Introduction
Vertebrae, together with intervertebral discs, compose the vertebral column, also referred to as the "spine." The vertebral column extends from the skull to the coccyx and is divided into cervical, thoracic, lumbar, and sacral regions (see Image. Vertebral Column). The spine serves multiple vital roles, including protection of the spinal cord and branching spinal nerves, structural support for the thorax and abdomen, and facilitation of flexibility and mobility. Intervertebral discs permit mobility while preserving the supportive strength of the vertebral column.
The thoracic region contains 12 vertebrae, designated T1 to T12. Intervertebral discs, in conjunction with the laminae, pedicles, and articular processes of adjacent vertebrae, form spaces through which spinal nerves exit. The thoracic vertebrae collectively contribute to a kyphotic curvature of the vertebral column. Thoracic vertebrae are distinguished by an additional function of providing articulation sites for the ribs.[1][2][3]
Typical vertebrae consist of a vertebral body, a vertebral arch, and 7 processes (see Image. Typical Thoracic Vertebra Anatomy). The vertebral body bears the majority of the axial load transmitted through the vertebral column. Vertebral bodies increase in size from superior to inferior. The vertebral body is composed of trabecular bone containing red marrow, surrounded by a thin external layer of compact bone.
The vertebral arch, together with the posterior aspect of the vertebral body, forms the vertebral (spinal) canal, which contains the spinal cord. The arch consists of bilateral pedicles, which are cylindrical segments of bone connecting the arch to the vertebral body. The arch also includes bilateral laminae, which form most of the arch and connect the transverse and spinous processes.
A typical vertebra contains 4 articular processes, including 2 superior and 2 inferior processes. These processes articulate with the inferior and superior articular processes of adjacent vertebrae, respectively. The articulation between opposing articular facets forms a facet, or zygapophyseal, joint. Facet joints maintain vertebral alignment, limit excessive motion, and bear load in certain positions.
The spinous process projects posteriorly and inferiorly from the vertebral arch and may overlap inferior vertebrae to varying degrees, depending on the spinal region. Two transverse processes project laterally from the vertebral arch in a symmetric configuration.
Typical thoracic vertebrae exhibit several features that distinguish this region from the cervical and lumbar vertebrae. Vertebrae T5 to T8 are often considered the most representative, as these levels demonstrate features present across the thoracic region. The defining characteristic of thoracic vertebrae is the presence of costal facets.
Each thoracic vertebra contains 6 costal facets, including 2 facets on the transverse processes and 4 demifacets. Facets on the transverse processes articulate with the tubercle of the corresponding rib. The demifacets are bilaterally paired and located on the superior and inferior posterolateral aspects of the vertebral body. This arrangement permits articulation such that the superior demifacet of the inferior vertebra and the inferior demifacet of the superior vertebra both articulate with the head of the same rib. For example, the inferior demifacet of T4 and the superior demifacet of T5 articulate with the head of rib 5.
The length of the transverse processes progressively decreases from superior to inferior levels. The orientation of the ribs and the morphology of the spinous processes substantially limit flexion and extension within the thoracic spine. Vertebrae T5 to T8 demonstrate the greatest rotational capacity within the thoracic region.
Thoracic vertebrae possess superior articular facets oriented in a posterolateral direction. The spinous processes are elongated relative to other spinal regions and project posteroinferiorly. This angulation increases progressively through the midthoracic levels before decreasing rapidly from T9 to T12. Intervertebral disc height in the thoracic region is, on average, the smallest among the vertebral regions.
Three atypical vertebrae are present within the thoracic region (see Image. Atypical Thoracic Vertebrae). These vertebrae differ in costal facet configuration and articular morphology from typical thoracic vertebrae.
The superior costal facets of T1 are complete, or “whole,” costal facets. These facets articulate exclusively with the 1st rib. C7 lacks costal facets. T1 also contains typical inferior demifacets that articulate with the 2nd rib. The spinous process of T1 is elongated and resembles that of a cervical vertebra. In some individuals, the length approaches that of the vertebra prominens at C7.
Vertebrae T11 and T12 are atypical in that each contains a single pair of complete costal facets. These facets articulate with the 11th and 12th ribs, respectively. Facets on the transverse processes are absent at these levels. Anatomic variation may result in T10 exhibiting similar atypical characteristics. When this variation is present, T9 lacks an inferior demifacet, as articulation with the 10th rib is unnecessary.
