 Anatomy, Bony Pelvis and Lower Limb: Foot Bones
Anatomy, Bony Pelvis and Lower Limb: Foot Bones
Introduction
The foot is a complex structure comprising more than 26 bones, 30 joints, numerous tendons, ligaments, and muscles. The foot's structural organization enables upright stance, supports full body weight, and forms the foundation of bipedal gait mechanics. The foot corresponds to the portion of the lower extremity distal to the ankle joint and is subdivided into hindfoot, midfoot, and forefoot. The articular surfaces of each bone are covered with hyaline cartilage. Each joint is enclosed by a capsule and supported by ligamentous structures. Foot musculature attaches to osseous structures via tendons, permitting muscular contraction to transmit force to bone.
Complex foot anatomy enables adaptation to uneven terrain during heel strike and conversion into a rigid lever during toe-off, facilitating propulsion during gait. Given the functional importance of these structures in activities of daily living, foot injury and pain are common presentations in emergency departments and primary care settings. Although ligamentous and soft tissue components are essential to foot function, this activity primarily focuses on osseous structures.[1][2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The foot comprises 26 bones distal to the ankle joint and is subdivided into the hindfoot, midfoot, and forefoot.[3] Osseous structures are also categorized into the tarsal, metatarsal, and phalangeal groups (see Image. Foot Bones).[4][5] The hindfoot consists of the talus and calcaneus, 2 of the 7 tarsal bones. The ankle joint forms the articulation between the hindfoot and the more proximal lower extremity and is composed of the tibia, fibula, and talus. The distal tibia, which includes the medial malleolus, posterior malleolus, and tibial plafond, together with the distal fibula (lateral malleolus), forms a mortise, which articulates with the body of the talus, termed the "talar dome."[6][7]
The talus is the 2nd-largest tarsal bone. The bone slopes inferomedially and terminates in a convex, cartilage-covered head that articulates with the navicular. The body of the talus articulates with the calcaneus at the subtalar joint, which is composed of multiple facets, including the posterolateral (posterior facet), the middle facet at the sustentaculum tali located medially, and the anteromedial (anterior) facet. The superior aspect of the talar body forms the talar dome, serving as the articular surface of the tibiotalar joint. The talar neck lies between the body and head of the talus and forms the roof of the tarsal canal, which opens laterally as the sinus tarsi. The posterior process of the talus consists of medial and lateral tubercles, with the flexor hallucis longus tendon coursing within the groove between these structures. An elongated lateral tubercle represents a normal anatomic variant known as the Stieda process. An osseous ridge is typically present at the distal aspect of the talar neck and serves as the attachment site for the joint capsule and ligamentous structures.[8]
The talus is approximately 60% covered with hyaline cartilage and lacks muscular or tendinous attachments. This unique anatomy renders the bone susceptible to avascular necrosis despite arterial contributions from 3 sources. The posterior tibial artery supplies the body of the talus, while the anterior tibial artery supplies the superior 1/2 of the head and neck. The posterior tibial artery gives rise to the tarsal canal artery approximately 1 cm proximal to its bifurcation into the medial (MPA) and lateral (LPA) plantar arteries.[9] The tarsal sinus artery supplies the central and lateral 2/3 of the talar body. Anastomoses with the tarsal canal artery occur, and deltoid branches arising from this network supply the remaining portions of the talus.[10]
Inferior to the talus lies the largest tarsal bone, the calcaneus. The calcaneus articulates superiorly with the talus at the anterior, middle, and posterior facets. Each facet represents an encapsulated synovial joint, with the middle and anterior facets enclosed within a shared joint capsule. Between the posterior and middle facets, the calcaneal sulcus extends posteromedially and forms the floor of the sinus tarsi. Anteriorly, the calcaneus articulates with the cuboid.[11] The calcaneus is adapted to withstand weight-bearing stresses, with approximately 50% of body weight transmitted through the subtalar joints and calcaneus, typically distributed equally between both feet in the absence of gait abnormalities. Traction trabeculae radiate from the inferior cortex on radiographs, while compression trabeculae extend posteriorly from the anterior and posterior subtalar facets. A small region with relatively sparse trabeculation is identified as the neutral triangle.[12]
The midfoot consists of the cuboid, navicular, and cuneiforms (medial, intermediate, and lateral), comprising 5 of the 7 tarsal bones. The talus and calcaneus constitute the remaining 2 tarsal bones of the hindfoot. The navicular demonstrates a proximally concave and distally convex configuration. The concave posterior surface of the navicular receives the ellipsoid-shaped talar head, forming a ball-and-socket articulation analogous to the hip joint and termed "coxa pedis."[13] Three facets along the distal convex surface articulate with the cuneiforms, while a single inferolateral facet articulates with the cuboid. Medially, the posterior tibial tendon inserts at the navicular tuberosity.
The cuboid is a roughly cube-shaped bone that ossifies between the 9th fetal month and 6 months postnatally. Proximally, articulation occurs with the calcaneus, and distally with the lateral cuneiform as well as the 4th and 5th metatarsals. Rare articulation with the head of the talus occurs in some cases. The inferolateral margin of the cuboid contains a sulcus that accommodates the fibularis longus tendon.[14][15]
The talonavicular and calcaneocuboid articulations connect the hindfoot to the midfoot and collectively form the Chopart joint. The joint is named after the French surgeon François Chopart.[16]
The cuneiforms articulate proximally with the navicular and distally with the 1st through 3rd metatarsals, forming an arch with a keystone-like configuration. The medial cuneiform is the largest of the 3 cuneiform bones and articulates distally with the 1st metatarsal, medially with the intermediate (middle) cuneiform, and proximally with the navicular. A vertical, square-shaped facet accommodates the dorsomedial base of the 2nd metatarsal. The medial cuneiform typically contains 2 ossification centers and ossifies during the 2nd year of life. Bipartite medial cuneiform may result from failure of fusion between ossification centers and is generally an incidental finding. The Lisfranc ligament complex attaches to the distal and lateral aspect of the medial cuneiform and courses obliquely to the base of the 2nd metatarsal. This structure transmits substantial axial load to the 2nd metatarsal during ambulation.[17]
The intermediate (middle) cuneiform is the smallest of the 3 cuneiforms. Articulation occurs with the navicular proximally and the 2nd metatarsal distally, as well as with the adjacent cuneiforms medially and laterally. Relative shortening compared with adjacent cuneiforms creates a mortise that accommodates the base of the 2nd metatarsal. The intermediate cuneiform has 1 ossification center and ossifies during the 3rd year of life.[18]
The lateral cuneiform articulates with the cuboid, navicular, 3rd metatarsal, and intermediate cuneiform. The plantar surface receives slips from the posterior tibial tendon and, in some cases, the flexor hallucis brevis (FHB).
