 Anatomy, Bony Pelvis and Lower Limb, Foot Muscles
Anatomy, Bony Pelvis and Lower Limb, Foot Muscles
Introduction
A total of 29 muscles are associated with the human foot. Of these muscles, 10 originate proximally, crossing the ankle joint to act upon the foot, while the other 19 lie entirely within the foot. The foot plays a fundamental role in locomotion and postural stability, with its musculature primarily contributing to these functions. The plantar fascia provides structural support, maintaining the posture, contour, and strength of the foot while facilitating the transmission of muscular tension both toward the ground and through the entire musculoskeletal system.
Foot musculature plays a pivotal role in stability, shock absorption, and efficient locomotor mechanics, underscoring its clinical relevance in both orthopedic and neurological disorders. Variations in muscular origin, insertion, or innervation can complicate surgical exposure, alter biomechanical function, and predispose to unexpected complications. Mastery of the anatomy and physiology of the foot muscles is vital for accurate diagnosis, safe intervention, and effective rehabilitation of foot and gait disorders.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Foot Compartments
The foot muscles are organized into 9 compartments enclosed by fascia. However, previous studies on the exact delineation of these compartments have varied considerably.[1][2]
The medial compartment contains the abductor hallucis, flexor hallucis brevis, and the tendon of the flexor hallucis longus. The lateral compartment contains the abductor digiti minimi and flexor digiti minimi. The superficial central compartment includes the flexor digitorum brevis, the 4 lumbricals, and the tendons of the flexor digitorum longus. The deep central (calcaneal) compartment, which communicates with the deep posterior compartment of the lower leg, contains the quadratus plantae and the posterior tibial neurovascular bundle. The adductor compartment contains the adductor hallucis.
Four interosseous compartments exist. The 1st lies between the 1st and 2nd metatarsals and contains the 1st dorsal interosseous muscle. The 2nd lies between the 2nd and 3rd metatarsals and contains both the dorsal and plantar interosseous muscles. The 3rd and 4th lie between the 3rd and 4th, and 4th and 5th metatarsals, respectively, and also contain the dorsal and plantar interosseous muscles.[3][4][5][6]
Foot musculature may also be categorized as extrinsic, originating outside the foot, or intrinsic, originating within the foot.[7][8][9] The intrinsic muscles are further divided into dorsal and plantar groups, with the plantar muscles arranged in 4 distinct layers.
Extrinsic Muscles of the Foot
Extrinsic foot muscles arise from the tibia, fibula, and surrounding structures of the lower leg, extending distally to act on the foot (see Image. Tendons of the Extrinsic Foot Muscles). These muscles enable plantarflexion, dorsiflexion, inversion, and eversion, thereby supporting weight-bearing and dynamic postural adjustments. Table 1 summarizes the origins, insertions, actions, blood supply, and innervation of the major extrinsic muscles of the foot (see Table 1. Overview of the Extrinsic Foot Muscles).
Table 1. Overview of the Extrinsic Foot Muscles
| Leg Compartment | Muscle | Origin | Insertion | Action | Blood Supply | Innervation |
| Lateral compartment | Fibularis longus | Head and superior 1/2 of fibula | Posterolateral medial cuneiform and lateral base of 1st metatarsal | Eversion, plantarflexion, supports transverse arch | Anterior tibial artery | Superficial fibular nerve |
| Fibularis brevis | Inferior 2/3 lateral fibula | Styloid process of 5th metatarsal | Eversion, plantarflexion | Fibular artery | Superficial fibular nerve | |
| Anterior compartment | Fibularis tertius | Inferior 1/3 of middle fibular shaft; interosseous membrane | Dorsal surface of 5th metatarsal | Dorsiflexion, eversion, abduction | Anterior tibial artery | Deep fibular nerve |
| Tibialis anterior | Lateral condyle and proximal 1/2 of tibial shaft; superomedial fibula; interosseous membrane | Medial and plantar surfaces of medial cuneiform and base of 1st metatarsal | Dorsiflexion, inversion | Anterior tibial artery | Deep fibular nerve | |
| Extensor hallucis longus | Middle anterior fibula and interosseous membrane | Dorsal aspect of distal phalanx of great toe | Extends great toe; dorsiflexes foot | Anterior tibial artery | Deep fibular nerve | |
| Extensor digitorum longus | Lateral tibial condyle and superomedial surface of fibula; interosseous membrane | Dorsum of middle and distal phalanges 2-5 | Extends digits 2-5; assists dorsiflexion | Anterior tibial artery | Deep fibular nerve | |
| Superficial posterior compartment | Gastrocnemius | Medial and lateral femoral condyles | Joins soleus to form Achilles tendon, inserting on calcaneus | Plantarflexion | Sural branch of popliteal artery | Tibial nerve |
| Soleus | Upper 1/4 posterior fibula and middle posterior tibia | Joins gastrocnemius to form Achilles tendon, inserting on calcaneus | Plantarflexion | Posterior tibial, fibular, sural arteries | Tibial nerve | |
| Deep posterior compartment | Tibialis posterior | Superior 2/3 medial posterior tibia; posterior fibula; interosseous membrane | Superficial: navicular tuberosity, cuneiform, and cuboid; Deep: plantar surfaces of 2nd-4th metatarsals | Inversion, adduction, plantarflexion; aids supination | Sural, fibular, posterior tibial arteries | Tibial nerve |
| Flexor hallucis longus | Inferior 2/3 posterior fibula; inferior aspect of interosseous membrane | Plantar surface of distal phalanx of great toe | Flexes great toe; minimal supination and plantarflexion | Fibular and posterior tibial arteries | Tibial nerve | |
| Flexor digitorum longus | Posterior tibia distal to soleal line | Plantar surfaces of distal phalanges 2-5 | Flexes digits 2-5; may aid plantarflexion | Posterior tibial artery | Tibial nerve |
From the lateral leg compartment
The lateral compartment of the leg encases the fibularis longus and fibularis brevis muscles. Both are primarily involved in foot eversion and plantarflexion.
The fibularis longus originates from the head and proximal 1/2 of the fibula. The muscle's tendon passes posterior to the lateral malleolus and inserts onto the posterolateral aspect of the medial cuneiform and the lateral surface of the base of the 1st metatarsal. In addition to contributing to eversion and plantarflexion, the fibularis longus reinforces the transverse arch of the foot. The muscle receives vascular supply mainly from branches of the anterior tibial artery and is innervated by the superficial fibular nerve.
The fibularis brevis arises from the distal 2/3 of the fibula’s lateral surface and attaches to the styloid process of the 5th metatarsal. The muscle assists the fibularis longus in foot eversion and plantarflexion. The fibular artery provides the principal blood supply, and the superficial fibular nerve supplies motor innervation.
From the anterior leg compartment
The anterior compartment of the leg comprises the fibularis tertius, tibialis anterior, extensor hallucis longus, and extensor digitorum longus muscles. Collectively, these muscles facilitate dorsiflexion of the foot, with additional roles in toe extension, inversion, eversion, and abduction.
