 Anatomy, Bony Pelvis and Lower Limb: Distal Tibiofibular Joint (Tibiofibular Syndesmosis)
Anatomy, Bony Pelvis and Lower Limb: Distal Tibiofibular Joint (Tibiofibular Syndesmosis)
Introduction
The distal tibiofibular syndesmosis includes 4 stabilizing ligaments: the anterior-inferior (AITFL) and posterior-inferior (PITFL) tibiofibular ligaments, the inferior transverse ligament (ITL), and the interosseous ligament (IOL), the latter representing a distal continuation of the interosseous membrane (see Image. Lateral Ankle Ligaments).[1] Blood supply to the distal tibiofibular syndesmosis is primarily derived from the fibular artery, with variable contributions from tibial artery branches. Innervation is provided by the deep fibular, tibial, and sural nerves. Anatomical variants include differences in vascular patterns and fibular incisura morphology, influencing syndesmotic stability and surgical outcomes.
Syndesmotic integrity is essential for the maintenance of ankle mortise stability and normal load transmission during gait, while disruption of the distal tibiofibular syndesmosis commonly results in ankle instability, anterolateral pain, and impaired weight-bearing capacity. Surgical management is indicated in cases of syndesmotic instability associated with ankle fractures or isolated ligamentous disruption, with the primary objective of achieving and maintaining anatomic reduction of the fibula within the tibial incisura using fixation methods such as screw or suture button constructs.[2][3] Detailed knowledge of syndesmotic anatomy and biomechanics enables clinicians to improve diagnostic accuracy, optimize interpretation of physical examination and imaging findings, and guide appropriate selection and execution of operative or nonoperative management strategies.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Syndesmotic articulation of the distal tibiofibular joint occurs between the convex surface of the distal fibular tip and the concave fibular notch of the distal tibia. Stability of the syndesmosis is essential for normal dynamic ankle and lower extremity function. Osseous components of the distal tibiofibular syndesmosis include the tibia and fibula, with 4 connecting ligaments that include the AITFL, PITFL, ITL, and IOL.[4] The primary function of the distal tibiofibular syndesmotic ligaments involves the prevention of fibular displacement, including lateral, anterior, and posterior translation from the tibial incisura.[5] Ankle syndesmosis resists pathologic external rotational forces that externally rotate the talus, producing lateral displacement of the fibula relative to the tibia.
The AITFL originates from the longitudinal tubercle on the anterior surface of the lateral malleolus and inserts on the anterolateral tubercle of the tibia (Chaput fragment). This ligament stabilizes the tibia and fibula while preventing excessive fibular displacement and external talar rotation.
The PITFL originates from the posterior tibial tubercle (Volkmann fragment) and attaches to the posterior aspect of the lateral malleolus. The PITFL synergizes with the AITFL to maintain tibiofibular stability.
The ITL lies deep to the PITFL and contributes to the formation of a posterior labrum, deepening the tibial articular surface and enhancing posterior joint stability. The IOL constitutes the distal continuation of the interosseous membrane and functions as a spring-like stabilizer, limiting excessive separation of the tibiofibular mortise during ankle dorsiflexion and heel strike.
Embryology
The limb buds of the embryo typically begin forming approximately 4 to 5 weeks after fertilization, following activation of mesenchymal cells of the lateral plate mesoderm that initiates limb bud outgrowth. Limb bud formation depends on multiple regulatory factors, including activity of the apical ectodermal ridge (AER), HOX genes, retinoic acid, sonic hedgehog (Shh), and the zone of polarizing activity (ZPA). Formation of the AER occurs through thickening of the distal ectodermal border and generates signals that induce rapid, undifferentiated proliferation of the underlying mesenchyme within the progress zone, initiating limb development.
Retinoic acid promotes transcriptional activity and limb growth through upregulation of HOX genes and Shh, resulting in coordinated limb outgrowth along the anteroposterior, dorsoventral, and proximodistal axes. T-box transcription factor 4 (Tbx4), expressed in lower limb development, produces fibroblast growth factor 10, which acts on the AER to stimulate mitosis and further limb elongation.
