Introduction
Vertebrae, together with intervertebral discs, compose the vertebral column, also referred to as the "spine." The vertebral column extends from the skull to the coccyx and includes the cervical, thoracic, lumbar, and sacral regions. The spine serves several critical functions, including protection of the spinal cord and branching spinal nerves, structural support for the thorax and abdomen, and facilitation of flexibility and mobility. Intervertebral discs permit this mobility while preserving the supportive strength of the vertebral column.
The lumbar region contains 5 vertebrae, designated L1 through L5. The intervertebral discs, in combination with the laminae, pedicles, and articular processes of adjacent vertebrae, form spaces through which spinal nerves exit. The lumbar vertebrae collectively produce a lordotic curvature.[1]
Typical vertebrae consist of a vertebral body, a vertebral arch, and 7 processes. The vertebral body bears the majority of the axial load transmitted through the vertebral column. The vertebral body is composed of trabecular bone containing red marrow, surrounded by a thin external layer of compact bone. The vertebral arch, together with the posterior aspect of the vertebral body, forms the vertebral canal, which houses the spinal cord. The arch consists of paired pedicles connecting it to the vertebral body and paired laminae extending posteriorly from the pedicles to meet at the midline spinous process. A typical vertebra also contains 4 articular processes, including 2 superior and 2 inferior processes, which articulate with the corresponding articular processes of the adjacent vertebrae above and below.
The articulation between the superior and inferior articular facets forms a facet, or zygapophyseal, joint. These joints maintain vertebral alignment, limit the range of motion, and bear weight in certain positions. The spinous process projects posteriorly and inferiorly from the vertebral arch and overlaps the inferior vertebrae to varying degrees, depending on the spinal region. The paired transverse processes project laterally from the vertebral arch in a symmetric fashion.
Typical lumbar vertebrae demonstrate several features distinct from those of cervical or thoracic vertebrae. The most prominent distinguishing feature is the presence of a large vertebral body. The spinous process is short and thick relative to overall vertebral size and projects perpendicularly from the vertebral body. The articular facets are oriented predominantly in the vertical plane, with the superior facets directed posteromedially and medially. The facets also exhibit a curved articular surface. This characteristic distinguishes lumbar vertebrae from thoracic vertebrae. A mammillary process is present on the posterior aspect of the superior articular process (see Image. Lumbar Vertebra). Intervertebral disc thickness generally increases from rostral to caudal levels, with lumbar disc height exceeding that of cervical and thoracic intervertebral discs.[2]
Only 1 lumbar vertebra is considered atypical. L5 has the largest vertebral body and transverse processes of all vertebrae. The anterior height of the vertebral body exceeds the posterior height. This configuration contributes to the formation of the lumbosacral angle between the lumbar spine and the sacrum.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Lumbar vertebral bodies are the primary load-bearing structures and enlarge caudally in response to increasing compressive demands. Pooled contemporary morphometric data demonstrate predictable level-by-level gradients with relevance to computed tomography (CT) and magnetic resonance (MRI) interpretation. In a meta-analysis, spinal canal width increased from L1 (22.04 mm) to L5 (26.46 mm), and transverse process width increased from L1 (68.08 mm) to L5 (85.91 mm). Pedicle height decreased from L1 through L4, with a subsequent increase at L5 (14.73 mm).[3] Posterior elements, including the pedicles, laminae, and processes, form the structural ring that completes the vertebral canal and provides attachment sites necessary for segmental stability.
Lumbar facet joints are diarthrodial articulations between adjacent vertebrae characterized by complex 3-dimensional geometry and capsuloligamentous restraints. Degenerative morphologic changes of the lumbar facet joints are frequently associated with low back pain.
The lumbar spine comprises 5 vertebrae (L1–L5) organized into motion segments optimized for axial load transmission with constrained mobility. Segmental mechanics are best conceptualized as an articular triad, in which the anterior intervertebral disc and the paired posterior facet (zygapophyseal) joints function as a coupled unit. This trijoint construct permits physiologic motion while limiting injurious translation and rotation. These constraints protect posterior elements and neural structures during routine loading.[4]
The lumbar spine exhibits the greatest degree of extension within the vertebral column. This characteristic reflects the relative thickness of the intervertebral discs compared with vertebral body height, as well as the size and predominantly horizontal orientation of the spinous processes. The near-vertical orientation of the superior articular facets permits flexion, extension, and lateral flexion while restricting axial rotation. Mammillary processes serve as attachment sites for the intertransversarii muscles and multifidus. The curvature of the articular facets contributes to the stabilization and weight-bearing capacity of the lumbar vertebrae.[5]
Lumbar lordosis constitutes a key functional property arising from vertebral body and disc wedging across spinal levels. The distribution of caudal lordosis (L4–S1) and cranial lordosis (L1–L4), expressed as a fraction of total lordosis, varies with pelvic incidence, with a greater cephalad contribution observed as pelvic incidence increases.[6] This relationship explains why “normal” alignment cannot be reduced to a single angle and why adjacent-segment symptoms may develop following level-specific maldistribution of lordosis after injury, degeneration, or fusion.