Vertebra T12 is further distinguished by its transitional anatomy between the thoracic and lumbar regions. Thoracic characteristics include the presence of costal facets and superior articular facets that permit rotation and flexion. Lumbar characteristics include inferior articular processes oriented to restrict rotation while allowing flexion and extension. T12 also contains mammillary processes. These small tubercles are located on the posterior surface of the superior articular processes and serve as attachment sites for the intertransversarii and multifidus muscles.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Thoracic vertebrae are uniquely defined by costal facets that articulate with ribs, producing a rib-cage–coupled spinal segment optimized for stability and respiration rather than maximal flexion-extension. Typical thoracic vertebrae exhibit a heart-shaped vertebral body and a relatively circular vertebral foramen that encloses and protects the spinal cord. The spinous process is long and directed posteroinferiorly, serving as an extended lever arm for paraspinal muscle attachment. This posterior projection increases the moment arm of these muscles relative to the instantaneous axis of rotation of the thoracic motion segment, which, during flexion and extension, is located within the intervertebral disc. The resulting mechanical configuration improves the efficiency of paraspinal muscle action.
Thoracic zygapophyseal joints are oriented predominantly in the coronal plane relative to lumbar facets, shaping the thoracic spine’s characteristic biomechanics. This configuration restricts flexion, extension, and lateral bending while preserving axial rotation, as coronal facets favor rotational motion. Experimental stepwise-resection data indicate that facet capsules materially contribute to stability in axial rotation, explaining why capsular disruption, severe arthropathy, or surgical facetectomy can produce disproportionate rotational instability despite modest changes on neutral imaging.[4]
Costovertebral and costotransverse joints mechanically couple respiration with spinal stability. Ligamentous constraints maintain rib-spine congruence under cyclical loading, with respiratory motion functioning as repetitive microloading. A dedicated review of costovertebral joint ligaments emphasizes their underappreciated role in alignment and stability, supporting the clinical practice of evaluating costovertebral pathology in cases of focal thoracic pain that is posture- or respiration-sensitive.[5] Provocation studies demonstrate that costotransverse joints can refer pain in characteristic patterns, validating their consideration as therapeutic targets in carefully selected patients when explanations limited to facets and intervertebral discs are insufficient.[6]
The progressive increase in vertebral body size along the descending spinal column reflects the corresponding increase in weight-bearing requirements. Inferior vertebrae support a greater proportion of body mass than superior levels.[7]
Embryology
Vertebral development begins when paraxial mesoderm segments into somites, paired transient blocks of tissue that form sequentially along the craniocaudal axis adjacent to the neural tube. Somite formation is paced by the segmentation clock, consisting of coupled oscillations in Notch, Wnt, and fibroblast growth factor (FGF) signaling circuits. This process establishes segment boundaries and polarity, which later constrain vertebral number and alignment.[8]
Each somite differentiates into a sclerotome, which gives rise to vertebrae and ribs, and a dermomyotome, which forms skeletal muscle and dermis. Therefore, early segmentation errors predict coupled anomalies across bone, intervertebral discs, and paraspinal soft tissues, rather than isolated bony defects.
Sclerotome cells migrate around the notochord and neural tube. Through resegmentation, these cells recombine across adjacent somites to form vertebral bodies and neural arches aligned with spinal nerves and myotomes.[9] Intervertebral discs develop concurrently as composite structures. The nucleus pulposus originates from the embryonic notochord, whereas the annulus fibrosus and cartilaginous endplates are derived from the surrounding sclerotome.[10]
All vertebrae begin ossification during the embryonic period, approximately 8 weeks of gestation. Ossification occurs at 3 primary centers: 1 in the endochondral centrum, which develops into the vertebral body, and 1 in each neural process, which forms the pedicles. Ossification initiates at the thoracolumbar junction and progresses in both cranial and caudal directions. Neural processes fuse with the centrum between 3 and 6 years of age. During puberty, 5 secondary ossification centers emerge: at the tip of the spinous process, at both transverse processes, and on the superior and inferior surfaces of the vertebral body. Vertebral body ossification centers drive superoinferior growth of the vertebrae. Complete ossification is typically achieved around 25 years of age.[11]
Blood Supply and Lymphatics
Thoracic vertebrae receive segmental arterial inflow predominantly from the posterior intercostal arteries, with upper levels supplied via the subclavian system and the remaining levels via the thoracic aorta. These vessels give rise to periosteal and equatorial branches that continue into anterior and posterior vertebral canal branches. Nutrient branches enter the vertebral body to perfuse trabecular bone and marrow. Segmental vessels exhibit clinically significant anatomic variability in origin and dorsal course.[12] Segmental arteries also provide radiculomedullary branches that support spinal cord circulation, including the artery of Adamkiewicz. The artery of Adamkiewicz typically arises between T8 and L1, more often on the left side, and serves as the dominant feeder for the lower thoracic to lumbosacral spinal cord.[13]
Spinal veins form venous plexuses inside and outside the vertebral canal. These valveless plexuses permit bidirectional blood flow according to pressure gradients. Venous blood eventually drains into the segmental veins of the trunk.