The ZPA consists of a group of cells located near the posterior aspect of the AER and shifts distally as limb growth progresses. The ZPA secretes signaling molecules that regulate anteroposterior patterning of the developing limb. Shh and fibroblast growth factor signaling enhance HOX gene expression, contributing to limb polarization and regional differentiation. Errors in HOX gene expression and T-box gene regulation result in limb malformations or altered limb morphology.[6]
Blood Supply and Lymphatics
Blood supply to the distal leg includes the anterior and posterior tibial arteries, both branches of the popliteal artery, which originates proximally from the femoral artery and then the external iliac artery. Blood supply to the syndesmotic region itself has not been extensively studied. Published literature describes anatomical variations in the vascular supply to the anterior aspect of the tibiofibular syndesmosis. Reported variants of anterior syndesmotic blood supply include the following:
- Branches arising primarily from the perforating branch of the fibular artery
- Branches arising from the fibular artery, with additional contribution from smaller tibial artery vessels
- Predominant supply from the tibial artery with smaller contributions from the fibular artery [7]
Blood supply to the posterior aspect of the distal tibiofibular syndesmosis demonstrates less anatomical variation. In most cases, vascular supply to the posterior syndesmotic ligaments is derived solely from the fibular artery. In rarer instances, additional contributions from branches of the tibial artery supplements circulation in the region.[8]
Lymphatic vessels of the lower extremity are divided into superficial and deep systems, with further subdivision into medial and lateral groups. Drainage from these channels occurs into the popliteal, deep or superficial inguinal, external iliac, and lumbar lymph nodes.
Nerves
Nerves in the region of the tibiofibular syndesmosis include the deep fibular, tibial, and sural nerves.[9][10] The fibular nerve is a branch of the sciatic nerve and originates at the bifurcation of the sciatic nerve into the common tibial and common fibular nerves, typically at the level of the lower thigh.[11][12] The fibular nerve further divides into a superficial branch, which innervates muscles of the lateral compartment of the leg, and a deep branch, which innervates muscles of the anterior compartment of the leg and the dorsum of the foot. The tibial nerve courses posterior to the tibia and supplies the deep muscles of the posterior compartment of the leg.
Physiologic Variants
Variation in the physiology of the tibiofibular syndesmosis is uncommon. However, 2 recent studies explored anatomic variations related to growth, as well as computed tomography (CT) characterization of morphologic and structural differences in the distal tibiofibular syndesmosis.
Liu et al described inconsistencies in reduction outcomes of the tibiofibular syndesmosis attributed to anatomical variation in the morphology of the fibular incisura of the tibia. Morphologic variation was confirmed using CT imaging, with 5 distinct patterns identified: crescentic, trapezoid, widow’s peak, flat, and chevron. Careful evaluation and measurement using CT imaging to account for these anatomical differences are integral in preventing malreduction of the syndesmosis.[13]
Additionally, Nault et al reported changes in syndesmotic anatomy during growth in young children and adolescents. During skeletal maturation, the fibula demonstrates a slight lateral shift as measured by the tibia–fibula distance at the midfibular incisura, along with a decrease in the external rotation of the fibula.[14] These physiologic variants are important considerations for surgeons during syndesmotic injury management.
Surgical Considerations
Injuries to the distal tibiofibular syndesmosis account for approximately 5% to 10% of ankle sprains and 11% to 20% of ankle fractures. Operative treatment is indicated in cases of confirmed syndesmotic instability, either during intraoperative fixation of an associated ankle fracture or in isolated syndesmotic injury.[15]
Regardless of the surgical technique utilized, the primary goal of syndesmotic repair and fixation is the achievement of anatomic reduction of the distal tibiofibular syndesmosis. Anatomic reduction has been demonstrated to be critical for successful clinical outcomes.[16]
A 2018 meta-analysis comparing suture button fixation and screw fixation for syndesmotic injuries reported improved functional outcomes with suture button fixation, along with lower rates of implant failure and joint malreduction compared with screw fixation.[17][18][19] Similar rates of postoperative complications were otherwise observed between the 2 treatment groups.
Syndesmotic malreduction associated with screw fixation techniques has been reported in up to 52% of cases, with subsequent association with poor functional outcomes. Standard fixation commonly involves placement of two 3.5- or 4.5-mm syndesmotic screws approximately 2 to 5 cm above the ankle joint line. No consistent evidence demonstrates improved outcomes with the use of 1 compared with 2 screws or with specific screw size selection.
Level I evidence generally favors suture button fixation due to lower malreduction rates, fewer implant-related complications, reduced reoperation rates, and potential reduction in long-term osteoarthritis risk. Clinical significance of differences in functional scores remains debated, and cost considerations may influence implant selection, particularly in settings without routine screw removal.
