 Anatomy, Head and Neck: Sternocleidomastoid Muscle
Anatomy, Head and Neck: Sternocleidomastoid Muscle
Introduction
The sternocleidomastoid (SCM) is a prominent superficial neck muscle that divides the neck into anterior and posterior triangles (see Image. Superficial Neck Anatomy). Originating from the sternal manubrium and medial clavicle, the muscle inserts onto the mastoid process and superior nuchal line. The SCM facilitates lateral neck flexion, contralateral head rotation, and bilateral cervical flexion or extension, depending on cervical spine rigidity, and contributes to inspiration.
The muscle's blood supply emanates from branches of the external carotid artery. Innervation is primarily via the accessory nerve (cranial nerve XI), with proprioceptive fibers coming from the cervical plexus. Anatomical variants include differences in origins, insertions, number of muscle heads, and occasional aberrant innervation. The SCM also participates in posture regulation, temporomandibular function, and complex cervicofacial muscle coordination.
The SCM serves as a key landmark in the assessment of neck and head pathologies and the execution of surgical procedures such as carotid endarterectomy. Dysfunction or injury of this muscle can contribute to postural abnormalities, torticollis, impaired cervical mobility, and altered temporomandibular function. Electrophysiological studies indicate that SCM activity reflects broader cervicofacial muscular coordination, making its evaluation useful in diagnosing neuromuscular disorders. SCM palpation and functional testing can aid clinicians in identifying muscle hypotrophy, asymmetry, or altered activation patterns associated with chronic neck pain, congenital muscular abnormalities, or secondary musculoskeletal adaptations.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Anatomy
The SCM divides the neck into anterior and posterior triangles. The anterior triangle is bounded by the posterior border of the SCM, the inferior border of the mandible, and the medial line of the neck. Suprahyoid and infrahyoid muscles lie within the anterior triangle. The posterior triangle is bounded by the SCM anteriorly, the clavicle inferiorly, and the trapezius posteriorly. Scalene muscles reside within the posterior triangle. The SCM is a large, easily identifiable, and palpable muscle (see Image. Cross-Section of the Human Neck).
The SCM originates from the upper edge of the sternal manubrium and the medial quarter of the clavicle, with the 2 heads merging into a single muscle belly directed upward and laterally. Insertions occur at the mastoid process of the temporal bone and the anterior portion of the superior nuchal line. Fibers are arranged in parallel. The SCM is not pennate.
The SCM may be subdivided into 4 portions based on origin and insertion: sternomastoid, sterno-occipital, cleidomastoid, and cleido-occipital (see Image. Anterior Neck Muscles and Related Structures). The sternomastoid portion generates the greatest contractile force, whereas the cleido-occipital portion produces the least.[1]
Function
The unilateral contraction of the SCM produces a triple movement: rotation of the head to the side opposite the contracting muscle, lateral inclination toward the contracting side, and extension. The effects of simultaneous contraction of both SCM muscles depend on the state of contraction of other cervical spine muscles. If the cervical spine is mobile, bilateral contraction induces cervical hyperlordosis with head extension and dorsal bending of the cervical spine. If the cervical spine is rigid and rectilinear due to paravertebral muscle contraction, simultaneous SCM contraction produces cervical flexion along the dorsal spine and forward flexion of the head. The SCM also contributes to inspiration by anchoring to the temporal bone and elevating the sternum and clavicles.[2]
The SCM contributes significantly to cervical and overall body posture. Vestibular stimulation electrically activates the SCM, demonstrating a close connection between the vestibular system and SCM motoneurons.[3] Lateral inclination is the movement in which the SCM exhibits maximal speed and force.[4]
The SCM also supports proper temporomandibular joint function. During mastication, a trigeminal-cervical reflex activates the SCM, and its innervation is essential for optimal temporomandibular joint occlusion. Mandibular occlusal alterations disrupt SCM function, leading to muscular incoordination and abnormal neck inclinations. Correction of occlusal defects or dental treatment has resolved torticollis in some cases. During unilateral mastication, SCM activity synchronizes with the masseter, whereas bilateral chewing elicits anticipatory SCM activation, likely to stabilize the neck.[5]
Embryology
The SCM derives from paraxial (preoptic) mesoderm and occipital (postoptic) somites and partially from neural crests.[6][7] The SCM appears on the 14th day of gestation in animal models. Recent studies indicate that progenitor cells forming the neck muscles occupy the same region as cardiac progenitor cells within the cardiopharyngeal mesoderm.[8]
Blood Supply and Lymphatics
The arterial supply of the SCM derives from branches of the external carotid artery, including the occipital artery and the superior thyroid artery, which are palpable in the medial-anterior portion of the muscle. Blood flow to the respiratory muscles, including the SCM, during intense physical activity increases at the expense of limb muscles.[9] The external jugular vein courses inferiorly and posteriorly to the SCM, draining venous blood via anterior and posterior branches. The lymphatic drainage of the SCM follows the vertical chain, comprising the anterior superficial lymph nodes and the posterior triangle lymph nodes inferiorly.