Lymphatic structures relevant to thoracic vertebrae are predominantly mediastinal and paravertebral. The thoracic duct ascends from the cisterna chyli and courses anterior to the vertebral column within the posterior mediastinum. This lymphatic vessel passes between the aorta and the azygos vein, posterior to the esophagus near T7, and crosses from right to left near the T5 level before draining into the left venous angle.[14] Mediastinal lymph nodes, including posterior paravertebral groups, serve as a central hub for thoracic lymphatic drainage.
Nerves
Thoracic spinal nerves exit through the intervertebral foramina and divide into dorsal and ventral rami. Ventral rami form the intercostal nerves from T1 to T11, traveling within the intercostal spaces and carrying mixed motor and sensory fibers. Dorsal rami innervate intrinsic back musculature and posterior cutaneous territories and provide articular branches to thoracic zygapophyseal joints.
At thoracic levels, recurrent meningeal (sinuvertebral) branches reenter the vertebral canal via the intervertebral foramen. These branches provide segmental sensory innervation to pain-sensitive vertebral canal structures, including the posterior longitudinal ligament, dura, epidural vessels, annulus fibrosus, and periosteum of the vertebral body.[15] Posterior element and facet-joint nociception is primarily conveyed by medial branches of the dorsal ramus rather than sinuvertebral nerves.[16] Intraosseous vertebral body nerves typically enter posteriorly via the basivertebral foramen and course with nutrient vessels toward the endplates, establishing a functional pathway for vertebral body nociception.
Autonomic nervous system structures are closely associated with thoracic vertebrae. This relationship is exemplified by the thoracic sympathetic chain, which lies paravertebrally.
Muscles
Thoracic vertebrae serve as attachment points for layered intrinsic stabilizers and movers, including the semispinalis, multifidus, and rotatores, as well as short intersegmental muscles such as the interspinales and intertransversarii, which support segmental control. Thoracic vertebrae also anchor extrinsic muscles connecting the axial skeleton to the shoulder girdle and thoracic wall, including the trapezius, latissimus dorsi, rhomboids, serratus posterior, and splenius muscles.
Physiologic Variants
Segment Number Variants
The standard pattern of 12 thoracic vertebrae with 12 rib pairs is not universal. In a trauma population undergoing computed tomography (CT), 3.4% of individuals presented with 11 rib pairs.[17] Therefore, rib counting alone is an unreliable surrogate for vertebral numbering when a “missing” or “extra” rib is present.
Thoracolumbar transitional vertebrae (TLTV) occur at the thoracolumbar junction and partially retain both thoracic and lumbar morphological characteristics. TLTV further complicates thoracic numbering by blurring the rib-bearing definition of T12 versus L1. In a whole-spine CT study, TLTV occurred in 11.2% of cases, while abnormal rib counts were observed in 8.4%. Abnormal rib counts frequently cooccurred with TLTV and lumbosacral transitional vertebrae (LSTV).[18]
A radiographic study of asymptomatic young adults identified spinal segment distribution variants in 23.8%, including cervical ribs in 4.2%, TLTV in 15.3%, and LSTV in 26.4%.[19] Cervical ribs were associated with LSTV. A cervical rib can produce an off-by-1 error when counting caudally from C7, particularly in limited-field imaging studies. Conversely, a TLTV may make the last rib-bearing level appear thoracic despite its functional transitional nature. When any of these variants is present, subsequent thoracic imaging should maintain consistent numbering conventions across encounters to prevent longitudinal discordance.
Sagittal Alignment
Thoracic kyphosis is frequently considered normal up to 40°, yet healthy populations often exceed this threshold. A systematic review of healthy adults (n = 7,633) demonstrated a moderate positive correlation between kyphosis and age, with kyphosis exceeding 40° in 65% of cases.[20] No consistent sex differences were observed, while ethnicity influenced kyphosis magnitude. Clinically, rigid application of a 40° cutoff risks overdiagnosis of “hyperkyphosis” in older adults and misattribution of pain or dyspnea to alignment alone.
Surgical Considerations
Thoracic spine surgery presents unique challenges due to several anatomic factors. The spinal canal exhibits a narrow diameter. Critical vascular structures lie in close proximity, including the aorta, which overlies the left side from T3 to T7; the thoracic sympathetic chain, extending from T1 to T12; and the azygos vein, which crosses the lateral aspect of the spinal column at T4 to T5. Pedicles are relatively narrow, further complicating surgical access and instrumentation.
