 Anatomy, Shoulder and Upper Limb, Acromioclavicular Joint
Anatomy, Shoulder and Upper Limb, Acromioclavicular Joint
Introduction
The acromioclavicular joint (ACJ) is an articulation between the lateral end of the clavicle and the acromion of the scapula, as the acromion projects anteriorly. This joint provides stability and motion to the shoulder complex. The ACJ is a commonly injured shoulder joint, with pathology ranging from sprains to frank tears, occasionally requiring surgical management.[1] The coracoclavicular ligament (CCL) serves as the primary support structure of the ACJ (see Image. Ligaments and Osseous Landmarks of the Human Shoulder). Stabilization of the ACJ results from the coordinated function of the 2 ligaments. The ACJ is a synovial planar joint that contributes to the stabilization of the shoulder girdle.[2] CCL injuries are commonly associated with acromioclavicular separations, particularly in high-impact sports or trauma. Surgical intervention may be necessary in cases of severe CCL injury. Understanding the anatomy and function of the CCL is essential for the management of various conditions affecting the shoulder.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The ACJ is a diarthrodial articulation defined by the lateral clavicle and the acromion process of the scapula, as the acromion projects anteriorly. The ACJ is a planar synovial joint that permits primarily gliding motion under normal physiological conditions. As a component of the scapulothoracic linkage, the ACJ contributes to scapular mobility and facilitates upper limb movements, including shoulder abduction and flexion. Force transmission from the upper limb to the axial skeleton also occurs through this articulation.
The ACJ is enclosed by a fibrous capsule and lined by synovial membrane. An intra-articular fibrocartilaginous disk is interposed between the osseous components. Articulating surfaces are covered by fibrocartilage rather than hyaline cartilage. Three principal ligamentous structures stabilize the ACJ: the acromioclavicular ligament, the CCL complex, and the coracoacromial ligament.
The acromioclavicular ligament consists of superior, inferior, anterior, and posterior components, with superior and posterior portions providing the greatest mechanical strength. The primary function of this ligament is horizontal stability.
The CCL serves as the primary extrinsic stabilizer of the ACJ. The CCL connects the coracoid process of the scapula to the inferior aspect of the lateral 1/3 of the clavicle and is composed of the conoid and trapezoid ligaments. These components insert onto the posteromedial and anterolateral regions of the undersurface of the distal clavicle, respectively.[3][4]
The trapezoid ligament inserts approximately 3 cm from the distal clavicle, whereas the conoid ligament inserts approximately 4.5 cm from the distal clavicle. Inferiorly, both ligaments are continuous at the coracoid attachment but diverge superiorly to their respective clavicular insertions. A bursa frequently separates the conoid and trapezoid ligaments. The conoid ligament attaches to the conoid tubercle of the clavicle, posteromedial to the trapezoid tubercle. A conical configuration characterizes the conoid ligament, with a broad superior clavicular attachment and a narrower inferior coracoid attachment. The ligament courses posteromedially toward the root of the coracoid process.
The trapezoid ligament lies anterolateral to the conoid ligament. A quadrilateral configuration characterizes the trapezoid ligament, which has reduced thickness compared with the conoid ligament. Attachment occurs to the trapezoid line on the inferior clavicular surface and to the posterosuperior aspect of the coracoid process, where contact occurs along the anterior margin of the conoid ligament. The trapezoid ligament courses anterolaterally, whereas the conoid ligament assumes a near-vertical orientation.
The ACJ functions as a synovial plane joint contributing to the stabilization of the shoulder girdle.[5] Primary stabilization arises from the intrinsic acromioclavicular ligament and the extrinsic CCL. The CCL does not directly traverse the ACJ but maintains the spatial relationship between the clavicle and the acromion. CCL injuries are frequently associated with acromioclavicular separations, particularly in high-impact trauma and contact sports. Surgical intervention may be required in severe CCL injury. Understanding of CCL anatomy and function is essential for the management of ACJ-related pathology.
Blood Supply and Lymphatics
Branches of the suprascapular artery, arising from the subclavian artery, and branches of the thoracoacromial artery, arising from the axillary artery, constitute the 2 principal vascular sources supplying the ACJ. The primary vascular supply to the CCL is derived from 2 arterial systems. The suprascapular artery originates from the subclavian artery via the thyrocervical trunk. The thoracoacromial branch originates from the axillary artery. Venous drainage of the region associated with the CCL is mediated by the suprascapular vein, which drains toward the external jugular vein. Lymphatic drainage from the CCL region proceeds to the axillary and cervical lymphatic basins.
