Introduction
The gallbladder is a pear-shaped organ situated in the right upper quadrant of the abdomen, measuring approximately 7 to 10 cm in length and 4 cm in width (see Image. Gallbladder and Bile Ducts). This saccular structure lies in a fossa between hepatic segments IV and V and attaches to the visceral surface of the liver by connective tissue. Arterial supply arises primarily from the cystic artery, most often a branch of the right hepatic artery. Venous drainage occurs through small cystic veins into hepatic sinusoids and the gallbladder bed of the liver. The hepatic plexus supplies innervation, with parasympathetic fibers arising from the vagus nerve (cranial nerve X) and sympathetic fibers coming from the celiac plexus. The gallbladder arises from the caudal foregut hepatic diverticulum. Anatomic variants include agenesis and duplication.
The gallbladder is a frequent source of abdominal pathology and one of the most commonly resected organs in surgical practice. Understanding the anatomy and physiology of this organ, as well as its common anatomic variants, is important for accurate diagnosis and safe and effective management of gallbladder and extrahepatic biliary pathology (see Image. Anatomical Variants of the Gallbladder and Biliary Tree).
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The gallbladder is a saccular organ formed by a wall composed of several microscopic tissue layers. The innermost layer is the mucosa, which consists of simple columnar epithelial cells with apical microvilli that absorb water and electrolytes, concentrating bile. Progressing from inner to outer layers, the gallbladder wall comprises a lamina propria, an irregular smooth muscular layer, a perimuscular connective tissue layer, and an outer serosa or adventitia. Unlike most of the gastrointestinal tract, the gallbladder lacks muscularis mucosae and submucosal layers. Rokitansky-Aschoff sinuses are present as deep mucosal invaginations extending into the muscular layer, capable of retaining luminal contents and contributing to chronic wall inflammation.
The gallbladder lies along hepatic segments IV and V. Connective tissue anchors the hepatic surface to the liver. Although lacking a true capsule, portions of the exposed surface are described by some histologists as being covered by the Glisson capsule. The free surface is lined by visceral peritoneum. The gallbladder contains an expansile fundus and body, similar in configuration to the stomach and the uterus. The body narrows through an asymmetric infundibulum (Hartmann pouch) into a neck that connects to the common bile duct (CBD) via a single cystic duct in most cases. Spiral mucosal folds within the cystic duct (valves of Heister) modulate bile flow in response to neurohormonal stimuli. Fundal folding may produce a Phrygian cap configuration, a normal variant that can simulate gallbladder wall thickening on imaging and mimic pathology.[1]
The gallbladder functions as a bile reservoir, storing 30 to 50 mL of bile and facilitating lipid digestion. Bile is produced by hepatocytes and consists of cholesterol, bilirubin, bile salts, phospholipids, water, and electrolytes. Gastric distension and duodenal enteroendocrine cell detection of fatty acids trigger the release of cholecystokinin (CCK). CCK stimulates gallbladder fundus contraction and relaxation of the hepatopancreatic sphincter (sphincter of Oddi), propelling bile from the gallbladder through the valves of Heister and the sphincter of Oddi into the duodenal lumen.[1]
Hypercholesterolemia, hemolytic disorders like sickle cell disease, and biliary infections alter bile composition, often leading to bile crystallization and cholelithiasis. Choleliths range from microlithiasis or biliary sludge resembling sand grains to stones exceeding 3 cm. Gallstones are classified by primary biochemical composition. Cholesterol stones are the most common type. Pigmented stones consist primarily of bilirubin derivatives, often associated with hemolysis in conditions like sickle cell disease.[2]
Embryology
The gallbladder and bile ducts develop from foregut endoderm. By the end of the 4th week of embryogenesis, a bud of tissue that will generate the liver protrudes from the distal ventral wall of the foregut. The cranial portion of this hepatic diverticulum forms the liver and the intrahepatic ducts, while the caudal portion forms the gallbladder and the cystic duct. The narrow connection between the developing hepatic bud and the duodenum becomes the extrahepatic bile duct system.