The thoracic spine’s rigid rib cage, kyphotic sagittal profile, and relatively narrow canal reduce spinal cord tolerance for retraction, translation, or rotational maneuvers, rendering surgical approach selection a critical consideration. Posterior midline exposure is efficient for dorsal compression and instrumentation but becomes hazardous for ventral pathology when decompression requires circumferential cord manipulation. Ventral disease should be addressed through anterolateral or posterolateral approaches, which provide direct access to the anterior canal while accepting pleural and pulmonary risk to prevent neurologic catastrophe.
Narrow and variable corridors limit thoracic pedicle screw instrumentation. The proximity of the spinal cord, pleura, and segmental vessels further constrains safe screw placement.
Thoracic spine procedures must explicitly account for cord perfusion because segmental radiculomedullary supply is variable, and interruption can produce rare but catastrophic infarction. Practical risk-reduction measures include maintaining robust intraoperative cord perfusion, minimizing the sacrifice of segmental arteries, and considering preoperative vascular mapping in high-risk multilevel exposures to identify the precise location of the artery of Adamkiewicz.
Intraoperative neuromonitoring is recommended for high-risk thoracic spine procedures. Continuous monitoring of spinal cord function helps detect early neurologic compromise and guide surgical maneuvers.
Clinical Significance
Spinal injuries cluster at the thoracolumbar junction (T11–L2) due to transitional biomechanics. These forces arise from the change between the rigid thoracic spine and the relatively mobile lumbar spine.
The thoracic spine possesses a relatively narrow vertebral canal, which increases susceptibility to spinal cord injury and neurologic deficit. The orientation of facet joints, thin intervertebral discs, and the ribcage confers functional rigidity. Consequently, a greater amount of energy is required to produce fractures and dislocations.
In acute trauma, fracture classification guides communication, imaging selection, and urgency of spine consultation. The Arbeitsgemeinschaft für Osteosynthesefragen Spine (AOSpine) thoracolumbar injury classification system categorizes injuries into type A compression, type B tension band disruption, and type C displacement or translation patterns, incorporating neurologic grading and clinically relevant modifiers.[21] The Thoracolumbar Injury Classification and Severity Score (TLICS) similarly evaluates morphology, posterior ligamentous complex integrity, and neurologic status to structure treatment decisions.[22]
The World Federation of Neurosurgical Societies (WFNS) recommendations support conservative management for compression-type and stable burst fractures in selected patients, with escalation to surgery when significant vertebral body damage, kyphotic angulation, neurologic deficit, or spinal canal compromise is present. Type B and C injuries, according to the AOSpine classification, are preferably managed surgically.[23]
Osteoporotic vertebral compression fractures (OVCF) frequently involve the thoracic and thoracolumbar spine and may be clinically indistinguishable from malignant or infectious fractures during early presentation. Morphologic stratification enhances triage.
The Deutsche Gesellschaft für Orthopädie und Unfallchirurgie (DGOU) osteoporotic fracture (OF) classification defines 5 groups, ranging from OF 1, vertebral edema without deformation, to OF 5, distraction or rotation injuries, and explicitly incorporates posterior wall involvement and collapse patterns that influence stability and neurologic risk (see Image. Osteoporotic Fracture Classification System).[24] The North American Spine Society (NASS) has summarized evidence-based recommendations for the diagnosis and management of adults with OVCF.[25] Vertebral augmentation is recommended for acute OVCF, as it provides rapid and sustained improvement in pain and function that is both clinically and statistically significant.
