan:302(1):19-31. doi: 10.1002/ar.24020. Epub 2018 Nov 29 [PubMed PMID: 30408340]
Kohnken R, Schober K, Godman J, Gardner A, Jenkins T, Schroeder E, Baker P, Dunbar L. Double outlet right ventricle with subpulmonary ventricular septal defect (Taussig-Bing anomaly) and other complex congenital cardiac malformations in an American Quarter Horse foal. Journal of veterinary cardiology : the official journal of the European Society of Veterinary Cardiology. 2018 Feb:20(1):64-72. doi: 10.1016/j.jvc.2017.10.005. Epub 2017 Nov 22 [PubMed PMID: 29174590]
Gopalakrishnan A, Sasidharan B, Tharakan J, Valaparambil A. Left atrial outflow obstruction in double-outlet right atrium. Asian cardiovascular & thoracic annals. 2018 Jan:26(1):50-53. doi: 10.1177/0218492317736962. Epub 2017 Oct 8 [PubMed PMID: 28988491]
Saremi F, Sánchez-Quintana D, Mori S, Muresian H, Spicer DE, Hassani C, Anderson RH. Fibrous Skeleton of the Heart: Anatomic Overview and Evaluation of Pathologic Conditions with CT and MR Imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 2017 Sep-Oct:37(5):1330-1351. doi: 10.1148/rg.2017170004. Epub 2017 Aug 18 [PubMed PMID: 28820653]
Level 3 (low-level) evidencePatrick WL, Mainwaring RD, Reinhartz O, Punn R, Tacy T, Hanley FL. Major Aortopulmonary Collateral Arteries With Anatomy Other Than Pulmonary Atresia/Ventricular Septal Defect. The Annals of thoracic surgery. 2017 Sep:104(3):907-916. doi: 10.1016/j.athoracsur.2017.02.029. Epub 2017 May 17 [PubMed PMID: 28527961]
Jensen B, Spicer DE, Sheppard MN, Anderson RH. Development of the atrial septum in relation to postnatal anatomy and interatrial communications. Heart (British Cardiac Society). 2017 Mar:103(6):456-462. doi: 10.1136/heartjnl-2016-310660. Epub 2016 Dec 21 [PubMed PMID: 28003417]
Anderson RH, Mohun TJ, Brown NA. Clarifying the morphology of the ostium primum defect. Journal of anatomy. 2015 Mar:226(3):244-57. doi: 10.1111/joa.12272. Epub 2015 Feb 9 [PubMed PMID: 25676858]
Level 3 (low-level) evidenceAnderson RH, Spicer DE, Brown NA, Mohun TJ. The development of septation in the four-chambered heart. Anatomical record (Hoboken, N.J. : 2007). 2014 Aug:297(8):1414-29. doi: 10.1002/ar.22949. Epub 2014 May 27 [PubMed PMID: 24863187]
Level 3 (low-level) evidenceTardy MM, Galvaing G, Sakka L, Garcier JM, Chazal J, Filaire M. [Embryology of the heart walls]. Morphologie : bulletin de l'Association des anatomistes. 2013 Mar:97(316):2-11. doi: 10.1016/j.morpho.2012.11.001. Epub 2013 Feb 12 [PubMed PMID: 23414788]
Level 3 (low-level) evidence