The forefoot consists of the 5 metatarsals and 14 phalanges. Each metatarsal is subdivided into 3 regions: base, shaft (diaphysis), and head.
The junction between the midfoot and forefoot occurs at the tarsometatarsal articulations, collectively termed the "Lisfranc joint," named after the French surgeon Jacques Lisfranc de Saint-Martin. The 1st metatarsal articulates with the medial cuneiform, the 2nd with the intermediate cuneiform, the 3rd with the lateral cuneiform, and the 4th and 5th with the cuboid, thereby linking the midfoot to the forefoot.[19]
The 1st (great) metatarsal warrants special attention. Medial and lateral grooves accommodate the sesamoid bones at the plantar aspect of the metatarsal head. The intersesamoidal ridge separates these grooves. The intersesamoidal ligament connects the medial and lateral sesamoid bones. These structures contribute to the plantar plate complex.[20][21]
The 14 phalanges are analogous to the fingers, with 2 phalanges in the great toe and 3 in each of the remaining digits. Segmental anomalies are not uncommon.
Functionally, the osseous structures of the foot form 3 arches. The calcaneus, cuboid, and 4th and 5th rays constitute the rigid lateral arch. The medial arch demonstrates dynamic variation in shape, permitting adaptation to uneven terrain, and includes the medial 3 rays, cuneiforms, navicular, talus, and calcaneus. The transverse arch extends obliquely across the tarsometatarsal joints.[22]
The foot contains 7 tarsal bones
- Cuboid
- Calcaneus (heel bone)
- Medial, intermediate, and lateral cuneiforms
- Navicular
- Talus
Distal to the tarsal bones are the 5 metatarsals, numbered 1 through 5 from medial to lateral. The osseous framework of the toes consists of 14 phalanges. The 1st digit contains 2 phalanges, whereas the 2nd through 5th digits each contain 3 phalanges.
Sesamoid bones of the foot contribute to stability and function. Two sesamoid bones are typically located plantar to the head of the 1st metatarsal at the 1st MTP joint. Both sesamoids are embedded within the tendon of the FHB. A sesamoid is generally situated laterally, whereas the other is positioned medially. In some individuals, only a single sesamoid bone is present near the 1st MTP joint.
The foot is anatomically divided into the forefoot, midfoot, and hindfoot. The forefoot contains the metatarsals and phalanges. The midfoot consists of 5 of the 7 tarsal bones, including the navicular, cuboid, and 3 cuneiforms. The hindfoot is composed of the talus and the calcaneus, the remaining 2 tarsal bones.
Several major articulations contribute to foot function. The subtalar joint is formed by the articulation between the talus and calcaneus and consists of 6 facets, 3 on each bone. These facets are divided into anterior and posterior joints, with the anterior joint comprising the anterior and middle facets.[23] The Chopart joint, also termed the "midtarsal joint," connects the hindfoot to the midfoot. Constituent articulations include the talonavicular and calcaneocuboid joints. The joint is named after the French surgeon François Chopart. The Lisfranc joint is the junction between the midfoot and forefoot and is composed of the tarsometatarsal articulations. The joint is named after the French surgeon Jacques Lisfranc de Saint-Martin. The plantar plates are fibrocartilaginous structures associated with the MTP joints. Injury involving the 1st MTP joint is termed "turf toe."[24]
Embryology
During the 4th through 8th weeks of gestation, development of the appendicular skeleton begins as ventrolateral swellings of mesenchymal cells covered by ectoderm, progressing from limb buds to fetal extremities. Mesenchymal cells give rise to the skeleton, muscles, tendons, and ligaments, whereas the ectoderm develops into the skin. Limb formation progresses in proximal-to-distal, anterior-to-posterior, and dorsal-to-ventral directions, with the foot becoming apparent at approximately 4.5 weeks of gestation. Ossification centers form by the 9th week and continue to develop throughout gestation. Several foot bones remain cartilaginous at birth and undergo ossification during infancy and childhood, as described above.[25][26]
Blood Supply and Lymphatics
The anterior and posterior tibial arteries provide perfusion to the foot. The anterior tibial artery bifurcates into the dorsalis pedis artery, which courses along the dorsomedial aspect of the foot, and the lateral tarsal artery. Together, these vessels supply the dorsal foot. Distally, convergence of these vessels forms the transversely oriented arcuate artery.
The posterior tibial artery is palpable posterior to the medial malleolus in the region of the proximal tarsal tunnel. The vessel courses anteriorly along the medial aspect of the ankle and plantar hindfoot, giving rise to the artery of the tarsal canal before dividing into the MPA and the LPA. Distal anastomosis of the MPA and the LPA forms the transversely oriented deep plantar arch. Terminal branches of the arcuate artery and the deep plantar arch supply the toes.
The fibular (peroneal) artery courses along the posterolateral aspect of the ankle and hindfoot. Communicating arteries and anastomoses between branches of the anterior tibial, posterior tibial, and fibular arteries provide collateral circulation.[27][28]
Nerves
Branches of the saphenous, superficial fibular, deep fibular, medial (MPN) and lateral plantar (LPN), and calcaneal nerves provide innervation to the foot. Sensation to the medial ankle and foot is supplied by the saphenous nerve, a branch of the femoral nerve. Injury to the saphenous nerve may occur during Achilles tendon repair and can result in pain and a burning sensation in the medial hindfoot.
The common fibular (peroneal) nerve divides into the superficial and deep fibular nerves near the level of the knee. The superficial fibular nerve, a terminal branch of the common fibular nerve, provides sensation to most of the dorsal foot. The deep fibular nerve innervates the extensor digitorum brevis and extensor hallucis brevis and provides sensory innervation to the 1st webspace between the 1st and 2nd digits.
