 Hyperbaric Treatment of Central Retinal Artery Occlusion
Hyperbaric Treatment of Central Retinal Artery Occlusion
Introduction
Central retinal artery occlusion (CRAO) is a relatively rare emergency and a potentially devastating eye condition. Patients present with sudden, painless monocular vision loss. The prognosis for visual recovery is poor, and no treatments are supported by prospective randomized controlled trials (RCTs). However, retrospective analyses support potential visual benefit from hyperbaric oxygen therapy (HBOT). HBOT was approved in 2006 for the treatment of CRAO without evidence from RCTs. No other interventions were recommended at the time for this condition, which is associated with poor visual outcomes. The retina has the highest oxygen consumption rate of any organ in the body at 13 mL/100 g/min, and retinal tissue demonstrates marked intolerance to hypoxia. HBOT increases oxygen delivery to hypoxic retinal tissue before irreversible cellular loss occurs.
Etiology
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Etiology
Blockage of the central retinal artery may be related to thromboembolic disease, vasospasm, and vasculitis. Risk factors for this ischemic event overlap with those for ischemic cerebrovascular accident and systemic vasculopathy, including hypertension, diabetes mellitus, hyperlipidemia, cardiovascular disease, ipsilateral carotid artery atherosclerosis, arrhythmia, smoking, obesity, older age, male sex, and coagulopathy. CRAO is classified into arteritic and nonarteritic causes. Giant cell arteritis is a potentially fatal vasculitic cause.
Epidemiology
CRAO occurs more frequently in men, with an incidence of approximately 1 in 50,000 to 100,000 and a mean age of 60 to 65 years.[1] CRAO due to arteritis is most commonly caused by giant cell arteritis, though systemic lupus erythematosus and other vasculitides, such as polyarteritis nodosa, may also cause CRAO. Most CRAOs are nonarteritic, with approximately 90% classified as such. Carotid artery disease is the most common cause of retinal artery occlusion, accounting for approximately 70% of cases.[2] Additional nonarteritic causes include cardioembolism from atrial fibrillation, thrombotic disorders associated with hypercoagulable states and hematologic malignancies, and vaso-occlusive disease, such as sickle cell disease.
CRAO is a rare emergent ocular condition and should be suspected in any patient with unilateral, sudden, painless vision loss, often limited to counting fingers or light perception. The absence of light perception suggests ophthalmic artery occlusion, which causes permanent and severe vision loss. HBOT is not appropriate in this setting due to the absence of ciliary collateral circulation required for retinal viability, though thrombolysis may be considered.
Pathophysiology
The central retinal artery is the 1st branch of the ophthalmic artery, itself a branch of the internal carotid artery. The central retinal artery perfuses the inner retinal layers via superior and inferior branches. Approximately 15% to 30% of the population also possesses a cilioretinal artery, a branch of the short posterior ciliary artery. The cilioretinal artery perfuses the fovea and preserves central visual acuity when spared. The classic cherry red spot fundus appearance develops due to edema of the ischemic inner retina, which obscures choroidal circulation. The foveola lacks inner retinal layers, allowing continued visualization of choroidal circulation as a cherry red spot surrounded by retinal edema and opacification. Inner retinal layer atrophy follows edema resolution and is associated with poor visual outcomes.
The retina has a dual blood supply, with the choroid supplying the outer retinal layers. The theory underlying HBOT is that increased fraction of inspired oxygen (FiO2) enhances oxygen diffusion from choroidal circulation to the ischemic inner retina. Increased FiO2 requires initiation prior to irreversible cellular loss and maintenance until retinal vessel recanalization. Recanalization typically occurs within 72 hours.
The most extensive published case series (Hayreh) demonstrated the natural progression of the disease without HBOT. Transient symptoms lasting minutes to hours were observed in some patients, with spontaneous resolution and minimal residual visual impairment. A variant retinal vascular supply, the cilioretinal artery, is present in nearly 50% of the population and approximately 1 in 3 eyes, with substantial variability in retinal territory perfusion.[3] Cilioretinal arteries may preserve central retinal function in selected cases. Outcomes in patients without cilioretinal arteries remain poor without HBOT, with less than 2% recovering baseline vision and approximately 80% limited to light perception, motion detection, or finger counting.[4] Patients with cilioretinal arteries demonstrate significantly more favorable outcomes.
