Introduction
The anal triangle is the posterior portion of the perineum by definition. The perineum is located between the thighs and inferior to the pelvic diaphragm. The perineum consists of the anal triangle and the urogenital triangle. A theoretical line connecting the ischial tuberosities of the pelvis divides the perineum into the posterior anal triangle and the anterior urogenital triangle.
The anal triangle is bounded by the coccyx, the sacrotuberous ligaments, and an imaginary line connecting the ischial tuberosities. The anal triangle contains the anal canal and 2 ischioanal (ischiorectal) fossae, positioned on either side of the anal canal. The region's boundaries include the posterior margin of the perineal membrane anteriorly, the coccyx posteriorly, the sacrotuberous ligaments posterolaterally, and the levator ani muscle superiorly.
The anal triangle has clinical significance in the evaluation and management of hemorrhoids, anal cancer, and perirectal abscesses, which commonly present with pain, bleeding, pruritus, mass effect, or systemic symptoms. From a procedural standpoint, hemorrhoidectomy, Doppler-guided hemorrhoidal artery ligation, stapled hemorrhoidopexy, incision and drainage of abscesses, and oncologic management of anal canal tumors require precise knowledge of regional anatomy, including vascular supply and innervation. Knowledge of anal triangle anatomy and function enables clinicians to interpret symptoms relative to the pectinate line, anticipate differences in pain perception and lymphatic spread, and guide diagnostic evaluation while minimizing iatrogenic complications.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
As stated above, the anal triangle contains the anal canal. The region also contains 2 ischiorectal fossae.
Anal Canal
The anal canal constitutes the hindmost portion of the gastrointestinal system.[1] The anal canal has both an anatomic and a surgical definition. The anatomic anal canal extends from the anal verge to the pectinate (dentate) line. The surgical anal canal is longer and extends from the anal verge to the anorectal line.[2] The anal verge corresponds to the junction between the anoderm and perianal skin.
The pectinate line divides the anal canal into an upper 2/3 and a lower 1/3. Simple columnar epithelium lines the region above the pectinate line, whereas stratified squamous epithelium lines the region below the pectinate line.[3] The anal canal contains anal columns (or columns of Morgagni) and anal valves, representing the inferior ends of the anal columns (see Image. Interior of the Anal Canal and Lower Rectum). Anal sinuses lie superior to the anal valves and contain anal glands that secrete mucus into the anal canal.
Ischiorectal Fossae
The ischiorectal fossae contain the inferior rectal vessels, the inferior rectal nerve, and ischioanal fat, which supports the anal canal and permits expansion of the anal canal during defecation. The pudendal (Alcock) canals lie along the lateral wall of the ischiorectal fossae and contain the pudendal nerve and internal pudendal vessels (see Image. Neurovascular Structures of the Perineal Region).[4] Boundaries of the ischiorectal fossae include the sphincter urethrae muscle and deep transverse perineal muscles anteriorly, the gluteus maximus muscle and sacrotuberous ligament posteriorly, the external anal sphincter and levator ani superomedially, the fascia covering the obturator internus muscle laterally, and the skin forming the floor (see Image. Inferior View of the Male Pelvic Outflow and Perineum).[5]
Embryology
Above the pectinate line, the anal canal derives from the cloaca, which possesses an endodermal lining. Below the pectinate line, the anal canal develops from the proctodeum and is of ectodermal origin. The pectinate line represents the fusion between endoderm and ectoderm.
Convergence of the proctodeal ectoderm with cloacal endoderm forms the cloacal membrane. The urorectal septum partitions the cloaca into the ventral bladder and urogenital sinus and the dorsal rectum and anal canal. The urorectal septum joins the cloacal membrane. The cloacal membrane subsequently divides into an anal membrane and a urogenital membrane.[6]
Blood Supply and Lymphatics
The pectinate line is an important anatomic landmark (see Image. Neurovascular Divisions of the Anal Canal). This line separates regions with distinct patterns of blood supply, lymphatic drainage, and innervation.