The fibularis tertius originates from the inferior 1/3 of the middle fibular shaft and the interosseous membrane. Insertion occurs on the dorsal surface of the 5th metatarsal. The muscle contributes to dorsiflexion, eversion, and abduction of the foot. Vascular supply is derived from the anterior tibial artery, and innervation arises from the deep fibular nerve.
The tibialis anterior emerges from the lateral condyle and proximal 1/2 of the tibial shaft, the superomedial surface of the fibula, and the interosseous membrane. The tendon inserts onto the medial and plantar segments of the medial cuneiform and the base of the 1st metatarsal. The muscle produces dorsiflexion and inversion of the foot. The anterior tibial artery provides blood supply, and the deep fibular nerve provides motor innervation.
The extensor hallucis longus emanates from the middle anterior margin of the fibula and the interosseous membrane and inserts on the dorsal portion of the distal phalanx of the great toe. The muscle extends the great toe and assists in dorsiflexion of the foot. The anterior tibial artery perfuses the muscle. The deep fibular nerve provides motor fibers.
The extensor digitorum longus originates from the lateral tibial condyle, the superomedial surface of the fibula, and the interosseous membrane. Insertion occurs on the dorsal surfaces of the distal and middle phalanges of the lateral 4 toes. The muscle extends the lateral 4 toes and aids foot dorsiflexion. The anterior tibial artery provides circulation. The deep fibular nerve supplies motor input.
From the superficial posterior leg compartment
The superficial posterior leg compartment houses the gastrocnemius and soleus muscles. Both are primarily responsible for plantarflexion of the foot.
The gastrocnemius extends from the medial and lateral femoral condyles. The muscle's tendon merges with that of the soleus, forming the Achilles tendon, which inserts onto the calcaneus. The sural branch of the popliteal artery perfuses the gastrocnemius. Motor innervation is via the tibial nerve.
The soleus arises from the upper 1/4 of the posterior fibula and the middle posterior surface of the tibia. The tendon of this muscle fuses with the gastrocnemius tendon to form the Achilles tendon, which inserts on the calcaneus. Perfusion is supplied by the posterior tibial, fibular, and sural arteries, while the tibial nerve provides motor input.
From the deep posterior leg compartment
The deep posterior leg compartment contains the tibialis posterior, as well as the flexor hallucis longus and flexor digitorum longus. Collectively, these muscles contribute to plantarflexion, inversion, adduction, toe flexion, and support of foot supination.
The tibialis posterior originates from the superior 2/3 of the medial posterior tibia, the posterior fibula, and the interosseous membrane. The muscle's superficial tendon inserts on the navicular tuberosity, cuneiforms, and cuboid, while its deep tendon attaches to the plantar surfaces of the 2nd to 4th metatarsals. The tibialis posterior performs inversion, adduction, and plantarflexion, aiding foot supination. The sural, fibular, and posterior tibial arteries supply circulation. The tibial nerve provides motor input.
The flexor hallucis longus arises from the inferior 2/3 of the posterior fibula and the inferior aspect of the interosseous membrane. This muscle inserts on the plantar surface of the distal phalanx of the 1st digit, flexing the digit and contributing minimally to supination and plantarflexion. Perfusion is derived from the fibular and posterior tibial arteries. The tibial nerve supplies motor fibers.
The flexor digitorum longus originates from the posterior tibia distal to the soleal line and inserts on the plantar margins of the distal phalanges of digits 2 to 5. The muscle flexes these digits and may assist in plantarflexion. Perfusion emanates from the posterior tibial artery, with motor innervation from the tibial nerve.
Dorsal Intrinsic Muscles of the Foot
Intrinsic muscles on the dorsal surface of the foot originate and insert within the foot itself. These muscles are confined to the dorsal aspect of the foot and act locally on the toes. The dorsal intrinsic muscles facilitate extension of the digits and contribute to stabilization of the forefoot and the metatarsophalangeal (MTP) joints during weight-bearing activities (see Image. Muscles of the Anterior Leg Compartment and the Foot Dorsum). Table 2 outlines the key anatomical features and actions of the dorsal intrinsic muscles of the foot (see Table 2. Overview of the Dorsal Intrinsic Foot Muscles).
Table 2. Overview of the Dorsal Intrinsic Foot Muscles
| Muscle | Origin | Insertion | Action | Blood Supply | Innervation |
| Extensor digitorum brevis | Dorsolateral surface of calcaneus, inferior extensor retinaculum, talocalcaneal interosseous ligament | Extensor expansions of the tendons of extensor digitorum longus to toes 2-4 (lateral 3 toes) | Extends digits 2-4 | Fibular artery, anterior tibial artery, dorsalis pedis artery | Deep fibular nerve |
| Dorsal interossei (4 muscles) | Adjacent sides of metatarsals 1-5 | Bases of proximal phalanges and extensor expansions of toes 2-4 | Abduction of toes 2-4 at MTP joints; assists in flexion and extension | Dorsalis pedis, plantar metatarsal arteries, lateral plantar artery | Lateral plantar nerve |
| Extensor hallucis brevis | Dorsal surface of calcaneus (superolateral to extensor digitorum brevis origin) | Base of proximal phalanx of great toe | Extends great toe | Dorsalis pedis artery | Deep fibular nerve |
Extensor digitorum brevis
The extensor digitorum brevis extends from the dorsolateral surface of the calcaneus, the inferior extensor retinaculum, and the talocalcaneal interosseous ligament. The muscle's tendon attaches to the extensor expansions of the extensor digitorum longus tendons for toes 2 to 4, facilitating extension of the lateral 3 digits. The fibular, anterior tibial, and dorsalis pedis arteries perfuse the muscle. The deep fibular nerve supplies motor innervation.
Dorsal interossei
The 4 dorsal interossei arise from the adjacent sides of metatarsals 1 to 5. These muscles insert onto the bases of the proximal phalanges and extensor expansions of toes 2 to 4 (see Image. Dorsal Interossei of the Foot). The dorsal interossei abduct toes 2 to 4 at the MTP joints and assist in both flexion and extension. The dorsalis pedis, plantar metatarsal, and lateral plantar arteries supply the muscle. Motor input comes from the lateral plantar nerve.
Extensor hallucis brevis
The extensor hallucis brevis originates from the dorsal surface of the calcaneus, superolateral to the origin of the extensor digitorum brevis. The muscle's tendon inserts onto the base of the proximal phalanx of the 1st digit, producing extension of the digit. Perfusion is via the dorsalis pedis artery. The deep fibular nerve innervates the muscle.
Plantar Intrinsic Muscles of the Foot
Muscles in this group are located on the foot sole and primarily function to support the arches and facilitate toe movements. The plantar intrinsic foot muscles are organized into 4 distinct layers based on their depth and anatomical relationships. Table 3 provides an overview of the 4 layers of plantar intrinsic foot muscles, including their structure, function, and neurovascular supply (see Table 3. Overview of the Plantar Intrinsic Foot Muscles).