Superior and inferior vertebral endplates provide the critical interface between the vertebral body and the intervertebral disc. These endplates anchor the disc and transmit stress from the disc to cancellous bone. Endplates also function as a diffusion interface for disc nutrition, linking endplate microstructure to disc hydration and viscoelastic behavior under repetitive loading, as disc nutrition is largely diffusion-dependent. The intervertebral disc comprises a gelatinous nucleus pulposus surrounded by lamellar annulus fibrosus and anchored by cartilaginous endplates. Under normal loading, the nucleus functions as a pressurized system, transmitting compressive forces radially to the annulus, which resists expansion through tensile hoop stresses.
Embryology
Lumbar vertebrae originate from paraxial mesoderm, segmented into somites. Somites differentiate into sclerotomes, which form vertebrae and ribs, and dermomyotomes, which give rise to skeletal muscle and dermis. Sclerotome cells migrate circumferentially around the notochord and neural tube and undergo resegmentation, recombining across adjacent somites to form vertebral bodies and neural arches aligned with spinal nerves and associated myotomes. Intervertebral discs develop concurrently as composite structures, with the nucleus pulposus derived from the embryonic notochord and the annulus fibrosus and cartilaginous endplates originating from the surrounding sclerotome.
Vertebrae initiate ossification during the embryonic period, around 8 weeks of gestation. Three primary ossification centers contribute to vertebral formation: 1 in the endochondral centrum, which develops into the vertebral body, and 1 in each neural process, which develops into the pedicles. Ossification begins at the thoracolumbar junction and proceeds cranially and caudally. Fusion of the neural processes with the centrum occurs between 3 and 6 years of age.
During puberty, 5 secondary ossification centers appear at the tips of the spinous process, the transverse processes, and the superior and inferior surfaces of the vertebral body. The centers on the vertebral body drive superior-inferior growth of the vertebrae. Complete ossification is typically achieved by approximately 25 years of age.[7]
Blood Supply and Lymphatics
Lumbar vertebral arterial supply is segmental. The vascular network originates primarily from the lumbar arteries, typically L1 through L4, and the subcostal artery at the T12 level, with additional contribution to L5 from the iliolumbar and related pelvic branches. The segmental pattern is clinically relevant, as anterior and lateral lumbar approaches traverse the vascular plane adjacent to the vertebral bodies. Within the vertebral body, a posterior nutrient entry zone is organized around the basivertebral foramen and canal, which transmit a neurovascular bundle.[8]
Spinal veins form venous plexuses both inside and outside the vertebral canal. These plexuses lack valves, allowing bidirectional blood flow according to pressure gradients. Venous blood ultimately drains into the segmental veins of the trunk.
Nerves
Lumbar spinal nerve roots exit the spinal canal through the intervertebral foramina. These roots then branch into ventral and dorsal rami.
Lumbar vertebrae receive sensory and autonomic innervation from recurrent meningeal branches traversing the intervertebral foramina, collectively termed the "sinuvertebral nerve." Cadaveric dissections demonstrate a consistent presence of sinuvertebral nerves at lumbar levels, with multiple branches per foramen and reproducible entry patterns.[9] Anatomic review with clinical context identifies innervation targets that include the posterior annulus, posterior longitudinal ligament, periosteum, epidural vessels, and dura, providing the anatomic basis for discogenic and periosteal pain phenotypes.[10]
Lumbar dorsal rami divide into medial, intermediate, and lateral branches. Facet joint innervation is dominated by the medial branches of the dorsal rami, which course along predictable bony landmarks relevant to image-guided denervation. Cadaveric studies demonstrate that medial branches track along the lateral neck of the superior articular process, deep to the intertransversarii mediales, before turning toward the mamilloaccessory region.[11]
The basivertebral nerve provides intraosseous innervation of the vertebral body via posterior entry pathways that parallel nutrient vascular routes.[12] This pathway is clinically significant in vertebrogenic low back pain, frequently associated with Modic type 1 or 2 endplate changes.