The pancreas arises from dorsal and ventral pancreatic buds derived from foregut endoderm. Around the 5th week of gestation, elements of the biliary tree become recognizable at a macroscopic level. Around the 6th week of gestation, rotation of the duodenum carries the CBD and the ventral pancreatic bud posteriorly, allowing fusion of the ventral and dorsal pancreatic buds.
The developing gallbladder and biliary ducts undergo canalization, and bile production begins around the 12th week of gestation.[3] The sphincter of Oddi develops during weeks 10 to 28.[4]
Developmental variation occurs among individuals. Biliary system variants include gallbladder agenesis and, less commonly, duplication.[5][6] Most biliary variants involve the intrahepatic or extrahepatic ducts that connect the liver, gallbladder, and duodenum.
Blood Supply and Lymphatics
The gallbladder receives most of its blood supply from the cystic artery. The cystic artery typically arises as a branch of the right hepatic artery, itself originating from the proper hepatic artery. Anatomic variants of these vessels are common, including posteriorly situated cystic arteries and accessory cystic arteries.
The CBD receives a segmental plexiform arterial supply from branches of the right hepatic, gastroduodenal, right gastric, and posterior superior pancreaticoduodenal arteries. Preservation of these small vessels during surgery is essential to maintain perfusion of the cystic duct and CBD. Disruption may predispose to ischemia, bile leak, and subsequent stricture formation. Since the CBD is supplied predominantly by small periductal branches, it is particularly susceptible to thermal injury and devascularization during dissection. The CBD arteries, also termed "paracholedochal arteries," are classically described at the 3 o’clock and 9 o’clock positions and should be avoided during incision of the CBD.[7][8]
No single dominant or formal cystic vein is typically present. Venous drainage usually occurs directly into the gallbladder bed of the liver through short venules extending from the gallbladder into the hepatic parenchyma. Larger venous sinuses draining toward the liver may also be encountered during cholecystectomy and may complicate hemostasis.
Subserosal and submucosal lymphatics drain the gallbladder to the cystic lymph node of Lund, also termed the "node of Calot," located within the hepatocystic triangle, also called the "Calot triangle" (see Surgical Considerations). Gallbladder carcinoma may bypass this lymph node and metastasize directly to lymph nodes at the porta hepatis.[9]
Nerves
The gallbladder and the cystic duct receive innervation from autonomic fibers traveling through the hepatic plexus. Parasympathetic innervation is provided by branches of the vagus nerve, and sympathetic innervation is provided by fibers from the celiac plexus. Visceral pain afferents generally travel with sympathetic fibers, whereas diaphragmatic peritoneal irritation may refer pain to the right shoulder via the right phrenic nerve.
Gastric surgeries, including resections, bariatric procedures, and vagotomies performed for peptic ulcer disease, may result in gallbladder denervation and subsequent organ dysfunction. Gallbladder dysfunction may lead to biliary stasis, cholelithiasis, and cholecystitis. Prophylactic cholecystectomy may be considered concurrently in such cases to reduce the risk of cholecystitis.[10]
Surgical Considerations
Gallbladder dysfunction may require surgical or procedural intervention. Accurate classification of dysfunction guides appropriate management. Laboratory evaluation includes white blood cell count, total and fractionated bilirubin levels, and lipase and amylase levels, aiding differentiation among biliary disease processes. Imaging modalities include ultrasound, hepatobiliary iminodiacetic acid (HIDA) scan with or without CCK, computed tomography (CT), and magnetic resonance cholangiopancreatography (MRCP), used in conjunction with laboratory studies for diagnosis. Therapeutic options include surgical interventions, such as cholecystectomy and bile duct exploration, as well as procedural interventions, such as endoscopic retrograde cholangiopancreatography (ERCP), percutaneous cholecystostomy, and percutaneous transhepatic cholangiography.[11]
Cholecystectomy may be performed using an open, laparoscopic, or robotic approach. Laparoscopic cholecystectomy is a safe and effective alternative to open cholecystectomy, with shorter postoperative recovery.[12] Comparative data between robotic and laparoscopic cholecystectomy are mixed regarding safety, with some studies reporting increased complication rates and others reporting decreased complication rates.[13][14]
Selection among open, laparoscopic, and robotic approaches depends on surgeon proficiency with the chosen technique, anticipated case complexity, and patient tolerance of pneumoperitoneum. Imaging findings, patient condition, and prior surgical history are used to determine potential case difficulty. Operative intervention may not be feasible in select patients, necessitating nonoperative approaches, such as percutaneous cholecystostomy and percutaneous transhepatic biliary drainage or cholangiography.