Table 3. Overview of the Plantar Intrinsic Foot Muscles
| Layer | Muscle | Origin | Insertion | Action | Blood Supply | Innervation |
| 1st | Abductor hallucis | Calcaneal tuberosity; flexor retinaculum; plantar aponeurosis | Base and proximal phalanx of great toe | Abduction of great toe | Medial plantar artery | Medial plantar nerve |
| Flexor digitorum brevis | Calcaneal tuberosity; plantar aponeurosis; intermuscular septa | Middle phalanges of digits 2-5 | Flexion of digits 2-5 | Medial plantar artery | Medial plantar nerve | |
| Abductor digiti minimi | Calcaneal tuberosity; plantar aponeurosis; intermuscular septa | Base of 5th metatarsal | Abduction of 5th digit | Lateral plantar artery | Lateral plantar nerve | |
| 2nd | Quadratus plantae | Plantar surface of calcaneus | Tendon of flexor digitorum longus | Assists in flexion of distal phalanges | Lateral plantar artery | Lateral plantar nerve |
| Lumbricals (4 muscles) | Tendons of flexor digitorum longus | Medial aspect of extensor expansions (extensor hoods) on proximal phalanges of digits 2-5 | Flexion of MTP joints and extension of interphalangeal joints of digits 2-5 | Medial and lateral plantar arteries | 1st lumbrical: medial plantar nerve; 2nd-4th lumbricals: lateral plantar nerve | |
| 3rd | Flexor hallucis brevis | Cuboid and lateral cuneiform | Proximal phalanx of great toe via medial and lateral tendons | Flexion of great toe | Medial plantar artery | Medial plantar nerve |
| Adductor hallucis | Oblique head: base of metatarsals 2-4; Transverse head: MTP ligaments of digits 3-5 | Proximal phalanx of great toe | Adduction of great toe | 1st plantar metatarsal artery | Deep branch of lateral plantar nerve | |
| Flexor digiti minimi brevis | Base of 5th metatarsal | Proximal phalanx of 5th digit | Flexion of 5th digit | Lateral plantar artery | Lateral plantar nerve | |
| 4th | Plantar interossei (3 muscles) | Medial side of metatarsals 3-5 | Proximal phalanges of digits 3-5 | Adduction and flexion of digits; assist lumbricals in extension of interphalangeal joints | Plantar metatarsal artery | Lateral plantar nerve |
First layer
The 1st layer of plantar muscles includes the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi. These muscles contribute to toe abduction and flexion (see Image. Plantar Foot Anatomy, First Layer).
The abductor hallucis arises from the calcaneal tuberosity, the flexor retinaculum, and the plantar aponeurosis. The muscle's tendon inserts on the base and proximal phalanx of the great toe, producing abduction of the digit. The medial plantar artery supplies circulation, and the medial plantar nerve provides motor input.
The flexor digitorum brevis originates from the calcaneal tuberosity, plantar aponeurosis, and intermuscular septa. The muscle inserts onto the middle phalanges of digits 2 to 5, enabling flexion of these toes. The medial plantar artery provides circulation, and motor innervation comes from the medial plantar nerve.
The abductor digiti minimi arises from the calcaneal tuberosity, plantar aponeurosis, and intermuscular septa. This muscle's tendon attaches to the base of the 5th metatarsal, producing abduction of the 5th digit. Perfusion is supplied by the lateral plantar artery, with motor input from the lateral plantar nerve.
Second layer
The 2nd layer of plantar muscles comprises the quadratus plantae and the 4 lumbricals. These muscles aid in toe flexion and coordinated motion of the MTP and interphalangeal joints (see Image. Plantar Foot Anatomy, Second Layer).
The quadratus plantae originates from the plantar surface of the calcaneus and inserts onto the tendon of the flexor digitorum longus, assisting in flexion of the distal phalanges. Perfusion is supplied by the lateral plantar artery, and motor input is provided by the lateral plantar nerve.
The lumbricals extend from the tendons of the flexor digitorum longus and attach to the medial aspects of the extensor expansions on the proximal phalanges of digits 2 to 5. These muscles flex the MTP joints while extending the interphalangeal joints of toes 2 through 5. Perfusion is supplied by the medial and lateral plantar arteries. Motor innervation is provided by the medial plantar nerve for the 1st lumbrical and the lateral plantar nerve for the 2nd through 4th lumbricals.
Third layer
The 3rd layer of plantar muscles comprises the flexor hallucis brevis, adductor hallucis, and flexor digiti minimi brevis. This group contributes to toe flexion and adduction (see Image. Plantar Foot Anatomy, Third Layer).
The flexor hallucis brevis originates from the cuboid and lateral cuneiform. The muscle's dual tendons insert onto the proximal phalanx of the great toe, producing flexion of the digit. The medial plantar artery supplies the flexor hallucis brevis. The medial plantar nerve provides motor input.
The adductor hallucis consists of an oblique head, arising from the bases of metatarsals 2 to 4, and a transverse head, originating from the MTP ligaments of digits 3 to 5. Both heads insert on the proximal phalanx of the great toe, facilitating adduction of the digit. Perfusion is provided by the 1st plantar metatarsal artery, with motor innervation supplied by the deep branch of the lateral plantar nerve.
The flexor digiti minimi brevis arises from the base of the 5th metatarsal and inserts onto the proximal phalanx of the 5th digit, producing flexion. The lateral plantar artery supplies perfusion, and the lateral plantar nerve provides motor input.
Fourth layer
Situated within the foot’s 4th muscular layer, the 3 plantar interossei muscles originate from the medial sides of metatarsals 3 to 5 and insert onto the proximal phalanges of the corresponding digits (see Image. Plantar Interossei of the Foot). These muscles adduct and flex toes 3 to 5 and assist the lumbricals in extending the interphalangeal joints. The plantar metatarsal artery supplies circulation. The lateral plantar nerve provides motor fibers.
Embryology
Limb development begins during the 4th postovulatory week, corresponding to embryonic stage 13 (3-6 mm in length).[10] Limb formation progresses in a proximodistal direction, with the foot appearing at approximately 4.5 weeks (embryonic stage 15). The cartilaginous skeleton and associated musculature become visible within days, followed shortly by the appearance of the digits (embryonic stage 18-19). Skeletal elements initially form as mesodermal condensations, which subsequently organize in a defined sequence. Ossification proceeds via the formation of a periosteal collar in tubular bones. Vascularization of the tarsal bones occurs during the fetal period, whereas endochondral ossification in certain tarsal bones does not commence until after birth.
The limbs originate from the proliferation of the somatopleuric mesoderm in the lateral body wall. These outgrowths form at the lumbar region corresponding to the 3rd through 5th lumbar somites for the hind limbs.[11]
Blood Supply and Lymphatics
The primary arterial supply to the foot originates from the popliteal artery, which is a continuation of the superficial femoral artery. The popliteal artery gives rise to 3 principal branches supplying the lower leg and foot, arranged from proximal to distal as the anterior tibial, fibular, and posterior tibial arteries (see Image. Arteries of the Lower Limb, Anterior and Posterior Views). The anterior tibial artery courses distally to supply the anterior and dorsal regions of the foot. After passing beneath the extensor retinaculum, this blood vessel continues as the dorsalis pedis artery, which is commonly palpated for the pedal pulse. The dorsalis pedis courses under the extensor hallucis longus and lies between this muscle and the extensor digitorum longus.
