 Anatomy, Shoulder and Upper Limb, Wrist Extensor Muscles
Anatomy, Shoulder and Upper Limb, Wrist Extensor Muscles
Introduction
The wrist extensor muscles form a coordinated group within the posterior compartment of the forearm and are essential for hand positioning, grip mechanics, and overall upper extremity function. Many of these muscles share a common origin at or near the lateral epicondyle of the humerus and act synergistically to extend the wrist and produce radial or ulnar deviation. Functionally, the wrist extensors contribute substantially to stability during gripping and complex motor tasks by maintaining the wrist in slight extension and permitting optimal force generation by the flexors.[1]
The wrist extensors' superficial location, repetitive loading, and frequent use during sports and occupational activities predispose these muscles to certain disorders. Common pathophysiological processes include overuse injuries and nerve palsies. For example, stenosing tenosynovitis and tendinopathies associated with repetitive microtrauma may produce pain and impair movement.[2] Neurologic injury is another important clinical consideration. For example, radial nerve palsy may impair wrist extensor function, resulting in the characteristic presentation of wrist drop.[3] Familiarity with the anatomy and function of the wrist extensors informs diagnosis, treatment planning, and rehabilitation strategies for disorders affecting wrist motion and grip performance.
Structure and Function
Register For Free And Read The Full Article
 Search engine and full access to all medical articles
Search engine and full access to all medical articles- 10 free questions in your specialty
- Free CME/CE Activities
- Free daily question in your email
- Save favorite articles to your dashboard
- Emails offering discounts
Learn more about a Subscription to StatPearls Point-of-Care
Structure and Function
The forearm is classically divided into 2 compartments: anterior (flexor-pronator) and posterior (extensor-supinator). These compartments are separated by the deep fascia of the forearm, intermuscular septa, and the interosseous membrane (IOM), a fibrous tissue layer spanning the ulna and radius (see Image. Cross Section of the Forearm).
The posterior compartment is further subdivided into superficial and deep layers. The superficial layer contains the brachioradialis, extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor digitorum, extensor digiti minimi (EDM; also called "extensor digiti quinti proprius"), and extensor carpi ulnaris (ECU) muscles. The deep layer includes the supinator, abductor pollicis longus (APL), extensor pollicis longus (EPL), extensor pollicis brevis (EPB), and extensor indicis (also termed "extensor indicis proprius") muscles.
The muscles of the posterior compartment act in coordination to produce complex movements that stabilize the wrist and position the hand. Although each muscle may function independently, specific forearm and hand positions may help isolate select muscles during clinical examination. For example, neutral wrist extension requires balanced activation of the principal radial deviators, the ECRL and ECRB, and the ulnar deviator, the ECU.[4][5] Contributions from deviators within the flexor compartment further influence this balance, underscoring the integrated biomechanics necessary for wrist stability and effective hand function.
Embryology
All skeletal muscle originates from the paraxial mesoderm, which segments into paired structures called somites during early embryogenesis.[6] Each somite differentiates into the myotome, which gives rise to skeletal muscle; the dermatome, which forms the dermis; and the sclerotome, which develops into the axial skeleton.[7]
Muscle tissue formation (myogenesis) begins when cells within the myotome differentiate into myoblasts. These muscle precursor cells subsequently proliferate, migrate to their final anatomical locations, and fuse to form multinucleated myotubes, which later mature into skeletal muscle fibers.[8] Over time, skeletal muscle fibers organize into fascicles and ultimately form functional muscles. Genetic signaling pathways and myogenic regulatory factors tightly regulate this process and coordinate cell proliferation, migration, differentiation, and fusion. Proper skeletal muscle development depends on the precise coordination of cell migration, differentiation, and molecular signaling during early embryogenesis.[9] Disruption of these processes may result in congenital musculoskeletal abnormalities or myopathic conditions.
In the developing upper limb, myogenic precursor cells from the cervical somites migrate into the limb bud and organize into dorsal (extensor) and ventral (flexor) muscle masses, which give rise to the muscles of the posterior and anterior forearm compartments, respectively.[10] Early patterning establishes the fundamental compartmental organization of the forearm.
Blood Supply and Lymphatics
Arterial supply to the upper extremity originates from major vessels arising from the aortic arch. On the right, blood flow passes through the brachiocephalic trunk before entering the right subclavian artery, whereas on the left, the subclavian artery arises directly from the aortic arch. Distal to these origins, the arterial supply to the upper extremities follows a largely symmetrical course, although anatomic variations are common.
The subclavian artery becomes the axillary artery as it crosses the lateral border of the 1st rib. The axillary artery traverses the axilla and continues as the brachial artery at the inferior border of the teres major muscle. The brachial artery courses along the medial aspect of the arm and gives off the deep brachial (profunda brachii) artery, which supplies the posterior compartment of the arm, along with multiple smaller branches that supply the elbow joint.[11] The brachial artery divides into the radial and ulnar arteries upon reaching the cubital fossa.
Near their origins, the radial and ulnar arteries give rise to the recurrent radial artery and the anterior and posterior recurrent ulnar arteries. The ulnar artery also gives rise to the common interosseous artery, which divides into the anterior and posterior interosseous arteries, with the posterior interosseous artery providing the principal arterial supply to the muscles of the posterior forearm.[12]
The radial and ulnar arteries traverse the forearm. The ulnar artery provides the primary contribution to the superficial palmar arch, whereas the radial artery serves as the chief contributor to the deep palmar arch. Both arches anastomose within the palm (see Image. Forearm Arteries).
Lymphatic drainage of the upper extremity remains less well characterized in vivo but has been increasingly studied using near-infrared fluorescence lymphatic imaging with indocyanine green.[13] These studies describe 3 primary channels of lymphatic drainage of the forearm and hand: medial, arising from the volar surface of the forearm; radial, arising from the 1st webspace; and ulnar, arising from the 4th webspace. Proximally, these channels converge along the basilic (medial) and cephalic (lateral) veins and ultimately drain into the axillary lymph node basin.
Nerves
Innervation of the posterior forearm is provided by the radial nerve, which originates from the posterior cord of the brachial plexus (C5–T1). Within the arm, the radial nerve travels along the posterior surface of the humerus in the radial (spiral) groove, accompanied by the deep brachial (profunda brachii) artery. The radial nerve then courses anteriorly around the lateral aspect of the distal humerus, passing between the brachialis and brachioradialis, before passing anterior to the lateral epicondyle. The radial nerve divides into superficial (sensory) and deep (motor) branches near the level of the radial head (see Image. Nerves of the Posterior Upper Limb). The main branch of the radial nerve provides motor innervation to the brachioradialis and ECRL proximal to this division. The deep branch typically innervates the ECRB before piercing the 2 heads of the supinator. Distal to the supinator, the deep branch continues as the posterior interosseous nerve (PIN), which supplies the remaining extensor muscles.[14]
The radial tunnel extends from the lateral condyle to the distal supinator and serves as the pathway for the deep radial nerve prior to its emergence as the PIN.[15] Within this tunnel, the arcade of Frohse appears as a fibrous band formed by the proximal edge of the supinator muscle and is the most common site of PIN compression.[16] The superficial branch of the radial nerve is purely sensory and courses along the lateral forearm deep to the brachioradialis. Distally, the superficial branch emerges to provide cutaneous sensation to the dorsolateral aspect of the hand, including the dorsal aspects of digits 1 to 3 and the dorsolateral 1/2 of digit 4, proximal to the nail beds.[17]
Muscles
The wrist extensor muscles are located in the posterior compartment of the forearm. Many of these muscles originate from or near the lateral epicondyle of the humerus, often referred to clinically as the "common extensor tendon." The posterior compartment is typically divided into superficial and deep layers, separated by an intervening fascial plane and distinguished primarily by functional and innervation differences. Collectively, the primary function of the posterior forearm muscles includes extension of the wrist and digits, with additional roles in radial and ulnar deviation of the wrist and abduction of the thumb.
