Introduction
Traumatic pneumothorax remains a significant injury in chest trauma, contributing to substantial morbidity and mortality (see Image. Left Pneumothorax on Radiography). The condition represents the 2nd most common injury in chest trauma, accounting for tens of thousands of cases annually in the US. Prompt recognition and treatment in the prehospital setting are critical to prevent progression to respiratory failure or obstructive shock secondary to tension physiology. Most emergency medical service (EMS) systems maintain protocols for rapid assessment and treatment. However, substantial variability persists in specific treatment modalities across levels of training and geographic regions, and no single universally accepted method is implemented nationally.[1][2][3][4] Recent advancements in diagnostic tools and treatment approaches continue to refine prehospital care strategies for this life-threatening condition.[5]
Anatomy and Physiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Anatomy and Physiology
A thorough understanding of the pleural space and surrounding tissues is essential to understand the pathophysiology of traumatic pneumothorax. The pleural space, a potential space between the visceral and parietal pleura, normally facilitates smooth lung movement. Trauma-induced disruption of this space allows accumulation of air, and often blood, resulting in increased intrathoracic pressure. The pressure buildup impinges on surrounding structures, impairing normal blood flow and ventilation.
Three broad classes of traumatic pneumothorax exist. These categories differ in mechanism, pleural pressure dynamics, and degree of hemodynamic impact.
A simple pneumothorax results from injury to the lung or pleura, allowing air to enter the pleural space. Blunt trauma commonly produces this injury, with fractured ribs capable of lacerating the pleura or lung tissue. Accumulated air typically produces minimal effect on adjacent structures unless volume becomes substantial.
Tension pneumothorax is a life-threatening progression of simple pneumothorax, characterized by progressive accumulation of air within the pleural space and formation of a 1-way valve effect. Markedly increased intrathoracic pressure results in collapse of the affected lung, mediastinal shift, and compression of the great vessels and heart. Reduced ventilation, impaired venous return, and decreased cardiac output can rapidly progress to obstructive shock, characterized by tachycardia, hypotension, and eventual cardiac arrest if untreated.
Open or communicating pneumothorax occurs following penetrating chest wall injury that establishes a direct communication between the atmosphere and pleural space. Atmospheric air enters the pleural space during inspiration, disrupting the negative intrathoracic pressure required for effective ventilation. The open defect often permits air egress, limiting significant pressure accumulation compared with tension pneumothorax. However, persistent respiratory compromise remains, with potential progression to tension physiology if the external opening becomes occluded.
Indications
Traumatic pneumothorax should be strongly suspected in any patient with thoracic trauma presenting with signs of respiratory or circulatory compromise. Classic clinical findings include hypoxia, tachypnea, tachycardia, hypotension, chest wall crepitus, diminished or absent breath sounds on the affected side, and a sucking chest wound. Tracheal deviation, while traditionally cited, is a late and unreliable finding and should not be required before initiating treatment. Assessment of these signs occurs during the primary survey. However, EMS providers must recognize that reliance on any single finding, particularly in a dynamic prehospital environment, can delay life-saving intervention.[6][7][8][9][10]
Prehospital intervention should not be delayed when tension pneumothorax is suspected based on the clinical presentation. Needle thoracostomy remains the standard prehospital decompression technique and is indicated in the presence of significant thoracic trauma with absent or diminished breath sounds accompanied by hemodynamic instability or severe respiratory distress. Finger thoracostomy is an emerging advanced skill incorporated into select EMS protocols, particularly when traumatic arrest has occurred or needle thoracostomy has failed, and may provide more reliable decompression in selected settings. Vented or valved occlusive chest seals are the preferred intervention for open pneumothorax. Vigilance is required during application of any occlusive dressing, as sealing an open wound without venting can convert a communicating pneumothorax into tension physiology, necessitating immediate readiness for needle decompression.