Nerves
The cutaneous branches of the cervical plexus emerge from the posterior edge of the SCM and contribute to the muscle’s proprioceptive functions. The accessory nerve passes through the posterior triangle to innervate the trapezius and the SCM.[10]
Muscles
The muscles of the neck are components of the myofascial system, which establishes both an anatomical and functional continuum (see Image. Muscles of the Head, Face, and Neck).[11] Dysfunction of a single muscle or muscle segment produces functional alterations throughout the neck musculature. For example, ocular pathology modifies the electromyographic activity of the masseter and neck muscles, including the SCM.[12][13]
Superficial and deep neck muscles are activated by the cortical system via the reticulospinal pathway, with synchronous activation regardless of muscle layer depth.[14] Therefore, consideration of the entire neck muscle complex is essential when evaluating pathology that appears to involve a single muscle.
In healthy subjects, the SCM contains mostly white, anaerobic fibers (~65%) and fewer red, aerobic fibers (~35%).[15] The muscle generates substantial force rapidly with minimal resistance over prolonged periods. The relative proportion of white and red fibers in the SCM changes with age, with red fibers increasing to approximately 44% at the expense of white fibers.[16] The SCM demonstrates adaptive responses to the surrounding environment and age-related physiological changes.
Physiologic Variants
Agenesis of the SCM, which may be accompanied by the absence of the trapezius, is a rare anomaly that often does not produce clinical or functional deficits. This outcome likely reflects compensatory adaptations by other neck muscles.[17]
Other anatomical variations of the SCM involve its origins, which can influence surgical approaches in the region. The clavicular attachment may be narrow or wide, measuring up to 7 to 8 cm. Multiple clavicular attachments may also be observed. Variations in origin can affect the acromioclavicular joint or produce additional muscular bellies in the SCM. Insertions at the sternoclavicular joint have been documented, altering neck anatomy.[18]
An increased number of SCM heads is relatively common. For example, one side may exhibit 2 sternomastoid heads, a cleido-occipital head, and a cleidomastoid occipital head, whereas the contralateral side may present a single sternomastoid, a cleido-occipital, and 2 cleidomastoid heads, totaling 4 heads.[19]
Rarely, the margin of the SCM contacts the trapezius, likely due to embryological malformations. Known insertion variants include cleido-epistrophic, cleido-cervical, and cleido-atlantic types, each with 1 or more heads.[20]
Innervation of the SCM exhibits variability. A study reported that the lower portion of the SCM receives fibers from a branch of C1 via the ansa cervicalis (descendens hypoglossi). Similar innervation may occur in the upper portion.[21] An aberrant branch of the facial nerve has been documented to innervate the deep portion of the upper 1/3 of the SCM.[22]
The SCM is also recognized by alternative names, including "nutator capitis," "mastoideus colli," "sternocleidomastoid muscle of Kopfnicker," and "sternomastoid muscle." Awareness of the muscle's anatomical variations is essential when performing surgical interventions in the region.
Surgical Considerations
The SCM can serve as an autograft for repairing surgical defects. This application allows reconstruction of soft tissue or bony areas in the head and neck.
A flap of the SCM may be employed during parotid gland resection for tumor removal. The muscle facilitates adequate flap length and rotation over the incision site, reduces depression of the parotidectomy area, and decreases the risk of necrosis due to the SCM’s rich vascularization. Complete prevention of Frey syndrome (auriculotemporal nerve injury) cannot be guaranteed.[23]
The SCM is utilized in a variety of procedures requiring reconstruction of orofacial and pharyngeal structures. The selection of muscular flaps or flaps incorporating bony segments depends on the specific surgical objective.[24] Examples of structures that may be reconstructed using SCM flaps include the following:
- Tongue and buccal floor
- Oral cavity, oropharynx, and laryngotracheal complex
- Regions of the head and neck
- Jawbone and mastoid defects
- Esophagopharyngeal complex
- Cheek
SCM muscle flaps are employed in the surgical repair of congenital muscular torticollis. In muscular torticollis, shortening and fibrosis of the SCM alter head and shoulder alignment, producing ipsilateral lateral flexion and contralateral rotation of the face. Treatment options include rehabilitation or surgical intervention. Delayed diagnosis without therapy may result in persistent shortening of the SCM and formation of a rigid muscle band. Severe cases can cause lasting craniofacial deformities.[25]
Favorable outcomes are achievable within the first 5 years of life, with earlier intervention providing optimal results.[26] Surgical release of the rigid SCM band can improve facial and cervical deformities in adults with untreated congenital stiff neck, although results are never equivalent to early childhood intervention. The standard surgical approach in both children and adults involves partial resection of the SCM.[27]
The SCM also serves as a critical anatomical landmark for surgical exposure during carotid endarterectomy, guiding incision placement and access to the carotid sheath. Identification and retraction of the SCM facilitate safe dissection while helping preserve adjacent neurovascular structures (see Image. Preoperative Markings for Carotid Endarterectomy).
