Introduction
Vertebrae, together with intervertebral discs, compose the vertebral column or spine. The spine extends from the skull to the coccyx and comprises the cervical, thoracic, lumbar, and sacral regions. Major functions include protection of the spinal cord and branching spinal nerves, support for the thorax and abdomen, and facilitation of flexibility and mobility. Intervertebral discs confer mobility while maintaining the structural integrity of the vertebral column.
The cervical region contains 7 vertebrae, C1 to C7, the smallest within the vertebral column. Intervertebral discs, laminae, and articular processes of adjacent vertebrae form spaces through which spinal nerves exit. The intervertebral foramen is bounded anteriorly by vertebral bodies and discs, superiorly and inferiorly by pedicles, and posteriorly by facet joints, capsules, and the ligamentum flavum. The lamina is not typically considered a primary boundary.
Cervical vertebrae collectively generate a lordotic curve. Although vertebrae share general morphologic features, several distinctive characteristics are present in the cervical region (see Image. Comparative Anatomy of Typical and Atypical Cervical Vertebrae).[1]
A typical vertebra consists of a vertebral body, a vertebral arch, and 7 processes. The vertebral body bears the majority of axial load and increases in size from superior to inferior. The body comprises trabecular bone containing red marrow, surrounded by a thin layer of compact bone. The vertebral arch, together with the posterior aspect of the body, forms the vertebral (spinal) canal, which houses the spinal cord (see Image. Cervical Spine Magnetic Resonance Imaging in Multiple Views). The arch includes bilateral pedicles, cylindrical bone structures connecting the arch to the body, and bilateral laminae, flat bone segments forming most of the arch and connecting the transverse and spinous processes (see Image. Computed Tomography Anatomy of the Cervical Vertebrae).
Each vertebra contains 4 articular processes—2 superior and 2 inferior—that articulate with the inferior and superior articular processes of adjacent vertebrae, respectively. The junction of superior and inferior articular facets forms a facet, or zygapophyseal, joint. These joints maintain vertebral alignment, regulate the range of motion, and bear weight in certain positions. The spinous process projects posteriorly and often inferiorly from the vertebral arch, overlapping the inferior vertebra to variable degrees, depending on the spinal region. Two transverse processes extend laterally from the vertebral arch symmetrically.
Typical cervical vertebrae exhibit several features distinct from thoracic and lumbar vertebrae. The most notable distinction is the presence of a transverse foramen in each transverse process. These foramina encircle the vertebral arteries and veins. In most individuals, the vertebral artery enters the transverse foramen at C6 and ascends through C6 to C1. Variants include entry at other levels, such as C5 or C7. The C7 transverse foramen frequently transmits a vein and sympathetic plexus rather than the artery, although this pattern is not universal.
Another feature unique to cervical vertebrae is the bifid spinous process, which may increase the surface area available for muscle attachment (see Physiologic Variants). Spinous process length increases progressively from superior to inferior cervical vertebrae. Superior articular facets of cervical vertebrae generally face posteriorly, although studies indicate that more inferior vertebrae may have superior facets oriented posterolaterally, resembling thoracic vertebrae. Cervical vertebrae also demonstrate the greatest relative disc height, defined as the disc height-to-vertebral body height ratio, contributing to an increased range of motion.
Three atypical vertebrae are present in the cervical region. These atypical vertebrae include C1, C2, and C7.
C1, also referred to as the "atlas," is unique among all vertebrae in lacking both a vertebral body and a spinous process. The relatively circular bone contains 2 bilateral masses that function in load-bearing in place of a body. Superior articular facets of these masses articulate with the occipital condyles of the skull, and inferior facets articulate with the superior facets of C2.
C2, also called the "axis," is characterized by bilateral masses for articulation with C1, a vertebral body transmitting weight to C3 and inferior vertebrae, and an odontoid process, or dens, projecting from the superior aspect of the body. The dens articulates with the posterior surface of the anterior arch of C1.
C7 may be classified as typical or atypical and exhibits 2 distinguishing features. First, the vertebral artery typically does not traverse the transverse foramen. Second, C7 possesses a long spinous process, termed "vertebra prominens."[2]
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
Cervical vertebral anatomy is optimized for mobility while maintaining protected neurovascular transit. The smaller size of cervical vertebrae relative to thoracic and lumbar regions reflects reduced load-bearing requirements. This decreased size permits the greatest range of motion among all vertebral segments. Transverse and spinous processes function as attachment points and leverage for cervical and upper thoracic musculature (see Image. Cervical Spine Radiographic Anatomy and Motion). In the absence of a vertebral body, C1 transmits load primarily through the lateral masses rather than a body-disc complex.
Atlantooccipital joints contribute predominantly to head flexion and extension, whereas subaxial segments largely facilitate overall cervical flexion-extension and lateral bending. The dens of C2 serves as a pivot around which C1 rotates, enabling head rotation in the transverse plane. The C1–C2 joint accounts for the majority of cervical axial rotation due to its pivot structure and ligamentous constraints.[3]
Cervical motion is normally coupled, with lateral bending accompanied by ipsilateral axial rotation in the subaxial spine, resulting from facet orientation and uncovertebral guidance. Coupled motion is an inherent property of the cervical spine, arising from facet orientation and the constrained geometry of each motion segment.[4]
In typical subaxial vertebrae, the vertebral body and intervertebral disc constitute the anterior load-bearing column, whereas posterior elements, including pedicles, laminae, spinous process, and paired articular processes, form a protective arch and provide leverage for motion (see Image. Computed Tomography Anatomy of the Cervical Spine). Facet joints are synovial structures that guide movement and resist excessive translation, supporting controlled mobility rather than unrestricted motion. In the subaxial cervical spine (C3–C7), uncinate processes form uncovertebral joints that direct translation and contribute to coupled motion during lateral bending and rotation.[5] In vivo cervical kinematics demonstrate that motion is not uniformly distributed across vertebral levels. Flexion-extension and lateral bending occur predominantly in the subaxial spine, whereas C1–C2 provides the primary contribution to axial rotation.[6]
Ligaments of the Vertebral Column
The anterior longitudinal ligament (ALL) is positioned anterior to vertebral bodies and intervertebral discs, extending from the base of the skull to the sacrum. The ALL functions as a major anterior stabilizer and limits excessive extension across motion segments. The ligament also prevents anterior protrusion of herniated intervertebral discs.
The posterior longitudinal ligament (PLL) lies within the vertebral canal posterior to the vertebral bodies and connects intervertebral discs from C2 to the sacrum.[7] Absence of attachment to C1 corresponds to the lack of an intervertebral disc at the atlas. The PLL continues superiorly as the tectorial membrane, which is tightly attached to the clivus, passes over the atlantoaxial joint, and attaches firmly to the axis. Imaging evaluation of the tectorial membrane is critical in the assessment of patients with suspected traumatic craniovertebral dislocation.[8]
The PLL reinforces the posterior aspect of vertebral bodies and intervertebral discs within the spinal canal and contributes to the restraint of excessive flexion and posterior translation. This ligament prevents direct posterior dislocation of the nucleus pulposus during disc herniation. Herniated material typically passes lateral to the PLL. Rich innervation with nociceptive fibers, associated with the meningeal branch of each spinal nerve, contributes to the pain experienced during disc herniation.[9]
The PLL may undergo ossification, a condition known as ossification of the PLL (OPLL), which is associated with cervical myelopathy. In patients with cervical OPLL, the extent of ossified lesions throughout the spine correlates with female sex and higher body mass index.[10] Genetic factors may also contribute to disease development.