Fibular nerve injury may occur following high-energy trauma at the level of the fibular head, including motor vehicle collisions, knee dislocation, or proximal fibular fractures. Clinical manifestations may include foot drop, characterized by impaired dorsiflexion during ambulation, as well as numbness or burning over the dorsum of the foot.[29][30]
The tibial nerve divides into the MPN and the LPN at the level of the medial ankle within the tarsal tunnel. The MPN provides sensation to the plantar aspect of the 1st through 3rd digits and the medial aspect of the 4th digit. Motor innervation is supplied to the flexor digitorum brevis, FHB, abductor hallucis, and 1st lumbrical.[31]
The LPN provides sensation to the lateral plantar aspect of the 4th digit and the entire plantar surface of the 5th digit. Motor innervation is supplied to the quadratus plantae, abductor digiti minimi, and flexor digiti minimi. Compression or injury of the 1st branch of the LPN is termed "Baxter neuropathy." This condition commonly occurs in runners and in patients with plantar fasciitis or acquired flatfoot deformity. Clinical manifestations include numbness and pain along the plantar and lateral hindfoot.[32]
The sural nerve is unique in arising from contributions of both the tibial and common fibular nerves and provides sensory innervation to the lateral hindfoot and midfoot. Calcaneal branches of the tibial and sural nerves provide sensory innervation to the heel.
Muscles
Muscles responsible for foot movement are categorized as extrinsic or intrinsic. Extrinsic muscles originate outside the foot, whereas intrinsic muscles are located entirely within the foot. The extrinsic musculature is further subdivided into anterior, posterior, and lateral compartments. Intrinsic musculature is classified into dorsal and plantar groups, with the plantar muscles organized into 4 layers.[33]
The anterior compartment of the extrinsic musculature includes the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and fibularis (peroneus) tertius, the latter being absent in approximately 5% to 10% of the population. The posterior compartment is divided into superficial and deep groups. The superficial group consists of the gastrocnemius, soleus, and plantaris. The deep posterior group includes the tibialis posterior, flexor hallucis longus, and flexor digitorum longus. These muscles course within the tarsal tunnel deep to the flexor retinaculum. The flexor digitorum accessorius longus, a common accessory muscle present in approximately 6% to 13% of the population, may also be identified within this compartment. The lateral compartment contains the fibularis (peroneus) longus and brevis.
The dorsal intrinsic musculature includes the extensor digitorum brevis, extensor hallucis brevis, and dorsal interossei. The plantar intrinsic musculature is arranged into 4 layers. The 1st layer contains the abductor hallucis, flexor digitorum brevis, and abductor digiti minimi. The 2nd layer consists of the quadratus plantae and lumbricals. The 3rd layer contains the FHB, adductor hallucis, and flexor digiti minimi brevis. The 4th layer consists of the plantar interossei.
Physiologic Variants
Accessory Ossicles
Numerous accessory ossicles of the foot and ankle may cause symptoms or be mistaken for pathology. The os trigonum is located posterior to the talus and is best visualized on lateral radiographs. Nonfusion of the lateral tubercle of the posterior talar process produces this variant, which corresponds to an unfused Stieda process. The reported prevalence ranges from approximately 7% to 25% of the population. Association with posterior ankle impingement, also termed "os trigonum syndrome," has been described and is a recognized cause of posterior ankle pain, particularly in ballet dancers and soccer players. Entrapment of the os trigonum may occur between the talus and calcaneus during plantarflexion.[34]
The os peroneum is a sesamoid bone located lateral to the cuboid within the fibularis longus tendon and has a reported prevalence of up to 30%. The ossicle lies within the fibularis longus tendon as the fibrous structure courses plantar to the cuboid. Pain associated with the os peroneum may result from fracture, avascular necrosis, chronic repetitive trauma, or contusion. Fracture of the os peroneum may be mistaken for a bipartite os peroneum. A fractured os peroneum may also be associated with rupture of the fibularis longus tendon. Radiographic separation of osseous fragments by more than a few millimeters may indicate tendon rupture. Alternatively, displacement of the ossicle on radiographs, most commonly in a proximal direction, suggests rupture of the fibularis longus tendon.[35][36]
The os naviculare is located along the medial aspect of the midfoot, adjacent to the navicular bone. Three types are described. Type 1 consists of a small, well-corticated ossified sesamoid bone within the distal portion of the posterior tibialis tendon. Type 2 is triangular or semispherical in shape and demonstrates fibrocartilaginous bridging at a pseudoarticulation (synchondrosis) with the navicular tuberosity. Type 3 comprises a prominent navicular tuberosity, also referred to as a "cornuate navicular." Symptoms may arise from type 2 variants due to shear stress across the synchondrosis with the navicular. Excision of the os naviculare (Kidner procedure) may be performed when symptomatic and refractory to conservative management.
The os intermetatarsum is a pyramidal-shaped ossicle located between the bases of the 1st and 2nd metatarsals along the dorsal aspect of the foot. Visualization is best achieved on anteroposterior and lateral radiographs of the foot (see Image. Anteroposterior and Oblique Radiographs of the Foot). Confusion with the fleck sign of a Lisfranc injury may occur. Although typically an asymptomatic anatomic variant, association with compression of the deep fibular nerve has been described.[37][38]
Coalitions
Tarsal coalitions are abnormal fusions between at least 2 tarsal bones. The etiology is thought to involve primitive mesenchymal segmentation abnormalities, with coalitions classified as fibrous or osseous. Calcaneonavicular and talocalcaneal coalitions account for approximately 90% of all tarsal coalitions.
Calcaneonavicular coalitions are best visualized on internal oblique radiographs of the foot (see Image. Lateral Radiograph of the Right Foot). Osseous coalitions demonstrate a bony bridge between the calcaneus and navicular, whereas fibrous coalitions show close apposition with irregular cortical margins. On lateral radiographs, calcaneonavicular coalition may appear as elongation of the anterior calcaneal process, termed the “anteater sign.”