A sucking chest wound warrants occlusive dressing placement regardless of initial respiratory status, given the risk of rapid deterioration. In patients with suspected simple pneumothorax who remain stable hemodynamically and show no respiratory compromise, consideration should be given to balancing on-scene intervention against expedited transport to a definitive care facility.
Contraindications
No absolute contraindications have been identified for needle thoracostomy, finger thoracostomy, or application of occlusive dressings in the management of tension pneumothorax or communicating pneumothorax in individuals demonstrating hemodynamic instability. Patient-specific factors, including chronic anticoagulation, and the overall clinical context, warrant consideration. However, emergent life-saving interventions should not be delayed. Given the high morbidity and mortality associated with these injuries, immediate treatment remains paramount in patients with cardiorespiratory compromise.
Equipment
The optimal equipment for needle thoracostomy is a subject of ongoing debate. Traditional angiocatheters remain in use, while commercial devices specifically designed for chest decompression are also available. Success rates for needle thoracostomy are a key concern, particularly in the context of increasing patient body mass index. Evidence increasingly supports the use of longer and larger-bore needles, such as 8 cm, 14-gauge catheters, to reliably access the pleural space, particularly given the variability in chest wall thickness.[11] EMS providers must maintain familiarity with system-available equipment and its appropriate use.
Historically, 3-sided occlusive dressings were the standard intervention for communicating pneumothorax. Concerns regarding placement time, difficulty achieving an adequate seal with tape, and risk of converting an open pneumothorax into a tension pneumothorax have driven the development of commercial vented chest seals. These devices incorporate 1-way valves, suction ports, or engineered channels to permit air egress while preventing air ingress. Large-scale randomized controlled trials comparing specific devices are currently limited. However, comparative studies and systematic reviews suggest vented seals are more effective and easier to apply than traditional improvised dressings and may reduce the risk of tension pneumothorax development.[12] Selection between commercial vented seals and traditional methods generally reflects balancing cost, ease of application, and demonstrated efficacy within a given EMS system.
Personnel
Both procedures fall within the scope of practice of prehospital providers with appropriate equipment. Finger thoracostomy typically requires advanced training and is generally performed by physicians or critical care paramedics in the prehospital setting. Familiarity with these protocols and techniques remains essential. Most prehospital systems maintain protocols defining provider eligibility and procedural indications.
Advancing technology supports the adaptation of in-hospital diagnostic approaches to the prehospital setting to improve diagnostic accuracy and reduce time to diagnosis. Ultrasound has been repeatedly demonstrated in emergency department literature to provide rapid and effective diagnosis of pneumothorax and is now incorporated into the standard evaluation of the traumatically injured patient (see Image. Normal Lung Ultrasound). Previously large and cumbersome systems have evolved into portable and accessible devices with potential application in prehospital care. Ultrasound probes now interface with portable electronic devices, enabling mobile field assessment. With continued development, ultrasound may become a standard component of prehospital care, though further research is required to define the impact on patient outcomes.
Preparation
Needle thoracostomy and occlusive dressing application fall within the scope of practice for most prehospital providers, contingent on appropriate training and established protocols. Familiarity with these protocols and techniques remains essential.
Technological advancements have facilitated the adaptation of in-hospital diagnostic approaches to the prehospital setting. Point-of-care ultrasound (POCUS) is rapidly emerging as a vital tool for prehospital providers. [13] Although further research is required to establish effects on patient outcomes definitively, POCUS demonstrates significant potential to improve diagnostic accuracy and reduce time to definitive treatment in the prehospital environment.
Technique or Treatment
Needle decompression involves the insertion of a large-bore catheter through the chest wall into the pleural space to release entrapped air. Anatomical landmarks are identified by palpation and visualization, with needle placement just superior to the rib to avoid the neurovascular bundle. Although an audible release of air may indicate successful placement, improvement in vital signs, including heart rate, blood pressure, and oxygen saturation, is the most reliable indicator of effective decompression.