The dorsalis pedis gives rise to 3 lateral branches—the proximal tarsal, distal tarsal, and arcuate arteries—and 2 medial branches, the medial tarsal arteries. The arcuate artery originates at the level of the 1st tarsal-metatarsal joint and courses over metatarsals 2 to 4, giving rise to the 2nd, 3rd, and 4th dorsal metatarsal arteries. The 1st dorsal metatarsal artery arises directly from the dorsalis pedis. These metatarsal branches perfuse the dorsal interosseous muscles. The fibular artery supplies the lateral leg musculature and the posterior aspect of the foot. The posterior tibial artery provides circulation to the posterior and lateral leg as well as the plantar surface of the foot.
The posterior tibial artery bifurcates deep to the abductor hallucis into medial and lateral plantar branches. The medial plantar artery supplies the medial plantar surface and the hallux, whereas the larger lateral plantar artery traverses the sole to form the plantar arterial arch by uniting with the deep plantar branch of the dorsalis pedis artery. The arch gives rise to the plantar metatarsal arteries, which continue distally as the proper digital arteries to the toes (see Image. Plantar Foot Anatomy, Arterial Supply).
The lower limb's venous system consists of deep veins, which run between the muscles, and superficial veins, forming an intricate network immediately beneath the skin. These 2 systems are interconnected by valved transfascial vessels, the perforating veins, which direct approximately 10% of superficial blood flow into the deep venous system.
In the plantar region, a network of intertwined superficial and deep veins functions as a compressible reservoir, which is emptied with each step during ground contact. This mechanism facilitates the propulsion of blood from the foot toward the calf.
Venous return originates in the microcirculation, where arterial capillaries transition to venous capillaries. These blood vessels converge into collecting venules and, subsequently, into collecting veins, forming the initial efferent pathway of the macrocirculatory venous system.
In the anterior region, the dorsal venous network of the foot communicates through intercapitular veins that traverse the interdigital spaces. Digital veins, converging in pairs within the interdigital spaces, give rise to the metatarsal veins, which course into the deep plantar venous arch and subsequently converge in the lateral plantar veins. After posterior convergence with the medial plantar veins, the lateral plantar veins form the 2 posterior tibial veins. The anterior tibial veins originate from the deep veins of the dorsal foot. The medial marginal vein, rising anterior to the medial malleolus, empties into the great saphenous vein, whereas the lateral marginal vein, coursing anterior to the lateral malleolus, drains toward the small saphenous vein.
Lymphatic drainage of the lower extremities originates in the foot, where lymph nodes are classified as superficial (epifascial) or deep (subfascial). The epifascial and subfascial networks are interconnected by anastomoses. The epifascial system primarily drains the skin and subcutaneous tissues, while the subfascial system drains joints, muscles, and bones.[12] The major portion of epifascial collectors forms a ventromedial bundle over the dorsum of the foot, which empties into the superficial inguinal nodes, whereas a smaller dorsal bundle drains initially into the popliteal nodes.[13] The subfascial nodes drain into the deep inguinal nodes.
Nerves
The sciatic nerve constitutes the principal source of innervation for the lower extremity. This nerve emerges from the lumbosacral plexus and passes beneath the piriformis muscle before coursing distally. At the distal 1/3 of the femur, the sciatic nerve ramifies into the tibial and common fibular nerves. The tibial nerve descends distally, branching into the medial calcaneal, medial sural cutaneous, and medial and lateral plantar nerves (see Image. Plantar Foot Anatomy, Innervation). The common fibular nerve diverges into the superficial and deep fibular nerves. The superficial fibular nerve primarily provides cutaneous innervation to the dorsum of the foot, whereas the deep fibular nerve supplies motor fibers to the muscles responsible for foot dorsiflexion.[14][15]
Physiologic Variants
Tibialis Anterior Tendon
Variability exists in the insertion of the tibialis anterior tendon, which may give rise to potential alterations in force distribution across the foot and ankle. These differences become particularly relevant during tibialis anterior tendon ruptures, where restoration of tendon biomechanics may require alignment with the native insertion pattern.
Accessory Fibular Muscles
The fibularis quartus is an accessory muscle present in 6% to 22% of individuals, depending on the study. This muscle most commonly originates from the fibularis brevis, although origins from the fibularis tertius and longus have been reported. Insertion points vary, including the cuboid, lateral tubercle of the calcaneus, apophysis of the calcaneal cochlea, or the retrotrochlear eminence of the calcaneus. In some cases, the muscle gives rise to a tendon that inserts on the 5th digit, referred to as the "fibularis digiti quinti," which may assist in the extension of this digit.[16]
The presence of a fibularis quartus has been associated with lateral ankle pathology. Symptomatic individuals may present with chronic ankle pain in the absence of trauma. Additional reported pathologies include fibular tendon subluxation, tendinous calcification, and hypertrophy of the retrotrochlear eminence of the calcaneus, contributing to lateral hindfoot pain.[17]
Accessory Soleus Muscle
The accessory soleus muscle is an anatomical variant located anterior or anteromedial to the Achilles tendon, originating from the fibula, soleus, or tibia and inserting on the Achilles tendon or calcaneus. Prevalence ranges from 0.7% to 5.5% in the general population, though this variant is generally considered rare. An accessory soleus muscle may be asymptomatic or cause pain, swelling, exertional compartment syndrome, and neurovascular compression. Clinically, this variant can mimic soft-tissue tumors. Medical management involves activity modification, while surgical excision is indicated for persistent pain, functional limitation, or compartment syndrome, with careful dissection to prevent injury to surrounding tendons and neurovascular structures.[18][19]
Surgical Considerations
Foot Drop
Foot drop is a condition marked by weakness or paralysis of the muscles responsible for ankle dorsiflexion, often resulting in a steppage gait and functional impairment. In many cases, foot drop arises iatrogenically from surgical injury to the deep fibular nerve or its branches during procedures involving the foot, ankle, or distal leg. Surgical interventions, including neurolysis, nerve repair, and tendon transfers, are employed to restore motor function, depending on the severity and chronicity of nerve damage. Early identification and tailored operative management can significantly improve functional outcomes and reduce long-term disability.[20]
Foot Reconstruction Using Muscle Flaps
Foot muscle flap surgeries use vascularized muscle tissue to reconstruct soft-tissue defects over bone, tendon, or joint exposures. Examples include the abductor hallucis muscle flap, typically used for medial-column or 1st MTP joint defects, and the flexor hallucis brevis muscle flap, applied to cover forefoot soft tissue injuries.[21][22] Intrinsic muscle flaps are suitable for smaller defects, often combined with split-thickness skin grafts to enhance healing. Indications include chronic ulcers, osteomyelitis, and trauma.[23] Microsurgical free muscle transfers are employed for extensive defects when local flaps are insufficient, allowing vascularized tissue coverage and functional restoration.[24]
Risks of Dorsalis Pedis Artery Anomalies
Variations in the origin, course, and branching of the dorsalis pedis artery are observed in approximately 20% to 30% of examined feet, including absence, lateral deviation, duplication, or replacement by a branch of the fibular artery.[25] The plantar arterial arch shows variability in completeness and the dominant contributor. Cadaveric studies indicate that the plantar arterial arch is usually complete, with variable dominance of the lateral plantar artery or the deep plantar branch of the dorsalis pedis artery. In some cases, both vessels contribute roughly equally to the arch.[26]
Unrecognized variation may lead to unexpected ischemia, arterial disruption in dorsal-midfoot surgery, or flap reconstruction failure in the forefoot.[27] Preoperative imaging can help prevent intraoperative vascular complications.