Superficial Layer
The superficial muscles of the posterior forearm primarily extend the wrist, with most also contributing to extension of digits 2 through 5 (see Image. Forearm Extensor Muscles and Tendons). The origins, insertions, and actions of these muscles are outlined below.
The brachioradialis originates from the proximal 2/3 of the lateral supracondylar ridge of the humerus and inserts on the lateral surface of the distal radius, proximal to the radial styloid process. The primary function of this muscle is elbow flexion, especially when the forearm is in a neutral position, midway between pronation and supination. Clinically, the brachioradialis reflex is used to assess C5 and C6 nerve root function, as well as radial nerve integrity. An abnormal or inverted reflex response may indicate radial nerve injury or cervical spinal cord pathology, including degenerative cervical myelopathy.[18][19]
The ECRL originates from the lateral supracondylar ridge of the humerus and inserts on the dorsal base of the 2nd metacarpal. The muscle's main functions include wrist extension and radial deviation, along with stabilization of the wrist during power grip and fist clenching.
The ECRB originates from the lateral epicondyle of the humerus and inserts on the dorsal base of the 3rd metacarpal. This muscle primarily extends the wrist and assists in radial deviation, contributing to wrist stabilization during finger flexion.
The mobile wad (of Henry) comprises the brachioradialis, ECRL, and ECRB, which collectively occupy the posterolateral forearm. Although located within the superficial layer of the posterior compartment, these muscles are often described separately due to their anatomical position and functional roles at the elbow and wrist, as well as their collective surgical mobility.[20][21] These muscles are also described as forming a functional lateral compartment of the forearm.[22]
The extensor digitorum (extensor digitorum communis) originates from the lateral epicondyle of the humerus and inserts into the common extensor expansions of digits 2 through 5. The muscle primarily extends the medial 4 digits at the metacarpophalangeal (MCP) joints, with secondary contribution to interphalangeal joint extension via the extensor mechanism.
The EDM originates from the lateral epicondyle of the humerus and inserts into the extensor expansion of the 5th digit. The muscle's chief function is to extend digit 5, particularly at the MCP joint.
The ECU originates from the lateral epicondyle of the humerus and the posterior border of the ulna and inserts on the dorsal base of the 5th metacarpal. The muscle’s primary functions are to extend the wrist and assist in ulnar deviation, with additional contribution to wrist stabilization during gripping and fist clenching.
Deep Layer
The deep muscles of the posterior forearm primarily control thumb movement, index finger extension, and forearm supination (see Image. Muscles of the Forearm, Wrist, and Hand). The origins, insertions, and actions of these muscles are discussed below.
The supinator originates from the lateral epicondyle of the humerus, the radial collateral and annular ligaments, the supinator fossa, and the crest of the ulna, and inserts on the lateral, posterior, and anterior surfaces of the proximal radius. The muscle supinates the forearm, most effectively when the elbow is extended.
The extensor indicis originates from the posterior surface of the distal 3rd of the ulna and IOM and inserts on the extensor hood of the 2nd digit. The muscle extends the 2nd digit independently and contributes to wrist extension.
The APL originates from the proximal posterior surfaces of the radius and ulna, as well as the posterior IOM, and inserts on the base of the 1st metacarpal. The muscle acts to abduct and extend the thumb at the carpometacarpal (CMC) joint.
The EPL originates from the posterior surface of the ulna and IOM and inserts on the dorsal base of the distal phalanx of the thumb. The muscle functions to extend the thumb at the interphalangeal joint and contributes to extension at the MCP and CMC joints.
The EPB originates from the posterior surface of the distal radius and IOM and inserts on the dorsal base of the proximal phalanx of the thumb. The muscle extends the thumb at the MCP joint and contributes to extension and abduction at the CMC joint.
Extensor Retinaculum and Dorsal Compartments
Distally, the tendons of the posterior forearm muscles pass deep to the extensor retinaculum, a fibrous band located on the dorsal aspect of the wrist. The extensor retinaculum stabilizes the extensor tendons and prevents bowstringing during wrist extension.
Deep to the extensor retinaculum, the tendons are organized into 6 osteofibrous compartments, numbered 1 through 6 from radial to ulnar. Although anatomical variations exist and should be considered, the tendons of the muscles typically pass through these compartments as follows:
- Compartment 1: APL and EPB
- Compartment 2: ECRL and ECRB
- Compartment 3: EPL
- Compartment 4: Extensor digitorum and extensor indicis
- Compartment 5: EDM
- Compartment 6: ECU [23]
These compartments have clinical significance because tendon inflammation or additional septation within a compartment may lead to stenosing tenosynovitis. De Quervain tenosynovitis most notably involves the 1st dorsal compartment.
Physiologic Variants
Anatomic variation within the extensor musculature of the posterior forearm and the dorsal extensor compartments of the wrist is common. Reported variations include the presence of accessory muscle bellies, duplicated or absent tendons, anomalous attachments, and septation of the fibro-osseous tunnels deep to the extensor retinaculum. Although many variants are incidental findings, some carry important clinical implications, particularly in relation to tendon entrapment syndromes, surgical decompression, and tendon transfer procedures. Recognition of these variants may reduce diagnostic error and improve operative planning.[24]
First Dorsal Compartment Septation
One of the most clinically relevant variations involves the 1st dorsal extensor compartment of the wrist, which typically contains the tendons of APL and EPB.[25] These tendons are generally expected to share a single tunnel without internal septation. However, a septum dividing the compartment into separate APL and EPB subcompartments has been reported in more than 60% of the population.[26] Incomplete release of a separate EPB subcompartment is a recognized cause of persistent symptoms following surgical treatment of De Quervain tenosynovitis.