Talocalcaneal coalitions most commonly involve the middle facet. Lateral radiographs may demonstrate the “C-sign,” resulting from osseous bridging between the talus and sustentaculum tali. Talocalcaneal coalitions are often difficult to identify on standard radiographic views.[39][40]
Bipartite Bones
Incomplete fusion of ossification centers may result in bipartite bones. Bipartite medial cuneiforms are rare, with a reported prevalence of approximately 0.3% of the population. Bipartition may be partial or complete, with osseous segments often connected by cartilage or fibrocartilage. Bipartite medial cuneiforms are divided into dorsal and plantar components by a horizontal synchondrosis. This horizontal division produces the “E-sign” on sagittal magnetic resonance imaging (MRI). Bipartite sesamoids occur more frequently and may be mistaken for fractures. The os peroneum and hallucal sesamoids are most commonly involved. Differentiation between sesamoid fractures and bipartite variants may be challenging. Fractures typically demonstrate jagged, irregular margins, whereas bipartite sesamoids demonstrate smooth, well-corticated sclerotic margins.[41][42]
Clinical Significance
Fractures
The talar neck contains less trabecular bone than the talar head and body and is, therefore, relatively weak. The most common mechanism of injury involves forced dorsiflexion. The first case series was described in World War I fighter pilots and termed “aviator astragalus.” Current cases most commonly result from motor vehicle collisions or falls. Talar neck fractures are classified using the Hawkins–Canale system, and fracture classification shows a strong correlation with the risk of avascular necrosis.
Blood supply to the talus is similar to that of the scaphoid, with vascularity progressing in a distal-to-proximal direction. Talar neck fractures may compromise perfusion to the talar dome and lead to avascular necrosis. The Hawkins sign is a radiographic indicator of preserved vascularity of the talar dome. The sign appears as a subcortical lucency of the talar dome, whereas sclerosis of the talar dome is concerning for avascular necrosis.
Lateral talar process fractures are uncommon and may be radiographically occult. The most common mechanism involves forced inversion with dorsiflexion, with increased incidence in snowboarders. Clinical presentation typically includes persistent lateral ankle pain located approximately 1 cm inferior and anterior to the fibula. These injuries are frequently misdiagnosed as ligamentous sprains.
On radiographs, the normally symmetric V-shaped contour of the calcaneus may appear distorted on the lateral view in cases of displaced fracture. Several classification systems exist, with the McCrory–Bladin system most commonly used. Nondisplaced and small fractures are typically managed conservatively, whereas open reduction and internal fixation is indicated for fractures with greater than 2 mm displacement.[43]
Calcaneal fractures are historically severe injuries and comprise the most common tarsal fractures. These injuries occur secondary to increased axial loading and are classified as intraarticular or extraarticular. Approximately 3 out of 4 calcaneal fractures are intraarticular. Intraarticular fractures include a shear component involving the posterior facet and a compression fracture line resulting from wedging of the anterolateral talar process into the angle of Gissane.
Extraarticular fractures involve the anterior process, midcalcaneus (body, sustentaculum tali, fibular (peroneal) tubercle, and lateral process), and posterior calcaneus. Computed tomography (CT) is the preferred imaging modality for characterization of calcaneal fractures, particularly for assessment of posterior subtalar joint involvement. Calcaneal fractures are associated with thoracolumbar spine fractures, and clinical screening for concurrent spinal injury is essential. Thoracolumbar CT imaging is indicated in the presence of back pain. Axial loading–related calcaneal fractures have also been termed “Lover’s fractures” or “Casanova fractures."[44][45]
Lisfranc injuries are fracture-dislocation injuries of the tarsometatarsal joints. The Lisfranc ligament complex consists of 3 components: dorsal oblique, plantar oblique, and interosseous fibers, which stabilize the base of the 2nd metatarsal to the medial cuneiform. Although the interosseous component is the strongest stabilizer, disruption of any 2 of the 3 ligamentous bands results in instability of the 2nd tarsometatarsal joint. These injuries occur commonly in sports such as football, basketball, and gymnastics. The typical mechanism involves axial loading of a plantarflexed foot.
Clinical presentation includes dorsal midfoot swelling and nonspecific midfoot pain. Weight-bearing radiographs are more sensitive for detection, although findings may be subtle. The “fleck” sign suggests an avulsion fracture fragment. Additional radiographic features include dorsal midfoot soft tissue swelling and widening of the interval between the bases of the 1st and 2nd metatarsals. Lisfranc injuries are classified as divergent or homolateral based on the direction of metatarsal displacement. Radiographic assessment requires careful evaluation of tarsometatarsal alignment. In the setting of midfoot pain and swelling following trauma, a high index of suspicion is required for subtle or occult Lisfranc injury. CT or MRI may be warranted for further evaluation and exclusion of injury.[46]