Clinical Significance
Muscles acting directly on or surrounding the foot mediate multiple functions essential for normal gait and postural stability. Injury to these muscles can lead to conditions that impair the performance of activities of daily living. Common disorders associated with foot musculature include Achilles tendon rupture, hammer toe, and pes planus (flat foot), each presenting with variable functional impairment and potential comorbidities. Management strategies are determined by the severity of the condition and the patient's age. For instance, conservative nonoperative treatment of Achilles tendon rupture has demonstrated outcomes comparable to surgical intervention in older patients.[28]
Other Issues
Flexor Hallucis Longus Transfer for Achilles Rupture
Chronic Achilles tendon rupture includes cases where the rupture persists or is untreated for more than 4 weeks following the initial injury, resulting in tendon retraction, poor vascularization, and atrophic tendon ends. The condition often arises from missed acute injuries and is increasingly common in adults aged 30 to 40. Weak plantarflexion persists due to compensation by tibialis posterior, peroneus, flexor hallucis longus, and flexor digitorum longus, causing impaired gait and push-off strength.
Surgical management via single-incision flexor hallucis longus tendon transfer addresses large tendon defects (>5 cm), restoring ankle function and daily activity. Benefits include low rerupture rates and significant functional improvement. Risks involve hallux plantarflexion weakness, wound complications, and rare nerve injury. Long-term follow-up demonstrates high patient satisfaction and durable correction in the majority of cases.[29]
Overuse Injuries from Ballet Training
Recurrent plantarflexion, forefoot elevation (relevé), and sustained distal toe loading (en pointe) contribute to foot and ankle overuse injuries in ballet dancers. Common conditions include Achilles tendinopathy, plantar fasciitis, metatarsal stress fractures, hallux valgus, and claw or hammer toes. Movements that require extreme dorsiflexion and toe extension overload the intrinsic foot muscles, flexor hallucis longus, gastrocnemius-soleus complex, and tibialis posterior. Repeated en pointe activity particularly stresses the medial longitudinal arch and 1st MTP joint. Preventive strategies include targeted strengthening, gradual load progression, proper technique, and structured rest.[30]
Media
(Click Image to Enlarge)
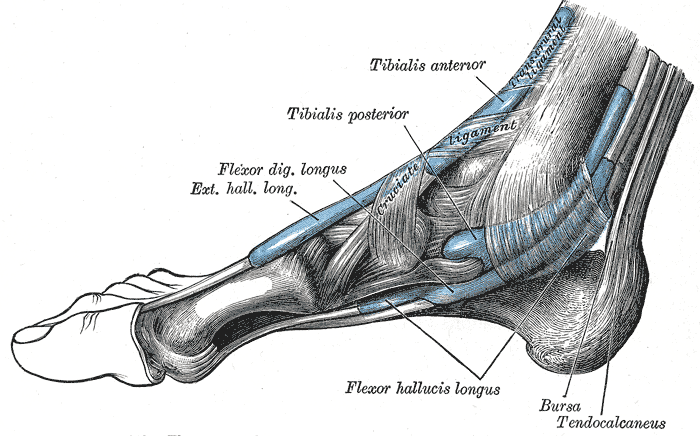
Tendons of the Extrinsic Foot Muscles. This medial view of the right foot shows the tendons of the tibialis anterior, tibialis posterior, flexor digitorum longus, extensor hallucis longus, and flexor hallucis longus. The retrocalcaneal bursa, tendo calcaneus (Achilles tendon), and transcrural and cruciate ligaments are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
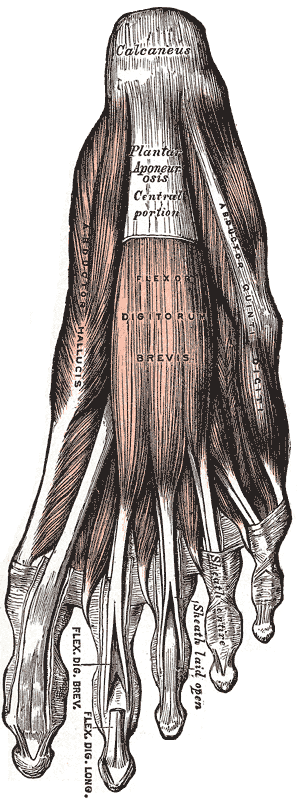
Plantar Foot Anatomy, First Layer. This illustration depicts the superficial dissection of the foot sole. Visible and labeled structures include the calcaneus, plantar aponeurosis (central portion), abductor hallucis, flexor digitorum brevis, flexor digitorum longus tendons, abductor digiti minimi (abductor quinti digiti), and the sheath for the flexor tendon. The key muscles, tendons, and aponeurotic layers are identified for anatomical orientation and educational use.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)

Plantar Foot Anatomy, Third Layer. This illustration displays the 3rd muscular layer of the foot sole. Labeled anatomical structures include the adductor hallucis (oblique and transverse heads), flexor hallucis brevis, plantar aponeurosis, tibialis posterior tendon, sheath of peroneus longus tendon, flexor digiti quinti brevis, and the sesamoid bone location. The diagram highlights muscles, tendons, and supporting connective tissues that contribute to hallux stability, lateral toe flexion, and foot arch structure. Structures are clearly identified for orientation and instructional reference.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
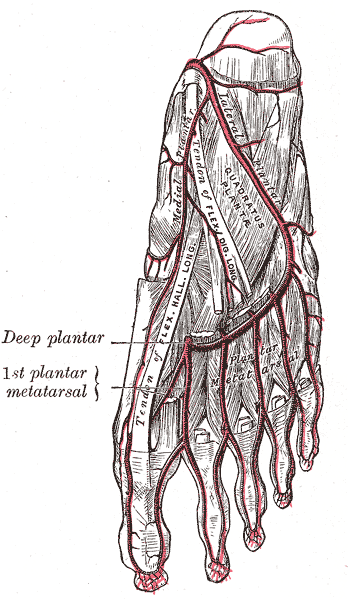