Abductor Pollicis Longus Tendon Variability
Marked variability exists in the number and morphology of the APL tendon, with multiple tendon slips reported frequently. Accessory slips may insert on the base of the 1st metacarpal, trapezium, opponens pollicis, or APB, with insertion onto the APB being the most common pattern. Multiple APL slips may increase crowding within the 1st dorsal compartment, alter thumb CMC biomechanics, and complicate decompression surgery.[27]
Extensor Digitorum Variability
The extensor digitorum demonstrates considerable variation in tendon distribution, including splitting or absence of tendon slips to digits 2 through 5.[28] Such variations may affect independent finger extension and influence clinical examination findings, as well as tendon reconstruction strategies.[29]
Extensor Indicis Variations
The extensor indicis may present with multiple slips or be duplicated, underdeveloped, or absent. Preoperative awareness of anomalous anatomy is clinically important, especially when reconstructing the EPL after rupture, since the extensor indicis is frequently used as a donor tendon.[30] Multiple extensor indicis slips within the 4th dorsal compartment may rarely lead to extensor indicis proprius syndrome, which is characterized by dorsal wrist pain and painful tenosynovitis from crowding within the compartment.[31]
Extensor Carpi Ulnaris Stabilizing Variants
The ECU tendon is typically stabilized within the 6th dorsal compartment by a fibro-osseous subsheath. Any variations in the structure due to congenital laxity, shallow ulnar groove morphology, or subsheath attenuation may predispose individuals to ECU tendon instability or subluxation, particularly athletes who perform repetitive forearm rotation (eg, tennis, golf, rugby).[32]
Accessory Extensor Muscles
Accessory extensor muscles are relatively uncommon. However, the clinical relevance of these structures stems from their potential to present as dorsal wrist masses, produce pain, crowd the dorsal wrist compartments, or serve as donor tendons in reconstructive procedures.[33]
The extensor medii proprius is analogous to the extensor indicis, although its primary function involves extension of the middle finger. The extensor medii proprius typically originates from the distal ulna and IOM and inserts on the extensor expansion of the 3rd digit.[34]
The extensor indicis et medii communis is a rare muscle variant in which a single muscle belly or tendon supplies both the index (indicis) and middle (medii) fingers.[35] The extensor indicis et medii communis may replace or coexist with the extensor indicis and carries importance in surgical planning, particularly during tendon grafting and reconstructive procedures.[36]
The extensor pollicis et indicis is a rare anomalous muscle that provides a shared tendon or muscle belly to both the thumb and index finger extensors. The extensor pollicis et indicis may alter expected thumb mechanics and warrants recognition during surgical exploration.
The extensor digitorum brevis manus is an anomalous muscle that typically originates from the distal radius, dorsal radiocarpal ligament, or wrist capsule and inserts into the extensor expansion of the index or middle finger.[37] The extensor digitorum brevis manus is located on the dorsum of the hand and may be mistaken for a ganglion cyst or soft-tissue mass.[38]
Surgical Considerations
Disorders involving the posterior forearm compartment and dorsal wrist extensors are typically managed initially with nonoperative treatment, including activity modification, splinting, physical therapy, anti-inflammatory medication intake, and corticosteroid injections when appropriate. Surgical intervention is considered when conservative treatment fails or urgent management is required for acute pathology. Common procedures include tendon decompression or compartment release, tendon repair, tendon transfer or grafting following rupture or nerve palsy, synovectomy, and fasciotomy for acute compartment syndrome. Successful surgical management requires familiarity with extensor tendon anatomy, dorsal compartment relationships, regional neurovascular organization and distribution, and common anatomic variations.
Dorsal Compartment Anatomy
A thorough understanding of the extensor retinaculum and dorsal extensor compartments is essential. The 1st dorsal compartment was originally described anatomically as containing the tendons of the EPB and APL within a single tunnel formed by the extensor retinaculum. Subsequent studies have demonstrated considerable anatomic variability, often including an intertendinous septum that divides the compartment into separate APL and EPB subcompartments. Failure to identify and release all septated portions is a well-documented cause of unsuccessful De Quervain release. Although the anatomy of the 1st dorsal compartment is highly variable, all dorsal compartments warrant evaluation for additional septations or anomalous tendons that may contribute to tenosynovitis.
Nerve Protection
Nerve protection requires careful identification and dissection of neural structures to prevent iatrogenic sensory loss or painful neuroma formation.[39] The superficial branch of the radial nerve is particularly vulnerable during radial-sided wrist approaches and 1st dorsal compartment release procedures. The deep branch of the radial nerve and its continuation, the PIN, are especially vulnerable during proximal forearm surgery, radial tunnel decompression, and procedures involving the supinator.
Tendon Transfer Considerations
Tendon transfer is commonly performed in cases of irreparable extensor tendon rupture or radial nerve palsy. A common example involves the transfer of the extensor indicis to the EPL to restore thumb interphalangeal extension. Preoperative identification of anatomic variants is important to ensure appropriate donor tendon availability and function.
Vascular Considerations
Vascular considerations involve radial and ulnar arterial contributions to collateral perfusion of the hand via the superficial and deep palmar arches, with substantial anatomic variability.[40] Assessment of collateral flow may be performed using the Allen Test and confirmed with Doppler ultrasonography when arterial injury, harvest, or compromise is anticipated prior to surgery (see Image. Modified Allen Test).[41]
Forearm Compartment Syndrome
Acute forearm compartment syndrome is a surgical emergency caused by elevated compartment pressure leading to impaired tissue perfusion and progressive ischemia of muscle and nerve.[42] Common causes include fracture, crush injury, reperfusion injury, anticoagulation, and prolonged external compression of the forearm. Timely recognition and fasciotomy are essential to minimize permanent dysfunction.
Common Surgical Complications
Common surgical complications following extensor tendon, dorsal compartment, and radial-sided wrist procedures arise from soft-tissue dissection, tendon manipulation, nerve proximity, and postoperative scarring. Iatrogenic nerve injury may occur during exposure or decompression. Incomplete tendon release or compartment decompression may result in persistent symptoms. Tendon adhesions may limit gliding and reduce function. Infection may complicate wound healing. Scar hypersensitivity may develop after incision or dissection. Persistent postoperative pain may reflect nerve irritation or unresolved pathology. Stiffness and reduced range of motion may follow immobilization or fibrosis. Recurrent instability or tenosynovitis may occur due to incomplete correction or ongoing mechanical stress.
Clinical Significance
Lateral Epicondylitis
Lateral epicondylitis, also known as tennis elbow, is a common cause of elbow musculoskeletal pain, affecting approximately 1% to 3% of the population. The condition is most often associated with degenerative tendinopathy of the ECRB at its origin on the lateral epicondyle, resulting from repetitive wrist extension and forearm supination.
Patients typically present with localized pain over the lateral epicondyle of the humerus, exacerbated by resisted wrist extension or gripping activities. Clinical diagnosis is supported by resisted wrist extension testing, with reproduction of pain supporting the diagnosis of lateral epicondylitis. Functional assessments, such as the chair lift test, may also reproduce symptoms when pain occurs during the lifting of a chair with the wrist extended.
Management of lateral epicondylitis is initially conservative, including nonsteroidal anti-inflammatory drug therapy, corticosteroid injections, physical therapy, and muscle strengthening.[43] Surgical options are considered when conservative management fails, with primary focus on release or debridement of degenerated ECRB tendon tissue.
De Quervain Tenosynovitis
De Quervain tenosynovitis is a stenosing tenosynovitis affecting the 1st dorsal compartment, involving the APL and EPB tendons within this compartment (see Image. De Quervain Tenosynovitis Anatomy). The condition most commonly affects women aged between 30 and 50 years and individuals performing repetitive wrist deviation and thumb abduction.