Nerves
Joint innervation follows the Hilton law, which states that joints receive articular branches from nerves supplying the muscles acting across the joint. The ACJ receives innervation from articular branches of the suprascapular, axillary, and lateral pectoral nerves. These nerves originate from the brachial plexus. Cutaneous sensory supply to the ACJ is provided by a sensory branch of the suprascapular nerve. This branch courses superiorly to the supraspinatus muscle toward the acromioclavicular region. Pain originating from the ACJ may be referred to the neck, trapezius region, lateral deltoid, and shoulder. The CCL region receives innervation from brachial plexus branches, specifically articular branches of the suprascapular, axillary, and lateral pectoral nerves.
Muscles
Various muscles contribute to the movement and stabilization of the shoulder girdle. The CCL supports the coracoclavicular articulation during complex shoulder movements, limiting separation between the scapula and clavicle. The muscles primarily involved in the movement of these structures include the serratus anterior, trapezius, teres major, rhomboid major, rhomboid minor, and the long head of the triceps brachii. Direct scapular attachments of these muscles contribute to mechanical stabilization and restriction of excessive motion at the coracoclavicular complex. The pectoralis minor tendon crosses the fascial arch formed by the medial CCL at the level of the coracoid process.
Physiologic Variants
A 2021 study reported that CCL variation may include replacement of the ligament by a coracoclavicular bone bridge.[6] The study identified this anomaly in 9% of 2,724 subjects, with higher prevalence among African American individuals and women. Reported frequencies of the coracoclavicular joint (CCJ) vary widely across studies. A 2023 radiographic study comparing the prevalence of CCJs in a French population with skeletal remains from medieval periods reported a prevalence of 0.82%.[7] Another cadaveric study evaluated 24 CCL specimens to assess anatomical variation. Three variants of the conoid ligament were identified among 18 conoid ligaments examined. Nine conoid ligaments attached to the root of the coracoid process. Six were confluent with the superior transverse scapular ligament. Three demonstrated a distinct fascicle originating from the inferior conoid attachment and inserting onto the lateral aspect of the trapezoid ligament.[8]
Surgical Considerations
Injuries to the ACJ are common and may present as sprains or dislocations. Sprains are the most frequent injury pattern. The most common mechanism involves direct trauma to the ACJ or lateral shoulder impact, producing axial loading across the joint. Potential etiologies include motor vehicle collisions, sports-related injuries, and accidental trauma. Falls onto an outstretched hand or elbow may also result in ACJ injury. ACJ injuries account for more than 40% of all shoulder injuries. ACJ dislocation is distinct from “shoulder dislocation,” which refers to glenohumeral joint dislocation.[9]
Clinical presentation typically includes pain localized to the ACJ with a mechanism consistent with injury. Pain may radiate to the shoulder or neck and is commonly exacerbated by arm movement or use. Physical examination findings may include swelling, ecchymosis, or visible deformity. Localized tenderness to palpation is common. Active and passive range of motion of the shoulder or neck may be reduced. Assessment of anterior-posterior and superior-inferior mobility is required to evaluate laxity. Gross deformity may be evident in cases of dislocation.
Evaluation should include assessment of the entire clavicle and shoulder region for associated injuries, in addition to a complete neurovascular examination. Special tests assist in the evaluation of suspected ACJ injury. Pain reproduction during testing suggests ACJ pathology. The adduction (cross-arm) test is performed by active or passive adduction of the arm across the body in the axial plane. Pain at the ACJ indicates a positive finding and is the most sensitive maneuver for ACJ pathology. The shear test is performed by applying opposing anterior and posterior forces to the clavicle and scapula. The Paxinos test (1-handed shear test) is performed by placing the thumb on the posterior acromion and fingers on the midclavicle, followed by compression of the 2 points.
Radiographic evaluation is standard in suspected ACJ injury or in cases of undifferentiated shoulder pain following trauma. Standard imaging includes anteroposterior, lateral, and axillary radiographs. The Zanca view provides the most accurate assessment of the ACJ when diagnostic uncertainty persists. This projection consists of an anteroposterior view with 10° of cephalic tilt centered on the ACJ. Grade I ACJ sprain, the most common injury pattern, typically demonstrates normal radiographic findings. Grades II through VI demonstrate varying degrees of joint disruption.