Bone lesions may be categorized as aggressive or nonaggressive based on the pattern of osseous destruction. The Lodwick–Madewell grading system classifies lesion aggressiveness and demonstrates strong prognostic and pathologic correlation. Key imaging features include lesion margins, cortical disruption, presence of an associated soft tissue mass, and degree of endosteal scalloping. Well-circumscribed lesions with a thin sclerotic margin are more likely to be benign. Lesions demonstrating a wide zone of transition, poorly defined margins, or cortical destruction are highly suspicious for an aggressive process, including malignancy or infection.[47]
Patient age is essential in formulating an appropriate differential diagnosis, as specific entities occur more commonly in defined age groups. Ewing sarcoma and osteosarcoma occur more frequently in younger patients. Lesions that are enlarging, contain a soft tissue component, or exceed 5 cm in size are indicative of malignancy. The most frequent benign lesions of the foot include unicameral bone cysts (predominantly in the calcaneus), enchondromas (most frequently in the metatarsals), and osteochondromas (most often in the forefoot and ankle). The most common malignant lesions include chondrosarcoma, osteosarcoma (often involving the calcaneus), and Ewing sarcoma (predominantly involving the midfoot and hindfoot).[48][49][50]
"Osteonecrosis" refers to ischemic death of bone and is commonly termed "avascular necrosis." Common etiologies include trauma, corticosteroid use, alcoholism, sickle cell disease, and collagen vascular diseases. Several site-specific entities merit attention. A Freiberg infraction involves the metatarsal heads, most frequently the 2nd (approximately 68%) and 3rd (approximately 28%) metatarsals. Radiographically, Freiberg infractions may demonstrate mottled sclerosis with or without subchondral collapse of the metatarsal head. Freiberg disease occurs more commonly in women and has been associated with high-heeled footwear. Köhler disease, also referred to as "Müller-Weiss disease" in adult presentations, is osteonecrosis of the navicular. Bilateral involvement is common, with initial changes typically affecting the lateral aspect of the bone. Köhler disease, the pediatric form, most commonly affects boys aged 4 to 6 years. Osteonecrosis of the talus most commonly occurs following trauma and may progress to collapse of the talar dome.[51]
Gout is a metabolic disease characterized by monosodium urate crystal deposition. The lower extremities are most frequently involved, classically the great toe, where the condition is termed "podagra." Osseous erosions may occur anywhere within bone but are most commonly intraarticular and paraarticular. Acute episodes typically resolve within a few days without treatment. Early gout may be radiographically occult. However, progressive disease demonstrates marginal joint erosions with overhanging edges. Soft tissue masses called "tophi" may develop secondary to urate deposition within soft tissues. Soft tissue tophi are “pseudolesions” that may mimic malignant processes. Suggestive clinical findings, in conjunction with characteristic erosive changes on imaging, typically allow accurate diagnosis and prevent unnecessary tissue sampling.[52]
Metatarsal stress injuries are common in military recruits, runners, and ballet dancers. Conditions that alter weight-bearing mechanics, such as hallux valgus or pes planus, also increase the risk of stress injury. Metabolic disorders and vitamin deficiencies may further predispose to fracture development. Fatigue fractures result from repetitive stress on normal bone, whereas insufficiency fractures result from repetitive stress on structurally weakened bone. These injuries are frequently radiographically occult until periosteal reaction or sclerosis develops, reflecting the healing response. MRI and nuclear medicine bone scans demonstrate higher sensitivity than radiography and are indicated when symptoms persist despite conservative management. Common locations in the foot and ankle include the calcaneal tuberosity, subchondral talar head, navicular, bases of the 1st and 5th metatarsals, and the diaphyseal to neck regions of the 2nd through 4th metatarsals.[53]
Sesamoiditis may occur secondary to repetitive injury, falls from height, or stepping on uneven surfaces. MRI best characterizes the condition, demonstrating increased short τ inversion recovery (STIR) signal with a normal T1 signal. Surrounding soft tissues are often inflamed. Osteomyelitis of the foot most commonly results from penetrating trauma or ulceration and is most frequently seen in diabetic patients. Radiographs may demonstrate osseous destruction, although findings may be absent in early disease. MRI provides greater sensitivity, with typical findings including decreased T1 signal and increased STIR signal.[54][55]
Media
(Click Image to Enlarge)
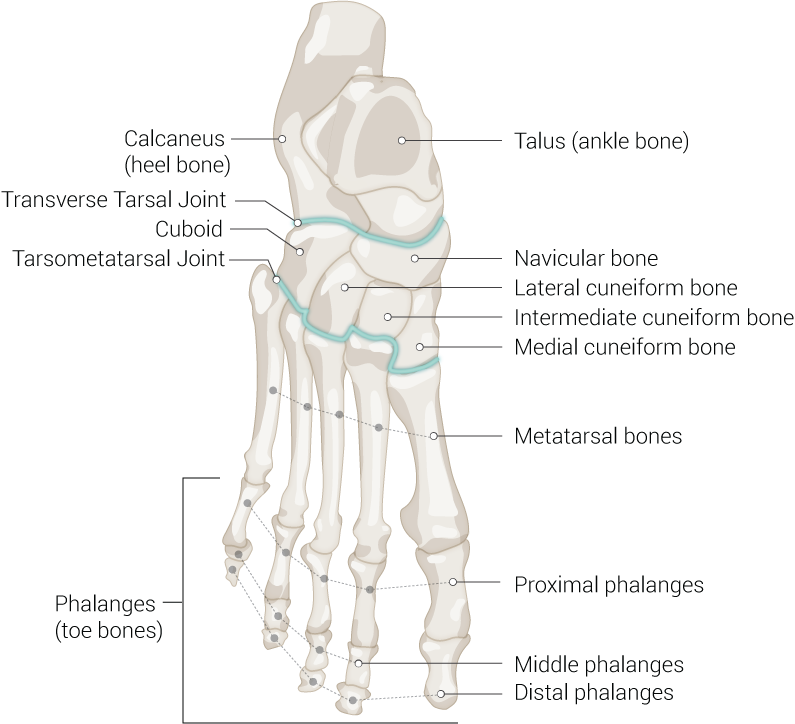
Foot Bones. Anatomy of the foot including talus (ankle bone), navicular bone, lateral cuneiform bone, intermediate cuneiform bone, medial cuneiform bone, metatarsal bones, proximal phalanges, middle phalanges, distal phalanges, phalanges (toe bones), tarsometatarsal joint, cuboid, transverse tarsal joint, and calcaneus (heel bone).