Patients typically present with pain over the radial styloid, often exacerbated by thumb movements during grasping, pinching, or lifting. Diagnosis has commonly relied on provocative maneuvers such as the Finkelstein test, although the wrist hyperflexion and abduction of the thumb (WHAT) test, along with ultrasonography, has gained increasing use.
Anatomic variations, including the formation of multiple APL tendon slips and septation of the 1st dorsal compartment, may predispose to De Quervain tenosynovitis and contribute to treatment failure in some cases. The initial management consists of conservative therapy with splinting, nonsteroidal anti-inflammatory drug intake, activity modification, and corticosteroid injection. Surgical release of the 1st extensor compartment may be required when conservative management fails.
Intersection Syndrome
Intersection syndrome is an overuse tenosynovitis caused by friction at the intersection of extensor tendons in the posterior forearm. Two types are recognized: proximal and distal. Proximal intersection syndrome occurs at the crossing of the 1st dorsal compartment tendons (APL, EPB) over the 2nd compartment tendons (ECRL, ECRB), approximately 4 to 8 cm proximal to the Lister tubercle. Distal intersection syndrome is less common and involves the intersection of the 3rd compartment (EPL) with the 2nd compartment.
Patients with intersection syndrome present with pain, swelling, and crepitus over the dorsal forearm, exacerbated by repetitive wrist motion. Diagnosis is clinical but may be supported by ultrasound or magnetic resonance imaging (MRI) demonstrating peritendinous edema and tenosynovitis. Most patients respond to conservative management, but persistent cases may require surgical synovectomy.
Extensor Pollicis Longus Rupture
EPL rupture is most commonly associated with distal radius fractures and may also occur in inflammatory conditions such as rheumatoid arthritis.[44] The region around the Lister tubercle is the point of greatest vulnerability, where the tendon is subjected to mechanical wear and has relatively limited vascular supply. Patients often report dorsal wrist pain, a snapping sensation, or sudden inability to extend the thumb at the interphalangeal joint.[45] Diagnosis is clinical and may be confirmed with imaging modalities such as ultrasound or MRI. Limited healing capacity of the tendon generally necessitates surgical management, with extensor indicis tendon transfer being the most common reconstructive approach.
Extensor Carpi Ulnaris Tendon Disease
ECU tendon disease encompasses a spectrum of pathologies, including tendinopathy (tendon thickening), tenosynovitis (inflammatory changes of the tendon or tendon sheath), tendon instability, and tendon rupture. These entities may occur as isolated or combined entities and may be identified using ultrasound (see Image. Extensor Carpi Ulnaris Tenosynovitis on Magnetic Resonance Imaging). These conditions are commonly observed in athletes performing repetitive forearm rotation and ulnar deviation, as in golf, tennis, and rugby.
ECU tendon pathology typically presents with ulnar-sided wrist pain, often aggravated by supination, ulnar deviation, and resisted wrist extension. Dynamic ultrasonography and MRI are useful adjuncts to clinical evaluation, particularly in atypical presentations and cases resistant to conservative management.[46]
Radial Nerve Injury
Radial nerve injury results in motor or sensory deficits distal to the site of injury, depending on the level involved. Proximal injuries at the axilla or along the radial groove of the humerus may result in wrist drop, loss of finger extension, and sensory deficits over the dorsolateral hand and posterior forearm. Compression injuries may result from sustained external pressure, as seen in individuals using crutches (crutch palsy) or resting the arm on a chair back for prolonged periods (Saturday night palsy).
When an injury occurs distal to the radial nerve branching, clinical features depend on the involved branch. Superficial branch injury results in sensory deficits with preserved motor function. Deep branch injury produces motor deficits with preserved sensation.
PIN syndrome is a compressive neuropathy most commonly caused by PIN entrapment at the arcade of Frohse within the radial tunnel. Patients typically present with painless weakness of finger and thumb extension. PIN involvement is purely motor. Thus, patients do not experience sensory deficits. Diagnosis relies primarily on clinical evaluation and may be supported by ultrasonography or MRI. Conservative management is often effective, with surgical decompression reserved for persistent or progressive cases.
Ganglion Cyst Compression of Extensor Tendons
Ganglion cysts are the most common soft tissue masses of the wrist and may arise dorsally or volarly (see Image. Clinical Presentation of a Ganglion Cyst).[47] Most cases are asymptomatic, without ligament disruption, edema, or intraosseous communication. Dorsal ganglion cysts may compress or irritate adjacent extensor tendons, particularly the extensor digitorum and EPL, resulting in pain, mechanical symptoms, or findings that may mimic tenosynovitis.[48]
Media
(Click Image to Enlarge)
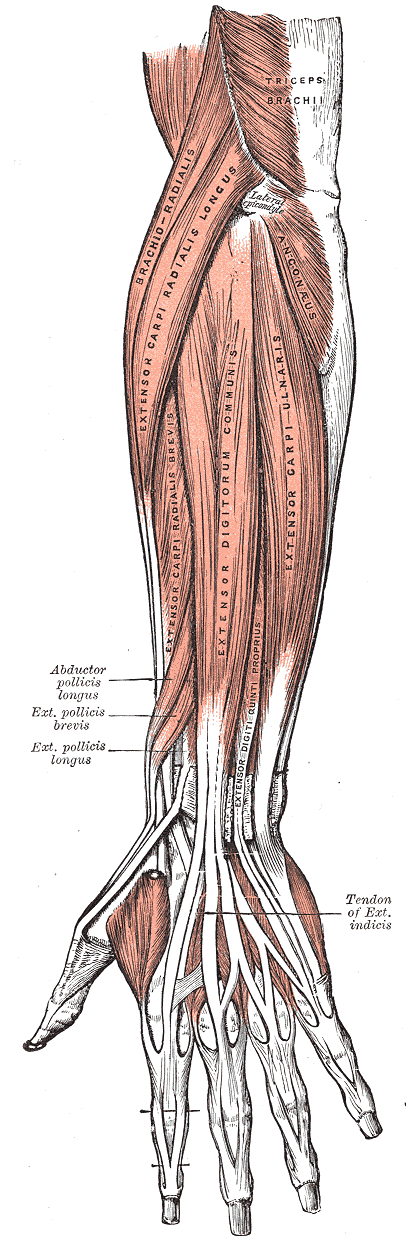
Forearm Extensor Muscles and Tendons. This illustration demonstrates the anatomic relationships of the superficial muscles of the posterior forearm, including the brachioradialis, extensor carpi radialis longus, extensor carpi radialis brevis, extensor digitorum (extensor digitorum communis), extensor digiti minimi (extensor digiti quinti proprius), and extensor carpi ulnaris. Tendons arising from the deep layer are also shown, including the abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, and extensor indicis tendons. The common extensor origin at the lateral epicondyle of the humerus is illustrated. Posterior arm musculature, including the triceps brachii and anconeus, is also depicted.