The hepatocystic triangle, also termed the "triangle of Calot," contains the course of the cystic artery and the cystic lymph node of Lund, also called the "node of Calot." Boundaries of the triangle include the cystic duct on the right, the common hepatic duct on the left, and the undersurface of the liver superiorly (see Image. Calot Triangle). The original 1891 definition of the triangle included the cystic duct, common hepatic duct, and cystic artery as its boundaries. Subsequent modifications improved identification of anatomical landmarks for locating the cystic artery. The gallbladder neck may occasionally be connected to the 1st part of the duodenum by loose fibrous bands known as the peritoneal cholecystoduodenal fold.
The left and right hepatic ducts unite outside the liver to form the common hepatic duct. The cystic duct joins the common hepatic duct after exiting the gallbladder to form the CBD. The CBD travels inferiorly within the hepatoduodenal ligament, with the proper hepatic artery positioned to the left and the portal vein at the posterior aspect. The normal CBD diameter ranges from 4 mm to 7 mm.
CBD dilation may indicate distal obstruction due to an intraluminal stone, benign stricture, or neoplasm of the bile duct, pancreatic head, or ampulla. Accessory bile ducts may drain directly from the liver parenchyma to the gallbladder or course to the gallbladder fossa from extrahepatic bile ducts. These structures are termed "ducts of Luschka."[15] The ducts of Luschka may be injured during cholecystectomy, potentially leading to biloma formation. Intraoperative indocyanine green fluorescence helps delineate biliary anatomy and identify bile leakage.[16]
The paracholedochal arteries usually course at the 3 o’clock and 9 o’clock positions and should be avoided during incision of the CBD. The paracholedochal arteries comprise the primary blood supply of the bile ducts and are prone to thermal injury and stricture formation.
The main pancreatic duct and CBD join to form a common channel known as the hepatopancreatic ampulla, or ampulla of Vater. The hepatopancreatic ampulla is surrounded by smooth muscle forming the hepatopancreatic sphincter, also termed the "sphincter of Oddi." The sphincter of Oddi regulates the flow of bile and pancreatic secretions into the duodenum and prevents reflux of duodenal contents into the bile and pancreatic ducts.
Clinical Significance
The gallbladder may serve as a source of abdominal pain and infection in many patients. Gallstones may lead to symptomatic cholelithiasis, cholecystitis, choledocholithiasis, and ascending cholangitis. Obstruction of the cystic, biliary, and pancreatic ducts, together with biliary stasis, gallbladder contraction, and reflux of bile into the liver or pancreas, contributes to these conditions. Biliary abdominal pain may also occur in the absence of gallstones, including hepatopancreatic sphincter dysfunction and acalculous cholecystitis. Clinical presentation may be acute or chronic.