Illustrated by B Palmer
(Click Image to Enlarge)
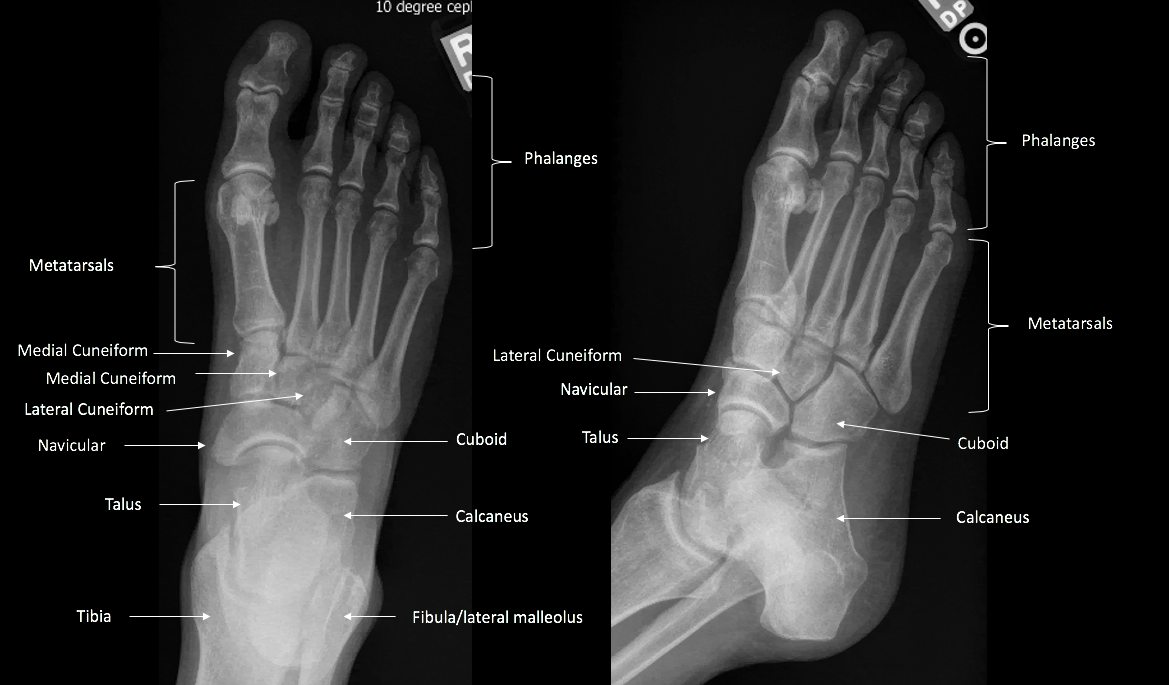
Anteroposterior and Oblique Radiographs of the Foot. The dual-panel image demonstrates skeletal anatomy of the foot from 2 diagnostic projections. Labels identify the phalanges, metatarsals, medial cuneiform, lateral cuneiform, navicular, talus, cuboid, and calcaneus. Structures of the ankle joint, including the tibia and fibula (lateral malleolus), are also visualized on the anteroposterior projection.
Contributed by Douglas Byerly, MD PhD
(Click Image to Enlarge)

Lateral Radiograph of the Right Foot. The image provides a profile view of the pedal skeleton, highlighting the alignment of the longitudinal arch. Identified structures include the phalanges, metatarsals, navicular, talus, and calcaneus. The midfoot section demonstrates the overlapping and superimposed nature of the cuneiforms and cuboid from this diagnostic angle.
Contributed by Douglas Byerly, MD PhD
References
Stirling P, MacKenzie SP, Maempel JF, McCann C, Ray R, Clement ND, White TO, Keating JF. Patient-reported functional outcomes and health-related quality of life following fractures of the talus. Annals of the Royal College of Surgeons of England. 2019 Jul:101(6):399-404. doi: 10.1308/rcsann.2019.0044. Epub 2019 Jun 3 [PubMed PMID: 31155885]
Level 2 (mid-level) evidenceBrockett CL, Chapman GJ. Biomechanics of the ankle. Orthopaedics and trauma. 2016 Jun:30(3):232-238 [PubMed PMID: 27594929]
Ficke J, Byerly DW. Anatomy, Bony Pelvis and Lower Limb: Foot. StatPearls. 2026 Jan:(): [PubMed PMID: 31536304]
Melenevsky Y, Mackey RA, Abrahams RB, Thomson NB 3rd. Talar Fractures and Dislocations: A Radiologist's Guide to Timely Diagnosis and Classification. Radiographics : a review publication of the Radiological Society of North America, Inc. 2015 May-Jun:35(3):765-79. doi: 10.1148/rg.2015140156. Epub [PubMed PMID: 25969933]
Prapto D, Dreyer MA. Anatomy, Bony Pelvis and Lower Limb: Navicular Bone. StatPearls. 2026 Jan:(): [PubMed PMID: 31613455]
Russell TG, Byerly DW. Talus Fracture. StatPearls. 2026 Jan:(): [PubMed PMID: 30969509]
Shamrock AG, Byerly DW. Talar Neck Fractures. StatPearls. 2026 Jan:(): [PubMed PMID: 31194455]
Resnick D. Talar ridges, osteophytes, and beaks: a radiologic commentary. Radiology. 1984 May:151(2):329-32 [PubMed PMID: 6709899]
Level 3 (low-level) evidenceMulfinger GL, Trueta J. The blood supply of the talus. The Journal of bone and joint surgery. British volume. 1970 Feb:52(1):160-7 [PubMed PMID: 5436202]
Pearce DH, Mongiardi CN, Fornasier VL, Daniels TR. Avascular necrosis of the talus: a pictorial essay. Radiographics : a review publication of the Radiological Society of North America, Inc. 2005 Mar-Apr:25(2):399-410 [PubMed PMID: 15798058]
Kumar R, Matasar K, Stansberry S, Shirkhoda A, David R, Madewell JE, Swischuck LE. The calcaneus: normal and abnormal. Radiographics : a review publication of the Radiological Society of North America, Inc. 1991 May:11(3):415-40 [PubMed PMID: 1852935]
Daftary A, Haims AH, Baumgaertner MR. Fractures of the calcaneus: a review with emphasis on CT. Radiographics : a review publication of the Radiological Society of North America, Inc. 2005 Sep-Oct:25(5):1215-26 [PubMed PMID: 16160107]
Walter WR, Hirschmann A, Alaia EF, Tafur M, Rosenberg ZS. Normal Anatomy and Traumatic Injury of the Midtarsal (Chopart) Joint Complex: An Imaging Primer. Radiographics : a review publication of the Radiological Society of North America, Inc. 2019 Jan-Feb:39(1):136-152. doi: 10.1148/rg.2019180102. Epub 2018 Nov 30 [PubMed PMID: 30500305]
Manganaro D, Dollinger B, Nezwek TA, Sadiq NM. Anatomy, Bony Pelvis and Lower Limb, Foot Joints. StatPearls. 2026 Jan:(): [PubMed PMID: 30725626]
Gill M, Vilella RC. Anatomy, Bony Pelvis and Lower Limb: Foot Cuboid Bone. StatPearls. 2026 Jan:(): [PubMed PMID: 31751102]
Walter WR, Hirschmann A, Tafur M, Rosenberg ZS. Imaging of Chopart (Midtarsal) Joint Complex: Normal Anatomy and Posttraumatic Findings. AJR. American journal of roentgenology. 2018 Aug:211(2):416-425. doi: 10.2214/AJR.17.19310. Epub 2018 Jun 21 [PubMed PMID: 29927330]
Cenatiempo M, Buzzi R, Bianco S, Iapalucci G, Campanacci DA. Tarsometatarsal joint complex injuries: A study of injury pattern in complete homolateral lesions. Injury. 2019 Jul:50 Suppl 2():S8-S11. doi: 10.1016/j.injury.2019.01.038. Epub 2019 Feb 2 [PubMed PMID: 30745126]
Mason L, Jayatilaka MLT, Fisher A, Fisher L, Swanton E, Molloy A. Anatomy of the Lateral Plantar Ligaments of the Transverse Metatarsal Arch. Foot & ankle international. 2020 Jan:41(1):109-114. doi: 10.1177/1071100719873971. Epub 2019 Sep 10 [PubMed PMID: 31502882]