Clinical Significance
Sternocleidomastoid Muscle Function Evaluation
Assessment begins with the patient in a seated position to observe hypotrophy of the SCM and postural abnormalities of the neck, head, shoulder, scapula, clavicle, and sternal manubrium. Voluntary neck movements are performed to evaluate motor or pain limitations. Forced inhalation and simulated mastication are used to assess SCM function.
Reflexes are tested using a small tendon hammer at the clavicular insertion of the SCM. Muscle strength is evaluated by having the patient move the head through flexion, rotation, and lateral inclination against minimal resistance applied by the examiner. Lesions involving the SCM may affect the accessory nerve, although such occurrences are infrequent.[28] Spinal accessory nerve injury results in absent tendon reflexes, atrophy of the SCM and trapezius, shoulder depression, and the sign of Sicard, characterized by increased depth of the supraclavicular fossa. Paralysis of the SCM can produce torticollis.
Types of Torticollis
Torticollis can be classified into several types. Paralytic torticollis results from injury to the spinal accessory nerve.[29] Congenital torticollis is frequently associated with intrauterine packaging disorders, including metatarsus adductus, developmental dysplasia of the hip, acetabular dysplasia, and congenital hip dislocations.[30][31] Metatarsus adductus occurs in approximately 15% of congenital torticollis cases.[32] Spasmodic torticollis is a form of segmental dystonia. Ocular torticollis arises when diplopia affects SCM posture.[33]
Symptomatic torticollis has variable etiologies, such as pain, inflammation, infection, or abnormal cervical vertebral positioning.[34] “Psychic pillow” torticollis is observed in severe neurological conditions, including Parkinson disease and catatonic disorders, in which patients maintain the head bent forward as if resting on a pillow, even in the supine position. Psychogenic torticollis is characterized by fear of correct neck movements due to pain or vertigo. Accurate diagnosis of these disorders typically requires electromyography and imaging studies, including magnetic resonance imaging, computed tomography, or ultrasonography.
Other Issues
Manual Approach: Physiotherapy
All superficial and deep muscle layers should be assessed when managing SCM dysfunction. In congenital torticollis, which accounts for approximately 1/3 of congenital muscular abnormalities, physiotherapy plays a central role in resolving dysfunction or accelerating recovery following surgical intervention. Recommended conservative therapy includes stretching exercises, guided voluntary movements to improve posture in children of appropriate age, and parental modifications of the child’s posture. Conservative management resolves the condition in many cases.[35] Therapeutic approaches to SCM dysfunction vary according to the therapist’s assessment and specific medical indications.
Certain pathologies necessitate primary surgical intervention. These conditions include intramuscular hemangioma, pseudosarcomatous proliferative myositis, pseudotumor of infancy (fibromatosis colli), and rupture of the SCM.