History and Physical
CRAO presents as sudden-onset, painless vision loss. Visual acuity is often worse than 20/200, with presentation typically limited to light perception, hand motion detection, or finger counting. Absence of light perception suggests ophthalmic artery occlusion, with absence of perfusion to choroidal vessels. Preserved central visual acuity with fundoscopy consistent with CRAO suggests a cilioretinal artery blood supply. Fundoscopic findings may demonstrate a pale yellow ischemic retina. A cherry-red spot may be present at the macula but is an inconsistent and unreliable finding. The cherry-red spot is associated with poor outcomes (see Image. Central Retinal Artery Occlusion).[5]
Evaluation
CRAO represents a "stroke of the eye" and requires the same urgency as an evolving stroke or myocardial infarction. Oxygen administration by nonrebreather mask should be initiated immediately during the evaluation. Fundoscopy should be performed and documented without delay. Ophthalmology consultation, preferably with a vitreoretinal specialist, should be obtained promptly. Ocular pain, a history of trauma, flashers or floaters, and age younger than 40 years are more commonly associated with ocular trauma, retinal detachment, or vitreous hemorrhage and make CRAO less likely.
Treatment / Management
General Treatment
Immediate management includes administration of supplemental oxygen at the highest available normobaric FiO2. Ophthalmology consultation should be obtained without delaying treatment when HBOT is readily available. Baseline laboratory evaluation includes complete blood count, erythrocyte sedimentation rate, C-reactive protein, prothrombin time, partial thromboplastin time, and international normalized ratio in patients receiving warfarin. Electrocardiography should also be performed. Carotid ultrasound, magnetic resonance imaging, and echocardiography may be performed later as part of a comprehensive evaluation for vascular risk factor modification, similar to stroke assessment. Symptom onset within 24 hours of presentation and lack of response to normobaric hyperoxia after 15 minutes warrant emergency hyperbaric medicine consultation.[6](B3)
Hyperbaric Oxygen Treatment Protocol
HBOT in CRAO is initiated with compression to 2 atmospheres absolute (ATA). Significant visual improvement at 2 ATA warrants treatment at that depth for 90 minutes. Absence of visual improvement after 30 minutes at 2 ATA necessitates compression to 2.4 ATA, followed by treatment at that depth for 90 minutes if vision improves. Failure to improve at 2.4 ATA warrants compression to 2.8 ATA and administration of the US Navy Treatment Table No. 6
Lack of improvement after the initial US Navy Treatment Table No. 6 is an indication for treatment discontinuation, use of normobaric oxygen therapy, or 2 additional treatments at 2.8 ATA for 90 minutes with 5-minute air breaks every 30 minutes twice daily, followed by reassessment after 4 to 6 days. Most patients reach a treatment plateau beyond which further improvement in visual acuity does not occur, at which point treatment may be discontinued. Some patients require up to 8 treatments before visual acuity improves, although response beyond that point is uncommon.[7]
A simpler protocol associated with favorable outcomes consists of treatment at 2.5 ATA for 90 minutes with 5-minute air breaks every 30 minutes twice daily for 2 to 3 weeks.[8] Fluorescein angiography provides a safe and valuable method for assessing successful central retinal artery recanalization.[9]
Differential Diagnosis
The differential diagnosis for acute painless vision loss includes central retinal vein occlusion, vitreous hemorrhage, retinal detachment, posterior circulation stroke, ischemic optic neuropathy, and amaurosis fugax. Overlapping clinical features necessitate exclusion of these conditions during the initial evaluation.
Pertinent Studies and Ongoing Trials
An unfavorable meta-analysis published in 2002 failed to demonstrate significant improvement in CRAO outcomes with HBOT despite treatment initiation within 12 hours of symptom onset in most patients.[10] Another equivocal study compared outcomes between 2 hospitals, one using HBOT and the other not. Although HBOT was associated with better outcomes, clinical significance was minimal, and no significant difference was observed in the proportion of patients achieving visual acuity better than 20/200.[11] HBOT has also been explored for central retinal vein occlusion, although published evidence is limited to case reports and small case series. Case reports describing favorable outcomes despite delayed treatment initiation are encouraging.[12] [Source: Assaf-Harofeh Medical Center. Hyperbaric Chamber for Central Retinal Vein Occlusion (CRVO) Patients. 2015]
Prognosis
HBOT initiated within 8 hours of symptom onset is associated with an 83% likelihood of improving visual acuity by at least 3 Snellen lines.[13] A case series of 39 patients with CRAO reported visual improvement in 72% of patients, with a mean gain of 5 lines on a modified Snellen chart.