Each zygapophyseal joint possesses a joint capsule. Cervical joint capsules are particularly thin, facilitating increased movement of these joints.
The ligamenta flava (singular: ligamentum flavum) consist of thin connective tissue bands that connect adjacent laminae. These ligaments are relatively thin in the cervical region and increase in thickness in more caudal regions. Progressing caudally along the vertebral column, the ligamenta flava become broader and stronger. Composed primarily of elastic tissue, the ligamenta flava resist separation of the laminae during flexion of the vertebral column.
Interspinous ligaments connect adjacent spinous processes. In the cervical region, these ligaments merge with the ligamentum nuchae, a fibroelastic structure that extends from the base of the skull to the cervical vertebrae.
The atlas articulates with the occipital condyles, forming a joint that permits substantial flexion-extension and lateral flexion. Axial rotation at this joint is comparatively limited.
Ligamentous stabilization of the craniovertebral joint is provided by the alar, apical, and cruciate ligaments, as well as the tectorial membrane. The atlas and cranium are connected by the atlantooccipital membranes, which limit excessive joint motion. The transverse ligament of the atlas attaches to tubercles on the medial aspects of the lateral masses of C1. Superior and inferior vertical bands added to the transverse ligament form the cruciate ligament of the atlas. The alar ligaments extend from the dens to the lateral margins of the foramen magnum. Collectively, these ligaments restrict translation and rotation at the craniovertebral junction while permitting physiologic motion.[11][12]
Ligament integrity represents the primary determinant of stability at the craniovertebral junction. The absence of a vertebral body at C1 and the lack of an intervertebral disc at C1–C2 shift restraint demands on the transverse atlantal and alar ligaments. Biomechanical studies demonstrate failure of the transverse atlantal ligament (TAL) at lower force thresholds in elderly specimens, supporting a low threshold for clinical suspicion of instability in older patients, even after low-energy mechanisms.[13]
Ligamentous injury constitutes an important component of cervical trauma, including whiplash injury.[14] Herniated intervertebral discs occur in the cervical region, although lumbar involvement is more common. Cervical disc herniation carries an increased risk because the nucleus pulposus may compress the spinal cord. Vertebral bone marrow edema has been reported to correlate with herniated intervertebral discs, although the clinical significance of this finding remains controversial.[15]
Embryology
Vertebrae arise from somite-derived sclerotome, whereas intervertebral discs incorporate a notochord-derived nucleus pulposus.[16] Vertebral ossification begins in early fetal life, with primary ossification centers detectable by the 8th gestational week.[17]
A typical vertebra ossifies from 3 primary centers. A centrum forms the vertebral body, and paired neural process centers contribute to the pedicles and posterior elements. Ossification commences at the thoracolumbar junction and progresses in both cranial and caudal directions. Neural processes fuse with the centrum between 3 and 6 years of age.
During puberty, 5 secondary ossification centers develop at the tip of the spinous process, the tips of both transverse processes, and the superior and inferior surfaces of the vertebral body. Secondary centers on the vertebral body contribute to superior-inferior vertebral growth. Vertebral ossification typically completes by approximately 25 years of age.
Ossification is more complex at the craniocervical junction than at other vertebral levels, with multiple synchondroses and variable closure timing that may persist into later childhood. The atlas ossifies from the lateral masses and variable anterior arch centers, with posterior arch closure typically occurring in early childhood and anterior arch closure completing later in childhood or adolescence. The axis ossifies from multiple centers, including the dens, with fusion of subdental and neurocentral synchondroses taking place in later childhood and apical dens maturation continuing into the 2nd decade.[18][19]
Blood Supply and Lymphatics
Cervical vertebrae receive segmental arterial supply from branches of the vertebral and ascending cervical arterial systems, with clinically relevant nutrient channels perforating the anterior vertebral surface. A cadaveric study of anterior cervical blood supply demonstrated that nutrient vessels perforating cervical vertebrae arise from a vascular leash within the prevertebral fascia over the longus coli, originating from the ascending cervical artery with variable contribution from the transverse cervical artery. This relationship has clinical relevance because aggressive prevertebral dissection, prolonged retraction, or extensive longus coli elevation may disrupt nutrient inflow and plausibly contribute to impaired osseous healing and characteristic interface bleeding patterns during anterior approaches.[20]
The segmental course of the vertebral artery represents the dominant vascular hazard in cervical osseous procedures, and the prevalence of anatomic variants supports proactive imaging when surgical corridors approach the transverse foramen or the C1 sulcus. Contemporary anatomic synthesis describes a 4-segment model (V1–V4), with V2 traversing the transverse foramina and V3 looping around C1 before dural entry, a framework that predicts levels at risk during decompression, lateral dissection, and instrumentation.[21] Pooled anatomic data indicate that 92% of vertebral arteries enter the transverse foramen at C6, whereas a substantial minority enter at other levels, shifting the artery into unexpected exposure planes.[22]
Venous outflow from cervical vertebrae and adjacent paravertebral tissues occurs through the vertebral venous plexus (VVP, or Batson plexus), an interconnected network comprising the internal vertebral venous plexus (epidural), external vertebral venous plexus (paravertebral), and basivertebral veins within the vertebral bodies. The VVP freely intercommunicates along the spinal column and has clinical importance because this anatomy facilitates hematogenous spread and represents a major source of intraoperative epidural bleeding during intraspinal exposures, including decompression.[23]
In the craniocervical region, the suboccipital cavernous sinus forms a paired venous sinus complex surrounding the vertebral artery groove. This anatomy explains the potential for brisk venous bleeding in proximity to the V3 segment during surgical exposure.[24]
Unlike many cervical soft tissues, clinically significant dissemination from vertebral infection or malignancy is more commonly attributed to hematogenous pathways, particularly through vertebral venous networks. A distinct, well-characterized intrinsic vertebral lymphatic drainage system is not emphasized in standard surgical anatomy descriptions.
Nerves
Vertebral and perivertebral nociception is mediated largely by meningeal branches of spinal nerves, classically described within the sinuvertebral nerve system, which innervates pain-sensitive spinal structures. A contemporary review synthesizes sinuvertebral nerve anatomy and clinical applications, supporting the observation that pain arising from the posterior annulus, PLL, dura, and adjacent periosteal structures is transmitted through recurrent meningeal branches.[25]
Muscles
Cervical vertebrae provide points of attachment for numerous muscles, including erector spinae, interspinales, intertransversarii, levator scapulae, multifidus, obliquus capitis, rectus capitis, rhomboid minor, rotatores, semispinalis, splenius capitis, and trapezius. These vertebrae serve as attachment sites for layered muscular systems that collectively stabilize the cervical spine, control head posture, and enable coordinated motion in flexion, extension, rotation, and lateral bending. Muscles operate in balanced agonist–antagonist groups to maintain cervical lordosis and protect the spinal cord and vertebral arteries during both static posture and dynamic movement.