Recent studies demonstrate increased electrical activity of the SCM in individuals with chronic neck pain compared to subjects without pain. Chronic cervical pain is also associated with greater fat infiltration within the SCM.[36] Incorporating stretching and massage into conventional physiotherapy improves clinical outcomes in this context.[37]
Alterations in the electromyographic spectrum of the SCM correlate with the presence of temporomandibular disorders. Electromyographic evaluation of the SCM provides a tool to detect mandibular dysfunctions.[38]
Osteopathy and Manual Therapy
Osteopathic treatment aimed at SCM recovery after surgery can also positively influence scar formation. Gentle, noninvasive osteopathic manipulation addresses all myofascial layers of the neck and the intervertebral spaces of the cervical spine.[39][40][41]
Obstructive sleep apnea syndrome (OSAS) induces nonphysiological adaptation of the SCM, reducing the muscle's viscoelasticity. Greater muscle stiffness correlates with increased OSAS severity. Assessment of the SCM provides clinical insight for OSAS diagnosis. Improving muscle elasticity may offer therapeutic benefit.[42]
Swallowing difficulties frequently occur in patients with advanced head and neck cancer following radiotherapy. SCM stiffness strongly correlates with reduced laryngeal elevation. Enhancing SCM mobility may improve laryngeal elevation and mitigate swallowing impairments.[43]
Abnormal cervical lordosis is associated with altered neuromuscular activity of the SCM. This adaptation increases fatigue of the neck muscles and produces pain during movement. Optimizing SCM biomechanics may reduce these symptoms.[44]
Significant traumatic injury to the SCM is uncommon. Ultrasound or contrast-enhanced computed tomography can detect hematomas if injury is suspected. Conservative management with immobilization is sufficient when adjacent vital structures remain uncompromised.[45]
Parkinson disease is associated with instability in daily activities, including standing, sitting, and walking. Increased myoelectric activity of the SCM contributes to dynamic postural alterations in Parkinson disease. Further investigation is required.[46]
Chronic myofascial pain of the SCM occurs in approximately 55% of patients with head and neck cancer after treatment. This pain is linked to depression. Gentle therapies aimed at improving muscle tone may provide clinical benefit.[47]
Media
(Click Image to Enlarge)
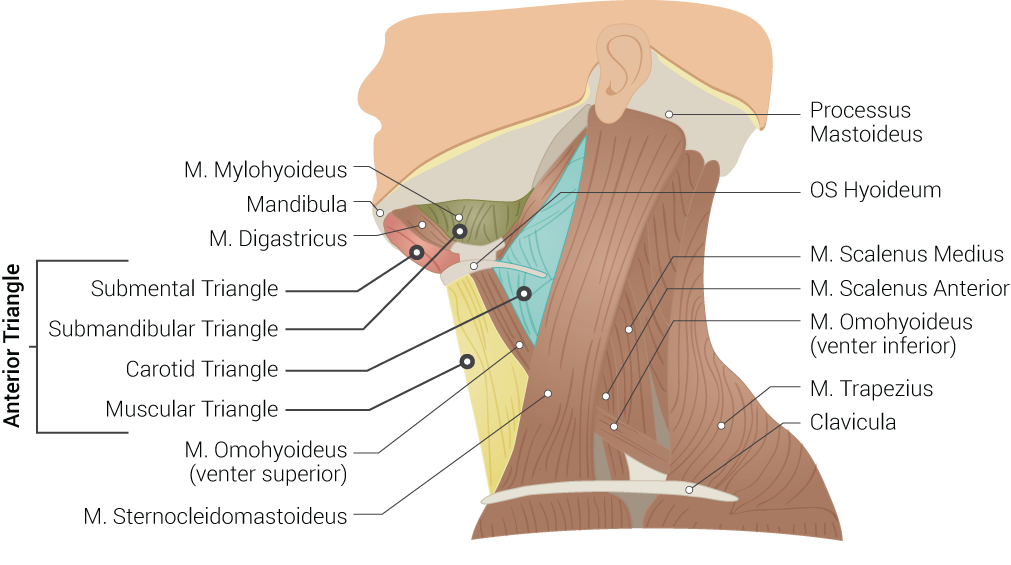
Superficial Neck Anatomy. This left lateral-view illustration shows the anterior and posterior triangles. The anterior triangle is further divided into the submental, submandibular, carotid, and muscular triangles. The muscles in this illustration include the mylohyoideus, digastricus, omohyoideus (venter superior and inferior), sternocleidomastoideus, scalenus medius and anterior, and trapezius. Bony structures include the mandible, mastoid process, left hyoid, and clavicle.
Illustrated by B Palmer
(Click Image to Enlarge)
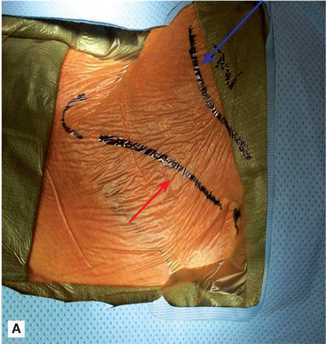
Preoperative Markings for Carotid Endarterectomy. This clinical photograph demonstrates the surgical markings on the lateral neck prior to a carotid endarterectomy. The red arrow indicates the planned incision line along the anterior border of the sternocleidomastoid, which allows for optimal arterial exposure. The blue arrow identifies the inferior border of the mandible, which ensures the incision is positioned correctly for distal access.