Complications
Neovascularization may develop after CRAO, particularly in patients with diabetes mellitus. Neovascularization may result in progressive visual loss, neovascular glaucoma, and vitreous hemorrhage despite initial visual salvage with HBOT.[14] The effects of HBOT on this process are unknown.[15] HBOT is generally well tolerated, although confinement anxiety and otic barotrauma may occur. Other complications are uncommon.
Deterrence and Patient Education
Immediate presentation for medical evaluation is essential, as CRAO is a highly time-sensitive condition. Visual salvage depends on rapid initiation of HBOT and, in selected patients, thrombolytic therapy. Patients at increased risk should be advised to seek immediate emergency department evaluation for sudden vision loss.
Pearls and Other Issues
Important concepts regarding HBOT implementation for CRAO are as follows:
- CRAO should be managed as a stroke of the eye, with hospital admission for close monitoring, diagnostic evaluation, and vascular risk factor modification.[16]
- Supplemental oxygen remains a cornerstone of CRAO management.
- Retinal blood flow may be restored within 72 hours through spontaneous recanalization.
- Vision may not recover despite recanalization if ischemia and hypoxia have caused irreversible cell death and necrosis of the inner retinal layers.
- The ischemic penumbra is retinal tissue capable of recovery within a limited therapeutic window.
- Acute CRAO frequently results in severe, permanent vision loss despite prompt treatment.[17]
- HBOT for CRAO carries a Level IIB recommendation from the Undersea and Hyperbaric Medical Society according to the American Heart Association classification.[18] HBOT remains one of the few therapeutic options available for this potentially devastating condition.
- Recovery or improvement in visual acuity during initial HBOT for CRAO indicates retinal viability and potential for visual recovery despite preceding ischemia.
- A primate study demonstrated no retinal damage when retinal ischemia was reversed within 90 minutes. Retinal damage developed shortly thereafter, with irreversible injury occurring after 240 minutes.[19]
- Animal models demonstrated reduced retinal cell loss from 58% to 30% following HBOT after experimental CRAO.[20]
- Recent investigations have evaluated thrombolytic therapy and surgical clot removal. Although promising, clinical outcomes are disappointing.[21][22][23]
Characteristic fundoscopic findings in the setting of acute painless monocular vision loss strongly support the diagnosis of CRAO. Optimal control of vascular risk factors remains the cornerstone of prevention for this ocular condition.
Enhancing Healthcare Team Outcomes
CRAO requires coordinated management by an interprofessional team that includes emergency department triage nurses, emergency medicine physicians, ophthalmologists, neurologists, and hyperbaric medicine specialists. Recognition of CRAO as a medical emergency is essential, as observational studies suggest HBOT may improve visual outcomes despite the absence of RCTs. Prompt triage and rapid transfer to a hyperbaric facility are critical to maximize the likelihood of visual recovery. Immediate fundoscopic examination with documentation should be performed, followed by ophthalmology consultation, preferably with a vitreoretinal specialist. Stroke team evaluation is also recommended. Patients presenting within 6 to 8 hours of symptom onset experience the greatest benefit from HBOT.[24][25]
Media
(Click Image to Enlarge)
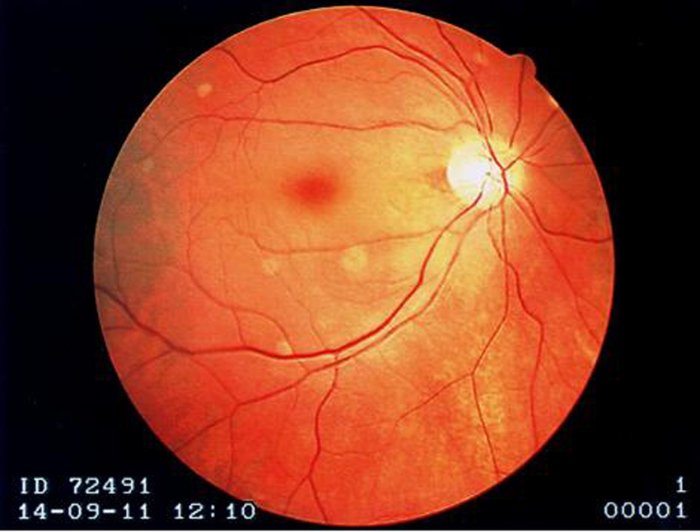
Central Retinal Artery Occlusion. Fundoscopic examination demonstrates a cherry-red fovea, optic disc pallor, and boxcar segmentation of the retinal veins.