Deep cervical muscles provide primary segmental stability and fine motor control.[26] Deep posterior muscles, including the multifidus and semispinalis cervicis, attach directly to spinous processes and laminae, generating short-lever-arm forces that resist shear and control intersegmental motion. Deep anterior muscles, such as the longus colli and longus capitis, attach to vertebral bodies and transverse processes, contributing to anterior column stabilization and cervical lordosis maintenance, particularly during sustained upright posture. Dysfunction or fatigue of these deep stabilizers shifts load to passive structures and more superficial muscles, altering normal biomechanics.
The suboccipital muscles form a specialized functional unit spanning the occiput, atlas, and axis, optimized for precision head positioning rather than gross power generation. These short muscles provide fine-tuned control of atlantooccipital and atlantoaxial motion, particularly in extension and axial rotation, and contain a high density of muscle spindles, consistent with a primary proprioceptive role in head–neck coordination.[27] Attachments of these muscles place them in close anatomic relationship to the posterior arch of C1 and the spinous process of C2, supporting rapid reflexive adjustments that stabilize gaze and head orientation.
Intermediate and superficial cervical muscles, including the splenius, semispinalis capitis, trapezius, levator scapulae, and sternocleidomastoid, generate larger torque for gross head and neck movements and link cervical motion to shoulder girdle and thoracic posture.[28] These muscles coordinate cervical movement with upper extremity activity, distributing mechanical loads across the cervicothoracic junction and reducing focal stress on individual vertebral segments. Normal function depends on coordinated activation patterns rather than isolated muscle strength, highlighting that cervical motion is a multisegmental process rather than single-level movement.
Collectively, the cervical musculature enables the vertebral column to function as a stable yet mobile unit, balancing flexibility with protection of neural and vascular structures. Proper muscle function maintains alignment, modulates load transmission through the vertebrae, and provides proprioceptive feedback essential for posture, balance, and coordinated head movement.
Physiologic Variants
The bifid spinous process is a characteristic feature of cervical vertebrae but is not uniformly present across all levels or individuals. Consistent bifidity is reliably observed only at C2 to C4, with prevalence declining progressively at more caudal levels. C7 demonstrates the lowest likelihood of bifidity, occurring in approximately 0.3% of the population. Large imaging series indicate that C6 is monofid in nearly half of individuals, whereas C7 is monofid in over 99%, confirming that a truly bifid C7 spinous process is exceedingly uncommon.[29] Therefore, spinous process morphology alone is an unreliable guide for intraoperative level identification and may lead to wrong-level exposure. Accurate level localization should be confirmed with fluoroscopy or navigation rather than anatomic inspection alone.
The C1–C2 intervertebral articulation is the only vertebral level that lacks an intervertebral disc. Unfused synchondroses and secondary ossification centers at C1 and C2 can simulate fractures on radiographs or computed tomography (CT), particularly at the craniocervical junction, where multiple fusion fronts converge. A pediatric CT study mapped expected atlas and axis ossification patterns and synchondrosis fusion timelines to distinguish normal developmental lucencies from injury.[30] When injury mechanism, persistent midline tenderness, neurologic findings, or malalignment are discordant with “benign-appearing” lucencies, magnetic resonance imaging (MRI) serves as the decision pivot to detect marrow edema, ligament disruption, and SCIWORA (spinal cord injury without radiographic abnormality) patterns that CT can miss.[31]
Osseous bridges and transverse foramen variants can reduce the vertebral artery safety margin and should be explicitly reported, as they alter screw trajectory planning and procedural risk during posterior cervical approaches and injections. "Ponticulus posticus" refers to an osseous bridge over the vertebral artery groove of the atlas, whereas "foramen arcuale" denotes the bony canal formed when this bridge is complete.
Meta-analytic data indicate that ponticulus posticus occurs in 16.7% of individuals overall, with complete bridges in 9.3%, demonstrating that a substantial minority of patients exhibit partial or complete osseous enclosure of the V3 segment of the vertebral artery.[32] These osseous bridges can produce a false impression of a broader posterior arch corridor, obscure the true arterial course, and increase the risk of vertebral artery injury during C1 instrumentation unless recognized on preoperative CT.
Os odontoideum is a smooth, corticated ossicle separated from the C2 base and is clinically significant because C1–C2 stability is predominantly ligamentous in a segment that lacks an intervertebral disc. Incidence was 0.11% in a large retrospective series.[33]
Cervical ribs are often incidental findings but are strongly associated with thoracic outlet syndrome via brachial plexus or subclavian compression. The presence of these ribs should prompt symptom-directed counseling and triage rather than reflex referral in asymptomatic patients. Meta-analysis estimates prevalence at 1.1% in healthy populations versus 29.5% in thoracic outlet syndrome cohorts. Among symptomatic patients with cervical ribs, 51.3% exhibit vascular and 48.7% neurogenic thoracic outlet syndrome, informing urgency and imaging selection.[34]
Surgical Considerations
The position of the foramen transversarium is critical because it transmits the vertebral artery. This spatial orientation is particularly important during posterior lateral mass screw placement in the subaxial cervical spine or transarticular screw implantation for atlantoaxial fixation, as misdirection of a screw can injure the artery, potentially causing significant neurological deficits and catastrophic bleeding.
Vertebral artery anatomy is variable, and clinically relevant variants in origin, dominance, tortuosity, and foraminal relationships make imaging-guided planning mandatory when instrumentation approaches the transverse foramen or upper-cervical screw corridors. Although iatrogenic vertebral artery injury is uncommon overall, population-level data indicate that risk is procedure-dependent and increases substantially in C1–C2 posterior fusion, supporting a lower threshold for preoperative vascular mapping in those cases.[35]
Cervical pedicle screws provide biomechanical advantages but traverse millimeter-scale corridors adjacent to the spinal canal and transverse foramina. This anatomy supports selective use of navigation for pedicle screw placement in small pedicles, deformity, revision procedures, or aberrant vascular anatomy.[36]
Clinical Significance
Atlas fractures are uncommon but clinically important because instability is determined by TAL integrity rather than bony fracture pattern alone. In unstable atlas fractures with TAL injury, multicenter comparative data demonstrate higher osseous healing with surgical fixation compared with halo-vest immobilization and highlight the limitations of external immobilization in maintaining reduction.[37]
Odontoid process fractures may occur via hyperflexion, with or without anterior deviation of the dens and atlas. Fractures may also occur via hyperextension, with or without posterior displacement of the dens and atlas.
Hangman's fracture is a bilateral spondylolisthesis of C2 resulting from hyperextension-distraction, in which the pars interarticularis of C2 fractures and the C2 body is displaced relative to C3. The Levine and Edwards classification describes 4 subtypes of this injury. The eponym is misleading, as this fracture is rarely observed in hanging victims and occurs most commonly in automotive collisions.
Cervical spondylosis is a degenerative disease affecting the spine, intervertebral discs, ligaments, and cartilage. The condition is common in individuals older than 40 years, with age and occupation representing the primary risk factors. Cervical spondylosis significantly increases the likelihood of cervical radiculopathy, defined as nerve root compression, and cervical spondylotic myelopathy, which involves spinal cord compression.
Electromyography and nerve conduction studies assess the severity of nerve damage, while MRI detects abnormalities of bone, spinal cord, and intervertebral discs. Depending on severity, these conditions may be managed with conservative measures, including anti-inflammatory medication and physical therapy, or surgical intervention.