Above the pectinate line, the superior rectal artery provides the primary blood supply. The superior rectal artery arises as a branch of the inferior mesenteric artery. Venous drainage above the pectinate line flows into the portal venous system, a distinction that is clinically significant when compared with regions below the pectinate line. The internal hemorrhoidal plexus drains into the superior rectal vein. Blood from the superior rectal vein continues through the inferior mesenteric vein, then the splenic vein, and, ultimately, the portal vein.[7] Lymphatic drainage of the anal canal above the pectinate line primarily follows the superior rectal vessels to the inferior mesenteric (superior rectal) lymph nodes, with additional drainage to the internal iliac lymph nodes.
Below the pectinate line, the inferior rectal arteries and veins supply and drain the muscles and skin surrounding the anus. The inferior rectal vessels arise as branches of the internal pudendal vessels. Venous blood from this region below the pectinate line ultimately drains into the caval venous system. Blood from the external hemorrhoidal plexus drains into the inferior rectal vein. Venous flow continues through the internal pudendal, internal iliac, and common iliac veins, and, finally, into the inferior vena cava. Lymphatic drainage of the perineum below the pectinate line proceeds toward the superficial inguinal lymph nodes.[8]
Nerves
The internal anal sphincter and the anal canal above the pectinate line receive visceral innervation from sympathetic and parasympathetic fibers. Sympathetic fibers derive from the inferior pelvic plexus, whereas parasympathetic fibers arise from the inferior pelvic plexus and pelvic splanchnic nerves.[9]
Below the pectinate line, the anal canal receives somatic innervation via the inferior rectal nerve. The inferior rectal nerve is a branch of the pudendal nerve. The inferior rectal nerve innervates the external anal sphincter and provides sensation to the anal canal extending up to 15 mm above the pectinate line, including pain, touch, and temperature.[10]
Muscles
The obturator internus muscle forms the lateral border of the ischiorectal fossae. The levator ani forms the superior boundary of the anal triangle and functions to support and elevate the pelvic floor. The levator ani consists of the puborectalis, pubococcygeus, and iliococcygeus muscles. The coccygeus muscle also contributes to the support and elevation of the pelvic floor.
The internal anal sphincter consists of involuntary smooth muscle and represents a continuation of the circular muscle layer of the rectum. Autonomic nervous system control maintains a state of constant contraction, with relaxation occurring during defecation. The internal anal sphincter provides the majority of anal continence. The longitudinal muscle layer of the rectum combines with fibers of the levator ani to form the conjoined longitudinal muscle, located between the internal and external anal sphincters.
The external anal sphincter consists of voluntary skeletal muscle and is divided into subcutaneous, superficial, and deep parts. Closure of the anus is the primary function of the external anal sphincter.
Physiologic Variants
Anal Sphincters
Agenesis or hypoplasia of the external anal sphincter is rare but occurs in anorectal malformations, such as imperforate anus, disrupting voluntary continence and requiring reconstructive surgery.[11] Internal anal sphincter defects in high imperforate anus variants contribute to reduced resting tone and incontinence and are frequently observed as part of the spectrum of anomalies in VACTERL (vertebral defects, anal atresia, cardiac defects, tracheoesophageal fistula, esophageal atresia, renal anomalies, limb abnormalities) association. [12] Congenital variation in anal gland or crypt anatomy may contribute to early cryptoglandular infection and predispose to intersphincteric abscess formation. (Source: El-Haddad, 2024)
Anal Canal Features
Stenosis or atresia of the anal canal, with absent or malformed anal columns, arises in the imperforate anus spectrum, impairing passage and causing obstruction. Variations in anal gland anatomy may contribute to early fistula formation through cryptoglandular infection, although evidence for congenital glandular anomalies remains limited. Posterior fistula predominance is commonly observed in clinical practice and is attributed to patterns of anal gland drainage.