Thoracic vertebrae are frequent targets for metastatic disease and epidural extension, facilitated by the valveless vertebral venous plexus that permits bidirectional flow and hematogenous dissemination.[26] Approximately 10% of patients with spinal metastases develop metastatic epidural spinal cord compression (MESCC), and delayed recognition increases the risk of loss of ambulation.[27]
Management follows a structured framework. The NOMS paradigm integrates Neurologic status, Oncologic tumor behavior and radiosensitivity, Mechanical stability, and Systemic disease burden to link imaging findings to decompression, radiotherapy modality, and stabilization strategy.[28]
Mechanical instability may be assessed using the Spinal Instability Neoplastic Score (SINS). SINS evaluates 6 factors: tumor location, presence of mechanical pain, type of bone lesion, spinal alignment, degree of vertebral body collapse, and involvement of posterolateral spinal elements. Each factor is assigned a predefined numeric score based on clinical findings and imaging characteristics, and the scores are summed to obtain a total SINS value. Total scores range from 0 to 18, with categories defined as stable (0–6), potentially unstable (7–12), and unstable (13–18). Surgical consultation is recommended for scores between 7 and 18.[29]
Media
(Click Image to Enlarge)
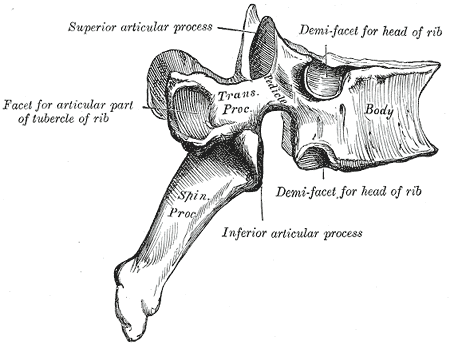
Typical Thoracic Vertebra Anatomy. The labeled diagram illustrates key features, including superior and inferior articular processes, spinous and transverse processes, vertebral body, and costal facets for rib articulation.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
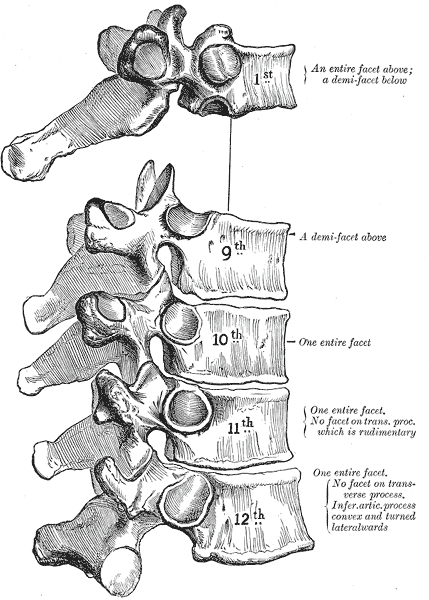
Atypical Thoracic Vertebrae. This labeled diagram shows T1 with a complete superior costal facet articulating with rib 1 and an inferior demifacet for rib 2. Transitional morphology occurs at T9 to T10 with paired demifacets. T10 to T12 exhibit complete costal facets for ribs 10 to 12, with T11 and T12 lacking transverse costal facets.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
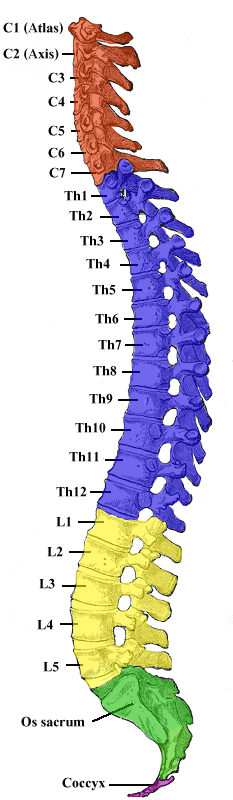
Vertebral Column. Schematic medial view of the entire vertebral column showing its 5 regions and their curvatures.
Contributed by Wikimedia Commons, Gray 111 (Public Domain)
(Click Image to Enlarge)
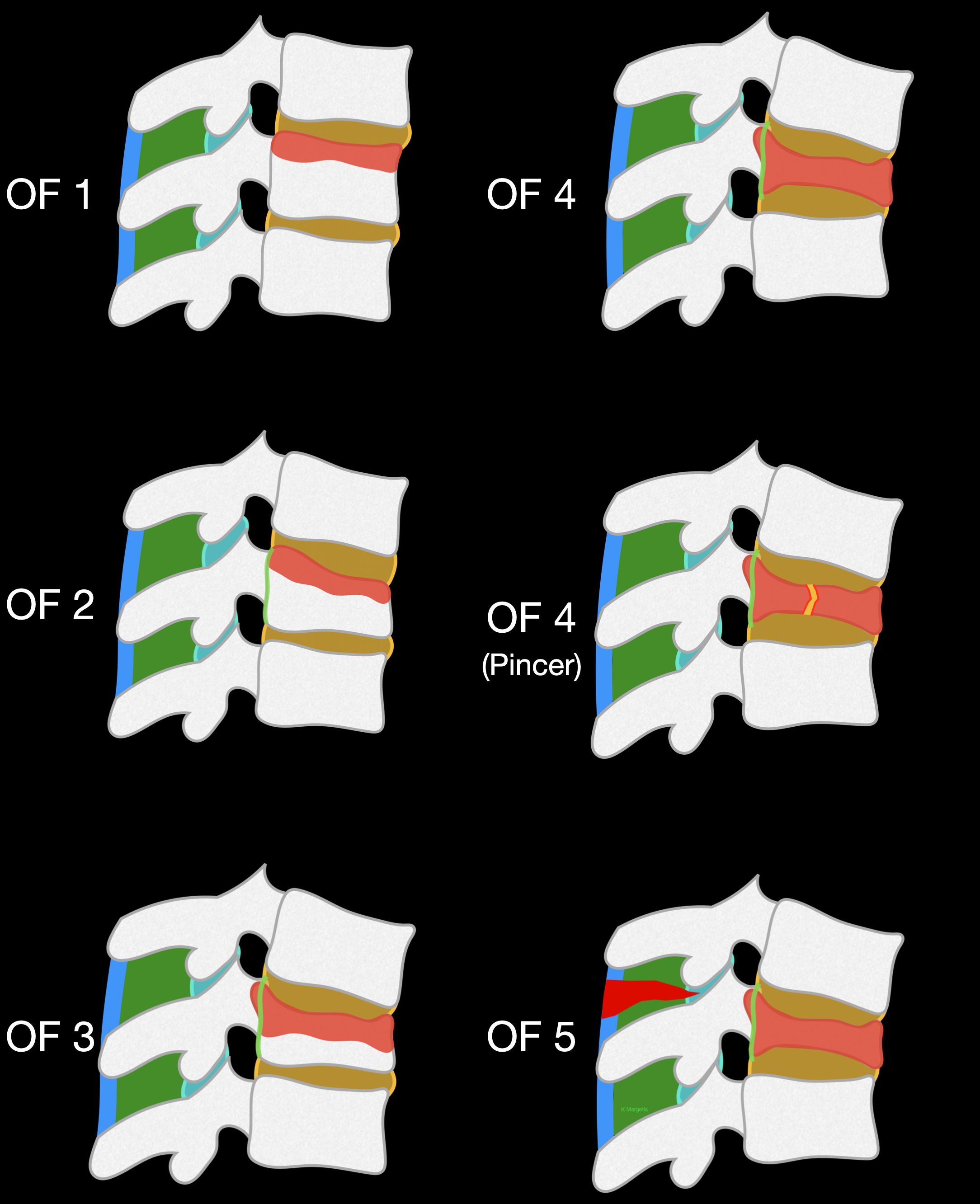
Osteoporotic Fracture Classification System. The DGOU (Deutsche Gesellschaft für Orthopädie und Unfallchirurgie) AOSpine (Arbeitsgemeinschaft für Osteosynthesefragen Spine) osteoporotic fracture classification system categorizes low-energy vertebral compression fractures based on the severity of vertebral body deformation and posterior wall involvement.
Contributed by K Margetis MD, PhD
References
DeSai C, Reddy V, Agarwal A. Anatomy, Back, Vertebral Column. StatPearls. 2025 Jan:(): [PubMed PMID: 30247844]