Media
(Click Image to Enlarge)
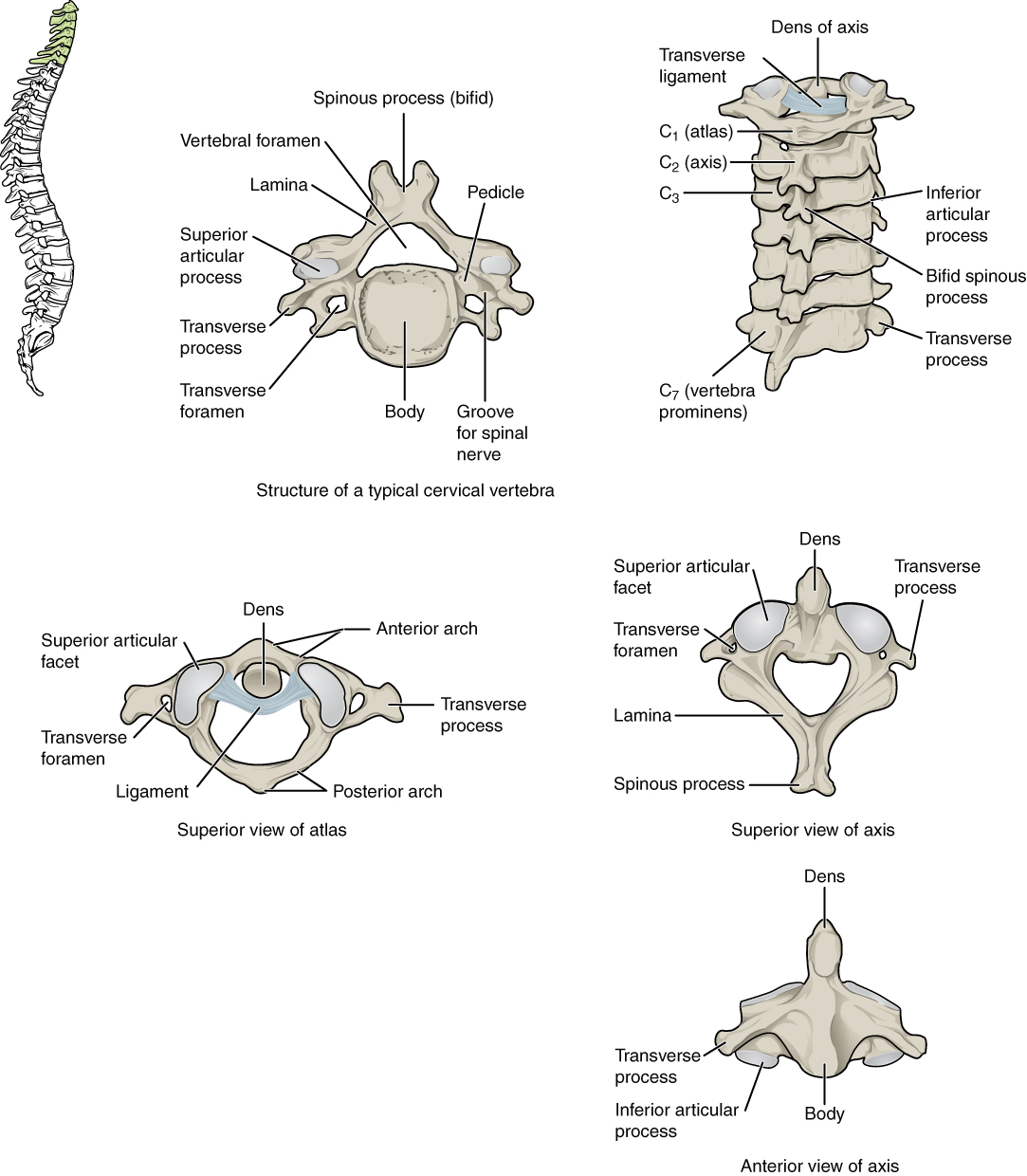
Comparative Anatomy of Typical and Atypical Cervical Vertebrae. This illustration details the specialized features of the cervical spine, including the typical cervical vertebra, the atlas (C1), and the axis (C2). Labeled structures across various views include the spinous process (bifid), vertebral foramen, lamina, pedicle, body, superior and inferior articular processes, transverse process, transverse foramen, and the groove for the spinal nerve. The diagram also highlights unique landmarks, such as the dens (odontoid process), the transverse ligament, the anterior and posterior arches of the atlas, the superior articular facet, and the vertebra prominens (C7).
Contributed by Anatomy & Physiology, Connexions (http://cnx.org/content/col11496/1.6/, Jun 19, 2013)
(Click Image to Enlarge)
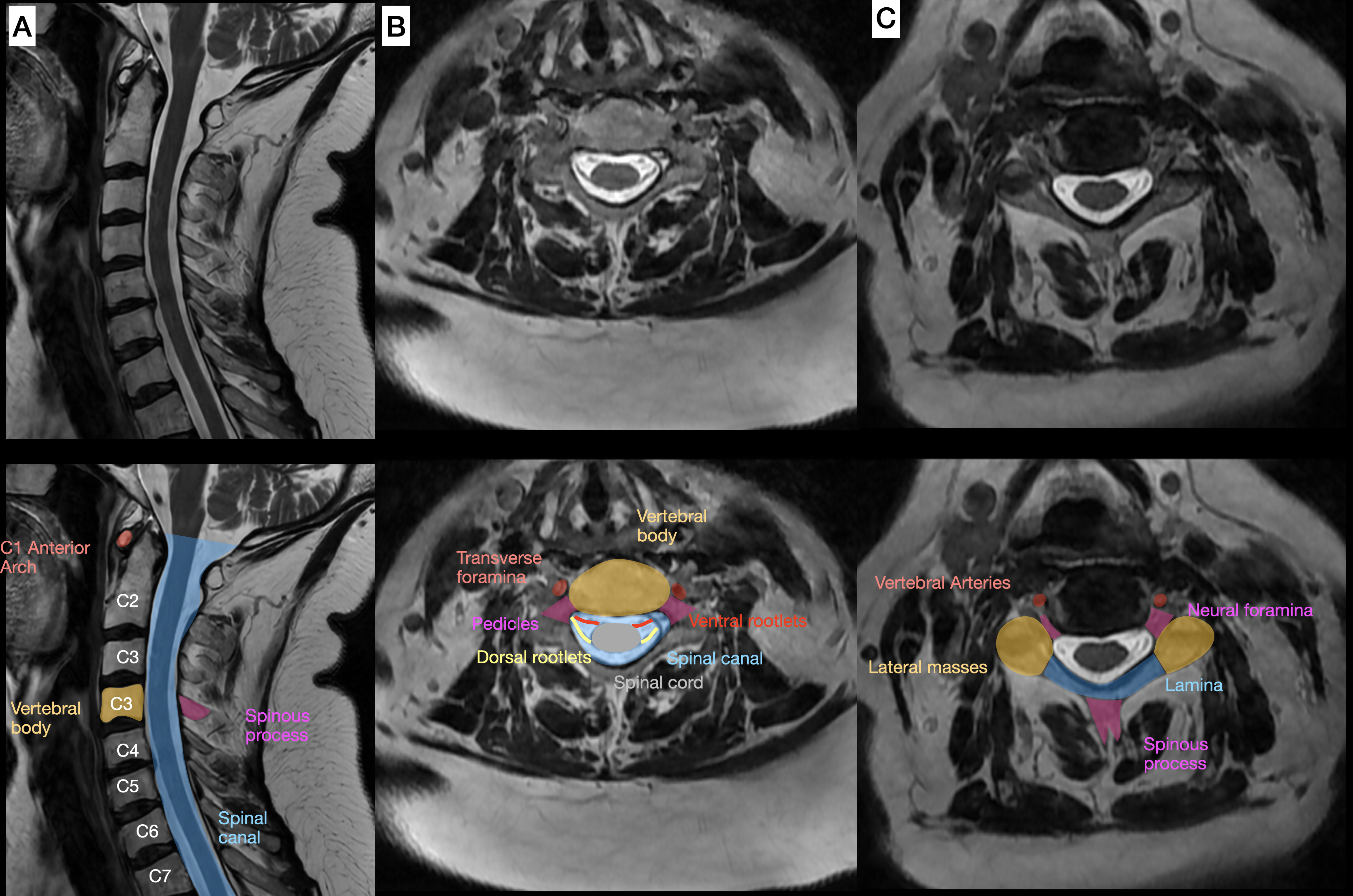
Cervical Spine Magnetic Resonance Imaging in Multiple Views. Midsagittal T2-weighted magnetic resonance imaging (A) displays the cervical spinal cord and vertebral profile. Axial T2-weighted images at midcervical pedicle (B) and foraminal (C) levels reveal cross-sectional anatomy. Annotated lower panels overlay colors on the spinal cord (blue), ventral and dorsal roots (yellow and purple), nerve rootlets (pink), anterior and posterior dura (orange and light blue), and vertebral elements.