Henry Vandyke Carter, Public domain, via Wikimedia Commons
(Click Image to Enlarge)
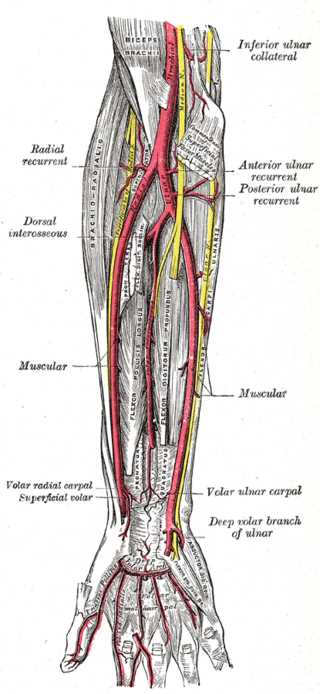
Forearm Arteries. This image highlights the ulnar artery's deep palmar branch and the radial, ulnar, anterior and posterior ulnar recurrent, dorsal interosseous, volar interosseous (termination), dorsal ulnar carpal, dorsal radial carpal arteries, muscular, radial recurrent, volar radial carpal, superficial volar, and volar ulnar carpal arteries. The arm's inferior ulnar collateral and profunda brachii arteries and the ulnar artery's deep volar branch in the hand are also shown.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
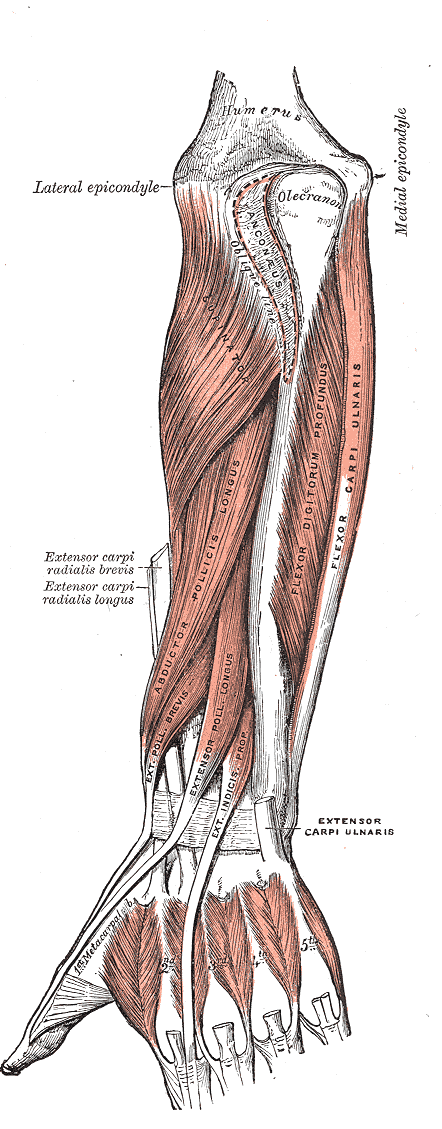
Muscles of the Forearm, Wrist, and Hand. This posterior view illustrates the deep layer of the posterior forearm musculature, including the supinator, abductor pollicis longus, extensor pollicis longus, extensor pollicis brevis, and extensor indicis (extensor indicis proprius). Also shown are the transected tendons of the superficial extensor muscles, including the extensor carpi radialis longus, extensor carpi radialis brevis, and extensor carpi ulnaris. Osseous landmarks include the distal humerus, medial and lateral epicondyles, olecranon, anconeal and oblique line markings of the ulna, and metacarpals 1-5. Portions of the anterior forearm compartment are also visible, including the flexor digitorum profundus and flexor carpi ulnaris muscles.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Image to Enlarge)
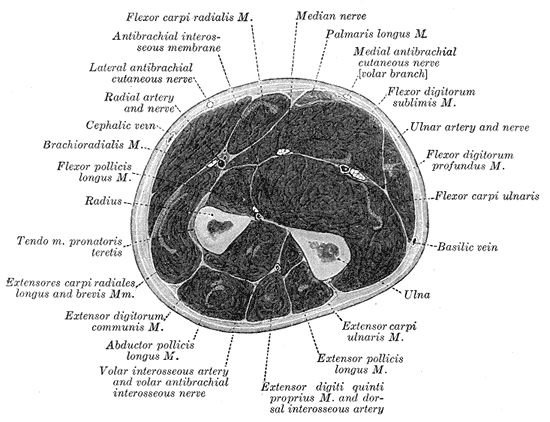
Cross Section of the Forearm. The illustrated image depicts the radius, ulna, muscles, and fasciae of the forearm.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
{kind=link}
(Click Image to Enlarge)
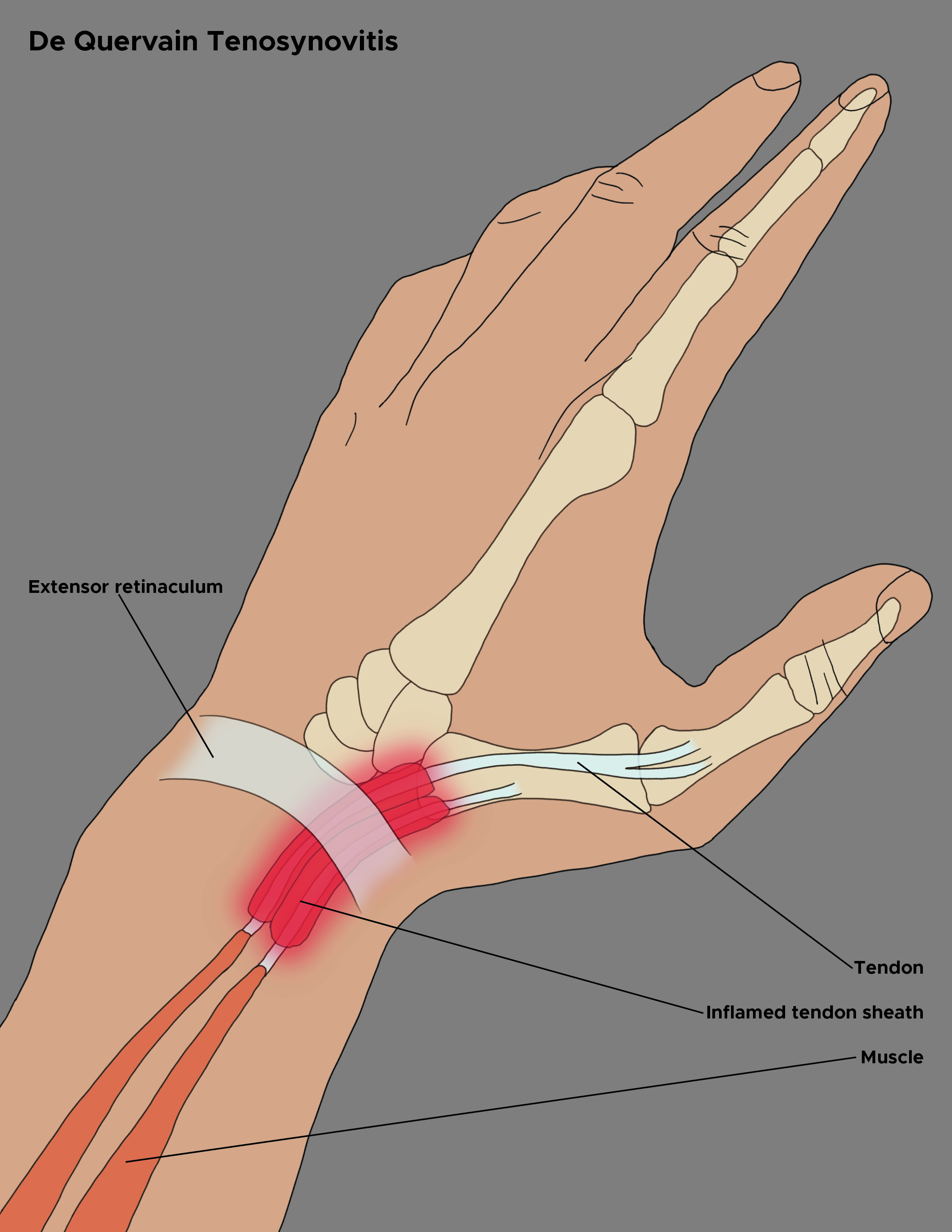
De Quervain Tenosynovitis Anatomy. This illustration highlights the inflammation of the tendon sheath at the base of the thumb. The image outlines the affected tendons and muscles, as well as the extensor retinaculum of the wrist.