Further evaluation with ultrasound or magnetic resonance imaging may be indicated when diagnostic uncertainty persists. ACJ dislocations are classified using the Rockwood classification of acromioclavicular and coracoclavicular injuries, as follows:
- Grade I: Acromioclavicular ligament sprain; CCL intact; no radiographic abnormalities
- Grade II: Acromioclavicular ligament torn; CCL sprain; clavicle elevated but not superior to the acromion border, or less than 25% increase in coracoclavicular interspace
- Grade III: Acromioclavicular ligament and CCL torn; clavicle elevated above the acromion border, or 25% to 100% increase in coracoclavicular interspace
- Grade IV: Acromioclavicular ligament and CCL torn; posterior displacement of the distal clavicle into the trapezius
- Grade V: Acromioclavicular ligament and CCL torn; superior displacement of the distal clavicle greater than 25 mm
- Grade VI: Acromioclavicular ligament and CCL torn; inferolateral displacement into a subacromial or subcoracoid position posterior to the coracobrachialis or biceps tendon
The prognosis of ACJ dislocations is generally favorable. Grades I and II injuries are self-limited and managed with conservative therapy, including a brief period of rest, sling immobilization, ice application, anti-inflammatory medication intake, physical therapy, and a progressive return to activity. Management of grade III dislocations remains controversial. Treatment selection depends on the patient's occupation, functional demands, goals, and orthopedic surgical consultation. Grades IV to VI injuries are rare and typically require surgical correction due to associated instability and risk of concomitant injuries. Surgically managed ACJ injuries are associated with longer recovery periods and higher complication rates.
The most common complication following ACJ injury is persistent pain, reported in approximately 30% to 50% of cases. Primary and secondary osteoarthritis frequently develop in the ACJ. Incidence of ACJ osteoarthritis increases with age. Degenerative changes may occur secondary to overuse, chronic degeneration, or prior trauma. Secondary osteoarthritis leads to narrowing of the articular disc and worsening cartilage degeneration. Progression of osteoarthritis may result in osteophytic formation, subacromial impingement, and compression of adjacent structures.[10]
Clinical Significance
Septic Arthritis of the Acromioclavicular Joint
ACJ septic arthritis can result in significant morbidity and mortality. Confusion with septic glenohumeral joint arthritis is common due to an overlapping clinical presentation. Pain and erythema over the ACJ are characteristic findings.[11]
ACJ septic arthritis is rare and predominantly affects immunocompromised individuals and men in the 5th and 6th decades of life. Septic arthritis most commonly results from hematogenous bacterial dissemination to the affected joint. Consequently, joints with higher vascularity demonstrate increased susceptibility to infection. The most commonly affected joints include the knee, hip, shoulder, ankle, and foot. By comparison, ACJ septic arthritis remains uncommon due to limited vascularity and small joint size.[12]
ACJ septic arthritis has been reported in a 69-year-old man with Klinefelter syndrome, presenting with shoulder pain and septic arthritis. Metabolic syndrome, including obesity, hypercholesterolemia, hypertension, and impaired glucose tolerance, is associated with increased risk of ACJ pathology.
Microbial pathogens associated with ACJ septic arthritis include Staphylococcus aureus, Cryptococcus neoformans, and Haemophilus influenzae. Osteomyelitis may occur as a complication of surgical reconstruction following ACJ injury. Poor hygiene and nonadherence to postoperative wound care protocols are potential risk factors. Management typically requires intravenous antibiotic therapy and, in many cases, surgical exploration.[13]
Coracoclavicular Joint Osteoarthritis
The CCJ is a rare anatomical entity. Degeneration of the CCL within this joint is even less common. When present, the condition may result in shoulder pain or discomfort. Diagnosis is often challenging due to limited clinician awareness, which may contribute to delayed treatment. Imaging modalities such as standing radiographs and dynamic magnetic resonance imaging may assist in the visualization of a symptomatic CCJ. Symptomatic CCJ may be differentiated from subcoracoid impingement using local anesthetic injection. Nonoperative management includes anti-inflammatory medication administration, physiotherapy, and corticosteroid injections. Surgical excision is reserved for cases refractory to conservative therapy. In addition to limiting shoulder movement and producing pain, the presence of a CCJ has been reported to exacerbate thoracic outlet syndrome in some individuals.
Media
(Click Image to Enlarge)
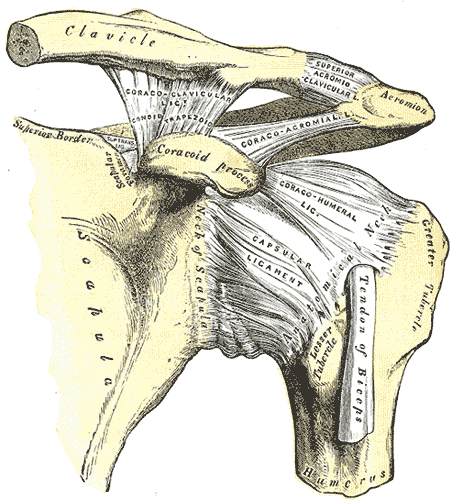
Ligaments and Osseous Landmarks of the Human Shoulder. The image displays the proximal humerus with its anatomical neck and tubercles alongside the scapular neck and superior border. Labeled connective tissues include the coracoacromial, coracohumeral, and capsular ligaments, as well as the superior transverse ligament bridging the scapular notch. The coracoclavicular ligament is further divided into its conoid and trapezoid components. The superior acromioclavicular ligament joins the clavicle to the acromion, while the tendon of the biceps is visible in the intertubercular area.