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)
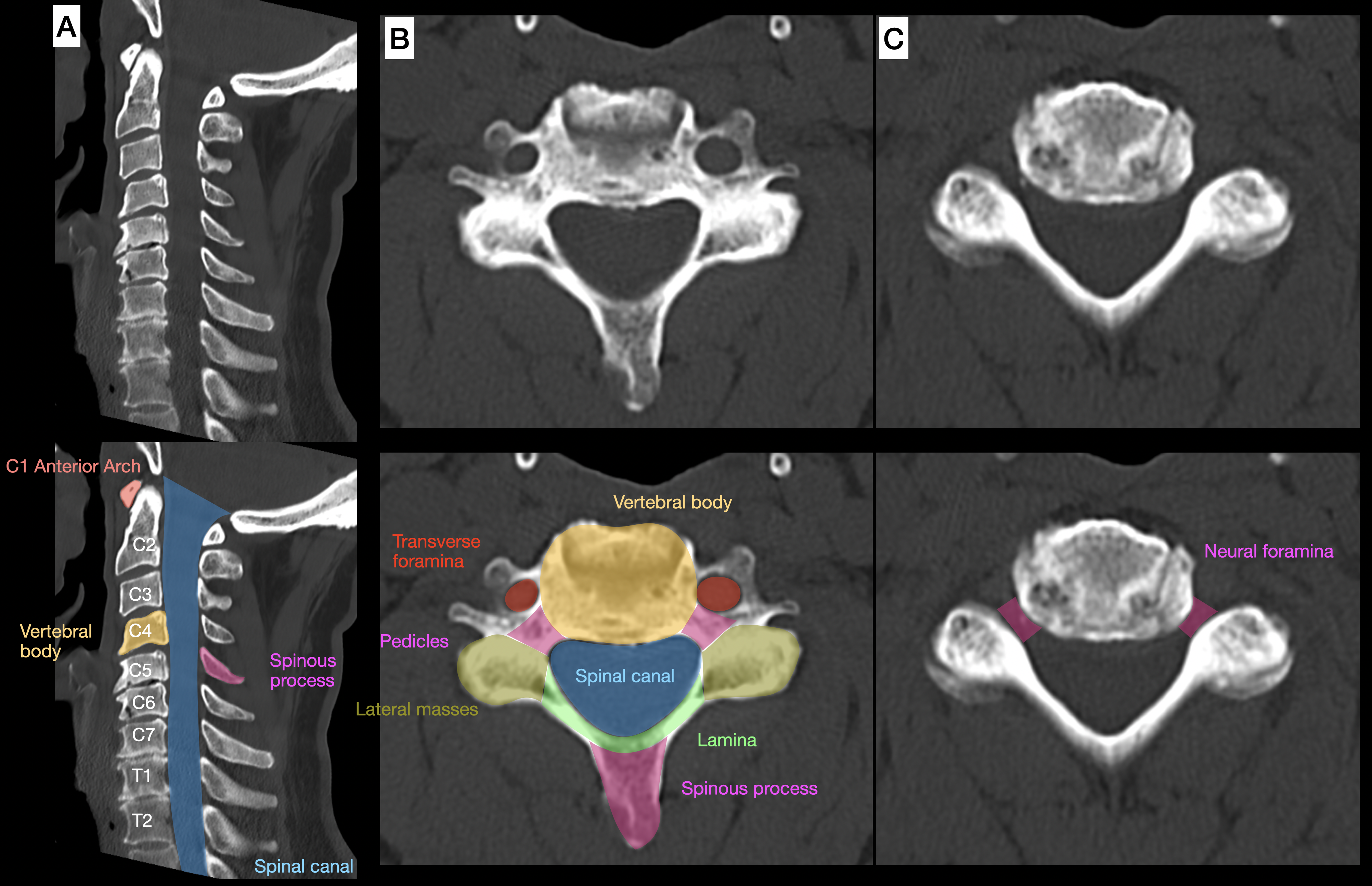
Computed Tomography Anatomy of the Cervical Vertebrae. A sagittal computed tomography (CT) reformat (bone window) shows the cervical vertebral bodies and posterior elements in profile, outlining the osseous boundaries of the spinal canal from C1 to the upper thoracic spine (A). Axial CT images demonstrate typical subaxial cervical vertebral anatomy, including the vertebral body, pedicles, laminae, spinous process, and transverse foramina (B), as well as the neural foramina at the intervertebral level (C). Corresponding lower panels provide color-annotated labeling of key osseous landmarks.