Contributed by S Dulebohn, MD
(Click Image to Enlarge)
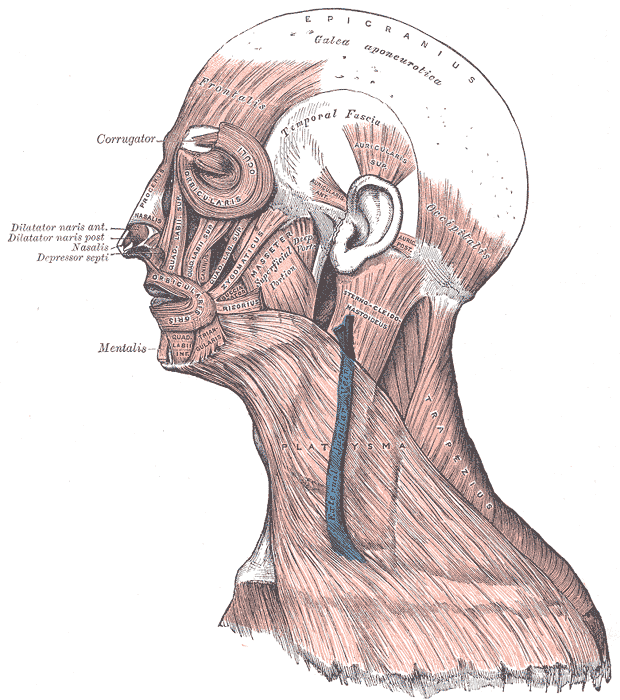
Muscles of the Head, Face, and Neck. The epicranius, galea aponeurotica, frontalis, temporal fascia, auricularis superior, auricularis anterior, auricularis posterior, occipitalis, sternocleidomastoid, platysma, trapezius, orbicularis oculi, corrugator, procerus, nasalis, dilator naris anterior, dilator naris posterior, depressor septi, mentalis, orbicularis oris, masseter, zygomaticus, and risorius muscles are shown in the image.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
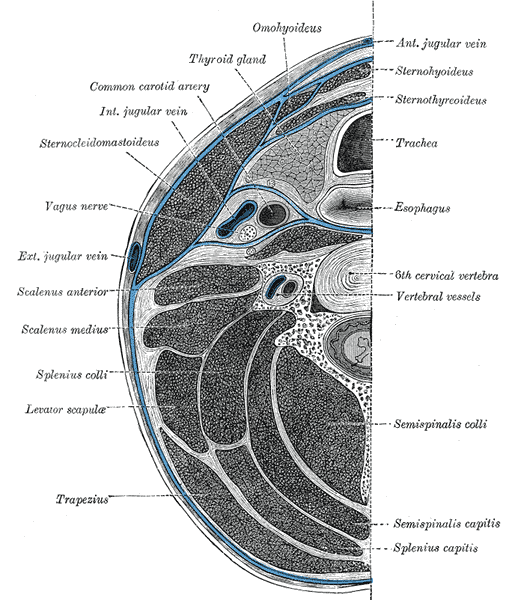
Cross-Section of the Human Neck. This diagram illustrates the anatomical relationships between the cervical fascia, major muscle groups, and visceral organs at the C6 level. Key neurovascular structures, including the carotid artery and vagus nerve, are shown within their respective compartments.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
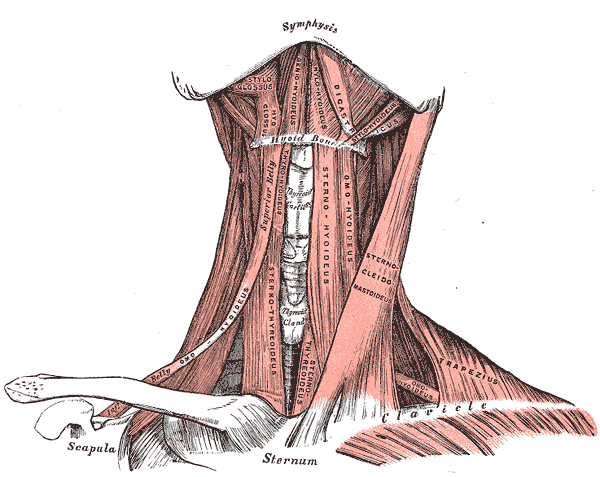
Anterior Neck Muscles and Related Structures. This illustration shows the suprahyoid, infrahyoid, styloglossus, hyoglossus, geniohyoideus, mylohyoideus, digastricus, stylohyoideus, omohyoideus, sternothyroideus, sternohyoideus, omohyoideus, sternocleidomastoideus, trapezius, and omohyoideus muscles. The mandibular symphysis, thyroid cartilage, thyroid gland, hyoid bone, clavicles, scapula, and sternum are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Kennedy E, Albert M, Nicholson H. The fascicular anatomy and peak force capabilities of the sternocleidomastoid muscle. Surgical and radiologic anatomy : SRA. 2017 Jun:39(6):629-645. doi: 10.1007/s00276-016-1768-9. Epub 2016 Nov 2 [PubMed PMID: 27807639]
Kohan EJ, Wirth GA. Anatomy of the neck. Clinics in plastic surgery. 2014 Jan:41(1):1-6. doi: 10.1016/j.cps.2013.09.016. Epub [PubMed PMID: 24295343]
Forbes PA, Fice JB, Siegmund GP, Blouin JS. Electrical Vestibular Stimuli Evoke Robust Muscle Activity in Deep and Superficial Neck Muscles in Humans. Frontiers in neurology. 2018:9():535. doi: 10.3389/fneur.2018.00535. Epub 2018 Jul 5 [PubMed PMID: 30026725]
Luciani BD, Desmet DM, Alkayyali AA, Leonardis JM, Lipps DB. Identifying the mechanical and neural properties of the sternocleidomastoid muscles. Journal of applied physiology (Bethesda, Md. : 1985). 2018 May 1:124(5):1297-1303. doi: 10.1152/japplphysiol.00892.2017. Epub 2018 Feb 8 [PubMed PMID: 29420159]
Guo SX, Li BY, Zhang Y, Zhou LJ, Liu L, Widmalm SE, Wang MQ. An electromyographic study on the sequential recruitment of bilateral sternocleidomastoid and masseter muscle activity during gum chewing. Journal of oral rehabilitation. 2017 Aug:44(8):594-601. doi: 10.1111/joor.12527. Epub 2017 Jun 22 [PubMed PMID: 28548212]
Nooij LS, Oostra RJ. Trapezius aplasia: indications for a dual developmental origin of the trapezius muscle. Clinical anatomy (New York, N.Y.). 2006 Sep:19(6):547-9 [PubMed PMID: 16583429]
Level 3 (low-level) evidenceSingh S, Chauhan P, Loh HK, Mehta V, Suri RK. Absence of Posterior Triangle: Clinical and Embryological Perspective. Journal of clinical and diagnostic research : JCDR. 2017 Feb:11(2):AD01-AD02. doi: 10.7860/JCDR/2017/23896.9176. Epub 2017 Feb 1 [PubMed PMID: 28384846]
Level 3 (low-level) evidenceLescroart F, Hamou W, Francou A, Théveniau-Ruissy M, Kelly RG, Buckingham M. Clonal analysis reveals a common origin between nonsomite-derived neck muscles and heart myocardium. Proceedings of the National Academy of Sciences of the United States of America. 2015 Feb 3:112(5):1446-51. doi: 10.1073/pnas.1424538112. Epub 2015 Jan 20 [PubMed PMID: 25605943]