Plantar Foot Anatomy, Arterial Supply. This illustration depicts the arterial network of the plantar surface of the foot. Labeled vascular structures include the medial plantar artery, lateral plantar artery, and plantar metatarsal arteries branching from the plantar arch. Additional identified structures include the quadratus plantae muscle and associated tendons and connective tissues of the sole, demonstrating their anatomical relationships to the plantar vascular network. The diagram emphasizes the organization of deep plantar circulation and its spatial relation to surrounding musculature for anatomical and clinical reference.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
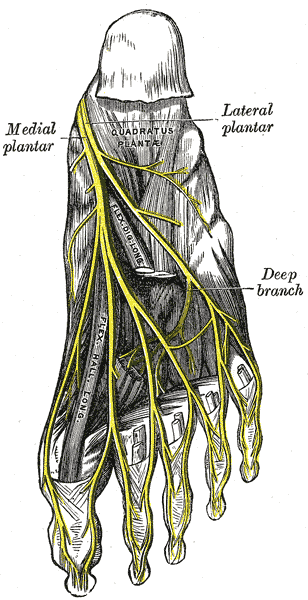
Plantar Foot Anatomy, Innervation. This illustration depicts the branching of the tibial nerve into the medial plantar nerve and the lateral plantar nerve. The lateral plantar nerve gives rise to a deep branch that curves medially. Crucial nonneural structures, such as the quadratus plantae muscle and the tendons of the flexor digitorum longus and flexor hallucis longus, demonstrate their anatomical relationships to the deep plantar innervation.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
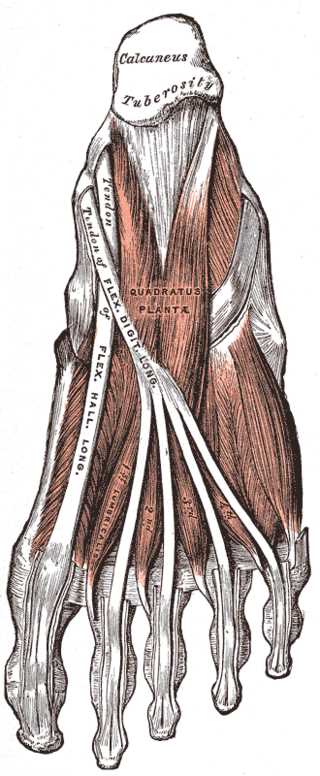
Plantar Foot Anatomy, Second Layer. This illustration highlights the 2nd muscular layer of the plantar aspect of the foot. Labeled anatomical structures include the calcaneus, tuberosity of the calcaneus, quadratus plantae, tendon of flexor digitorum longus, tendon of flexor hallucis longus, and the 4 lumbrical muscles (numbered 1 to 4). Major muscles, deep flexor tendons, and lumbricals are shown in anatomical relation, illustrating structures that assist in toe flexion and foot stability.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
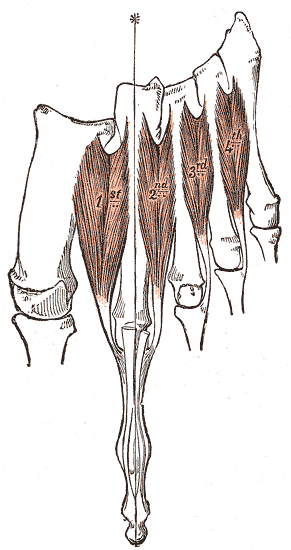
Dorsal Interossei of the Foot. This illustration depicts the 4 dorsal interossei muscles (labeled 1st, 2nd, 3rd, and 4th) located between the metatarsal bones on the dorsal side of the foot. These muscles originate from the opposing sides of adjacent metatarsals 1 to 5 and insert onto the bases of the proximal phalanges and the extensor expansions. Specifically, the 1st dorsal interosseous inserts onto the medial base of the 2nd toe; the 2nd to 4th muscles insert onto the lateral bases of the 2nd, 3rd, and 4th toes. The main action of these muscles is abduction of toes 2 to 4 away from the longitudinal axis of the 2nd toe, as indicated by the asterisk. The dorsal interossei also contribute to toe flexion at the metatarsophalangeal joints and extension at the interphalangeal joints.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
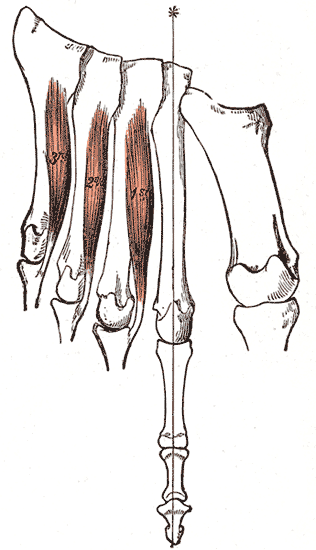
Plantar Interossei of the Foot. This illustration depicts the 3 plantar interossei muscles (1st, 2nd, and 3rd) located on the plantar surface of the foot. These muscles originate from the medial aspects of the 3rd, 4th, and 5th metatarsal bones and insert onto the medial bases of the proximal phalanges (and extensor expansions) of digits 3, 4, and 5. The primary function of these muscles is adduction of the 3rd to 5th toes toward the longitudinal axis of the second toe, as indicated by the asterisk. The muscles additionally assist in flexion at the metatarsophalangeal joints and extension at the interphalangeal joints.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
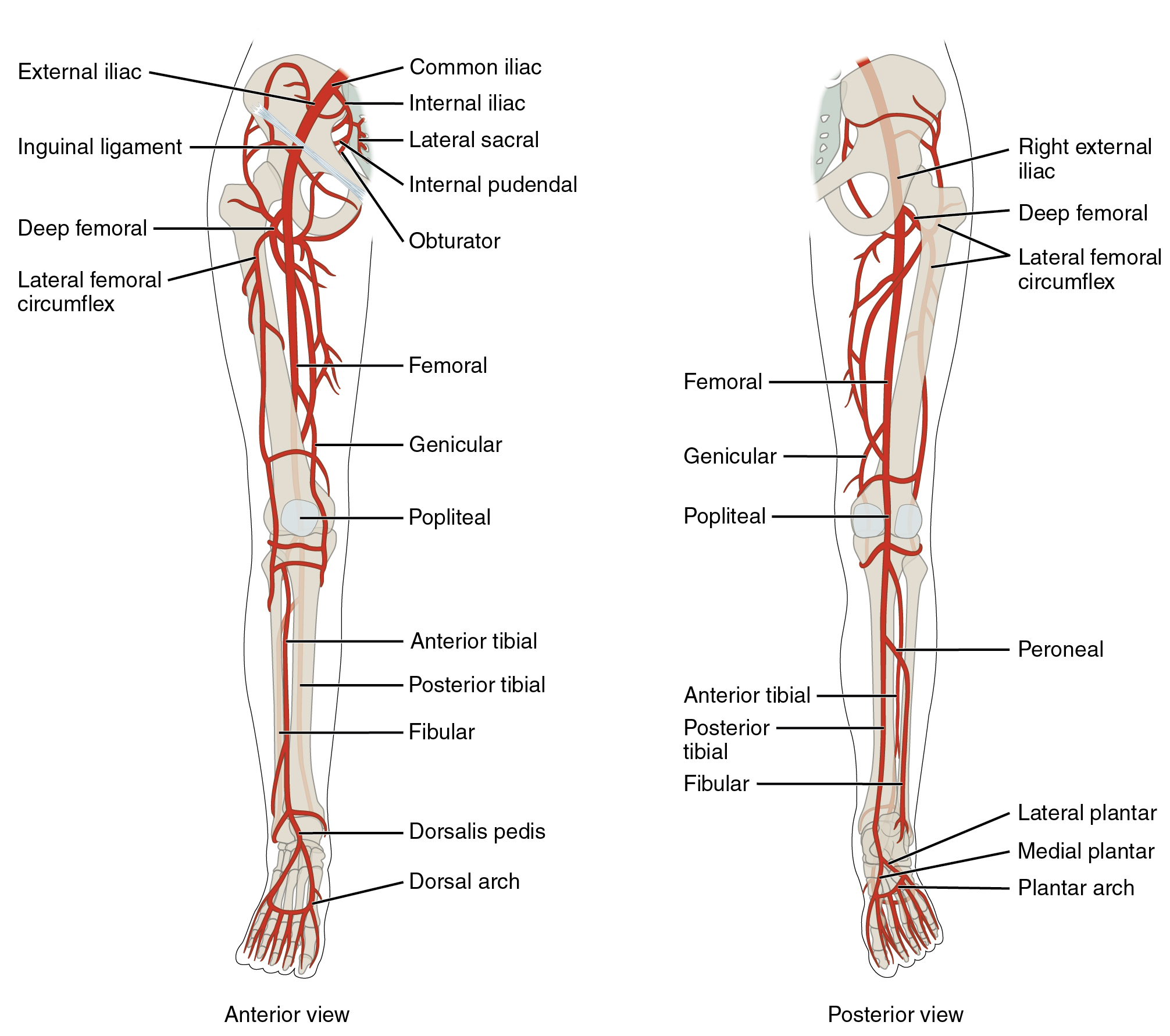
Arteries of the Lower Limb, Anterior and Posterior Views. This detailed illustration shows the arterial anatomy of the lower limb from both anterior and posterior perspectives. Labeled vessels include the common, external, and internal iliac arteries, femoral artery, profunda femoris (deep femoral) artery with its lateral and medial circumflex branches, genicular artery, popliteal artery, anterior and posterior tibial arteries, fibular (peroneal) artery, dorsalis pedis artery, medial and lateral plantar arteries, and the dorsal and plantar arches.
OpenStax College, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
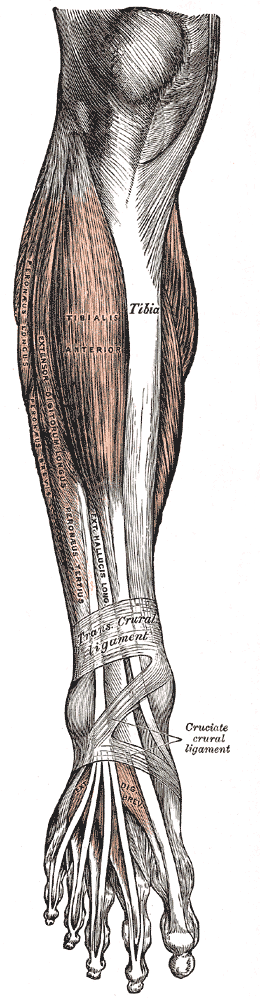