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)
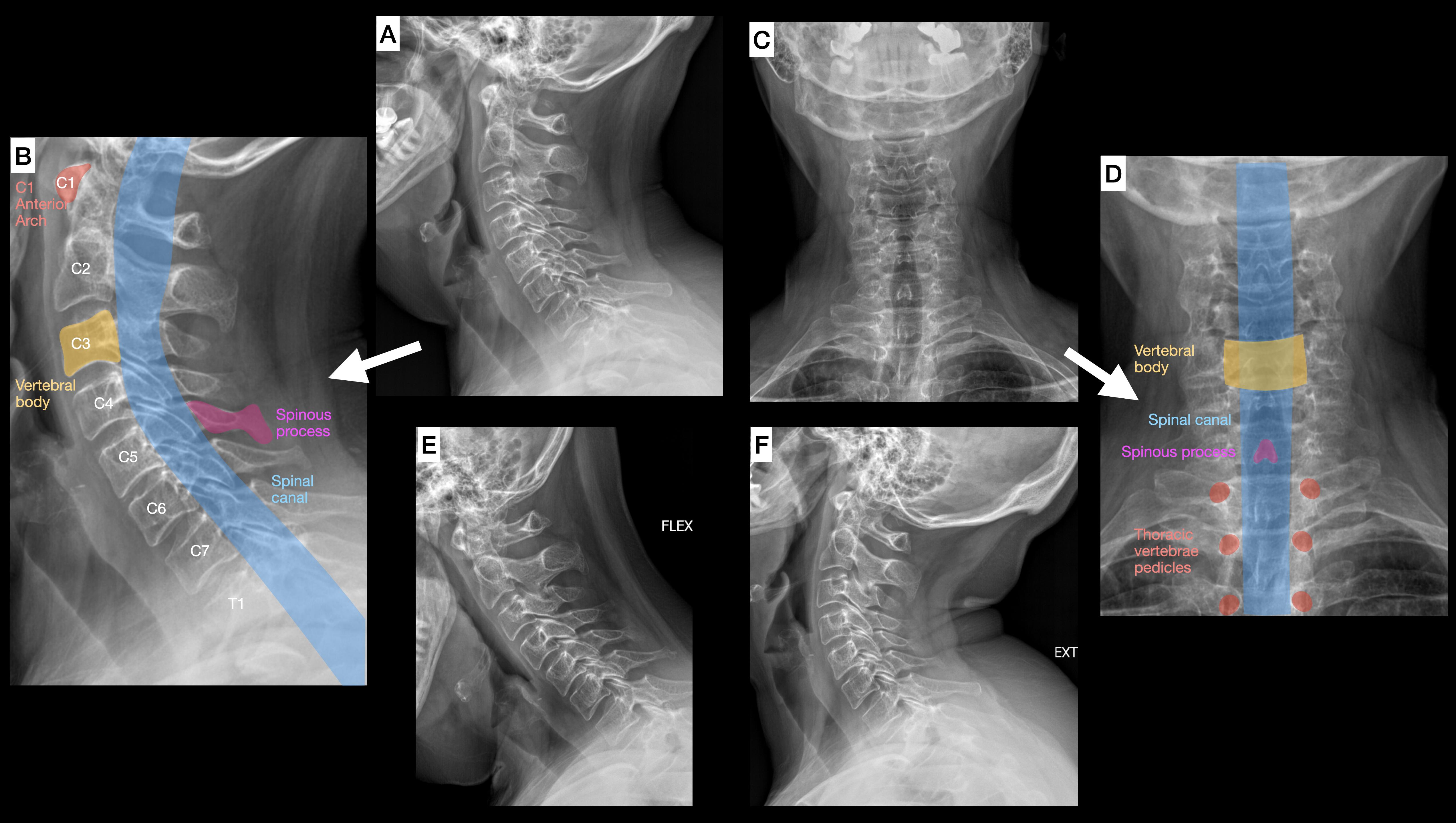
Cervical Spine Radiographic Anatomy and Motion. Neutral lateral cervical spine radiography demonstrates vertebral alignment and intervertebral disc spaces from the upper cervical spine through the cervicothoracic junction (A), with a corresponding annotated view identifying the C1 anterior arch, vertebral bodies, posterior elements, and projected course of the spinal canal (B). Anteroposterior radiography shows midline alignment and lateral osseous contours of the cervical spine (C), with an annotated counterpart highlighting vertebral body level, the projected spinal canal column, posterior midline structures, and inferior thoracic pedicles for orientation (D). Dynamic lateral radiographs acquired in flexion and extension demonstrate segmental cervical motion across multiple levels (E, F).
Contributed by Konstantinos Margetis MD
(Click Image to Enlarge)
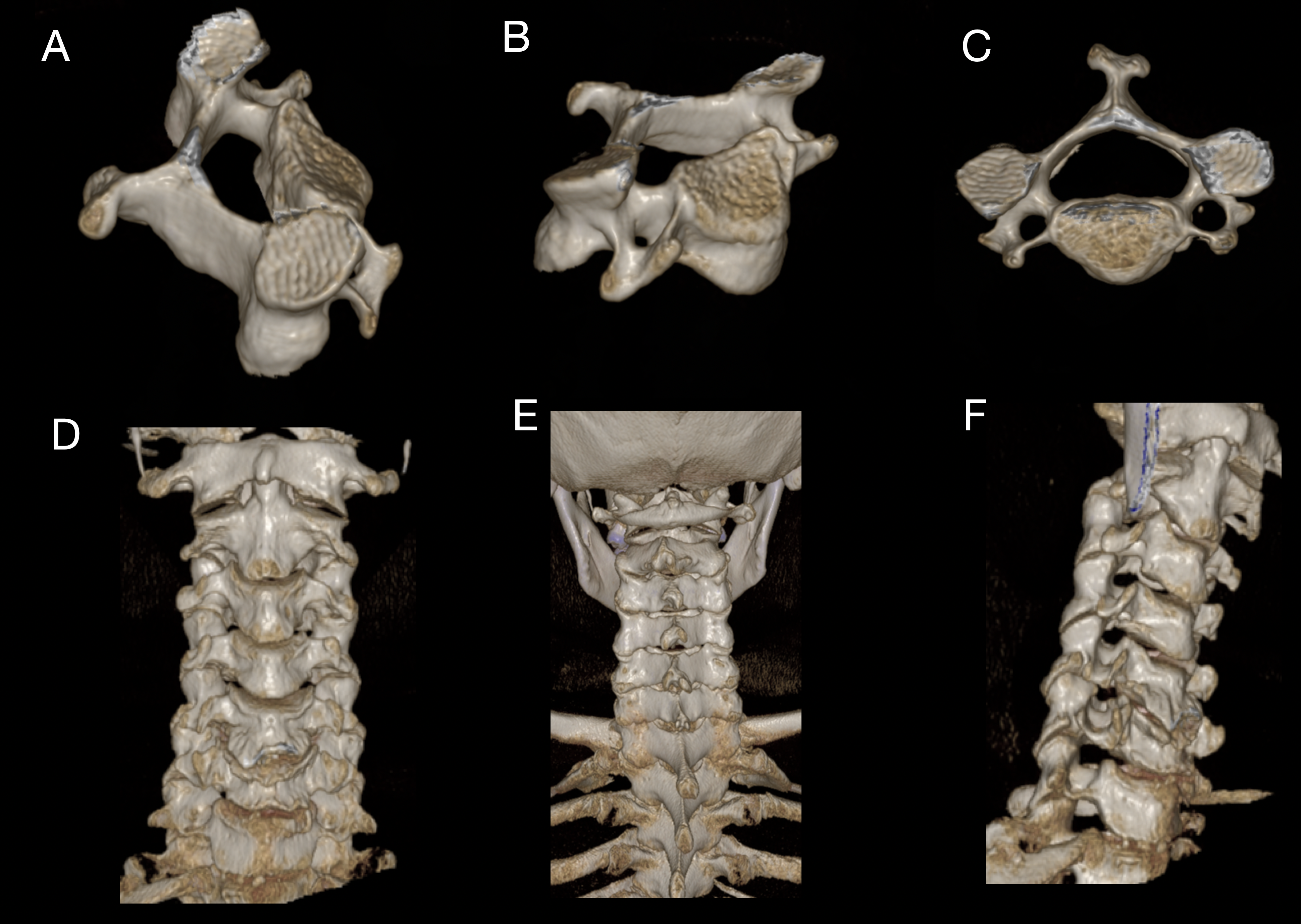
Computed Tomography Anatomy of the Cervical Spine. Oblique volume-rendered 3-dimensional computed tomography (CT) reconstructions depict a typical subaxial cervical vertebra, demonstrating the vertebral body, pedicles, laminae, articular processes, and posterior elements (A, B). A superior view of a typical subaxial cervical vertebra shows the vertebral body, vertebral foramen, posterior arch, and paired transverse foramina (C). Volume-rendered reconstructions of the cervical spine in anterior (D), posterior (E), and anterolateral (F) projections illustrate overall cervical alignment and the spatial relationships among vertebral bodies, facet joints, and posterior elements across multiple cervical levels.