Ischiorectal Fossae
Congenital anterior displacement of the anus (low imperforate variant) distorts fossae symmetry, narrowing one side and widening the other, increasing hernia risk via altered fat distribution.[13][14] Alterations in the ischioanal fossae may occur in association with anorectal malformations and caudal regression syndrome, potentially affecting the structural support of the anal canal and defecatory function.[15] Variable anatomy of the anal glands and crypts from birth may facilitate abscess formation and spread in neonates, particularly in the setting of immature immunity or underlying anorectal or sacral anomalies.[16]
Surgical Considerations
Hemorrhoids
Internal and external hemorrhoids unresponsive to conservative management may require surgical intervention. Surgical approaches are reserved for acute complicated hemorrhoids or cases in which nonoperative treatments have failed. Surgical treatment options include hemorrhoidectomy, plication, Doppler-guided hemorrhoidal artery ligation, and stapled hemorrhoidopexy.[17][18]
Anal Cancer
Concurrent chemotherapy and radiotherapy comprise the treatment of choice for cancer of the anal canal. Surgical management is considered in cases of recurrent or persistent tumors after chemoradiotherapy or in stage T1 tumors without sphincter involvement.[19]
Perirectal Abscess
Perianal abscesses represent a subtype of perirectal abscess. Perirectal abscesses encompass ischiorectal, intersphincteric, and supralevator abscesses. Abscess formation results from occlusion and infection of an anal crypt gland. Physical examination may reveal a small fluctuant mass with erythema and induration of the overlying skin. Clinical presentation includes perirectal pain and fever. Perirectal abscesses require surgical treatment with incision and drainage.[20][21][22]
Clinical Significance
Hemorrhoids
Hemorrhoids arise from the internal or external hemorrhoidal plexuses and result from dilation and irritation of the anal cushions. Risk factors include constipation, diarrhea, prolonged straining during defecation, and pregnancy.
Internal hemorrhoids typically present with painless bleeding during defecation. These vascular dilations originate above the pectinate line and are painless due to the visceral innervation of this region. External hemorrhoids may present with pruritus and bleeding. These submucosal prominences occur below the pectinate line. Thrombosis of external hemorrhoids produces pain due to somatic innervation below the pectinate line.
Hemorrhoids are primarily managed conservatively with a high-fiber diet, sitz baths, and stool softeners. Additional nonoperative treatments include pharmacologic therapy and procedures such as rubber band ligation, with surgical intervention reserved for refractory cases.
Anal Cancer
Most cancers of the anal canal are classified as squamous cell carcinoma and demonstrate a strong association with human papillomavirus infection of the anus. Anal canal malignancy may present similarly to benign anal disease, with symptoms including pain, bleeding, pruritus, and a palpable mass. Diagnostic evaluation includes biopsy, pelvic magnetic resonance imaging, and positron emission tomography/computed tomography (PET/CT). Anal cancer is treated with concurrent chemotherapy and radiotherapy and demonstrates a high success rate.
Other Issues
Delivery-Associated Levator Ani Injury
Levator ani muscle avulsion at the puborectalis insertion occurs in a significant proportion of women after vaginal delivery and is associated with pelvic organ prolapse, anal incontinence, and voiding dysfunction due to widening of the levator hiatus and diminished pelvic floor support. Loss of levator ani integrity increases fecal urgency and contributes to continence dysfunction, although preserved muscle morphology is associated with better functional outcomes after obstetric trauma.[23]
The risk of levator ani avulsion may be reduced by minimizing modifiable intrapartum risk factors, such as prolonged 2nd stage of labor and operative vaginal delivery when safe alternatives exist, and by optimizing perineal support through controlled delivery techniques. Current evidence underscores the lack of reliable predictors for avulsion and the need for individualized obstetric management to mitigate trauma risk during spontaneous vaginal birth.