Contributed by Chelsea Rowe
(Click Image to Enlarge)
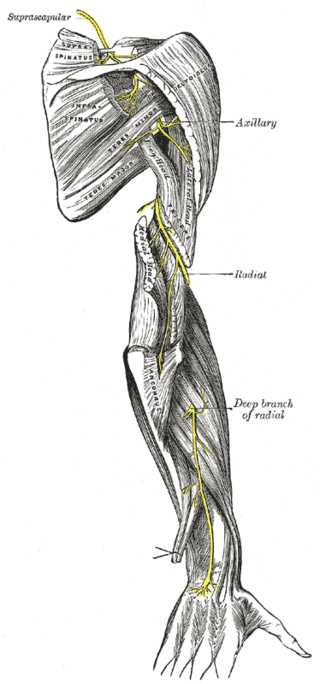
Nerves of the Posterior Upper Limb. This posterior view of the right upper extremity illustrates the distribution of the major nerves. The suprascapular nerve is shown innervating the rotator cuff muscles, while the axillary nerve supplies the deltoid and teres minor. The radial nerve is depicted descending the arm, providing branches to the 3 heads of the triceps brachii and the anconeus, before continuing as the deep branch to supply the posterior compartment of the forearm.
Henry Vandyke Carter, Public Domain, via Wikimedia Commons
(Click Video to Play)
Modified Allen Test. The modified Allen test assesses whether the ulnar artery can adequately supply the hand if the radial artery is ligated, as during radial forearm flap harvest.
Contributed by MH Hohman, MD, FACS
(Click Image to Enlarge)
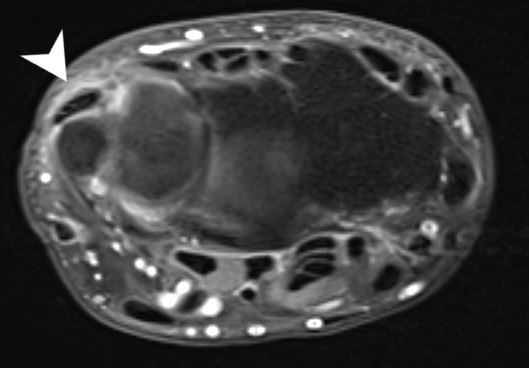
Extensor Carpi Ulnaris Tenosynovitis on Magnetic Resonance Imaging. This axial scan of the wrist displays inflammation and fluid accumulation within the 6th extensor compartment. The arrowhead points directly to the prominent fluid distention surrounding the extensor carpi ulnaris tendon.
Contributed by Dawood Tafti, MD.
(Click Image to Enlarge)

Clinical Presentation of a Ganglion Cyst. A photograph of the dorsal aspect of a human hand reveals a distinct, localized swelling near the joint. The highlighted area emphasizes a ganglion cyst protruding from the wrist tissue.
Contributed by StatPearls
References
Forman DA, Forman GN, Robathan J, Holmes MWR. The influence of simultaneous handgrip and wrist force on forearm muscle activity. Journal of electromyography and kinesiology : official journal of the International Society of Electrophysiological Kinesiology. 2019 Apr:45():53-60. doi: 10.1016/j.jelekin.2019.02.004. Epub 2019 Feb 19 [PubMed PMID: 30822679]
Fakoya AO, Tarzian M, Sabater EL, Burgos DM, Maldonado Marty GI. De Quervain's Disease: A Discourse on Etiology, Diagnosis, and Treatment. Cureus. 2023 Apr:15(4):e38079. doi: 10.7759/cureus.38079. Epub 2023 Apr 24 [PubMed PMID: 37252462]
Węgiel A, Karauda P, Zielinska N, Tubbs RS, Olewnik Ł. Radial nerve compression: anatomical perspective and clinical consequences. Neurosurgical review. 2023 Feb 13:46(1):53. doi: 10.1007/s10143-023-01944-2. Epub 2023 Feb 13 [PubMed PMID: 36781706]
Level 3 (low-level) evidenceWeber A, Reissner L, Friedl S, Schweizer A. Stability of the distal radioulnar joint with and without activation of forearm muscles. The Journal of hand surgery, European volume. 2023 Sep:48(8):762-767. doi: 10.1177/17531934231168299. Epub 2023 May 1 [PubMed PMID: 37125755]
Fridén J, Lieber RL. Wrist extensor pathomechanics: implications for tendon and nerve transfer. The Journal of hand surgery, European volume. 2024 Sep:49(8):1047-1050. doi: 10.1177/17531934231224737. Epub 2024 Jan 8 [PubMed PMID: 38190974]
Chal J, Pourquié O. Making muscle: skeletal myogenesis in vivo and in vitro. Development (Cambridge, England). 2017 Jun 15:144(12):2104-2122. doi: 10.1242/dev.151035. Epub [PubMed PMID: 28634270]
Wilde S, Feneck EM, Mohun TJ, Logan MPO. 4D formation of human embryonic forelimb musculature. Development (Cambridge, England). 2021 Feb 17:148(4):. doi: 10.1242/dev.194746. Epub 2021 Feb 17 [PubMed PMID: 33234713]
Zhang B, He P, Lawrence JEG, Wang S, Tuck E, Williams BA, Roberts K, Kleshchevnikov V, Mamanova L, Bolt L, Polanski K, Li T, Elmentaite R, Fasouli ES, Prete M, He X, Yayon N, Fu Y, Yang H, Liang C, Zhang H, Blain R, Chedotal A, FitzPatrick DR, Firth H, Dean A, Bayraktar OA, Marioni JC, Barker RA, Storer MA, Wold BJ, Zhang H, Teichmann SA. A human embryonic limb cell atlas resolved in space and time. Nature. 2024 Nov:635(8039):668-678. doi: 10.1038/s41586-023-06806-x. Epub 2023 Dec 6 [PubMed PMID: 38057666]
Thirkannad SM, Patil R. The Story of the Hand. Indian journal of plastic surgery : official publication of the Association of Plastic Surgeons of India. 2021 Apr:54(2):106-113. doi: 10.1055/s-0041-1729771. Epub 2021 Jul 5 [PubMed PMID: 34239230]
Suzuki T. Current research on mechanisms of limb bud development, and challenges for the next decade. Genes & genetic systems. 2024 Mar 29:99():. doi: 10.1266/ggs.23-00287. Epub 2024 Feb 21 [PubMed PMID: 38382923]
Friedman DD, Ponkowski MJ, Shetty AS, Hoegger MJ, Itani M, Rajput MZ, Mellnick VM, Raptis CA, Northrup BE, Ballard D, Cabrera Lebron JA, Tsai R. CT Angiography of the Upper Extremities: Review of Acute Arterial Entities. Radiographics : a review publication of the Radiological Society of North America, Inc. 2025 Jan:45(1):e240077. doi: 10.1148/rg.240077. Epub [PubMed PMID: 39745868]
Granoff MD, Pardo JA, Johnson AR, Fleishman A, Tillotson E, Thomson S, Lee BT, Singhal D. Superficial and Functional Lymphatic Anatomy of the Upper Extremity. Plastic and reconstructive surgery. 2022 Oct 1:150(4):900-907. doi: 10.1097/PRS.0000000000009555. Epub 2022 Aug 4 [PubMed PMID: 35939638]