The optimal anatomical site for needle thoracostomy remains under active investigation. The 2nd intercostal space in the midclavicular line was traditionally taught. However, studies increasingly demonstrate high failure rates at this site due to variable chest wall thickness and insufficient needle length.[14] Current recommendations, supported by military and civilian data, favor a lateral approach at the 4th or 5th intercostal space in the midaxillary line (see Image. Emergency Needle Decompression Sites).[15][16] Reduced soft tissue depth at this location increases the likelihood of pleural space penetration with standard needle lengths. A potential limitation of the lateral approach includes the risk of catheter kinking or occlusion, particularly during patient movement or prolonged transport in the supine position, as observed in military transport settings. Ongoing assessment of catheter patency remains necessary.
Finger thoracostomy, also referred to as "simple thoracostomy," may be performed in patients with confirmed or highly suspected tension pneumothorax, particularly when needle decompression is unsuccessful, or a more definitive prehospital intervention is indicated. The procedure involves the creation of a small incision through the skin and intercostal muscles, followed by blunt dissection through the chest wall into the pleural space and insertion of a gloved finger to confirm pleural entry and achieve immediate decompression. The approach is similar to chest tube insertion and is typically performed at the 4th or 5th intercostal space in the midaxillary line.
Finger thoracostomy provides a more definitive intervention and demonstrates lower rates of failure and recurrence of tension physiology compared with needle decompression, due to the formation of a larger and more stable opening. However, the procedure is more invasive, requires advanced training and sterile technique, and is generally restricted to advanced prehospital providers under specific protocols. The primary objective is rapid and complete decompression, serving as a bridge to formal chest tube insertion in the hospital. Performance of this procedure requires appropriate training, equipment, and protocol authorization.
For sucking chest wounds, the intervention aims to create a 1-way valve over the defect. Traditionally, an occlusive dressing is applied and secured on 3 sides, leaving the dependent side open to permit egress of air and blood. Commercial vented chest seals achieve this effect more efficiently by adhering over the wound and allowing drainage through integrated 1-way valves. In military prehospital care, current practice trends favor the use of a 4-sided occlusive dressing, effectively creating a complete seal, combined with prompt needle decompression if tension pneumothorax develops.[17]
Complications
Needle thoracostomy is an invasive procedure with potential complications, including injury to intercostal vessels, lung parenchyma, and cardiac structures, which may result in significant morbidity and mortality. Therefore, administration of this procedure should be limited to appropriate clinical indications. Infection at the insertion site has been reported, although its occurrence is rare. Needle thoracostomy functions as a temporizing measure. Definitive management typically requires tube thoracostomy upon hospital arrival. Some prehospital systems, including those in the UK, have explored prehospital chest tube placement. However, such practice generally results in increased on-scene times with similar success rates compared with needle decompression, supporting needle decompression as the preferred rapid intervention.
Although less common than failure of needle decompression, the complications of finger thoracostomy when performed incorrectly include bleeding, infection, and injury to underlying structures. Finger thoracostomy provides more reliable decompression when appropriately indicated and performed by trained personnel.
Complications associated with occlusive dressings primarily arise from failure to function as an effective 1-way valve. Common examples include loss of adherence, resulting in persistent communicating pneumothorax, or complete wound occlusion, which may convert a closed pneumothorax to tension physiology. Concurrent hemothorax often interferes with dressing adherence and may obstruct 1-way valves with blood clots. Localized allergic reactions to adhesive materials are rare but have been reported.