Mrozkowiak M, Walicka-Cupryś K, Magoń G. Comparison of Spinal Curvatures in the Sagittal Plane, as Well as Body Height and Mass in Polish Children and Adolescents Examined in the Late 1950s and in the Early 2000s. Medical science monitor : international medical journal of experimental and clinical research. 2018 Jun 30:24():4489-4500. doi: 10.12659/MSM.907134. Epub 2018 Jun 30 [PubMed PMID: 29959309]
Movahed A, Majdalany D, Gillinov M, Schiavone W. Association Between Myxomatous Mitral Valve Disease and Skeletal Back Abnormalities. The Journal of heart valve disease. 2017 Sep:26(5):564-568 [PubMed PMID: 29762925]
Wilke HJ, Grundler S, Ottardi C, Mathew CE, Schlager B, Liebsch C. In vitro analysis of thoracic spinal motion segment flexibility during stepwise reduction of all functional structures. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2020 Jan:29(1):179-185. doi: 10.1007/s00586-019-06196-7. Epub 2019 Oct 29 [PubMed PMID: 31664565]
Saker E, Graham RA, Nicholas R, D'Antoni AV, Loukas M, Oskouian RJ, Tubbs RS. Ligaments of the Costovertebral Joints including Biomechanics, Innervations, and Clinical Applications: A Comprehensive Review with Application to Approaches to the Thoracic Spine. Cureus. 2016 Nov 11:8(11):e874 [PubMed PMID: 27994992]
Young BA, Gill HE, Wainner RS, Flynn TW. Thoracic costotransverse joint pain patterns: a study in normal volunteers. BMC musculoskeletal disorders. 2008 Oct 15:9():140. doi: 10.1186/1471-2474-9-140. Epub 2008 Oct 15 [PubMed PMID: 18922181]
Bogduk N. Functional anatomy of the spine. Handbook of clinical neurology. 2016:136():675-88. doi: 10.1016/B978-0-444-53486-6.00032-6. Epub [PubMed PMID: 27430435]
Carraco G, Martins-Jesus AP, Andrade RP. The vertebrate Embryo Clock: Common players dancing to a different beat. Frontiers in cell and developmental biology. 2022:10():944016. doi: 10.3389/fcell.2022.944016. Epub 2022 Aug 11 [PubMed PMID: 36036002]
Ward L, Evans SE, Stern CD. A resegmentation-shift model for vertebral patterning. Journal of anatomy. 2017 Feb:230(2):290-296. doi: 10.1111/joa.12540. Epub 2016 Sep 1 [PubMed PMID: 27580767]
Alkhatib B, Ban GI, Williams S, Serra R. IVD Development: Nucleus pulposus development and sclerotome specification. Current molecular biology reports. 2018 Sep:4(3):132-141. doi: 10.1007/s40610-018-0100-3. Epub 2018 Jul 13 [PubMed PMID: 30505649]
Kalamchi L, Valle C. Embryology, Vertebral Column Development. StatPearls. 2025 Jan:(): [PubMed PMID: 31751107]
Kocbek L, Krajnc I, Anderhuber F. Anatomical variations of the posterior intercostal arteries and the thoracic vertebral artery. The Journal of international medical research. 2011:39(3):1001-5 [PubMed PMID: 21819734]
Taterra D, Skinningsrud B, Pękala PA, Hsieh WC, Cirocchi R, Walocha JA, Tubbs RS, Tomaszewski KA, Henry BM. Artery of Adamkiewicz: a meta-analysis of anatomical characteristics. Neuroradiology. 2019 Aug:61(8):869-880. doi: 10.1007/s00234-019-02207-y. Epub 2019 Apr 27 [PubMed PMID: 31030251]