Siddiqui NA, Galizia MS, Almusa E, Omar IM. Evaluation of the tarsometatarsal joint using conventional radiography, CT, and MR imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 2014 Mar-Apr:34(2):514-31. doi: 10.1148/rg.342125215. Epub [PubMed PMID: 24617695]
Nery C, Baumfeld D, Umans H, Yamada AF. MR Imaging of the Plantar Plate: Normal Anatomy, Turf Toe, and Other Injuries. Magnetic resonance imaging clinics of North America. 2017 Feb:25(1):127-144. doi: 10.1016/j.mric.2016.08.007. Epub [PubMed PMID: 27888844]
Linklater JM. Imaging of sports injuries in the foot. AJR. American journal of roentgenology. 2012 Sep:199(3):500-8. doi: 10.2214/AJR.12.8547. Epub [PubMed PMID: 22915389]
McKeon PO, Hertel J, Bramble D, Davis I. The foot core system: a new paradigm for understanding intrinsic foot muscle function. British journal of sports medicine. 2015 Mar:49(5):290. doi: 10.1136/bjsports-2013-092690. Epub 2014 Mar 21 [PubMed PMID: 24659509]
Level 3 (low-level) evidenceResnick D. Radiology of the talocalcaneal articulations. Anatomic considerations and arthrography. Radiology. 1974 Jun:111(3):581-6 [PubMed PMID: 4828991]
Yamada AF, Crema MD, Nery C, Baumfeld D, Mann TS, Skaf AY, Fernandes ADRC. Second and Third Metatarsophalangeal Plantar Plate Tears: Diagnostic Performance of Direct and Indirect MRI Features Using Surgical Findings as the Reference Standard. AJR. American journal of roentgenology. 2017 Aug:209(2):W100-W108. doi: 10.2214/AJR.16.17276. Epub 2017 Jun 1 [PubMed PMID: 28570126]
Lezak B, Massel DH. Anatomy, Bony Pelvis and Lower Limb: Metatarsal Bones. StatPearls. 2026 Jan:(): [PubMed PMID: 31751062]
Marín-Llera JC, Garciadiego-Cázares D, Chimal-Monroy J. Understanding the Cellular and Molecular Mechanisms That Control Early Cell Fate Decisions During Appendicular Skeletogenesis. Frontiers in genetics. 2019:10():977. doi: 10.3389/fgene.2019.00977. Epub 2019 Oct 11 [PubMed PMID: 31681419]
Level 3 (low-level) evidenceBasit H, Eovaldi BJ, Sharma S. Anatomy, Bony Pelvis and Lower Limb: Peroneal Artery. StatPearls. 2026 Jan:(): [PubMed PMID: 30855864]
Lezak B, Wehrle CJ, Summers S. Anatomy, Bony Pelvis and Lower Limb: Posterior Tibial Artery. StatPearls. 2026 Jan:(): [PubMed PMID: 30725666]
Fortier LM, Markel M, Thomas BG, Sherman WF, Thomas BH, Kaye AD. An Update on Peroneal Nerve Entrapment and Neuropathy. Orthopedic reviews. 2021:13(2):24937. doi: 10.52965/001c.24937. Epub 2021 Jun 19 [PubMed PMID: 34745471]
Drăghici NC, Văcăraș V, Bolchis R, Bashimov A, Domnița DM, Iluț S, Popa LL, Lupescu TD, Mureșanu DF. Diagnostic Approach to Lower Limb Entrapment Neuropathies: A Narrative Literature Review. Diagnostics (Basel, Switzerland). 2023 Nov 4:13(21):. doi: 10.3390/diagnostics13213385. Epub 2023 Nov 4 [PubMed PMID: 37958280]
Tang A, Bordoni B. Anatomy, Bony Pelvis and Lower Limb, Foot Nerves. StatPearls. 2026 Jan:(): [PubMed PMID: 30725977]
Desai SS, Cohen-Levy WB. Anatomy, Bony Pelvis and Lower Limb: Tibial Nerve. StatPearls. 2026 Jan:(): [PubMed PMID: 30725713]
Card RK, Bordoni B. Anatomy, Bony Pelvis and Lower Limb, Foot Muscles. StatPearls. 2026 Jan:(): [PubMed PMID: 30969527]
Sellon E, Robinson P. MR Imaging of Impingement and Entrapment Syndromes of the Foot and Ankle. Magnetic resonance imaging clinics of North America. 2017 Feb:25(1):145-158. doi: 10.1016/j.mric.2016.08.004. Epub [PubMed PMID: 27888845]
Hindi HF, Byerly DW. Os Peroneum. StatPearls. 2026 Jan:(): [PubMed PMID: 30855913]
Henrique Segatt P, Luiz Masson DE Almeida Prado J, Duarte ML. Painful Os Peroneum Syndrome: An Unusual Diagnosis. The Kurume medical journal. 2025 Nov 13:71(3.4):153-156. doi: 10.2739/kurumemedj.MS7134006. Epub 2025 Jun 13 [PubMed PMID: 40518310]
Chan BY, Markhardt BK, Williams KL, Kanarek AA, Ross AB. Os Conundrum: Identifying Symptomatic Sesamoids and Accessory Ossicles of the Foot. AJR. American journal of roentgenology. 2019 Aug:213(2):417-426. doi: 10.2214/AJR.18.20761. Epub 2019 Apr 11 [PubMed PMID: 30973781]
Nakasa T, Fukuhara K, Adachi N, Ochi M. Painful os intermetatarseum in athletes: report of four cases and review of the literature. Archives of orthopaedic and trauma surgery. 2007 May:127(4):261-4 [PubMed PMID: 16850328]
Level 3 (low-level) evidenceNewman JS, Newberg AH. Congenital tarsal coalition: multimodality evaluation with emphasis on CT and MR imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 2000 Mar-Apr:20(2):321-32; quiz 526-7, 532 [PubMed PMID: 10715334]