Conservative management after avulsion focuses on pelvic floor rehabilitation, including pelvic floor muscle training, although randomized evidence has not shown a clear reduction in avulsion prevalence compared with natural remission. Surgical repair techniques are poorly studied but may benefit selected patients. Continued research seeks to establish effective targeted interventions for persistent pelvic floor dysfunction associated with avulsion.[24]
Media
(Click Image to Enlarge)
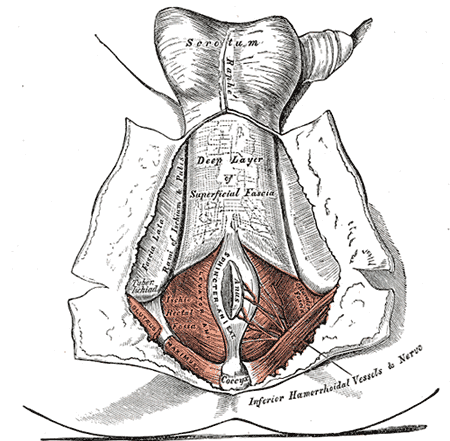
Inferior View of the Male Pelvic Outflow and Perineum. This illustration details the muscular and fascial layers of the perineum, highlighting the levator ani and sphincter ani externus. Visible landmarks include the coccyx, tuber ischiadicum, and the deep layer of superficial fascia. The distribution of the inferior hemorrhoidal vessels and nerves is shown within the ischiorectal fossa.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
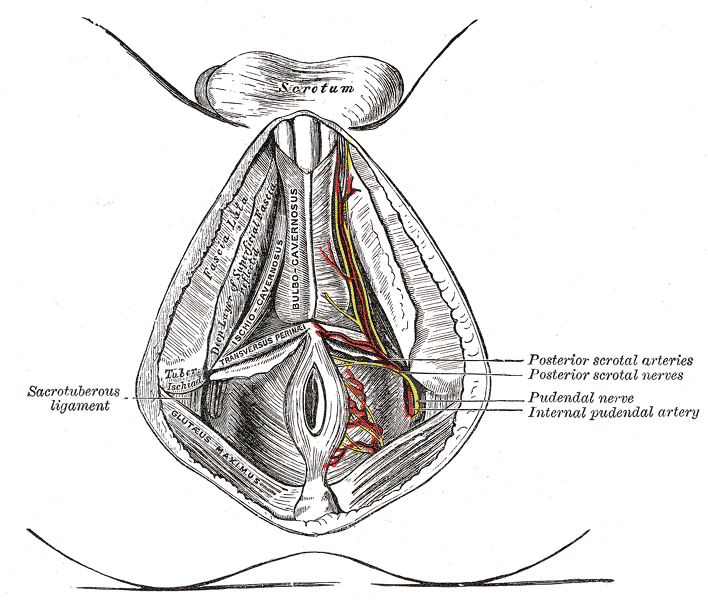
Neurovascular Structures of the Perineal Region. This anatomical illustration demonstrates the superficial and deep structures of the male perineal region. Labeled components include the sacrotuberous ligament, bulbocavernosus and ischiocavernosus muscles, pudendal nerve, and internal pudendal artery.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
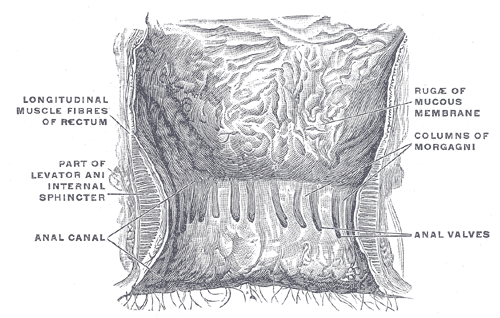
Interior of the Anal Canal and Lower Rectum. The diagram shows the specialized mucosal lining of the lower rectum and anal canal. Key features include the columns of Morgagni and anal valves.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
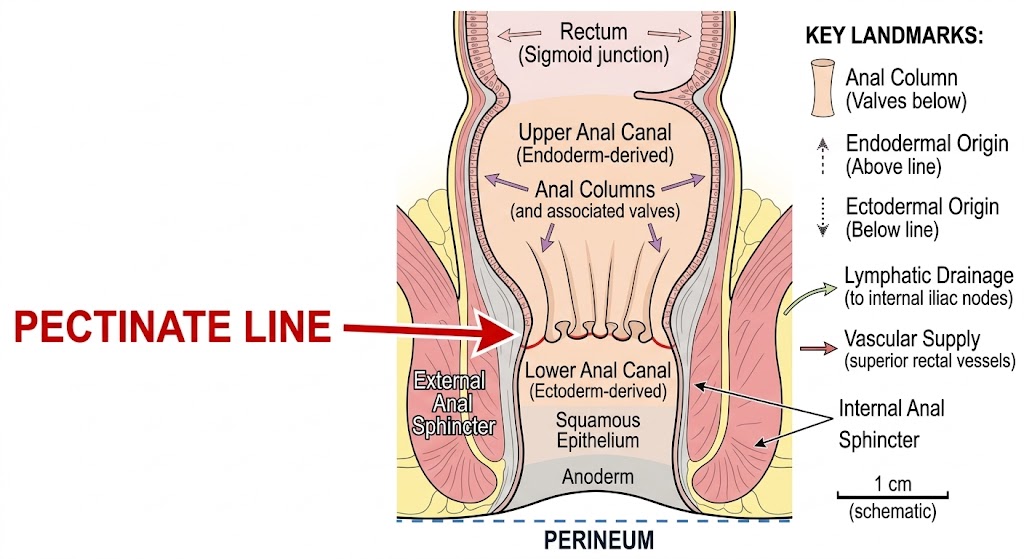
Neurovascular Divisions of the Anal Canal. The central red line tracing the anal valves is the pectinate line, which acts as a key landmark. The line divides the internal anal sphincter and provides a division point for different lymphatic drainage and vascular supply routes, as detailed in the key on the right.