Clinical Significance
Rapid assessment and timely intervention for traumatic pneumothorax in the prehospital setting are critical for the reversal of life-threatening respiratory and hemodynamic compromise. Guided by established protocols and emerging technologies, EMS providers can significantly influence patient outcomes. Continued evolution of techniques, coupled with integration of in-hospital diagnostic tools such as POCUS, is expected to further enhance prehospital management of this critical injury.[18][19][20]
Enhancing Healthcare Team Outcomes
Comprehensive management of pneumothorax requires an interprofessional team, including emergency department physicians, trauma surgeons, general surgeons, thoracic surgeons, and critical care specialists. Nursing personnel play a vital role in monitoring chest tube patency, providing wound care, and tracking vital signs closely. Prompt and effective prehospital management, followed by seamless handover to the hospital team, is associated with improved patient outcomes. Patient education regarding risk factors, including smoking cessation, is important to prevent future spontaneous pneumothoraces (see Image. Pulmonary Bulla on Computed Tomography).
Media
(Click Image to Enlarge)
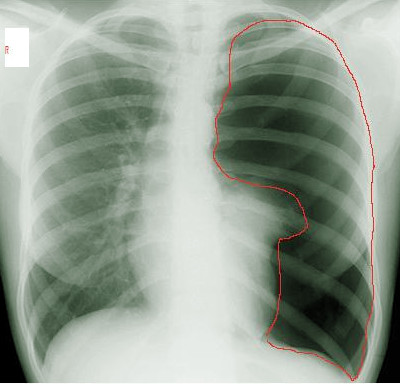