Muscles of the Anterior Leg Compartment and the Foot Dorsum. This anatomical plate illustrates the anterolateral musculature of the lower limb, specifically identifying the tibialis anterior, extensor digitorum longus, and extensor hallucis longus alongside the peroneus longus, peroneus brevis, and peroneus tertius. The diagram displays the relationship between the tibia and these muscle groups as they pass under the transverse crural and cruciate crural ligaments. On the foot, the extensor digitorum brevis is shown distally, completing the representation of the extrinsic and intrinsic muscles responsible for foot and toe movement.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
Ling ZX, Kumar VP. The myofascial compartments of the foot: a cadaver study. The Journal of bone and joint surgery. British volume. 2008 Aug:90(8):1114-8. doi: 10.1302/0301-620X.90B8.20836. Epub [PubMed PMID: 18669973]
Level 3 (low-level) evidenceReach JS Jr, Amrami KK, Felmlee JP, Stanley DW, Alcorn JM, Turner NS. The compartments of the foot: a 3-tesla magnetic resonance imaging study with clinical correlates for needle pressure testing. Foot & ankle international. 2007 May:28(5):584-94 [PubMed PMID: 17559766]
Faymonville C, Andermahr J, Seidel U, Müller LP, Skouras E, Eysel P, Stein G. Compartments of the foot: topographic anatomy. Surgical and radiologic anatomy : SRA. 2012 Dec:34(10):929-33. doi: 10.1007/s00276-012-0982-3. Epub 2012 May 26 [PubMed PMID: 22638720]
Orbay H, Kerem M, Unlü RE, Esmer AF, Cömert A, Tüccar E, Sensöz O. Vascular anatomy of plantar muscles. Annals of plastic surgery. 2007 Apr:58(4):420-6 [PubMed PMID: 17413886]
Alagoz MS, Orbay H, Uysal AC, Comert A, Tuccar E. Vascular anatomy of the metatarsal bones and the interosseous muscles of the foot. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2009 Sep:62(9):1227-32. doi: 10.1016/j.bjps.2007.12.083. Epub 2008 Jun 20 [PubMed PMID: 18572002]
Kalin PJ, Hirsch BE. The origins and function of the interosseous muscles of the foot. Journal of anatomy. 1987 Jun:152():83-91 [PubMed PMID: 3654378]
Olewnik Ł, Podgórski M, Polguj M, Topol M. A cadaveric and sonographic study of the morphology of the tibialis anterior tendon - a proposal for a new classification. Journal of foot and ankle research. 2019:12():9. doi: 10.1186/s13047-019-0319-0. Epub 2019 Feb 1 [PubMed PMID: 30733832]
Amis AA, de Leeuw PA, van Dijk CN. Surgical anatomy of the foot and ankle. Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2010 May:18(5):555-6. doi: 10.1007/s00167-010-1107-3. Epub [PubMed PMID: 20306016]
Chiou-Tan F, Furr-Stimming E, John J, Harrell JS, Zhang H, Taber KH. Procedure-oriented sectional anatomy of the foot. Journal of computer assisted tomography. 2015 Jan-Feb:39(1):140-2. doi: 10.1097/RCT.0000000000000165. Epub [PubMed PMID: 25279850]
Level 2 (mid-level) evidenceO'Rahilly R, Müller F. Developmental stages in human embryos: revised and new measurements. Cells, tissues, organs. 2010:192(2):73-84. doi: 10.1159/000289817. Epub 2010 Feb 26 [PubMed PMID: 20185898]
Jeanty P, Cousaert E, Cantraine F, Hobbins JC, Tack B, Struyven J. A longitudinal study of fetal limb growth. American journal of perinatology. 1984 Jan:1(2):136-44 [PubMed PMID: 6335042]
Level 2 (mid-level) evidenceJensen MR, Simonsen L, Karlsmark T, Bülow J. Lymphoedema of the lower extremities--background, pathophysiology and diagnostic considerations. Clinical physiology and functional imaging. 2010 Nov:30(6):389-98. doi: 10.1111/j.1475-097X.2010.00969.x. Epub 2010 Aug 16 [PubMed PMID: 20718809]
Schacht V, Luedemann W, Abels C, Berens von Rautenfeld D. Anatomy of the subcutaneous lymph vascular network of the human leg in relation to the great saphenous vein. Anatomical record (Hoboken, N.J. : 2007). 2009 Jan:292(1):87-93. doi: 10.1002/ar.20765. Epub [PubMed PMID: 18951505]
Yablon CM, Hammer MR, Morag Y, Brandon CJ, Fessell DP, Jacobson JA. US of the Peripheral Nerves of the Lower Extremity: A Landmark Approach. Radiographics : a review publication of the Radiological Society of North America, Inc. 2016 Mar-Apr:36(2):464-78. doi: 10.1148/rg.2016150120. Epub 2016 Feb 12 [PubMed PMID: 26871986]
Taber KH, Duncan G, Chiou-Tan F, Patni P, Hayman LA. Sectional neuroanatomy of the lower limb II: leg and foot. Journal of computer assisted tomography. 2001 Sep-Oct:25(5):823-6 [PubMed PMID: 11584247]