Contributed by Konstantinos Margetis MD
References
Waxenbaum JA, Reddy V, Futterman B. Anatomy, Back, Intervertebral Discs. StatPearls. 2025 Jan:(): [PubMed PMID: 29262063]
Bogduk N. Functional anatomy of the spine. Handbook of clinical neurology. 2016:136():675-88. doi: 10.1016/B978-0-444-53486-6.00032-6. Epub [PubMed PMID: 27430435]
Roche CJ, King SJ, Dangerfield PH, Carty HM. The atlanto-axial joint: physiological range of rotation on MRI and CT. Clinical radiology. 2002 Feb:57(2):103-8 [PubMed PMID: 11977941]
Bogduk N, Mercer S. Biomechanics of the cervical spine. I: Normal kinematics. Clinical biomechanics (Bristol, Avon). 2000 Nov:15(9):633-48 [PubMed PMID: 10946096]
Hartman J. Anatomy and clinical significance of the uncinate process and uncovertebral joint: A comprehensive review. Clinical anatomy (New York, N.Y.). 2014 Apr:27(3):431-40. doi: 10.1002/ca.22317. Epub 2014 Jan 22 [PubMed PMID: 24453021]
Lindenmann S, Tsagkaris C, Farshad M, Widmer J. Kinematics of the Cervical Spine Under Healthy and Degenerative Conditions: A Systematic Review. Annals of biomedical engineering. 2022 Dec:50(12):1705-1733. doi: 10.1007/s10439-022-03088-8. Epub 2022 Dec 10 [PubMed PMID: 36496482]
Level 1 (high-level) evidenceCouto AR, Parreira B, Power DM, Pinheiro L, Madruga Dias J, Novofastovski I, Eshed I, Sarzi-Puttini P, Pappone N, Atzeni F, Verlaan JJ, Kuperus J, Bieber A, Ambrosino P, Kiefer D, Khan MA, Mader R, Baraliakos X, Bruges-Armas J. Evidence for a genetic contribution to the ossification of spinal ligaments in Ossification of Posterior Longitudinal Ligament and Diffuse idiopathic skeletal hyperostosis: A narrative review. Frontiers in genetics. 2022:13():987867. doi: 10.3389/fgene.2022.987867. Epub 2022 Oct 7 [PubMed PMID: 36276944]
Level 3 (low-level) evidenceLee SH, Cho TH, Kwon HJ, Hong JE, Lee YH, Yang HM. An anatomical and radiological study of the tectorial membrane and its clinical implications. Scientific reports. 2022 Dec 12:12(1):21480. doi: 10.1038/s41598-022-25213-2. Epub 2022 Dec 12 [PubMed PMID: 36509799]
Kojima Y, Maeda T, Arai R, Shichikawa K. Nerve supply to the posterior longitudinal ligament and the intervertebral disc of the rat vertebral column as studied by acetylcholinesterase histochemistry. II. Regional differences in the distribution of the nerve fibres and their origins. Journal of anatomy. 1990 Apr:169():247-55 [PubMed PMID: 2384337]
Level 3 (low-level) evidenceHirai T, Yoshii T, Iwanami A, Takeuchi K, Mori K, Yamada T, Wada K, Koda M, Matsuyama Y, Takeshita K, Abematsu M, Haro H, Watanabe M, Watanabe K, Ozawa H, Kanno H, Imagama S, Fujibayashi S, Yamazaki M, Matsumoto M, Nakamura M, Okawa A, Kawaguchi Y. Prevalence and Distribution of Ossified Lesions in the Whole Spine of Patients with Cervical Ossification of the Posterior Longitudinal Ligament A Multicenter Study (JOSL CT study). PloS one. 2016:11(8):e0160117. doi: 10.1371/journal.pone.0160117. Epub 2016 Aug 22 [PubMed PMID: 27548354]
Level 2 (mid-level) evidenceOsmotherly PG, Cowin GJ, Rivett DA. Magnetic resonance imaging anatomy of the craniovertebral ligaments: A radiological study with confirmatory dissection. Journal of craniovertebral junction & spine. 2022 Jul-Sep:13(3):309-317. doi: 10.4103/jcvjs.jcvjs_62_22. Epub 2022 Sep 14 [PubMed PMID: 36263349]
Offiah CE, Day E. The craniocervical junction: embryology, anatomy, biomechanics and imaging in blunt trauma. Insights into imaging. 2017 Feb:8(1):29-47. doi: 10.1007/s13244-016-0530-5. Epub 2016 Nov 4 [PubMed PMID: 27815845]
Ishak B, Dupont G, Lachkar S, Yilmaz E, Glinski AV, Altafulla J, Kikuta S, Iwanaga J, Chapman JR, Oskouian R, Tubbs RS. Update on the Biomechanics of the Craniocervical Junction-Part I: Transverse Atlantal Ligament in the Elderly. Global spine journal. 2021 Mar:11(2):180-186. doi: 10.1177/2192568219896544. Epub 2020 Jan 7 [PubMed PMID: 32875854]
Tominaga Y, Ndu AB, Coe MP, Valenson AJ, Ivancic PC, Ito S, Rubin W, Panjabi MM. Neck ligament strength is decreased following whiplash trauma. BMC musculoskeletal disorders. 2006 Dec 21:7():103 [PubMed PMID: 17184536]
Lambrechts MJ, Brush P, Issa TZ, Toci GR, Heard JC, Syal A, Schilken MM, Canseco JA, Kepler CK, Vaccaro AR. Evaluating the Impact of Modic Changes on Operative Treatment in the Cervical and Lumbar Spine: A Systematic Review and Meta-Analysis. International journal of environmental research and public health. 2022 Aug 16:19(16):. doi: 10.3390/ijerph191610158. Epub 2022 Aug 16 [PubMed PMID: 36011795]
Level 1 (high-level) evidenceDraga M, Scaal M. Building a vertebra: Development of the amniote sclerotome. Journal of morphology. 2024 Jan:285(1):e21665. doi: 10.1002/jmor.21665. Epub [PubMed PMID: 38100740]
Baumgart M, Wiśniewski M, Grzonkowska M, Małkowski B, Badura M, Szpinda M. Morphometric study of the neural ossification centers of the atlas and axis in the human fetus. Surgical and radiologic anatomy : SRA. 2016 Dec:38(10):1205-1215 [PubMed PMID: 27142660]
Karwacki GM, Schneider JF. Normal ossification patterns of atlas and axis: a CT study. AJNR. American journal of neuroradiology. 2012 Nov:33(10):1882-7. doi: 10.3174/ajnr.A3105. Epub 2012 May 10 [PubMed PMID: 22576894]