Level 3 (low-level) evidenceDominelli PB, Archiza B, Ramsook AH, Mitchell RA, Peters CM, Molgat-Seon Y, Henderson WR, Koehle MS, Boushel R, Sheel AW. Effects of respiratory muscle work on respiratory and locomotor blood flow during exercise. Experimental physiology. 2017 Nov 1:102(11):1535-1547. doi: 10.1113/EP086566. Epub 2017 Sep 24 [PubMed PMID: 28841267]
Roberts SO, Cardozo A. A detailed review of the spinal accessory nerve and its anatomical variations with cadaveric illustration. Anatomical science international. 2024 Jun:99(3):239-253. doi: 10.1007/s12565-024-00770-w. Epub 2024 May 2 [PubMed PMID: 38696101]
Bordoni B, Marelli F, Morabito B, Sacconi B. The indeterminable resilience of the fascial system. Journal of integrative medicine. 2017 Sep:15(5):337-343. doi: 10.1016/S2095-4964(17)60351-0. Epub [PubMed PMID: 28844209]
Ciavarella D, Palazzo A, De Lillo A, Lo Russo L, Paduano S, Laino L, Chimenti C, Frezza F, Lo Muzio L. Influence of vision on masticatory muscles function: surface electromyographic evaluation. Annali di stomatologia. 2014 Apr:5(2):61-5 [PubMed PMID: 25002919]
Miralles R, Valenzuela S, Ramirez P, Santander H, Palazzi C, Ormeño G, Zúñiga C. Visual input effect on EMG activity of sternocleidomastoid and masseter muscles in healthy subjects and in patients with myogenic cranio-cervical-mandibular dysfunction. Cranio : the journal of craniomandibular practice. 1998 Jul:16(3):168-84 [PubMed PMID: 9852810]
Level 2 (mid-level) evidenceBlouin JS, Siegmund GP, Carpenter MG, Inglis JT. Neural control of superficial and deep neck muscles in humans. Journal of neurophysiology. 2007 Aug:98(2):920-8 [PubMed PMID: 17537909]
Cvetko E, Karen P, Eržen I. Myosin heavy chain composition of the human sternocleidomastoid muscle. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2012 Sep:194(5):467-72. doi: 10.1016/j.aanat.2012.05.001. Epub 2012 May 15 [PubMed PMID: 22658700]
Meznaric M, Eržen I, Karen P, Cvetko E. Effect of ageing on the myosin heavy chain composition of the human sternocleidomastoid muscle. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2018 Mar:216():95-99. doi: 10.1016/j.aanat.2017.12.001. Epub 2017 Dec 28 [PubMed PMID: 29289708]
Vajramani A, Witham FM, Richards RH. Congenital unilateral absence of sternocleidomastoid and trapezius muscles: a case report and literature review. Journal of pediatric orthopedics. Part B. 2010 Sep:19(5):462-4. doi: 10.1097/BPB.0b013e32833ce404. Epub [PubMed PMID: 20647939]
Level 3 (low-level) evidenceSaha A, Mandal S, Chakraborty S, Bandyopadhyay M. Morphological study of the attachment of sternocleidomastoid muscle. Singapore medical journal. 2014 Jan:55(1):45-7. doi: 10.11622/smedj.2013215. Epub [PubMed PMID: 24241357]
Kim SY, Jang HB, Kim J, Yoon SP. Bilateral four heads of the sternocleidomastoid muscle. Surgical and radiologic anatomy : SRA. 2015 Sep:37(7):871-3. doi: 10.1007/s00276-014-1397-0. Epub 2014 Nov 25 [PubMed PMID: 25422097]
Level 3 (low-level) evidenceSarikcioglu L, Donmez BO, Ozkan O. Cleidooccipital muscle: an anomalous muscle in the neck region. Folia morphologica. 2001 Nov:60(4):347-9 [PubMed PMID: 11770348]
Level 3 (low-level) evidenceBlythe JN, Matharu J, Reuther WJ, Brennan PA. Innervation of the lower third of the sternocleidomastoid muscle by the ansa cervicalis through the C1 descendens hypoglossal branch: a previously unreported anatomical variant. The British journal of oral & maxillofacial surgery. 2015 May:53(5):470-1. doi: 10.1016/j.bjoms.2015.01.005. Epub 2015 Mar 6 [PubMed PMID: 25747248]