Contributed by EJ Kaufman, OD, FAAO
References
Rumelt S, Dorenboim Y, Rehany U. Aggressive systematic treatment for central retinal artery occlusion. American journal of ophthalmology. 1999 Dec:128(6):733-8 [PubMed PMID: 10612510]
Level 1 (high-level) evidenceBabikian V, Wijman CA, Koleini B, Malik SN, Goyal N, Matjucha IC. Retinal ischemia and embolism. Etiologies and outcomes based on a prospective study. Cerebrovascular diseases (Basel, Switzerland). 2001 Aug:12(2):108-13 [PubMed PMID: 11490104]
Justice J Jr, Lehmann RP. Cilioretinal arteries. A study based on review of stereo fundus photographs and fluorescein angiographic findings. Archives of ophthalmology (Chicago, Ill. : 1960). 1976 Aug:94(8):1355-8 [PubMed PMID: 949278]
Hayreh SS, Zimmerman MB. Central retinal artery occlusion: visual outcome. American journal of ophthalmology. 2005 Sep:140(3):376-91 [PubMed PMID: 16138997]
Hadanny A, Maliar A, Fishlev G, Bechor Y, Bergan J, Friedman M, Avni I, Efrati S. Reversibility of retinal ischemia due to central retinal artery occlusion by hyperbaric oxygen. Clinical ophthalmology (Auckland, N.Z.). 2017:11():115-125. doi: 10.2147/OPTH.S121307. Epub 2016 Dec 29 [PubMed PMID: 28096655]
Celebi ARC. Hyperbaric Oxygen Therapy for Central Retinal Artery Occlusion: Patient Selection and Perspectives. Clinical ophthalmology (Auckland, N.Z.). 2021:15():3443-3457. doi: 10.2147/OPTH.S224192. Epub 2021 Aug 13 [PubMed PMID: 34413628]
Level 3 (low-level) evidenceMurphy-Lavoie H, Butler FK, Hagan C. Arterial insufficiencies: Central retinal artery occlusion. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2022 Fourth Quarter:49(4):533-547. doi: 10.22462/07.08.2022.12. Epub [PubMed PMID: 36446298]
Di Vincenzo H, Kauert A, Martiano D, Chiabo J, Di Vincenzo D, Sozonoff I, Baillif S, Martel A. Efficacy and safety of a standardized hyperbaric oxygen therapy protocol for retinal artery occlusion. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2022 Fourth Quarter:49(4):495-505. doi: 10.22462/07.08.2022.9. Epub [PubMed PMID: 36446295]
Chiabo J, Kauert A, Casolla B, Contenti J, Nahon-Esteve S, Baillif S, Arnaud M. Efficacy and safety of hyperbaric oxygen therapy monitored by fluorescein angiography in patients with retinal artery occlusion. The British journal of ophthalmology. 2024 Jun 20:108(7):956-962. doi: 10.1136/bjo-2023-323972. Epub 2024 Jun 20 [PubMed PMID: 37722767]
Rosignoli L, Chu ER, Carter JE, Johnson DA, Sohn JH, Bahadorani S. The Effects of Hyperbaric Oxygen Therapy in Patients with Central Retinal Artery Occlusion: A Retrospective Study, Systematic Review, and Meta-analysis. Korean journal of ophthalmology : KJO. 2022 Apr:36(2):108-113. doi: 10.3341/kjo.2021.0130. Epub 2021 Nov 8 [PubMed PMID: 34743490]
Level 1 (high-level) evidenceMasters TC, Westgard BC, Hendriksen SM, Decanini A, Abel AS, Logue CJ, Walter JW, Linduska J, Engel KC. CASE SERIES OF HYPERBARIC OXYGEN THERAPY FOR CENTRAL RETINAL ARTERY OCCLUSION. Retinal cases & brief reports. 2021 Nov 1:15(6):783-788. doi: 10.1097/ICB.0000000000000895. Epub [PubMed PMID: 31306292]
Level 2 (mid-level) evidenceJohnson DR, Cooper JS. Retinal Artery and Vein Occlusions Successfully Treated with Hyperbaric Oxygen. Clinical practice and cases in emergency medicine. 2019 Nov:3(4):338-340. doi: 10.5811/cpcem.2019.7.43017. Epub 2019 Sep 25 [PubMed PMID: 31763582]
Level 3 (low-level) evidenceBeiran I, Goldenberg I, Adir Y, Tamir A, Shupak A, Miller B. Early hyperbaric oxygen therapy for retinal artery occlusion. European journal of ophthalmology. 2001 Oct-Dec:11(4):345-50 [PubMed PMID: 11820305]