A 2026 review of 19 systematic reviews reported that suture-button fixation consistently produced statistically higher scores on the American Orthopaedic Foot and Ankle Society Scale and the Olerud-Molander Ankle Score. However, most weighted mean differences did not reach minimal clinically important difference thresholds, raising uncertainty regarding the clinical relevance of reported functional improvements.[20]
Clinical Significance
The tibiofibular syndesmosis plays a critical role in ankle stability and load transmission during gait and other weight-bearing activities. Syndesmotic injury commonly presents with ankle instability, difficulty bearing weight, and anterolateral ankle pain.[21]
The external rotation test and the squeeze test are commonly used to assess syndesmotic injury on physical examination. The external rotation test is performed with the patient seated and the knee flexed to 90°, while the foot is gently grasped and externally rotated with the ankle maintained in neutral position. Assessment focuses on pain reproduction and assessment of syndesmotic ligament integrity.
The squeeze test is performed by applying medial-lateral compression to the tibia and fibula in the middle of the leg using the thumb and fingers. Pain elicited during compression is considered a positive finding, suggestive of syndesmotic injury or associated fibular fracture.[22]
External rotation of the talus is the most common mechanism of tibiofibular syndesmotic injury, producing excessive separation of the fibula from the tibia, often followed by hyperdorsiflexion of the foot. Syndesmotic injury constitutes a significant proportion of sports- and physical activity–related ankle injuries and may be difficult to diagnose, contributing to suboptimal functional outcomes. Syndesmotic injuries are associated with prolonged recovery and persistent discomfort. Prolonged recovery has been attributed to potential injury of the perforating fibular artery, the primary vascular supply to the anterior syndesmosis, with subsequent compromise of local perfusion and delayed healing.
The primary goals in the management of syndesmotic injury include restoration of normal fibular length and maintenance of appropriate rotational alignment and anatomic position of the fibula relative to the tibia. Nonoperative treatment strategies have been described with generally favorable outcomes and are typically indicated for isolated syndesmotic sprains without diastasis or significant ankle instability. Nonoperative management may include immobilization in a controlled ankle motion boot or cast with restricted weight-bearing for 2 to 3 weeks, followed by progressive return to weight-bearing activity as tolerated and guided by pain resolution. Consensus regarding optimal management of syndesmotic injury remains limited across preoperative, intraoperative, and postoperative settings, with outcomes largely dependent on careful clinical assessment and individualized treatment planning.
Other Issues
Chronic syndesmotic instability most commonly develops after inadequately treated or missed syndesmotic injuries, persistent diastasis after ankle fracture fixation, failed prior stabilization procedures, or recurrent external rotation trauma in athletes. Progressive ligament attenuation, chronic pain, instability, and persistent widening of the distal tibiofibular joint may ultimately necessitate anatomic ligament reconstruction using tendon autograft or allograft techniques.[23][24]
Tendon grafts used for reconstruction of chronic syndesmotic instability are most commonly harvested from the semitendinosus tendon or gracilis tendon as autografts from the patient, typically from the ipsilateral hamstring. Allograft tissue from the donor semitendinosus tendon may also be used, particularly in revision surgery, poor tissue quality, or extensive ligamentous deficiency.[25]
A 2021 systematic review reported favorable outcomes after autogenous tendon graft reconstruction for chronic distal tibiofibular syndesmotic instability. Across five Level IV studies including 51 patients, postoperative symptoms improved substantially, with restoration of motion and exercise capacity. Postoperative assessment showed American Orthopaedic Foot and Ankle Society scores higher than baseline, increasing from 53 to 89, while visual analog scale pain scores decreased from 82.4 to 12.6. The reported complication rate was 9.8%.[26]
Media
(Click Image to Enlarge)
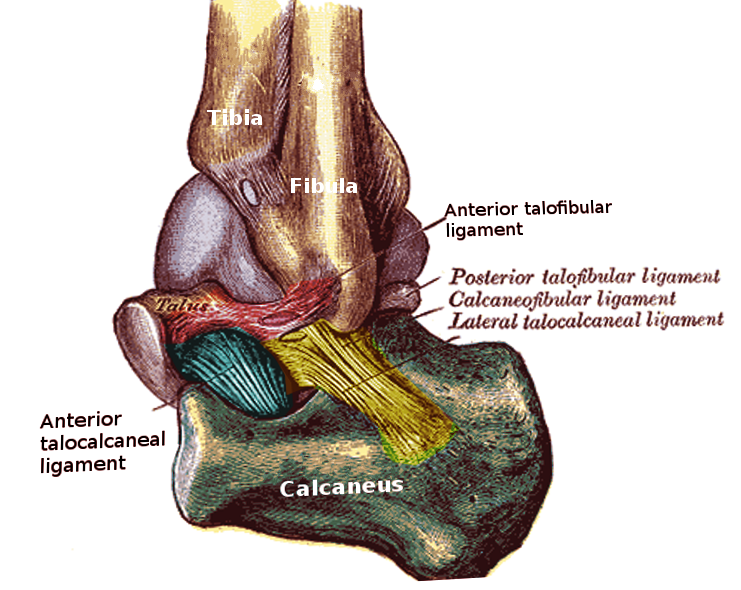
Lateral Ankle Ligaments. This illustration shows the distal tibia and fibula, as well as the talus and calcaneus, with the lateral ankle ligament complex, which includes the anterior talofibular, posterior talofibular, calcaneofibular, lateral talocalcaneal, and anterior talocalcaneal ligaments. Structures contributing to the distal tibiofibular syndesmosis include the distal tibia and distal fibula.