The gallbladder is distensible and may enlarge to twice its size when the cystic duct is obstructed. Obstruction may result in infection requiring surgical or procedural intervention. Therapeutic options include surgical procedures, such as cholecystectomy and bile duct exploration, and procedural approaches, such as endoscopic retrograde cholangiopancreatography, percutaneous cholecystostomy, and percutaneous transhepatic biliary drainage. These interventions carry inherent risks. Chronic diarrhea is a known complication following cholecystectomy.[17]
Media
(Click Image to Enlarge)
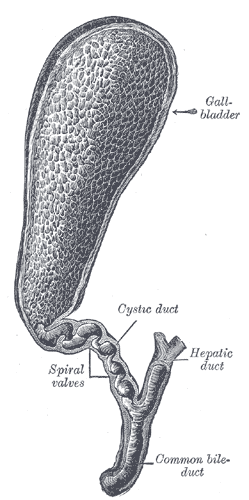
Gallbladder and Bile Ducts. This illustration displays the gallbladder and bile ducts laid open to expose their internal structures. Key labeled features include the hepatic duct, cystic duct, spiral valves, and common bile duct.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
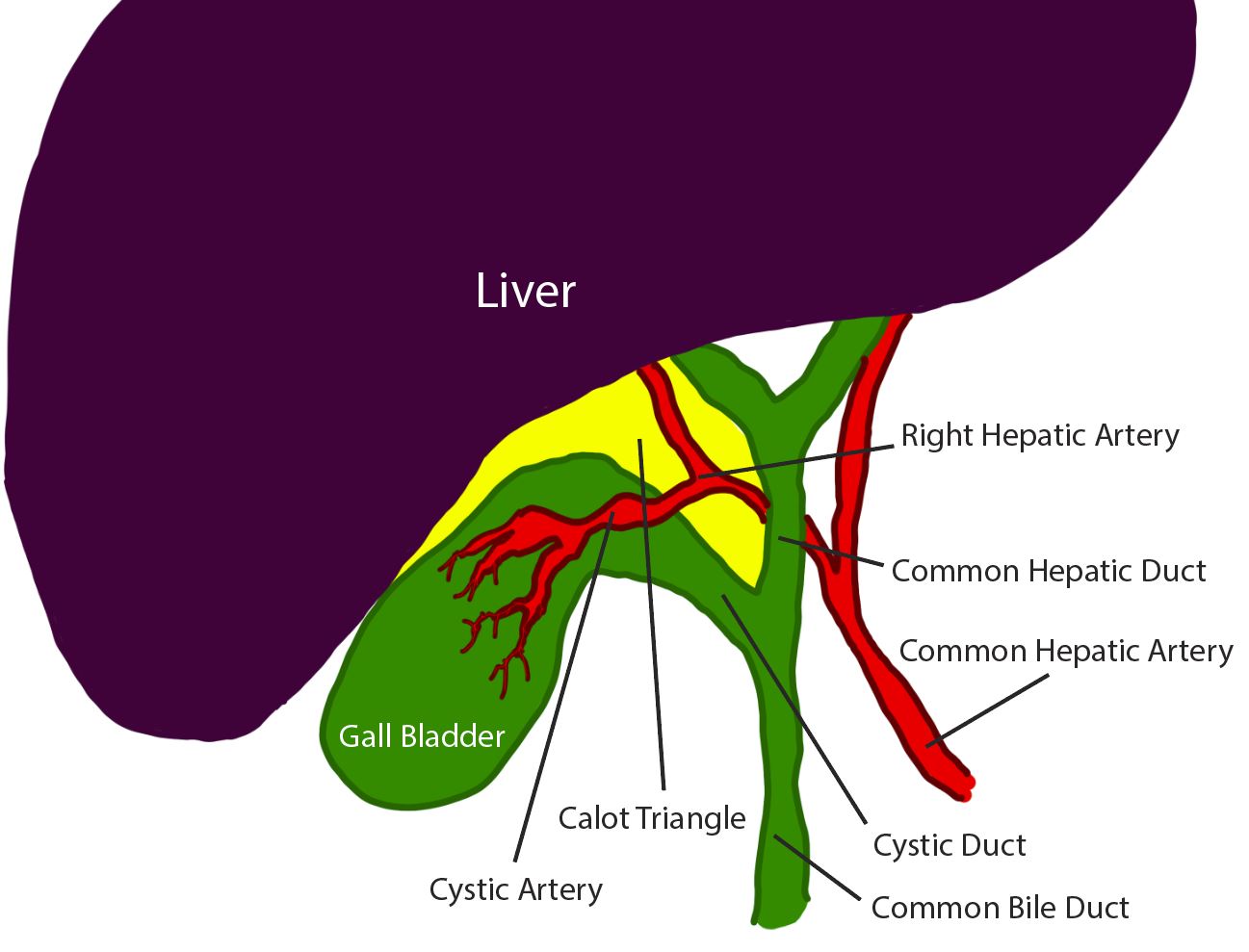
Calot Triangle. This anatomical diagram illustrates the boundaries and contents of the Calot triangle, highlighted in yellow beneath the liver. The labeled structures include the gallbladder, cystic duct, common hepatic duct, common bile duct, common hepatic artery, right hepatic artery, and cystic artery.