Level 1 (high-level) evidenceIlahi M, St Lucia K, Ilahi TB. Anatomy, Thorax, Thoracic Duct. StatPearls. 2025 Jan:(): [PubMed PMID: 30020599]
Gkasdaris G, Tripsianis G, Kotopoulos K, Kapetanakis S. Clinical anatomy and significance of the thoracic intervertebral foramen: A cadaveric study and review of the literature. Journal of craniovertebral junction & spine. 2016 Oct-Dec:7(4):228-235 [PubMed PMID: 27891032]
Shayota B, Wong TL, Fru D, David G, Iwanaga J, Loukas M, Tubbs RS. A comprehensive review of the sinuvertebral nerve with clinical applications. Anatomy & cell biology. 2019 Jun:52(2):128-133. doi: 10.5115/acb.2019.52.2.128. Epub 2019 Jun 30 [PubMed PMID: 31338228]
Gonzales-Portillo GS, Rizvi O, Avila MJ, Dumont TM. The prevalence of 11 ribs and its potential implications in spine surgery. Clinical neurology and neurosurgery. 2021 Apr:203():106544. doi: 10.1016/j.clineuro.2021.106544. Epub 2021 Feb 4 [PubMed PMID: 33711639]
Doo AR, Lee J, Yeo GE, Lee KH, Kim YS, Mun JH, Han YJ, Son JS. The prevalence and clinical significance of transitional vertebrae: a radiologic investigation using whole spine spiral three-dimensional computed tomographic images. Anesthesia and pain medicine. 2020 Jan 31:15(1):103-110. doi: 10.17085/apm.2020.15.1.103. Epub [PubMed PMID: 33329798]
Yoon ES, Pishgar F, Chhabra A, Del Grande F, Carrino JA. Frequency of Coexistent Spinal Segment Variants: Retrospective Analysis in Asymptomatic Young Adults. AJNR. American journal of neuroradiology. 2023 Dec 29:45(1):119-126. doi: 10.3174/ajnr.A8071. Epub 2023 Dec 29 [PubMed PMID: 38123916]
Level 2 (mid-level) evidenceZappalá M, Lightbourne S, Heneghan NR. The relationship between thoracic kyphosis and age, and normative values across age groups: a systematic review of healthy adults. Journal of orthopaedic surgery and research. 2021 Jul 9:16(1):447. doi: 10.1186/s13018-021-02592-2. Epub 2021 Jul 9 [PubMed PMID: 34243795]
Level 1 (high-level) evidenceVaccaro AR, Oner C, Kepler CK, Dvorak M, Schnake K, Bellabarba C, Reinhold M, Aarabi B, Kandziora F, Chapman J, Shanmuganathan R, Fehlings M, Vialle L, AOSpine Spinal Cord Injury & Trauma Knowledge Forum. AOSpine thoracolumbar spine injury classification system: fracture description, neurological status, and key modifiers. Spine. 2013 Nov 1:38(23):2028-37. doi: 10.1097/BRS.0b013e3182a8a381. Epub [PubMed PMID: 23970107]
Lee JY, Vaccaro AR, Lim MR, Oner FC, Hulbert RJ, Hedlund R, Fehlings MG, Arnold P, Harrop J, Bono CM, Anderson PA, Anderson DG, Harris MB, Brown AK, Stock GH, Baron EM. Thoracolumbar injury classification and severity score: a new paradigm for the treatment of thoracolumbar spine trauma. Journal of orthopaedic science : official journal of the Japanese Orthopaedic Association. 2005 Nov:10(6):671-5 [PubMed PMID: 16307197]