O'Brien WT Sr, Shen P, Lee P. The Dens: Normal Development, Developmental Variants and Anomalies, and Traumatic Injuries. Journal of clinical imaging science. 2015:5():38. doi: 10.4103/2156-7514.159565. Epub 2015 Jun 30 [PubMed PMID: 26199787]
Dunbar L, Vidakovic H, Löffler S, Hammer N, Gille O, Boissiere L, Obeid I, Pointillart V, Vital JM, Kieser DC. Anterior cervical spine blood supply: a cadaveric study. Surgical and radiologic anatomy : SRA. 2019 Jun:41(6):607-611. doi: 10.1007/s00276-019-02236-5. Epub 2019 Apr 1 [PubMed PMID: 30937565]
Peeters JB, Idriceanu T, El Hage G, Martin T, Salaud C, Champagne PO, Bojanowski MW. A comprehensive review of the vertebral artery anatomy. Neuro-Chirurgie. 2024 May:70(3):101518. doi: 10.1016/j.neuchi.2023.101518. Epub 2024 Jan 29 [PubMed PMID: 38277859]
Tudose RC, Rusu MC, Hostiuc S. The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature. Diagnostics (Basel, Switzerland). 2023 Jun 12:13(12):. doi: 10.3390/diagnostics13122036. Epub 2023 Jun 12 [PubMed PMID: 37370931]
Level 1 (high-level) evidenceCarpenter K, Decater T, Iwanaga J, Maulucci CM, Bui CJ, Dumont AS, Tubbs RS. Revisiting the Vertebral Venous Plexus-A Comprehensive Review of the Literature. World neurosurgery. 2021 Jan:145():381-395. doi: 10.1016/j.wneu.2020.10.004. Epub 2020 Oct 10 [PubMed PMID: 33049379]
Zhang XH, Gong J, Song Y, Hack GD, Jiang SM, Yu SB, Song X, Zhang J, Yang H, Cheng J, Sui HJ, Zheng N. An anatomical study of the suboccipital cavernous sinus and its relationship with the myodural bridge complex. Clinical anatomy (New York, N.Y.). 2023 Jul:36(5):726-736. doi: 10.1002/ca.24048. Epub 2023 Apr 25 [PubMed PMID: 37096831]
Shayota B, Wong TL, Fru D, David G, Iwanaga J, Loukas M, Tubbs RS. A comprehensive review of the sinuvertebral nerve with clinical applications. Anatomy & cell biology. 2019 Jun:52(2):128-133. doi: 10.5115/acb.2019.52.2.128. Epub 2019 Jun 30 [PubMed PMID: 31338228]
Röijezon U, Jull G, Djupsjöbacka M, Salomoni SE, Hodges PW. Deep and superficial cervical muscles respond differently to unstable motor skill tasks. Human movement science. 2021 Dec:80():102893. doi: 10.1016/j.humov.2021.102893. Epub 2021 Nov 9 [PubMed PMID: 34763288]
Kulkarni V, Chandy MJ, Babu KS. Quantitative study of muscle spindles in suboccipital muscles of human foetuses. Neurology India. 2001 Dec:49(4):355-9 [PubMed PMID: 11799407]
Vasavada AN, Li S, Delp SL. Influence of muscle morphometry and moment arms on the moment-generating capacity of human neck muscles. Spine. 1998 Feb 15:23(4):412-22 [PubMed PMID: 9516695]
Cho W, Maeda T, Park Y, Buchowski JM, Nabb CE, Riew D. The incidence of bifid c7 spinous processes. Global spine journal. 2012 Jun:2(2):99-104. doi: 10.1055/s-0032-1319776. Epub [PubMed PMID: 24353954]
Cingoz M, Shehata M, Kandemirli B, Cingoz E. Ossification patterns of the C1 (atlas) and C2 (axis) vertebrae children. Clinical imaging. 2025 Feb:118():110395. doi: 10.1016/j.clinimag.2024.110395. Epub 2024 Dec 24 [PubMed PMID: 39731961]
McAllister AS, Nagaraj U, Radhakrishnan R. Emergent Imaging of Pediatric Cervical Spine Trauma. Radiographics : a review publication of the Radiological Society of North America, Inc. 2019 Jul-Aug:39(4):1126-1142. doi: 10.1148/rg.2019180100. Epub 2019 Jun 7 [PubMed PMID: 31173542]
Elliott RE, Tanweer O. The prevalence of the ponticulus posticus (arcuate foramen) and its importance in the Goel-Harms procedure: meta-analysis and review of the literature. World neurosurgery. 2014 Jul-Aug:82(1-2):e335-43. doi: 10.1016/j.wneu.2013.09.014. Epub 2013 Sep 18 [PubMed PMID: 24055572]
Level 1 (high-level) evidenceÖğüt E, Şekerci R, Şen H, Çakın H, Gediz T, Keles-Celik N. Anatomo-radiological importance and the incidence of os odontoideum in Turkish subjects: a retrospective study. Surgical and radiologic anatomy : SRA. 2020 Jun:42(6):701-710. doi: 10.1007/s00276-020-02421-x. Epub 2020 Jan 27 [PubMed PMID: 31989216]
Level 2 (mid-level) evidenceHenry BM, Vikse J, Sanna B, Taterra D, Gomulska M, Pękala PA, Tubbs RS, Tomaszewski KA. Cervical Rib Prevalence and its Association with Thoracic Outlet Syndrome: A Meta-Analysis of 141 Studies with Surgical Considerations. World neurosurgery. 2018 Feb:110():e965-e978. doi: 10.1016/j.wneu.2017.11.148. Epub 2017 Dec 2 [PubMed PMID: 29203316]
Level 1 (high-level) evidenceBall JR, Shelby T, Mertz K, Mills ES, Ton A, Alluri RK, Hah RJ. The Incidence of Vertebral Artery Injury in Cervical Spine Surgery. World neurosurgery. 2024 Jan:181():e841-e847. doi: 10.1016/j.wneu.2023.10.144. Epub 2023 Nov 4 [PubMed PMID: 37931877]
Bindels BJJ, Dronkers BEG, Smits MLJ, Verlaan JJ. Accurate Placement and Revisions for Cervical Pedicle Screws Placed With or Without Navigation: A Systematic Review and Meta-Analysis. Global spine journal. 2024 Apr:14(3):1018-1037. doi: 10.1177/21925682231196456. Epub 2023 Aug 19 [PubMed PMID: 37596998]
Level 1 (high-level) evidenceShin JJ, Kim KR, Shin J, Kang J, Lee HJ, Kim TW, Hong JT, Kim SW, Ha Y. Surgical Versus Conservative Management for Treating Unstable Atlas Fractures: A Multicenter Study. Neurospine. 2022 Dec:19(4):1013-1025. doi: 10.14245/ns.2244352.176. Epub 2022 Oct 23 [PubMed PMID: 36274194]
Level 2 (mid-level) evidence