Image courtesy O. Chaigasame
References
Yuen CP, Lui TH. Distal Tibiofibular Syndesmosis: Anatomy, Biomechanics, Injury and Management. The open orthopaedics journal. 2017:11():670-677. doi: 10.2174/1874325001711010670. Epub 2017 Jul 31 [PubMed PMID: 29081864]
Dhillon MS, Patel S, Baburaj V. Ankle Sprain and Chronic Lateral Ankle Instability: Optimizing Conservative Treatment. Foot and ankle clinics. 2023 Jun:28(2):297-307. doi: 10.1016/j.fcl.2022.12.006. Epub 2023 Feb 26 [PubMed PMID: 37137624]
Drakos M, Hansen O, Kukadia S. Ankle Instability. Foot and ankle clinics. 2022 Jun:27(2):371-384. doi: 10.1016/j.fcl.2021.11.025. Epub 2022 May 11 [PubMed PMID: 35680294]
Hermans JJ, Beumer A, de Jong TA, Kleinrensink GJ. Anatomy of the distal tibiofibular syndesmosis in adults: a pictorial essay with a multimodality approach. Journal of anatomy. 2010 Dec:217(6):633-45. doi: 10.1111/j.1469-7580.2010.01302.x. Epub [PubMed PMID: 21108526]
Barham G, Clarke NM. Genetic regulation of embryological limb development with relation to congenital limb deformity in humans. Journal of children's orthopaedics. 2008 Feb:2(1):1-9. doi: 10.1007/s11832-008-0076-2. Epub 2008 Feb 7 [PubMed PMID: 19308596]
Lezak B, Summers S. Anatomy, Bony Pelvis and Lower Limb: Extensor Hallucis Longus Muscle. StatPearls. 2026 Jan:(): [PubMed PMID: 30969697]
Hyland S, Sinkler MA, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Popliteal Region. StatPearls. 2026 Jan:(): [PubMed PMID: 30422486]
McKeon KE, Wright RW, Johnson JE, McCormick JJ, Klein SE. Vascular anatomy of the tibiofibular syndesmosis. The Journal of bone and joint surgery. American volume. 2012 May 16:94(10):931-8. doi: 10.2106/JBJS.K.00604. Epub [PubMed PMID: 22617922]
Khan IA, Mahabadi N, D'Abarno A, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Leg Lateral Compartment. StatPearls. 2026 Jan:(): [PubMed PMID: 30137811]
Binstead JT, Varacallo MA. Anatomy, Bony Pelvis and Lower Limb: Calf. StatPearls. 2026 Jan:(): [PubMed PMID: 29083629]
Miniato MA, Black AC, Varacallo MA. Anatomy, Back, Lumbosacral Trunk. StatPearls. 2026 Jan:(): [PubMed PMID: 30969700]
Hicks BL, Lam JC, Varacallo MA. Piriformis Syndrome. StatPearls. 2026 Jan:(): [PubMed PMID: 28846222]
Liu GT, Ryan E, Gustafson E, VanPelt MD, Raspovic KM, Lalli T, Wukich DK, Xi Y, Chhabra A. Three-Dimensional Computed Tomographic Characterization of Normal Anatomic Morphology and Variations of the Distal Tibiofibular Syndesmosis. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2018 Nov-Dec:57(6):1130-1136. doi: 10.1053/j.jfas.2018.05.013. Epub 2018 Sep 7 [PubMed PMID: 30197255]
Nault ML, Hébert-Davies J, Yen YM, Shore B, Jarrett DY, Kramer DE. Variation of Syndesmosis Anatomy With Growth. Journal of pediatric orthopedics. 2016 Jun:36(4):e41-4. doi: 10.1097/BPO.0000000000000566. Epub [PubMed PMID: 26090974]
Fort NM, Aiyer AA, Kaplan JR, Smyth NA, Kadakia AR. Management of acute injuries of the tibiofibular syndesmosis. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie. 2017 May:27(4):449-459. doi: 10.1007/s00590-017-1956-2. Epub 2017 Apr 8 [PubMed PMID: 28391516]