Tang PH, Engel K, Parke DW 3rd. Early Onset of Ocular Neovascularization After Hyperbaric Oxygen Therapy in a Patient With Central Retinal Artery Occlusion. Ophthalmology and therapy. 2016 Dec:5(2):263-269 [PubMed PMID: 27613631]
John Blegen HM 4th, Reed DS, Giles GB, Wedel ML, Hobbs SD. Long-Term Outcomes After Central Retinal Artery Occlusion Treated Acutely With Hyperbaric Oxygen Therapy: A Case Series. Journal of vitreoretinal diseases. 2021 Mar-Apr:5(2):142-146. doi: 10.1177/2474126420951989. Epub 2020 Sep 17 [PubMed PMID: 37009086]
Level 2 (mid-level) evidenceLee KE, Tschoe C, Coffman SA, Kittel C, Brown PA, Vu Q, Fargen KM, Hayes BH, Wolfe SQ. Management of Acute Central Retinal Artery Occlusion, a "Retinal Stroke": An Institutional Series and Literature Review. Journal of stroke and cerebrovascular diseases : the official journal of National Stroke Association. 2021 Feb:30(2):105531. doi: 10.1016/j.jstrokecerebrovasdis.2020.105531. Epub 2020 Dec 10 [PubMed PMID: 33310593]
Kim SH, Cha YS, Lee Y, Kim H, Yoon IN. Successful treatment of central retinal artery occlusion using hyperbaric oxygen therapy. Clinical and experimental emergency medicine. 2018 Dec:5(4):278-281. doi: 10.15441/ceem.17.271. Epub 2018 Dec 31 [PubMed PMID: 30571907]
Murphy-Lavoie H, Butler F, Hagan C. Central retinal artery occlusion treated with oxygen: a literature review and treatment algorithm. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2012 Sep-Oct:39(5):943-53 [PubMed PMID: 23045923]
Hayreh SS, Kolder HE, Weingeist TA. Central retinal artery occlusion and retinal tolerance time. Ophthalmology. 1980 Jan:87(1):75-8 [PubMed PMID: 6769079]
Gaydar V, Ezrachi D, Dratviman-Storobinsky O, Hofstetter S, Avraham-Lubin BC, Goldenberg-Cohen N. Reduction of apoptosis in ischemic retinas of two mouse models using hyperbaric oxygen treatment. Investigative ophthalmology & visual science. 2011 Sep 29:52(10):7514-22. doi: 10.1167/iovs.11-7574. Epub 2011 Sep 29 [PubMed PMID: 21873680]
Raber FP, Gmeiner FV, Dreyhaupt J, Wolf A, Ludolph AC, Werner JU, Kassubek J, Althaus K. Thrombolysis in central retinal artery occlusion: a retrospective observational study. Journal of neurology. 2023 Feb:270(2):891-897. doi: 10.1007/s00415-022-11439-7. Epub 2022 Oct 28 [PubMed PMID: 36305969]
Level 2 (mid-level) evidenceFerreira D, Soares C, Tavares-Ferreira J, Fernandes T, Araújo R, Castro P. Acute phase treatment in central retinal artery occlusion: thrombolysis, hyperbaric oxygen therapy or both? Journal of thrombosis and thrombolysis. 2020 Nov:50(4):984-988. doi: 10.1007/s11239-020-02072-0. Epub [PubMed PMID: 32166539]
Huang L, Wang Y, Zhang R. Intravenous thrombolysis in patients with central retinal artery occlusion: a systematic review and meta-analysis. Journal of neurology. 2022 Apr:269(4):1825-1833. doi: 10.1007/s00415-021-10838-6. Epub 2021 Oct 9 [PubMed PMID: 34625849]
Level 1 (high-level) evidenceWu X, Chen S, Li S, Zhang J, Luan D, Zhao S, Chu Z, Xu Y. Oxygen therapy in patients with retinal artery occlusion: A meta-analysis. PloS one. 2018:13(8):e0202154. doi: 10.1371/journal.pone.0202154. Epub 2018 Aug 29 [PubMed PMID: 30157206]
Level 1 (high-level) evidenceSt Peter D, Na D, Sethuraman K, Mathews MK, Li AS. Hyperbaric oxygen therapy for central retinal artery occlusion: Visual acuity and time to treatment. Undersea & hyperbaric medicine : journal of the Undersea and Hyperbaric Medical Society, Inc. 2023 Third Quarter:50(3):253-264 [PubMed PMID: 37708058]