Level 3 (low-level) evidenceCvetko E. Sternocleidomastoid muscle additionally innervated by the facial nerve: case report and review of the literature. Anatomical science international. 2015 Jan:90(1):54-6. doi: 10.1007/s12565-013-0224-8. Epub 2013 Dec 18 [PubMed PMID: 24347311]
Level 3 (low-level) evidenceSanabria A, Kowalski LP, Bradley PJ, Hartl DM, Bradford CR, de Bree R, Rinaldo A, Ferlito A. Sternocleidomastoid muscle flap in preventing Frey's syndrome after parotidectomy: a systematic review. Head & neck. 2012 Apr:34(4):589-98. doi: 10.1002/hed.21722. Epub 2011 Apr 5 [PubMed PMID: 21472880]
Level 1 (high-level) evidenceKierner AC, Zelenka I, Gstoettner W. The sternocleidomastoid flap--its indications and limitations. The Laryngoscope. 2001 Dec:111(12):2201-4 [PubMed PMID: 11802026]
Level 1 (high-level) evidenceLim KS, Shim JS, Lee YS. Is sternocleidomastoid muscle release effective in adults with neglected congenital muscular torticollis? Clinical orthopaedics and related research. 2014 Apr:472(4):1271-8. doi: 10.1007/s11999-013-3388-6. Epub 2013 Nov 21 [PubMed PMID: 24258687]
Level 2 (mid-level) evidenceLee JK, Moon HJ, Park MS, Yoo WJ, Choi IH, Cho TJ. Change of craniofacial deformity after sternocleidomastoid muscle release in pediatric patients with congenital muscular torticollis. The Journal of bone and joint surgery. American volume. 2012 Jul 3:94(13):e93. doi: 10.2106/JBJS.K.01567. Epub [PubMed PMID: 22760394]
Level 2 (mid-level) evidencePombo Castro M, Luaces Rey R, Vázquez Mahía I, López-Cedrún Cembranos JL. Congenital muscular torticollis in adult patients: literature review and a case report using a harmonic scalpel. Journal of oral and maxillofacial surgery : official journal of the American Association of Oral and Maxillofacial Surgeons. 2014 Feb:72(2):396-401. doi: 10.1016/j.joms.2013.08.017. Epub 2013 Oct 16 [PubMed PMID: 24139297]
Level 3 (low-level) evidenceBordoni B, Varacallo MA. Neuroanatomy, Cranial Nerve 11 (Accessory). StatPearls. 2026 Jan:(): [PubMed PMID: 29939544]
Tomczak KK, Rosman NP. Torticollis. Journal of child neurology. 2013 Mar:28(3):365-78. doi: 10.1177/0883073812469294. Epub 2012 Dec 26 [PubMed PMID: 23271760]
Bourne M, Talkad A, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Foot Fascia. StatPearls. 2026 Jan:(): [PubMed PMID: 30252299]
Gold M, Munjal A, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb, Hip Joint. StatPearls. 2026 Jan:(): [PubMed PMID: 29262200]
Williams CM, James AM, Tran T. Metatarsus adductus: development of a non-surgical treatment pathway. Journal of paediatrics and child health. 2013 Sep:49(9):E428-33. doi: 10.1111/jpc.12219. Epub 2013 May 6 [PubMed PMID: 23647850]
Level 1 (high-level) evidenceAkbari MR, Khorrami-Nejad M, Kangari H, Akbarzadeh Baghban A, Ranjbar Pazouki M. Ocular Abnormal Head Posture: A Literature Review. Journal of current ophthalmology. 2021 Oct-Dec:33(4):379-387. doi: 10.4103/joco.joco_114_20. Epub 2022 Jan 6 [PubMed PMID: 35128182]
Ganos C, Edwards MJ, Bhatia KP. The Phenomenology of Functional (Psychogenic) Dystonia. Movement disorders clinical practice. 2014 Apr:1(1):36-44. doi: 10.1002/mdc3.12013. Epub 2014 Apr 10 [PubMed PMID: 30363921]
Carenzio G, Carlisi E, Morani I, Tinelli C, Barak M, Bejor M, Dalla Toffola E. Early rehabilitation treatment in newborns with congenital muscular torticollis. European journal of physical and rehabilitation medicine. 2015 Oct:51(5):539-45 [PubMed PMID: 25692687]
Van Looveren E, Cagnie B, Coppieters I, Meeus M, De Pauw R. Changes in Muscle Morphology in Female Chronic Neck Pain Patients Using Magnetic Resonance Imaging. Spine. 2021 May 15:46(10):638-648. doi: 10.1097/BRS.0000000000003856. Epub [PubMed PMID: 33290364]