Park YH, Ahn JH, Choi GW, Kim HJ. Comparison of Clamp Reduction and Manual Reduction of Syndesmosis in Rotational Ankle Fractures: A Prospective Randomized Trial. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2018 Jan-Feb:57(1):19-22. doi: 10.1053/j.jfas.2017.05.040. Epub 2017 Oct 13 [PubMed PMID: 29037926]
Level 1 (high-level) evidenceShimozono Y, Hurley ET, Myerson CL, Murawski CD, Kennedy JG. Suture Button Versus Syndesmotic Screw for Syndesmosis Injuries: A Meta-analysis of Randomized Controlled Trials. The American journal of sports medicine. 2019 Sep:47(11):2764-2771. doi: 10.1177/0363546518804804. Epub 2018 Nov 26 [PubMed PMID: 30475639]
Level 1 (high-level) evidenceKurtoglu A, Kochai A, Inanmaz ME, Sukur E, Keskin D, Türker M, Uysal M, Sen Z, Daldal I. A comparison of double single suture-button fixation, suture-button fixation, and screw fixation for ankle syndesmosis injury: A retrospective cohort study. Medicine. 2021 Apr 2:100(13):e25328. doi: 10.1097/MD.0000000000025328. Epub [PubMed PMID: 33787628]
Level 2 (mid-level) evidenceShevate I, Salunkhe R, Pervez F, Pawar P. A Prospective Study on Fixation of Syndesmotic Ankle Injury: Tight Rope Versus Screw Fixation. Cureus. 2024 Aug:16(8):e67172. doi: 10.7759/cureus.67172. Epub 2024 Aug 19 [PubMed PMID: 39295653]
Nieuwenkamp CL, Tausendfreund J, Schepers T. Suture button versus syndesmotic screw fixation in acute ankle fractures with syndesmotic injury: An umbrella review of functional outcomes and clinical relevance based on the minimal clinically important difference. Injury. 2026 Mar:57(3):113054. doi: 10.1016/j.injury.2026.113054. Epub 2026 Jan 29 [PubMed PMID: 41638088]
Level 1 (high-level) evidenceNorkus SA, Floyd RT. The anatomy and mechanisms of syndesmotic ankle sprains. Journal of athletic training. 2001 Jan-Mar:36(1):68-73 [PubMed PMID: 16404437]
Zalavras C, Thordarson D. Ankle syndesmotic injury. The Journal of the American Academy of Orthopaedic Surgeons. 2007 Jun:15(6):330-9 [PubMed PMID: 17548882]
Sharafeldin K, Eltinay M, Al Qahtani M, Alblaui SM. Ankle syndesmotic reconstruction in chronic ankle syndesmotic injury. BMJ case reports. 2023 Apr 11:16(4):. doi: 10.1136/bcr-2022-251434. Epub 2023 Apr 11 [PubMed PMID: 37041043]
Level 3 (low-level) evidenceGomaa AR, Mason L. Chronic syndesmotic instability - Current evidence on management. Journal of clinical orthopaedics and trauma. 2024 Mar:50():102382. doi: 10.1016/j.jcot.2024.102382. Epub 2024 Feb 23 [PubMed PMID: 38435397]
Mansur H, Danilo da Silva S, Maranho DA. Reconstruction of tibiofibular syndesmosis using autologous semitendinosus graft and lengthening derotational osteotomy of the distal fibula. Journal of clinical orthopaedics and trauma. 2021 Mar:14():80-84. doi: 10.1016/j.jcot.2020.09.013. Epub 2020 Sep 17 [PubMed PMID: 33717900]
Xu HL, Song YJ, Hua YH. Reconstruction of Chronic Injured Distal Tibiofibular Syndesmosis with Autogenous Tendon Graft: A Systematic Review. BioMed research international. 2021:2021():3182745. doi: 10.1155/2021/3182745. Epub 2021 Feb 1 [PubMed PMID: 33604371]
Level 1 (high-level) evidence