Muscles
Lumbar vertebrae provide attachment points for numerous muscles, including the erector spinae, interspinales, intertransversarii, latissimus dorsi, rotatores, and serratus posterior inferior. Posterior elements serve as anchors for deep stabilizers, including the multifidus and rotatores, as well as for the larger extensor complex, the erector spinae. Transverse processes and lateral vertebral elements provide fixation sites for the quadratus lumborum and psoas major.
Physiologic Variants
"Lumbosacral transitional vertebrae" (LSTV) refer to sacralization of the lowest lumbar vertebra or lumbarization of the most superior sacral segment. LSTV encompasses a morphological continuum, ranging from enlarged transverse processes to unilateral or bilateral pseudoarticulation with the sacrum or ilium, and extending to complete osseous fusion.[13]
The Castellvi system remains the most widely used radiographic classification framework and links morphology to clinically relevant patterns of disc herniation distribution.[14] Low back pain associated with LSTV may arise from the disc and facets above the transitional level (adjacent-segment overload), the contralateral facet in cases of unilateral anomalies (facet overload and arthropathy), or the anomalous articulation itself when present (degenerative pseudoarthrosis). Symptomatic LSTV is frequently discussed under the term “Bertolotti syndrome,” typically presenting as chronic low back pain in younger adults.
The presence of 5 lumbar vertebrae is common but not universal. In a surgical adolescent idiopathic scoliosis (AIS) cohort, the total number of vertebrae ranged from 23 to 25, with 15.5% exhibiting atypical vertebral variation patterns. LSTV occurred in 25.1% of that cohort.[15]
Lumbar ribs may mimic enlarged transverse processes and contribute to miscounting. A 2024 meta-analysis estimated pooled lumbar rib prevalence at 2.1% overall, 1.6% in CT-based studies, and 2.1% in radiograph-based studies, with bilateral ribs present in 65.4% of affected individuals.[16]
Surgical Considerations
Multiple surgical procedures are performed on the lumbar spine, particularly for degenerative, infectious, and traumatic conditions. Common operative approaches include laminectomy, posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, lateral interbody fusion, anterior lumbar interbody fusion, oblique lumbar interbody fusion, corpectomy, and lumbar microdiscectomy.
Clinical Significance
The vertebral venous plexuses lack valves, permitting cancer metastasis from the pelvis through these venous channels. A notable example is the metastatic spread of prostate cancer to the vertebral column. Tumors within bone are frequently associated with severe pain.
The lumbar region exhibits a lower incidence of neurological injury from fractures compared with the thoracic region. This reduced risk reflects the large size of the vertebral canal, the termination of the spinal cord at approximately the L2 level, and the relative resilience of the nerve roots of the cauda equina. Consequently, lumbar punctures are performed inferior to L2, where the spinal cord is absent and the cauda equina roots, suspended in cerebrospinal fluid, can move safely aside from the needle.
Spinal nerves increase in caliber as the spinal cord descends, whereas intervertebral foramina progressively decrease in size. Pathologic processes, including intervertebral disc degeneration that reduces intervertebral height, can exacerbate this mismatch, frequently resulting in lateral canal stenosis, in which the vertebral foramen compresses spinal nerves. Surgical decompression via laminectomy removes the spinous process and laminae to expand space for the thecal sac and spinal nerves.
Disc herniations may be treated surgically. Herniated disc material is excised to relieve pressure on affected nerve roots.
Media
(Click Image to Enlarge)
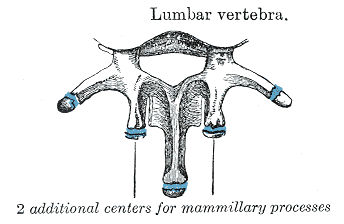
Lumbar Vertebra. This image illustrates a lumbar vertebra, with the mammillary processes marked to demonstrate their anatomical position and relevance.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
References
DeSai C, Reddy V, Agarwal A. Anatomy, Back, Vertebral Column. StatPearls. 2025 Jan:(): [PubMed PMID: 30247844]
Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Intervertebral Discs. StatPearls. 2026 Jan:(): [PubMed PMID: 29262063]
Bonczar M, Koszewski J, Czarnota W, Dziedzic M, Ostrowski P, Możdżeń K, Murawska A, Hajdyła P, Walocha A, Walocha E, Walocha J, Koziej M. The morphology of the lumbar vertebrae: a systematic review with meta-analysis of 1481 individuals with implications for spine surgery. Surgical and radiologic anatomy : SRA. 2024 Dec 6:47(1):22. doi: 10.1007/s00276-024-03509-4. Epub 2024 Dec 6 [PubMed PMID: 39643818]
Level 1 (high-level) evidenceInoue N, Orías AAE, Segami K. Biomechanics of the Lumbar Facet Joint. Spine surgery and related research. 2020:4(1):1-7. doi: 10.22603/ssrr.2019-0017. Epub 2019 Apr 26 [PubMed PMID: 32039290]
Berger-Pasternak B, Brylka D, Sipko T. Lumbar Spine Kinematics in Asymptomatic People When Changing Body Position From Sitting to Standing. Journal of manipulative and physiological therapeutics. 2021 Feb:44(2):113-119. doi: 10.1016/j.jmpt.2020.07.014. Epub 2021 Jan 9 [PubMed PMID: 33431283]
Diebo BG, Balmaceno-Criss M, Lafage R, McDonald CL, Alsoof D, Halayqeh S, DiSilvestro KJ, Kuris EO, Lafage V, Daniels AH. Sagittal Alignment in the Degenerative Lumbar Spine: Surgical Planning. The Journal of bone and joint surgery. American volume. 2024 Mar 6:106(5):445-457. doi: 10.2106/JBJS.23.00672. Epub 2024 Jan 25 [PubMed PMID: 38271548]
Kalamchi L, Valle C. Embryology, Vertebral Column Development. StatPearls. 2025 Jan:(): [PubMed PMID: 31751107]
Tzika M, Paraskevas GK, Piagkou M, Papatolios AK, Natsis K. Basivertebral foramina of true vertebrae: morphometry, topography and clinical considerations. Surgical and radiologic anatomy : SRA. 2021 Jun:43(6):889-907. doi: 10.1007/s00276-021-02690-0. Epub 2021 Feb 17 [PubMed PMID: 33598754]
Zhao Q, Cheng L, Yan H, Deng S, Zhao J, Liu Z, Tan X, Zhong E, Zhuo W, Jin D, Li Q. The Anatomical Study and Clinical Significance of the Sinuvertebral Nerves at the Lumbar Levels. Spine. 2020 Jan 15:45(2):E61-E66. doi: 10.1097/BRS.0000000000003190. Epub [PubMed PMID: 31415472]
Quinones S, Konschake M, Aguilar LL, Simon C, Aragones P, Hernández LM, Abramovic A, Tubbs RS, Bouzada J, Valderrama-Canales FJ, Vazquez T, Sanudo J. Clinical anatomy of the lumbar sinuvertebral nerve with regard to discogenic low back pain and review of literature. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2021 Oct:30(10):2999-3008. doi: 10.1007/s00586-021-06886-1. Epub 2021 May 30 [PubMed PMID: 34052894]
Tran J, Peng P, Loh E. Anatomical study of the medial branches of the lumbar dorsal rami: implications for image-guided intervention. Regional anesthesia and pain medicine. 2022 May 19:():. pii: rapm-2022-103653. doi: 10.1136/rapm-2022-103653. Epub 2022 May 19 [PubMed PMID: 35589133]
Bailey JF, Liebenberg E, Degmetich S, Lotz JC. Innervation patterns of PGP 9.5-positive nerve fibers within the human lumbar vertebra. Journal of anatomy. 2011 Mar:218(3):263-70. doi: 10.1111/j.1469-7580.2010.01332.x. Epub 2011 Jan 12 [PubMed PMID: 21223256]
Konin GP, Walz DM. Lumbosacral transitional vertebrae: classification, imaging findings, and clinical relevance. AJNR. American journal of neuroradiology. 2010 Nov:31(10):1778-86. doi: 10.3174/ajnr.A2036. Epub 2010 Mar 4 [PubMed PMID: 20203111]
Castellvi AE, Goldstein LA, Chan DP. Lumbosacral transitional vertebrae and their relationship with lumbar extradural defects. Spine. 1984 Jul-Aug:9(5):493-5 [PubMed PMID: 6495013]
Chiu CK, Chin TF, Chung WH, Chan CYW, Kwan MK. Variations in the Number of Vertebrae, Prevalence of Lumbosacral Transitional Vertebra and Prevalence of Cervical Rib Among Surgical Patients With Adolescent Idiopathic Scoliosis: An Analysis of 998 Radiographs. Spine. 2024 Jan 1:49(1):64-70. doi: 10.1097/BRS.0000000000004711. Epub 2023 May 5 [PubMed PMID: 37146062]
Osiowski M, Osiowski A, Preinl M, Stolarz K, Klepinowski T, Jasiewicz B, Taterra D. Prevalence and characteristics of lumbar ribs: a meta-analysis with anatomical and clinical considerations. Surgical and radiologic anatomy : SRA. 2024 Dec:46(12):2057-2066. doi: 10.1007/s00276-024-03504-9. Epub 2024 Oct 8 [PubMed PMID: 39377983]
Level 1 (high-level) evidence