Contributed by StatPearls.
References
Heinze T, Heimke M, Stelzner S, Wedel T. [Surgical anatomy of the anorectum]. Chirurgie (Heidelberg, Germany). 2025 May:96(5):431-444. doi: 10.1007/s00104-025-02244-9. Epub 2025 Mar 6 [PubMed PMID: 40047909]
Lee JM, Kim NK. Essential Anatomy of the Anorectum for Colorectal Surgeons Focused on the Gross Anatomy and Histologic Findings. Annals of coloproctology. 2018 Apr:34(2):59-71. doi: 10.3393/ac.2017.12.15. Epub 2018 Apr 30 [PubMed PMID: 29742860]
Lawson JO. Pelvic anatomy. II. Anal canal and associated sphincters. Annals of the Royal College of Surgeons of England. 1974 Jun:54(6):288-300 [PubMed PMID: 4833780]
Stoker J. Anorectal and pelvic floor anatomy. Best practice & research. Clinical gastroenterology. 2009:23(4):463-75. doi: 10.1016/j.bpg.2009.04.008. Epub [PubMed PMID: 19647683]
MORGAN CN. The surgical anatomy of the ischiorectal space. Proceedings of the Royal Society of Medicine. 1949 Mar:42(3):189-200 [PubMed PMID: 18126986]
Nakashima J, Zulfiqar H. Embryology, Rectum and Anal Canal. StatPearls. 2026 Jan:(): [PubMed PMID: 31869146]
Margetis N. Pathophysiology of internal hemorrhoids. Annals of gastroenterology. 2019 May-Jun:32(3):264-272. doi: 10.20524/aog.2019.0355. Epub 2019 Jan 23 [PubMed PMID: 31040623]
Gami B, Kubba F, Ziprin P. Human papilloma virus and squamous cell carcinoma of the anus. Clinical Medicine Insights. Oncology. 2014:8():113-9. doi: 10.4137/CMO.S13241. Epub 2014 Sep 17 [PubMed PMID: 25288893]
Yan Y, Inal B, Kapavarapu P, Alber K, Rao SSC. Novel Concepts on the Functional Neuroanatomy of the Anorectum: Implications for Anorectal Neuropathy and Neuromodulation Therapy. The American journal of gastroenterology. 2024 Nov 22:120(7):1478-1487. doi: 10.14309/ajg.0000000000003221. Epub 2024 Nov 22 [PubMed PMID: 39748794]
Mittal RK, Tuttle LJ. Anorectal Anatomy and Function. Gastroenterology clinics of North America. 2022 Mar:51(1):1-23. doi: 10.1016/j.gtc.2021.10.001. Epub [PubMed PMID: 35135656]
de Blaauw I, Stenström P, Yamataka A, Miyake Y, Reutter H, Midrio P, Wood R, Grano C, Pakarinen M. Anorectal malformations. Nature reviews. Disease primers. 2024 Nov 21:10(1):88. doi: 10.1038/s41572-024-00574-2. Epub 2024 Nov 21 [PubMed PMID: 39572572]
Smith CA, Avansino J. Anorectal Malformations. StatPearls. 2026 Jan:(): [PubMed PMID: 31194415]
Abeysuriya V, Salgado LS, Samarasekera DN. The distribution of the anal glands and the variable regional occurrence of fistula-in-ano: is there a relationship? Techniques in coloproctology. 2010 Dec:14(4):317-21. doi: 10.1007/s10151-010-0648-2. Epub 2010 Oct 15 [PubMed PMID: 20949301]