Contributed by R Kabir, MD
(Click Image to Enlarge)
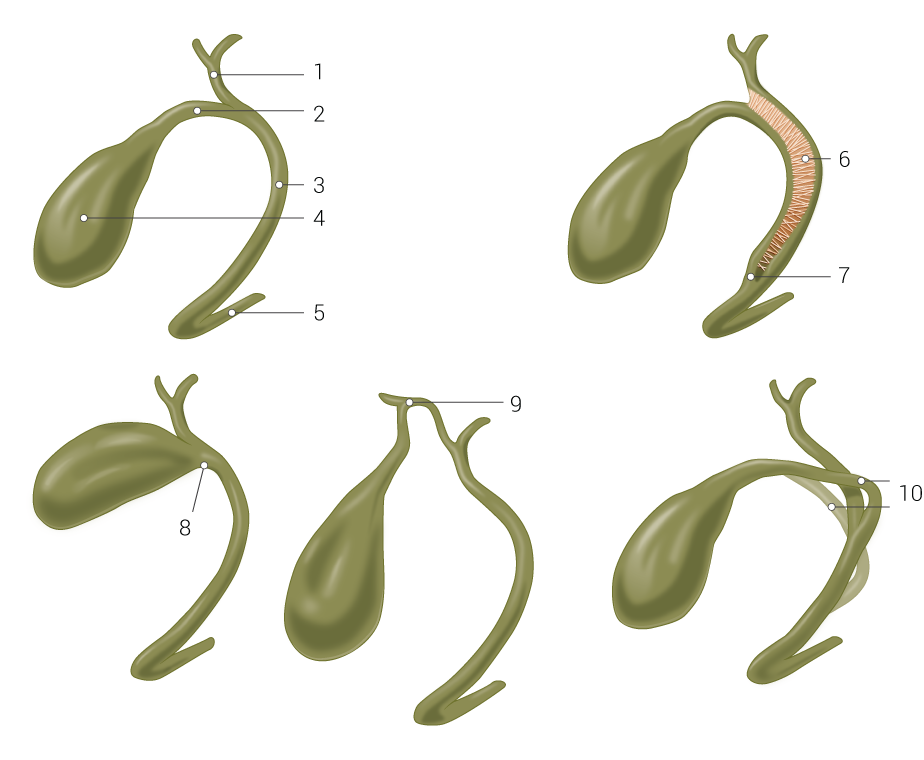
Anatomical Variants of the Gallbladder and Biliary Tree. This illustration highlights the normal anatomy and common structural variants of the cystic duct and gallbladder. The numbered structures demonstrate the common hepatic duct (1), cystic duct (2), common bile duct (3), gallbladder (4), and pancreatic duct (5). The image also outlines anatomical variations, including a fibrous connection (6), low junction (7), absent cystic duct (8), high junction with the right hepatic duct (9), and a cystic duct passing in front of or behind the common bile duct (10).
Illustrated by B Palmer
References
Portincasa P, Di Ciaula A, vanBerge-Henegouwen GP. Smooth muscle function and dysfunction in gallbladder disease. Current gastroenterology reports. 2004 Apr:6(2):151-62 [PubMed PMID: 15191695]
Lammert F, Gurusamy K, Ko CW, Miquel JF, Méndez-Sánchez N, Portincasa P, van Erpecum KJ, van Laarhoven CJ, Wang DQ. Gallstones. Nature reviews. Disease primers. 2016 Apr 28:2():16024. doi: 10.1038/nrdp.2016.24. Epub 2016 Apr 28 [PubMed PMID: 27121416]
Zeng Y, Hu R, Lu J, Qi Y, Chen D, Yang C, Wu J. Prenatal genetic detection in foetus with gallbladder size anomalies: cohort study and systematic review of the literature. Annals of medicine. 2025 Dec:57(1):2440638. doi: 10.1080/07853890.2024.2440638. Epub 2024 Dec 13 [PubMed PMID: 39670967]
Level 1 (high-level) evidenceAndo H. Embryology of the biliary tract. Digestive surgery. 2010:27(2):87-9. doi: 10.1159/000286463. Epub 2010 Jun 10 [PubMed PMID: 20551648]
Neuberg M, Detry O. Gallbladder agenesis. Acta chirurgica Belgica. 2023 Apr:123(2):218-219. doi: 10.1080/00015458.2023.2173836. Epub 2023 Feb 1 [PubMed PMID: 36697393]
Salazar MC, Brownson KE, Nadzam GS, Duffy A, Roberts KE. Gallbladder Agenesis: A Case Report. The Yale journal of biology and medicine. 2018 Sep:91(3):237-241 [PubMed PMID: 30258310]
Level 3 (low-level) evidenceChen WJ, Ying DJ, Liu ZJ, He ZP. Analysis of the arterial supply of the extrahepatic bile ducts and its clinical significance. Clinical anatomy (New York, N.Y.). 1999:12(4):245-9 [PubMed PMID: 10398383]
Iwao Y, Heaton ND. A Review of the Retroportal Artery in the Blood Supply of the Biliary Tree: Implications for Hepato-Pancreato-Biliary and Transplant Surgeons. Liver transplantation : official publication of the American Association for the Study of Liver Diseases and the International Liver Transplantation Society. 2021 Jun 1:27(6):918-922. doi: 10.1002/lt.25965. Epub 2021 Feb 16 [PubMed PMID: 37160000]