Büyükturan B, Şaş S, Kararti C, Büyükturan Ö. The effects of combined sternocleidomastoid muscle stretching and massage on pain, disability, endurance, kinesiophobia, and range of motion in individuals with chronic neck pain: A randomized, single-blind study. Musculoskeletal science & practice. 2021 Oct:55():102417. doi: 10.1016/j.msksp.2021.102417. Epub 2021 Jun 12 [PubMed PMID: 34147954]
Level 1 (high-level) evidenceChoi KH, Kwon OS, Kim L, Lee SM, Jerng UM, Jung J. Electromyographic changes in masseter and sternocleidomastoid muscles can be applied to diagnose of temporomandibular disorders: An observational study. Integrative medicine research. 2021 Dec:10(4):100732. doi: 10.1016/j.imr.2021.100732. Epub 2021 May 16 [PubMed PMID: 34141576]
Level 2 (mid-level) evidencePaul FA, Buser BR. Osteopathic manipulative treatment applications for the emergency department patient. The Journal of the American Osteopathic Association. 1996 Jul:96(7):403-9 [PubMed PMID: 8758873]
Galindez-Ibarbengoetxea X, Setuain I, Ramírez-Velez R, Andersen LL, González-Izal M, Jauregi A, Izquierdo M. Immediate Effects of Osteopathic Treatment Versus Therapeutic Exercise on Patients With Chronic Cervical Pain. Alternative therapies in health and medicine. 2018 May:24(3):24-32 [PubMed PMID: 29135458]
Marszałek S, Niebudek-Bogusz E, Woźnicka E, Malińska J, Golusiński W, Śliwińska-Kowalska M. Assessment of the influence of osteopathic myofascial techniques on normalization of the vocal tract functions in patients with occupational dysphonia. International journal of occupational medicine and environmental health. 2012 Jun:25(3):225-35. doi: 10.2478/S13382-012-0041-7. Epub 2012 Jun 22 [PubMed PMID: 22729499]
Mermit B, Durmaz F. Ultrasound shear wave elastography of the sternocleidomastoid muscle in patients with obstructive sleep apnea syndrome. Sleep & breathing = Schlaf & Atmung. 2025 Nov 21:29(6):361. doi: 10.1007/s11325-025-03537-3. Epub 2025 Nov 21 [PubMed PMID: 41269419]
Ono J, Nishi H, Takashima S, Soejima S, Toya R, Kumai Y. Neck stiffness and its correlation with dysphagia after radiotherapy in head and neck cancer. Auris, nasus, larynx. 2025 Dec:52(6):796-802. doi: 10.1016/j.anl.2025.10.011. Epub 2025 Nov 14 [PubMed PMID: 41240671]
Yang R, Wang M, Yang Y, Zhang X, Wu Y, Zhou W, Ding T, Xu J. Biomechanical mechanisms of multidirectional dynamic compensatory muscle fatigue induced by abnormal cervical curvature: a cross-sectional case-control study based on surface electromyography and Cobb angle. Frontiers in sports and active living. 2025:7():1704956. doi: 10.3389/fspor.2025.1704956. Epub 2025 Dec 4 [PubMed PMID: 41427260]
Level 2 (mid-level) evidenceÖzkaçmaz S. Rupture of the sternocleidomastoid muscle: A case report. The Journal of international medical research. 2025 Nov:53(11):3000605251392164. doi: 10.1177/03000605251392164. Epub 2025 Nov 9 [PubMed PMID: 41208019]
Level 3 (low-level) evidenceZhu S, Hong R, Wu Z, Bao Y, Song Y, Hu G, Bai Z, Zhu F, Liao Z, Pan L, Guan Q, Zhang Z, Jin L. Sternocleidomastoid Muscle Overactivity: A Potentially Critical Contributor to Postural Abnormalities in Parkinson's Disease. Annals of neurology. 2025 Nov:98(5):967-976. doi: 10.1002/ana.27310. Epub 2025 Jul 16 [PubMed PMID: 40667758]
Praveen A, Rao K, Gayatri S, Damani AD, Ghoshal A, Nair S, A N Kumar N, Salins SL, Pai A, Singh A, Udupa KS, Usman N, Salins NS. Prevalence, patterns, and impact of myofascial pain in patients with head and neck cancer after cancer treatment - a single-center cross-sectional study in India. BMC palliative care. 2025 Apr 21:24(1):109. doi: 10.1186/s12904-025-01745-y. Epub 2025 Apr 21 [PubMed PMID: 40259373]
Level 2 (mid-level) evidence