Motwani G, Kalnawat S, Ahir K, Bhandari K. Beyond The Sprain, Unmasking a Rare Anterolateral Ankle Pathology in a Young Athlete. Journal of orthopaedic case reports. 2026 Apr:16(4):225-229. doi: 10.13107/jocr.2026.v16.i04.7098. Epub [PubMed PMID: 41970743]
Level 3 (low-level) evidenceBrookes-Fazakerley SD, Jackson GE, Platt SR. An additional middle cuneiform? Journal of surgical case reports. 2015 Jul 29:2015(7):. pii: rjv076. doi: 10.1093/jscr/rjv076. Epub 2015 Jul 29 [PubMed PMID: 26224890]
Level 3 (low-level) evidenceAl-Taie A, Intekhab SS, Alam S, Ibrahem Adam R. Bipartite Medial Cuneiform: A Rare Cause of Chronic Midfoot Pain in a Young Man. Cureus. 2025 Jul:17(7):e88484. doi: 10.7759/cureus.88484. Epub 2025 Jul 22 [PubMed PMID: 40861754]
Wijers O, Posthuma JJ, De Haas MBJ, Halm JA, Schepers T. Lateral Process Fracture of the Talus: A Case Series and Review of the Literature. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2020 Jan-Feb:59(1):136-141. doi: 10.1053/j.jfas.2019.02.003. Epub 2019 Oct 25 [PubMed PMID: 31668959]
Level 2 (mid-level) evidenceBadillo K, Pacheco JA, Padua SO, Gomez AA, Colon E, Vidal JA. Multidetector CT evaluation of calcaneal fractures. Radiographics : a review publication of the Radiological Society of North America, Inc. 2011 Jan-Feb:31(1):81-92. doi: 10.1148/rg.311105036. Epub [PubMed PMID: 21257934]
Agel J, Reider L, Morshed S, Carlini AR, Castillo RC, Pensy RA, Yoo JJ, Bosse MJ. Treatment of high-energy lower extremity trauma is explained by the Orthopaedic Trauma Association Open Fracture Classification. OTA international : the open access journal of orthopaedic trauma. 2026 Mar:9(1):e469. doi: 10.1097/OI9.0000000000000469. Epub 2026 Mar 3 [PubMed PMID: 41783146]
Chun DI, Cho J, Won SH, Nomkhondorj O, Kim J, An CY, Yi Y. Weight-Bearing CT: Advancing the Diagnosis and Treatment of Hallux Valgus, Midfoot Pathology, and Progressive Collapsing Foot Deformity. Diagnostics (Basel, Switzerland). 2025 Jan 31:15(3):. doi: 10.3390/diagnostics15030343. Epub 2025 Jan 31 [PubMed PMID: 39941273]
Caracciolo JT, Temple HT, Letson GD, Kransdorf MJ. A Modified Lodwick-Madewell Grading System for the Evaluation of Lytic Bone Lesions. AJR. American journal of roentgenology. 2016 Jul:207(1):150-6. doi: 10.2214/AJR.15.14368. Epub 2016 Apr 12 [PubMed PMID: 27070373]
Azevedo CP, Casanova JM, Guerra MG, Santos AL, Portela MI, Tavares PF. Tumors of the foot and ankle: a single-institution experience. The Journal of foot and ankle surgery : official publication of the American College of Foot and Ankle Surgeons. 2013 Mar-Apr:52(2):147-52. doi: 10.1053/j.jfas.2012.12.004. Epub 2013 Jan 16 [PubMed PMID: 23333280]
Murai NO, Teniola O, Wang WL, Amini B. Bone and Soft Tissue Tumors About the Foot and Ankle. Radiologic clinics of North America. 2018 Nov:56(6):917-934. doi: 10.1016/j.rcl.2018.06.010. Epub 2018 Sep 17 [PubMed PMID: 30322490]
Matcuk GR Jr, Waldman LE, Fields BKK, Colangeli M, Palmas M, Righi A, Filonzi G, Crombé A, Spinnato P. Conventional radiography for the assessment of focal bone lesions of the appendicular skeleton: fundamental concepts in the modern imaging era. Skeletal radiology. 2025 Jul:54(7):1391-1406. doi: 10.1007/s00256-024-04854-6. Epub 2024 Dec 24 [PubMed PMID: 39718620]
Couturier S, Gold G. Imaging Features of Avascular Necrosis of the Foot and Ankle. Foot and ankle clinics. 2019 Mar:24(1):17-33. doi: 10.1016/j.fcl.2018.10.002. Epub 2018 Nov 26 [PubMed PMID: 30685010]
Desai MA, Peterson JJ, Garner HW, Kransdorf MJ. Clinical utility of dual-energy CT for evaluation of tophaceous gout. Radiographics : a review publication of the Radiological Society of North America, Inc. 2011 Sep-Oct:31(5):1365-75; discussion 1376-7. doi: 10.1148/rg.315115510. Epub [PubMed PMID: 21918049]
Gefen A. Biomechanical analysis of fatigue-related foot injury mechanisms in athletes and recruits during intensive marching. Medical & biological engineering & computing. 2002 May:40(3):302-10 [PubMed PMID: 12195977]
Ashman CJ, Klecker RJ, Yu JS. Forefoot pain involving the metatarsal region: differential diagnosis with MR imaging. Radiographics : a review publication of the Radiological Society of North America, Inc. 2001 Nov-Dec:21(6):1425-40 [PubMed PMID: 11706214]
Taylor JA, Sartoris DJ, Huang GS, Resnick DL. Painful conditions affecting the first metatarsal sesamoid bones. Radiographics : a review publication of the Radiological Society of North America, Inc. 1993 Jul:13(4):817-30 [PubMed PMID: 8356270]