Lung K, Lui F. Anatomy, Abdomen and Pelvis: Arteries. StatPearls. 2026 Jan:(): [PubMed PMID: 30247834]
Vernon H, Wehrle CJ, Alia VSK, Kasi A. Anatomy, Abdomen and Pelvis: Liver. StatPearls. 2026 Jan:(): [PubMed PMID: 29763190]
Xiao T, Xu C, Xu H, Feng Y, Su T, Zhang L, Zhao S. Cholangioscopy-guided lithotripsy and extraction of gallbladder stones through the natural lumen. Endoscopy. 2025 Dec:57(S 01):E177-E178. doi: 10.1055/a-2531-9303. Epub 2025 Feb 18 [PubMed PMID: 39965771]
Lujan JA, Parrilla P, Robles R, Marin P, Torralba JA, Garcia-Ayllon J. Laparoscopic cholecystectomy vs open cholecystectomy in the treatment of acute cholecystitis: a prospective study. Archives of surgery (Chicago, Ill. : 1960). 1998 Feb:133(2):173-5 [PubMed PMID: 9484730]
Kalata S, Thumma JR, Norton EC, Dimick JB, Sheetz KH. Comparative Safety of Robotic-Assisted vs Laparoscopic Cholecystectomy. JAMA surgery. 2023 Dec 1:158(12):1303-1310. doi: 10.1001/jamasurg.2023.4389. Epub [PubMed PMID: 37728932]
Level 2 (mid-level) evidenceMaegawa FB, Stetler J, Patel D, Patel S, Serrot FJ, Lin E, Patel AD. Robotic compared with laparoscopic cholecystectomy: A National Surgical Quality Improvement Program comparative analysis. Surgery. 2025 Feb:178():108772. doi: 10.1016/j.surg.2024.08.006. Epub 2024 Sep 13 [PubMed PMID: 39277483]
Level 2 (mid-level) evidenceMcDermott J, Sadeghi N, Telken D, Ahmed I. Duct of Luschka Bile Leak With Formation of Biloma Post-Cholecystectomy: A Case Study. Cureus. 2024 Oct:16(10):e72639. doi: 10.7759/cureus.72639. Epub 2024 Oct 29 [PubMed PMID: 39610573]
Level 3 (low-level) evidenceGijsen AF, de Vries RPH, Vaassen HGM, Geelkerken RH, Liem MSL, Lips DJ. The use of indocyanine green fluorescence imaging in preventing postoperative bile leakage of the hepaticojejunostomy in robot-assisted pancreatic surgery. HPB : the official journal of the International Hepato Pancreato Biliary Association. 2024 Dec:26(12):1515-1520. doi: 10.1016/j.hpb.2024.08.013. Epub 2024 Sep 2 [PubMed PMID: 39277436]
Zou Q, Du J, Lin Y, Xu L. Application of holmium laser in endoscopic retrograde cholangiopancreatographygall gallbladder-preserving cholecystolithotomy. Endoscopy. 2025 Dec:57(S 01):E118-E119. doi: 10.1055/a-2499-7536. Epub 2025 Feb 6 [PubMed PMID: 39914477]