Left Pneumothorax on Radiography. This chest x-ray shows the disappearance of lung markings in the left pleural cavity (area marked with a red line), indicating the presence of a pneumothorax. The collapsed lung is partially obscured by the heart.
Contributed by Steve Bhimji, MS, MD, PhD
(Click Image to Enlarge)
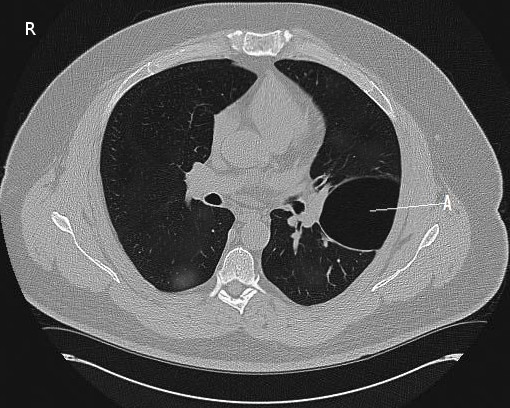
Pulmonary Bulla on Computed Tomography. This axial image reveals a gas-containing cystic structure on the left lung formed by dilated airspaces (A). The presence of this pulmonary bulla is often associated with conditions like pneumothorax.
Contributed by Steve Bhimji, MS, MD, PhD
(Click Image to Enlarge)
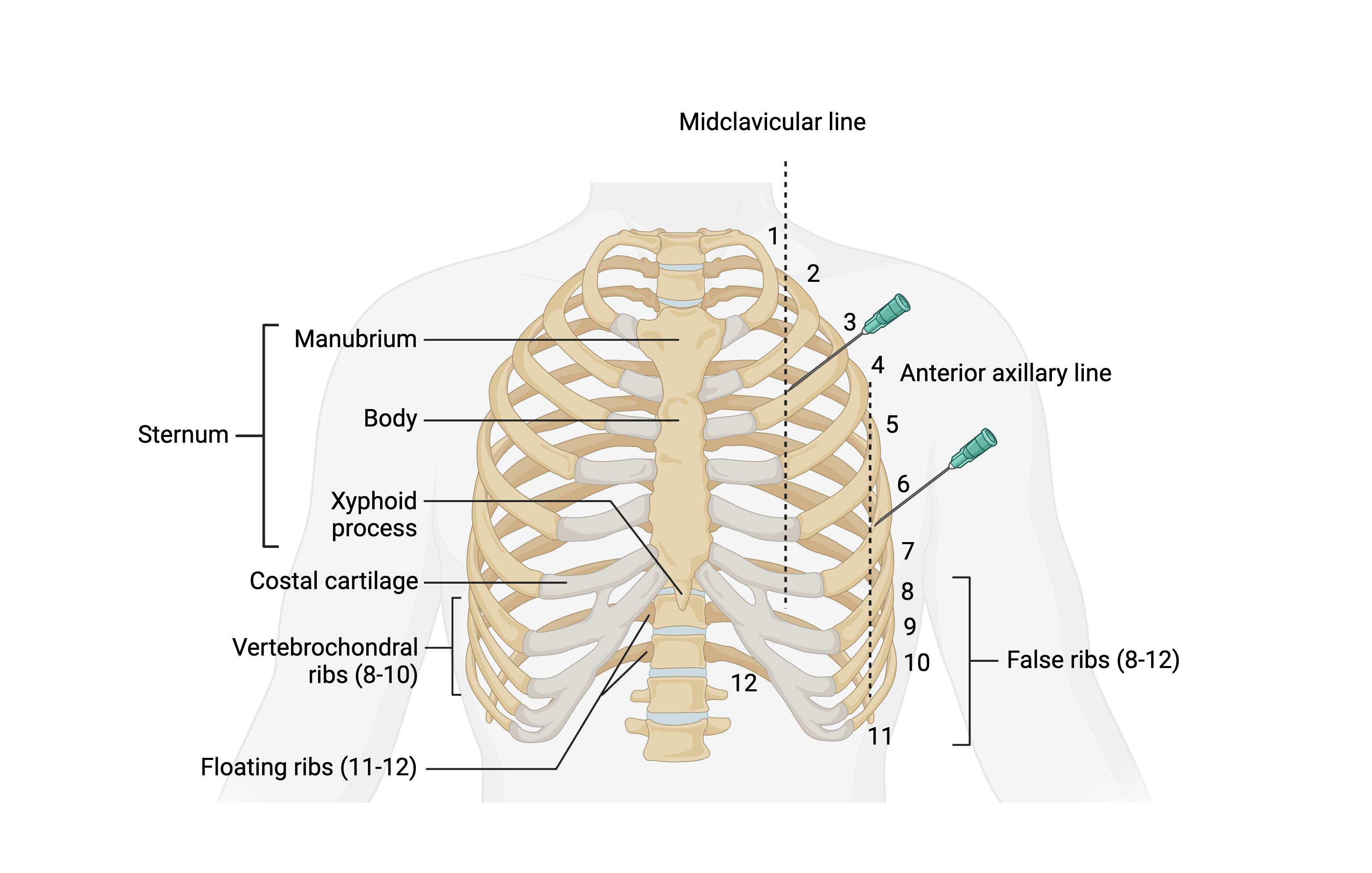
Emergency Needle Decompression Sites. This illustration shows the recommended sites for inserting a 14-gauge needle in tension pneumothorax cases. These sites include the 2nd intercostal space at the midclavicular line, positioned just superior to the 3rd rib, and the 5th intercostal space at the anterior axillary line, positioned just superior to the 6th rib.
Created in BioRender. Bohlen, J. (2025) https://BioRender.com/d53u966
(Click Video to Play)
Normal Lung Ultrasound. This video shows a normal lung ultrasound with lung sliding. The hyperechoic pleura is seen moving along the chest wall between 2 rib shadows. This indicates normal functioning and the absence of a pneumothorax.