Peev N, Zileli M, Sharif S, Arif S, Brady Z. Indications for Nonsurgical Treatment of Thoracolumbar Spine Fractures: WFNS Spine Committee Recommendations. Neurospine. 2021 Dec:18(4):713-724. doi: 10.14245/ns.2142390.195. Epub 2021 Dec 31 [PubMed PMID: 35000324]
Schnake KJ, Blattert TR, Hahn P, Franck A, Hartmann F, Ullrich B, Verheyden A, Mörk S, Zimmermann V, Gonschorek O, Müller M, Katscher S, Saman AE, Pajenda G, Morrison R, Schinkel C, Piltz S, Partenheimer A, Müller CW, Gercek E, Scherer M, Bouzraki N, Kandziora F, Spine Section of the German Society for Orthopaedics and Trauma. Classification of Osteoporotic Thoracolumbar Spine Fractures: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Global spine journal. 2018 Sep:8(2 Suppl):46S-49S. doi: 10.1177/2192568217717972. Epub 2018 Sep 7 [PubMed PMID: 30210960]
Cho CH, Hwang SW, Mazanec DJ, O'Toole JE, Watters WC 3rd, Annaswamy TM, Brook AL, Cheng DS, Christie SD, Cupler ZA, Enix DE, Eskay-Auerbach M, Goehl JM, Jones GA, Kalakoti P, Kasliwal MK, Kavadi NU, Kilincer C, Lantz JM, Rahmathulla G, Reinsel T, Shaw KA, Shawky Abdelgawaad A, Skuteris AM, Stone JA, Strayer AL, Vo AN. Guideline summary review: an evidence-based clinical guideline for the diagnosis and treatment of adults with osteoporotic vertebral compression fractures. The spine journal : official journal of the North American Spine Society. 2025 Aug:25(8):1670-1687. doi: 10.1016/j.spinee.2025.01.016. Epub 2025 Jan 31 [PubMed PMID: 39894268]
Carpenter K, Decater T, Iwanaga J, Maulucci CM, Bui CJ, Dumont AS, Tubbs RS. Revisiting the Vertebral Venous Plexus-A Comprehensive Review of the Literature. World neurosurgery. 2021 Jan:145():381-395. doi: 10.1016/j.wneu.2020.10.004. Epub 2020 Oct 10 [PubMed PMID: 33049379]
Van den Brande R, Thijs D, Bilsky M, Peeters M, Billiet C, Van de Kelft E. Treatment of ambulatory patients with metastatic epidural spinal cord compression: a systematic review and meta-analysis. Journal of neurosurgery. Spine. 2024 Feb 1:40(2):175-184. doi: 10.3171/2023.8.SPINE23541. Epub 2023 Oct 27 [PubMed PMID: 37890190]
Level 1 (high-level) evidenceLaufer I, Rubin DG, Lis E, Cox BW, Stubblefield MD, Yamada Y, Bilsky MH. The NOMS framework: approach to the treatment of spinal metastatic tumors. The oncologist. 2013 Jun:18(6):744-51. doi: 10.1634/theoncologist.2012-0293. Epub 2013 May 24 [PubMed PMID: 23709750]
Fisher CG, Schouten R, Versteeg AL, Boriani S, Varga PP, Rhines LD, Kawahara N, Fourney D, Weir L, Reynolds JJ, Sahgal A, Fehlings MG, Gokaslan ZL. Reliability of the Spinal Instability Neoplastic Score (SINS) among radiation oncologists: an assessment of instability secondary to spinal metastases. Radiation oncology (London, England). 2014 Mar 4:9():69. doi: 10.1186/1748-717X-9-69. Epub 2014 Mar 4 [PubMed PMID: 24594004]