Lee YW, Lee SH, You HJ, Jung JA, Yoon ES, Kim DW. Lymphatic vessel mapping in the upper extremities of a healthy Korean population. Archives of plastic surgery. 2018 Mar:45(2):152-157. doi: 10.5999/aps.2017.00983. Epub 2018 Mar 15 [PubMed PMID: 29566468]
Jeon A, Kim YG, Kwon SO, Lee JH. Relationship between the Branching Patterns of the Radial Nerve and Supinator Muscle. BioMed research international. 2021:2021():8691114. doi: 10.1155/2021/8691114. Epub 2021 Oct 14 [PubMed PMID: 34692843]
Caetano EB, Vieira LA, Sabongi Neto JJ, Caetano MBF, Picin CP, Silva Júnior LCND. Anatomical Study of the Motor Branches of the Radial Nerve in the Forearm. Revista brasileira de ortopedia. 2020 Dec:55(6):764-770. doi: 10.1055/s-0040-1713403. Epub 2020 Dec 18 [PubMed PMID: 33364657]
Benes M, Kachlik D, Kunc V, Kunc V. The arcade of Frohse: a systematic review and meta-analysis. Surgical and radiologic anatomy : SRA. 2021 May:43(5):703-711. doi: 10.1007/s00276-021-02718-5. Epub 2021 Mar 6 [PubMed PMID: 33677682]
Level 1 (high-level) evidencePejkova S, Filipce V, Peev I, Nikolovska B, Jovanoski T, Georgieva G, Srbov B. Brachial Plexus Injuries - Review of the Anatomy and the Treatment Options. Prilozi (Makedonska akademija na naukite i umetnostite. Oddelenie za medicinski nauki). 2021 Apr 23:42(1):91-103. doi: 10.2478/prilozi-2021-0008. Epub 2021 Apr 23 [PubMed PMID: 33894122]
Saunders LM, Sandhu HS, McBride L, Maniarasu VS, Taylor S, Dhokia R. Degenerative Cervical Myelopathy: An Overview. Cureus. 2023 Dec:15(12):e50387. doi: 10.7759/cureus.50387. Epub 2023 Dec 12 [PubMed PMID: 38213348]
Level 3 (low-level) evidenceLin-Wei O, Xian LLS, Shen VTW, Chuan CY, Halim SA, Ghani ARI, Idris Z, Abdullah JM. Deep Tendon Reflex: The Tools and Techniques. What Surgical Neurology Residents Should Know. The Malaysian journal of medical sciences : MJMS. 2021 Apr:28(2):48-62. doi: 10.21315/mjms2021.28.2.5. Epub 2021 Apr 21 [PubMed PMID: 33958960]
Ojike NI, Alla SR, Battista CT, Roberts CS. A single volar incision fasciotomy will decompress all three forearm compartments: a cadaver study. Injury. 2012 Nov:43(11):1949-52. doi: 10.1016/j.injury.2012.08.006. Epub 2012 Aug 17 [PubMed PMID: 22906919]
Raza H, Mahapatra A. Acute compartment syndrome in orthopedics: causes, diagnosis, and management. Advances in orthopedics. 2015:2015():543412. doi: 10.1155/2015/543412. Epub 2015 Jan 19 [PubMed PMID: 25688303]
Level 3 (low-level) evidenceThaker S, Almeer G, Stevenson J, Azzopardi C, Botchu R. Imaging of the lesions in the lateral muscle compartment of the forearm, alias mobile wad of Henry: Demographics, radiological anatomy and surgical relevance. Clinical imaging. 2021 Jan:69():374-379. doi: 10.1016/j.clinimag.2020.10.019. Epub 2020 Oct 13 [PubMed PMID: 33075596]
Marth T, Grob NA, Jacobson JA, Zechmann N, Guggenberger R, Falkowski AL. Tendon Anatomy and Tendon Disorders of the Wrist. RoFo : Fortschritte auf dem Gebiete der Rontgenstrahlen und der Nuklearmedizin. 2025 Oct:197(10):1148-1161. doi: 10.1055/a-2499-5875. Epub 2025 Feb 11 [PubMed PMID: 39933717]
Yammine K. The prevalence of the extensor indicis tendon and its variants: a systematic review and meta-analysis. Surgical and radiologic anatomy : SRA. 2015 Apr:37(3):247-54. doi: 10.1007/s00276-014-1352-0. Epub 2014 Aug 6 [PubMed PMID: 25096501]
Level 1 (high-level) evidenceBonczar M, Walocha J, Pasternak A, Depukat P, Dziedzic M, Ostrowski P, Bonczar T, Warchoł Ł, Koziej M. Anatomical variations in the first dorsal compartment of the wrist: meta-analysis. Folia morphologica. 2023:82(4):766-776. doi: 10.5603/FM.a2022.0081. Epub 2022 Sep 27 [PubMed PMID: 36165900]
Level 1 (high-level) evidenceCoşkun O, Ok F, Şahin B, Gürses İA. First extensor compartment morphology and clinical significance: a cadaver series study. Anatomy & cell biology. 2023 Sep 30:56(3):328-333. doi: 10.5115/acb.23.008. Epub 2023 Mar 29 [PubMed PMID: 36987785]
Marí-Gorreto J, San-Millán M, Carrera A, Tubbs RS, Iwanaga J, Cateura A, Acquabona L, Reina MA, Reina F. The anatomy of the tendon of abductor pollicis longus and its morphological variations: An anatomical approach emphasizing the clinical relevance. Annals of anatomy = Anatomischer Anzeiger : official organ of the Anatomische Gesellschaft. 2023 Apr:247():152068. doi: 10.1016/j.aanat.2023.152068. Epub 2023 Feb 6 [PubMed PMID: 36754243]
Yammine K. The prevalence of the extensor digitorum communis tendon and its insertion variants: a systematic review and meta-analysis. Clinical anatomy (New York, N.Y.). 2014 Nov:27(8):1284-90. doi: 10.1002/ca.22429. Epub 2014 Jun 23 [PubMed PMID: 24953717]
Level 1 (high-level) evidenceZhou J, Frey C, Segovia N, Yao J. Anatomic relationship of extensor indicis propius and extensor digitorum communis: Implications for tendon transfer. World journal of orthopedics. 2022 Nov 18:13(11):978-985. doi: 10.5312/wjo.v13.i11.978. Epub 2022 Nov 18 [PubMed PMID: 36439366]