Contributed by Evan Kuhl, MD
References
Talbott MM, Campos A, Kuhl EA, Martel TJ. EMS Pneumothorax Identification Without Ancillary Testing. StatPearls. 2026 Jan:(): [PubMed PMID: 30422463]
Dickson RL, Gleisberg G, Aiken M, Crocker K, Patrick C, Nichols T, Mason C, Fioretti J. Emergency Medical Services Simple Thoracostomy for Traumatic Cardiac Arrest: Postimplementation Experience in a Ground-based Suburban/Rural Emergency Medical Services Agency. The Journal of emergency medicine. 2018 Sep:55(3):366-371. doi: 10.1016/j.jemermed.2018.05.027. Epub 2018 Jun 28 [PubMed PMID: 29958708]
Weichenthal LA, Owen S, Stroh G, Ramos J. Needle Thoracostomy: Does Changing Needle Length and Location Change Patient Outcome? Prehospital and disaster medicine. 2018 Jun:33(3):237-244. doi: 10.1017/S1049023X18000316. Epub 2018 Apr 19 [PubMed PMID: 29669611]
Gurung I, Ghassemzadeh S. Spontaneous Pneumothorax. StatPearls. 2026 Jan:(): [PubMed PMID: 29083723]
Gómez-Restrepo C, Rodríguez MN, Eslava-Schmalbach J, Ruiz R, Gil JF. Self-recognition of mental disorders and mental problems in the adult population from the Colombian National Mental Health Survey. Revista Colombiana de psiquiatria. 2021 Apr-Jun:50(2):92-100. doi: 10.1016/j.rcp.2019.09.004. Epub 2020 Jun 6 [PubMed PMID: 33734994]
Level 3 (low-level) evidenceWeichenthal L, Crane D, Rond L. Needle Thoracostomy in the Prehospital Setting: A Retrospective Observational Study. Prehospital emergency care. 2016 May-Jun:20(3):399-403. doi: 10.3109/10903127.2015.1102992. Epub 2016 Jan 25 [PubMed PMID: 26807605]
Level 2 (mid-level) evidenceBhat SR, Johnson DA, Pierog JE, Zaia BE, Williams SR, Gharahbaghian L. Prehospital Evaluation of Effusion, Pneumothorax, and Standstill (PEEPS): Point-of-care Ultrasound in Emergency Medical Services. The western journal of emergency medicine. 2015 Jul:16(4):503-9. doi: 10.5811/westjem.2015.5.25414. Epub 2015 Jul 14 [PubMed PMID: 26265961]
Weichenthal L, Crane DH, Rond L, Roche C. Needle Thoracostomy for Patients with Prolonged Transport Times: A Case-control Study. Prehospital and disaster medicine. 2015 Aug:30(4):397-401. doi: 10.1017/S1049023X15004902. Epub 2015 Jul 8 [PubMed PMID: 26152549]
Level 2 (mid-level) evidenceKnotts D, Arthur AO, Holder P, Herrington T, Thomas SH. Pneumothorax volume expansion in helicopter emergency medical services transport. Air medical journal. 2013 May-Jun:32(3):138-43. doi: 10.1016/j.amj.2012.10.014. Epub [PubMed PMID: 23632222]
Chin EJ, Chan CH, Mortazavi R, Anderson CL, Kahn CA, Summers S, Fox JC. A pilot study examining the viability of a Prehospital Assessment with UltraSound for Emergencies (PAUSE) protocol. The Journal of emergency medicine. 2013 Jan:44(1):142-9. doi: 10.1016/j.jemermed.2012.02.032. Epub 2012 May 16 [PubMed PMID: 22595631]
Level 3 (low-level) evidenceHannick JH, Blais AS, Kim JK, Traubici J, Shiff M, Book R, Lorenzo AJ. Prevalence, Doppler Ultrasound Findings, and Clinical Implications of the Nutcracker Phenomenon in Pediatric Varicoceles. Urology. 2019 Jun:128():78-83. doi: 10.1016/j.urology.2019.03.001. Epub 2019 Mar 16 [PubMed PMID: 30885542]