Henry Vandyke Carter, Public Domain, Via Wikimedia Commons
References
Fraipont GM, Beyer RS, McGarry MH, Lee TQ. Acromioclavicular joint biomechanics: a systematic review. JSES reviews, reports, and techniques. 2024 Nov:4(4):668-675. doi: 10.1016/j.xrrt.2024.06.009. Epub 2024 Jul 20 [PubMed PMID: 39474188]
Level 1 (high-level) evidenceKibler WB, Sciascia A. Acromioclavicular joint injuries revisited: Pathoanatomy, pathomechanics, and clinical presentation. Shoulder & elbow. 2022 Oct:14(5):470-480. doi: 10.1177/17585732221122335. Epub 2022 Sep 1 [PubMed PMID: 36199503]
Kurata S, Inoue K, Hasegawa H, Shimizu T, Iida A, Kawamura K, Omokawa S, Mahakkanukrauh P, Tanaka Y. The Role of the Acromioclavicular Ligament in Acromioclavicular Joint Stability: A Cadaveric Biomechanical Study. Orthopaedic journal of sports medicine. 2021 Feb:9(2):2325967120982947. doi: 10.1177/2325967120982947. Epub 2021 Feb 10 [PubMed PMID: 33623800]
Hattori F, Ochiai N, Hashimoto E, Shimada Y, Ise S, Inagaki K, Hiraoka Y, Ohtori S. Effects of acromioclavicular and coracoclavicular ligament stability on acromioclavicular joint dislocation: insights from a cadaveric study. Clinics in shoulder and elbow. 2025 Sep:28(3):274-280. doi: 10.5397/cise.2025.00157. Epub 2025 Jul 2 [PubMed PMID: 40611801]
Graça NNJ, Duarte ML. Coracoclavicular Joint Arthrosis - An Uncommon Cause of Shoulder Pain. Prague medical report. 2024:125(2):158-162. doi: 10.14712/23362936.2024.15. Epub [PubMed PMID: 38761049]
Harlow ER, Sasala LM, Talbot CE, Desai BJ, Ina J, Miskovsky S. Prevalence and Morphology of the Coracoclavicular Joint: An Osteological Study of 2,724 Subjects Using Univariable and Multivariable Logistic Regression Analyses. Frontiers in surgery. 2021:8():761441. doi: 10.3389/fsurg.2021.761441. Epub 2021 Oct 28 [PubMed PMID: 34778366]
Williamson MA. A review of the coracoclavicular joint: Description, etiology, and clinical significance. Clinical anatomy (New York, N.Y.). 2023 Jul:36(5):715-725. doi: 10.1002/ca.24040. Epub 2023 Apr 4 [PubMed PMID: 36942973]
Hyland S, Charlick M, Varacallo MA. Anatomy, Shoulder and Upper Limb, Clavicle. StatPearls. 2026 Jan:(): [PubMed PMID: 30252246]
Abrams R, Akbarnia H. Shoulder Dislocations Overview. StatPearls. 2026 Jan:(): [PubMed PMID: 29083735]
Level 3 (low-level) evidenceCain EL Jr, Parker D. Open Anatomic Coracoclavicular Ligament Reconstruction for Acromioclavicular Joint Injuries. Clinics in sports medicine. 2023 Oct:42(4):589-598. doi: 10.1016/j.csm.2023.05.009. Epub 2023 Jul 3 [PubMed PMID: 37716723]
Thomas J, Daud M, Macmull S. Acute septic arthritis of the acromioclavicular joint caused by Staphylococcus aureus with marked soft tissue collection towards posterior medial aspect of the AC joint: A rare clinical presentation. IDCases. 2022:29():e01513. doi: 10.1016/j.idcr.2022.e01513. Epub 2022 May 24 [PubMed PMID: 35663610]
Level 3 (low-level) evidenceRamanan A, Balasubramanian V, C R, Sami P. Isolated Acromioclavicular Joint Septic Arthritis: A Case Report and Review of Literature. Cureus. 2024 Jul:16(7):e63590. doi: 10.7759/cureus.63590. Epub 2024 Jul 1 [PubMed PMID: 39087184]
Level 3 (low-level) evidenceOswald A, Alorda A, Tassone M, Walker A, Ganti L. Acromioclavicular Osteomyelitis: When Simple Cellulitis Is No Longer Simple. Orthopedic reviews. 2022:14(3):36909 [PubMed PMID: 35936799]