Yammine K. The accessory peroneal (fibular) muscles: peroneus quartus and peroneus digiti quinti. A systematic review and meta-analysis. Surgical and radiologic anatomy : SRA. 2015 Aug:37(6):617-27. doi: 10.1007/s00276-015-1438-3. Epub 2015 Feb 1 [PubMed PMID: 25638531]
Level 1 (high-level) evidenceZammit J, Singh D. The peroneus quartus muscle. Anatomy and clinical relevance. The Journal of bone and joint surgery. British volume. 2003 Nov:85(8):1134-7 [PubMed PMID: 14653594]
Level 2 (mid-level) evidencePlečko M, Knežević I, Dimnjaković D, Josipović M, Bojanić I. Accessory Soleus Muscle: Two Case Reports with a Completely Different Presentation Caused by the Same Entity. Case reports in orthopedics. 2020:2020():8851920. doi: 10.1155/2020/8851920. Epub 2020 Sep 14 [PubMed PMID: 33014494]
Level 3 (low-level) evidenceTrybulski R, Gałęziok K, Matuszczyk F, Halski T, Muracki J. Problems in Diagnosis and Treatment of Soleus Muscle Injuries-Narrative Review and Case Report. Journal of clinical medicine. 2025 Mar 13:14(6):. doi: 10.3390/jcm14061955. Epub 2025 Mar 13 [PubMed PMID: 40142763]
Level 3 (low-level) evidenceNath RK, Somasundaram C. Iatrogenic nerve injury and foot drop: Surgical results in 28 patients. Surgical neurology international. 2022:13():274. doi: 10.25259/SNI_146_2022. Epub 2022 Jun 23 [PubMed PMID: 35855127]
Ramanujam CL, Facaros Z, Zgonis T. Abductor hallucis muscle flap with circular external fixation for Charcot foot osteomyelitis: a case report. Diabetic foot & ankle. 2011:2():. doi: 10.3402/dfa.v2i0.6336. Epub 2011 May 11 [PubMed PMID: 22396821]
Level 3 (low-level) evidenceMasadeh S, Liette MD, Perry W, Bibbo C. Distally-based (Reverse) Medial Hemi-flexor Hallucis Brevis Muscle Flap in a Series of High-risk Patients: Retrospective Case Series. Plastic and reconstructive surgery. Global open. 2023 Jan:11(1):e4751. doi: 10.1097/GOX.0000000000004751. Epub 2023 Jan 20 [PubMed PMID: 36699217]
Level 2 (mid-level) evidenceCraig GC. Intrinsic Muscle Flaps for Coverage of Small Defects in the Foot. Clinics in podiatric medicine and surgery. 2020 Oct:37(4):789-802. doi: 10.1016/j.cpm.2020.07.006. Epub [PubMed PMID: 32919605]
Mert S, Heidekrueger PI, Fuchs B, Nuernberger T, Haas-Lützenberger EM, Giunta RE, Ehrl D, Demmer W. Microvascular Muscle vs. Fascio-Cutaneous Free Flaps for Reconstruction of Plantar Load-Bearing Foot Defects-An International Survey. Journal of clinical medicine. 2024 Feb 24:13(5):. doi: 10.3390/jcm13051287. Epub 2024 Feb 24 [PubMed PMID: 38592127]
Level 3 (low-level) evidenceHemamalini, Manjunatha HN. Variations in the origin, course and branching pattern of dorsalis pedis artery with clinical significance. Scientific reports. 2021 Jan 14:11(1):1448. doi: 10.1038/s41598-020-80555-z. Epub 2021 Jan 14 [PubMed PMID: 33446776]
Morehouse JL, Konstanty JM, Cacini AC, Stern JM, Sloan SS. Anatomical variations of the deep plantar arterial arch: surgical implications for partial foot amputations and soft tissue reconstruction. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2025 Jul 30:():. pii: S1067-2516(25)00229-7. doi: 10.1053/j.jfas.2025.07.012. Epub 2025 Jul 30 [PubMed PMID: 40749775]
Tonogai I, Tsuruo Y, Sairyo K. Implications of Dorsalis Pedis Artery Anatomical Variants for Dorsal Midfoot Surgery. Foot & ankle international. 2022 Jul:43(7):942-947. doi: 10.1177/10711007221081527. Epub 2022 Mar 17 [PubMed PMID: 35297698]
Zhou K, Song L, Zhang P, Wang C, Wang W. Surgical Versus Non-Surgical Methods for Acute Achilles Tendon Rupture: A Meta-Analysis of Randomized Controlled Trials. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2018 Nov-Dec:57(6):1191-1199. doi: 10.1053/j.jfas.2018.05.007. Epub [PubMed PMID: 30368430]
Level 1 (high-level) evidenceXu Y, Li C, Liu T, Xiang F, Deng Y, Li Z, Wei D. Long-term outcome of flexor hallucis longus tendon transfer for chronic Achilles tendon rupture with large defect: A retrospective series. Medicine. 2023 Sep 29:102(39):e35302. doi: 10.1097/MD.0000000000035302. Epub [PubMed PMID: 37773872]
Level 2 (mid-level) evidenceLi F, Adrien N, He Y. Biomechanical Risks Associated with Foot and Ankle Injuries in Ballet Dancers: A Systematic Review. International journal of environmental research and public health. 2022 Apr 18:19(8):. doi: 10.3390/ijerph19084916. Epub 2022 Apr 18 [PubMed PMID: 35457783]
Level 1 (high-level) evidence