Herriott JE, Zdilla MJ. Anatomical terminology regarding anatomical variations needs to be refined: An example systematic review of extensor pollicis et indicis and extensor indicis et medii variations. Proceedings of the West Virginia Academy of Science. 2025:97(1):27-39. doi: 10.55632/pwvas.v97i1.1105. Epub 2025 Jan 27 [PubMed PMID: 41346416]
Level 1 (high-level) evidencePatel MR, Moradia VJ, Bassini L, Lei B. Extensor indicis proprius syndrome: a case report. The Journal of hand surgery. 1996 Sep:21(5):914-5 [PubMed PMID: 8891996]
Level 3 (low-level) evidenceThirumavalavan J, Ibrahim Z, Byrne RA, Arant KR, Gil JA. Extensor Carpi Ulnaris Instability: A Comprehensive Review of Pathology and Operative Techniques. Hand (New York, N.Y.). 2024 Oct:19(7):1090-1096. doi: 10.1177/15589447231168908. Epub 2023 May 24 [PubMed PMID: 37226412]
Suwannakhan A, Tawonsawatruk T, Meemon K. Extensor tendons and variations of the medial four digits of hand: a cadaveric study. Surgical and radiologic anatomy : SRA. 2016 Nov:38(9):1083-1093 [PubMed PMID: 27056052]
von Schroeder HP, Botte MJ. The extensor medii proprius and anomalous extensor tendons to the long finger. The Journal of hand surgery. 1991 Nov:16(6):1141-5 [PubMed PMID: 1748763]
Tan ST, Smith PJ. Anomalous extensor muscles of the hand: a review. The Journal of hand surgery. 1999 May:24(3):449-55 [PubMed PMID: 10357521]
Yalçin B, Kutoglu T, Ozan H, Gürbüz H. The extensor indicis et medii communis. Clinical anatomy (New York, N.Y.). 2006 Mar:19(2):112-4 [PubMed PMID: 16283647]
Ranade AV, Rai R, Prabhu LV, Rajanigandha V, Prakash, Janardhanan JP, Ramanathan L, Prameela MD. Incidence of extensor digitorum brevis manus muscle. Hand (New York, N.Y.). 2008 Dec:3(4):320-3. doi: 10.1007/s11552-008-9111-5. Epub 2008 Jun 19 [PubMed PMID: 18780016]
Lee DH, Lee JH, Woo RS, Song DY, Baik TK, Yoo HI. A rare bilateral variation on the dorsum of the hand: extensor digitorum brevis manus and extensor medii proprius. Anatomy & cell biology. 2019 Mar:52(1):97-99. doi: 10.5115/acb.2019.52.1.97. Epub 2019 Mar 29 [PubMed PMID: 30984461]
Besmens IS, Enderlin T, Nietlispach V, Brackertz S, Knipper S, Calcagni M. Neuropathic pain of the superficial branch of the radial nerve - Factors influencing surgical outcome and patient satisfaction. Hand surgery & rehabilitation. 2024 Feb:43(1):101637. doi: 10.1016/j.hansur.2024.101637. Epub 2024 Jan 18 [PubMed PMID: 38244694]
Zarzecki MP, Popieluszko P, Zayachkowski A, Pękala PA, Henry BM, Tomaszewski KA. The surgical anatomy of the superficial and deep palmar arches: A Meta-analysis. Journal of plastic, reconstructive & aesthetic surgery : JPRAS. 2018 Nov:71(11):1577-1592. doi: 10.1016/j.bjps.2018.08.014. Epub 2018 Aug 24 [PubMed PMID: 30245020]
Level 1 (high-level) evidenceDawani P, Mahajan A, Vasudeva N, Mishra S. Variations in the Pattern of the Deep Palmar Arch of the Hand and Its Surgical Importance. Cureus. 2022 Jan:14(1):e20873. doi: 10.7759/cureus.20873. Epub 2022 Jan 2 [PubMed PMID: 35145780]
Botte MJ, Gelberman RH. Acute compartment syndrome of the forearm. Hand clinics. 1998 Aug:14(3):391-403 [PubMed PMID: 9742419]
Level 3 (low-level) evidenceKarabinov V, Georgiev GP. Lateral epicondylitis: New trends and challenges in treatment. World journal of orthopedics. 2022 Apr 18:13(4):354-364. doi: 10.5312/wjo.v13.i4.354. Epub 2022 Apr 18 [PubMed PMID: 35582153]
Kardashian G, Vara AD, Miller SJ, Miki RA, Jose J. Stenosing synovitis of the extensor pollicis longus tendon. The Journal of hand surgery. 2011 Jun:36(6):1035-8. doi: 10.1016/j.jhsa.2011.02.004. Epub [PubMed PMID: 21636022]
Lister RC, Bradford HC 4th, Joo A, Carr CW, Delancy A, Naram A, Rothkopf DM, Shufflebarger JV. Spontaneous Rupture of the Extensor Pollicis Longus Tendon: A Systematic Review. Hand (New York, N.Y.). 2024 Nov:19(8):1314-1320. doi: 10.1177/15589447231175513. Epub 2023 Jun 2 [PubMed PMID: 37269124]
Level 1 (high-level) evidenceCampbell D, Campbell R, O'Connor P, Hawkes R. Sports-related extensor carpi ulnaris pathology: a review of functional anatomy, sports injury and management. British journal of sports medicine. 2013 Nov:47(17):1105-11. doi: 10.1136/bjsports-2013-092835. Epub 2013 Oct 4 [PubMed PMID: 24096897]
Lowden CM, Attiah M, Garvin G, Macdermid JC, Osman S, Faber KJ. The prevalence of wrist ganglia in an asymptomatic population: magnetic resonance evaluation. Journal of hand surgery (Edinburgh, Scotland). 2005 Jun:30(3):302-6 [PubMed PMID: 15862373]
Tomori Y, Motoda N, Nanno M, Majima T. Intratendinous Ganglion of the Extensor Pollicis Longus: Case Report and Literature Review. Journal of Nippon Medical School = Nippon Ika Daigaku zasshi. 2021 Nov 17:88(5):500-505. doi: 10.1272/jnms.JNMS.2021_88-416. Epub 2020 Sep 30 [PubMed PMID: 32999177]
Level 3 (low-level) evidence