Hencke J, Staubach R, Loff S. Manometric Evaluation of the Sphincter Complex in Anterior Anus and Mild Anorectal Malformations-An Important Diagnostic Tool. Diagnostics (Basel, Switzerland). 2025 Apr 24:15(9):. doi: 10.3390/diagnostics15091078. Epub 2025 Apr 24 [PubMed PMID: 40361897]
Purbasari U, Nazar H, Miraj F, Aprilia D, Widiani W, Suprihatin M, Eureka AN. Caudal regression syndrome from radiology and clinical perspective: A case series and a proposed new integrated diagnostic algorithm. Radiology case reports. 2023 Jul:18(7):2478-2486. doi: 10.1016/j.radcr.2023.04.015. Epub 2023 May 12 [PubMed PMID: 37235076]
Level 2 (mid-level) evidencePark J. Management of perianal abscess and fistula-in-ano in infants and children. Clinical and experimental pediatrics. 2020 Jul:63(7):261-262. doi: 10.3345/cep.2020.00150. Epub 2020 Mar 23 [PubMed PMID: 32252144]
Lohsiriwat V. Hemorrhoids: from basic pathophysiology to clinical management. World journal of gastroenterology. 2012 May 7:18(17):2009-17. doi: 10.3748/wjg.v18.i17.2009. Epub [PubMed PMID: 22563187]
Hawkins AT, Davis BR, Bhama AR, Fang SH, Dawes AJ, Feingold DL, Lightner AL, Paquette IM, Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Hemorrhoids. Diseases of the colon and rectum. 2024 May 1:67(5):614-623. doi: 10.1097/DCR.0000000000003276. Epub 2024 Jan 31 [PubMed PMID: 38294832]
Level 1 (high-level) evidenceSymer MM, Yeo HL. Recent advances in the management of anal cancer. F1000Research. 2018:7():. pii: F1000 Faculty Rev-1572. doi: 10.12688/f1000research.14518.1. Epub 2018 Sep 28 [PubMed PMID: 30345012]
Level 3 (low-level) evidenceConner JN, Eren S, Tuma F. Perianal Abscess. StatPearls. 2026 Jan:(): [PubMed PMID: 29083652]
Turner SV, Singh J. Perirectal Abscess(Archived). StatPearls. 2026 Jan:(): [PubMed PMID: 29939672]
Gaertner WB, Burgess PL, Davids JS, Lightner AL, Shogan BD, Sun MY, Steele SR, Paquette IM, Feingold DL, Clinical Practice Guidelines Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons Clinical Practice Guidelines for the Management of Anorectal Abscess, Fistula-in-Ano, and Rectovaginal Fistula. Diseases of the colon and rectum. 2022 Aug 1:65(8):964-985. doi: 10.1097/DCR.0000000000002473. Epub 2022 Jul 5 [PubMed PMID: 35732009]
Level 1 (high-level) evidenceEstendahl K, Danielsson L. Women's experiences of life and healthcare after levator ani avulsion: a qualitative interview study. BMC women's health. 2025 Jul 7:25(1):336. doi: 10.1186/s12905-025-03892-z. Epub 2025 Jul 7 [PubMed PMID: 40624701]
Level 2 (mid-level) evidenceDoxford-Hook EA, Slemeck E, Downey CL, Marsh FA. Management of levator ani avulsion: a systematic review and narrative synthesis. Archives of gynecology and obstetrics. 2023 Nov:308(5):1399-1408. doi: 10.1007/s00404-023-06955-4. Epub 2023 Feb 21 [PubMed PMID: 36808288]
Level 1 (high-level) evidence