Lyng JW, Ward C, Angelidis M, Breyre A, Donaldson R, Inaba K, Mandt MJ, Bosson N. Prehospital Trauma Compendium: Traumatic Pneumothorax Care: Position Statement and Resource Document of NAEMSP. Prehospital emergency care. 2024 Dec 4:():1-21. doi: 10.1080/10903127.2024.2416978. Epub 2024 Dec 4 [PubMed PMID: 39499620]
Verhees V, de Kok LGC. Heart Point in Pneumothorax: A Case Report and Comparison to Mimicking Signs. Case reports in critical care. 2025:2025():8134006. doi: 10.1155/crcc/8134006. Epub 2025 Nov 19 [PubMed PMID: 41268042]
Level 3 (low-level) evidenceAho JM, Thiels CA, El Khatib MM, Ubl DS, Laan DV, Berns KS, Habermann EB, Zietlow SP, Zielinski MD. Needle thoracostomy: Clinical effectiveness is improved using a longer angiocatheter. The journal of trauma and acute care surgery. 2016 Feb:80(2):272-7. doi: 10.1097/TA.0000000000000889. Epub [PubMed PMID: 26670108]
Ahmad SJS, Degiannis JR, Head M, Ahmed AR, Gelber E, Hakky S, Kieser A, Müller M, Darling J, Jakob DA, Kyriazidis IP, Degiannis K, Dorn P, Lala A, Bowman C, Wilkinson D, Whiteley G, Hassan U, Mohamed Y, Loo KH, Davies YD, Egan R, Pouwels S, Coulthard A, Churchill L, Bhavra K, Bailey C, Johnson I, Rees I, Williams D, Hajibandeh S, Yang W, Subbe CP, Owen A, Rawaf D, Khamise A, Khalid AW, Parmar C, Soler JA, Khalil M, Mohajer-Bastami A, Moin S, Archid R, Abdulmajed M, Jones R, Balasubaramaniam V, Al-Salihi R, Shoker A, Hwang MJ, Griffiths O, Pandey S, Lee-Smith L, Exadaktylos AK. Meta-analysis of the optimal needle length and decompression site for tension pneumothorax and consensus recommendations on current ATLS and ETC guidelines. World journal of emergency surgery : WJES. 2025 May 19:20(1):39. doi: 10.1186/s13017-025-00613-7. Epub 2025 May 19 [PubMed PMID: 40383767]
Level 1 (high-level) evidenceLaan DV, Vu TD, Thiels CA, Pandian TK, Schiller HJ, Murad MH, Aho JM. Chest wall thickness and decompression failure: A systematic review and meta-analysis comparing anatomic locations in needle thoracostomy. Injury. 2016 Apr:47(4):797-804. doi: 10.1016/j.injury.2015.11.045. Epub 2015 Dec 13 [PubMed PMID: 26724173]
Level 1 (high-level) evidenceMontgomery HR, Drew B, Torrisi J, Adams MG, Remley MA, Rich TA, Greydanus DJ, Shaw TA. TCCC Guidelines Comprehensive Review and Edits 2020: TCCC Guidelines Change 20-05 01 November 2020. Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2021 Summer:21(2):122-127. doi: 10.55460/SU0P-ZNLN. Epub [PubMed PMID: 34105138]
Deaton TG, Drew B, Montgomery HR, Butler FK Jr. Tactical Combat Casualty Care (TCCC) Guidelines: 25 January 2024. Journal of special operations medicine : a peer reviewed journal for SOF medical professionals. 2024 Mar 1:24(1):100-108. doi: 10.55460/QT3B-XK5B. Epub [PubMed PMID: 38364091]
Marie I, Bliss J, Partyka C. Anatomical mapping of traumatic pneumothoraces missed by prehospital ultrasonography - a retrospective cohort study. Injury. 2026 Jan:57(1):112778. doi: 10.1016/j.injury.2025.112778. Epub 2025 Sep 30 [PubMed PMID: 41067963]
Level 2 (mid-level) evidenceGarramone RR Jr, Jacobs LM, Sahdev P. An objective method to measure and manage occult pneumothorax. Surgery, gynecology & obstetrics. 1991 Oct:173(4):257-61 [PubMed PMID: 1925893]
Level 2 (mid-level) evidence